
Abstract
Cross-informant ratings of are considered gold standard for child behavioral assessment. To date, little work has examined informant ratings of adaptive functioning for youth with autism spectrum disorder (ASD). In a large, diverse sample of youth with ASD, this study evaluated parent–teacher concordance of ratings of adaptive functioning and ASD-specific symptomatology across time. The impact of child clinical characteristics on concordance was also examined. Participants included 246 children, their caregivers and teachers. Parent–teacher concordance was variable but generally consistent across time. Concordance was significantly impacted by autism severity and child cognitive abilities. Findings inform the broader concordance literature and support the need to consider child clinical factors when assessing child functioning in samples of children with ASD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The use of multiple informant ratings is considered best practice in childhood behavioral assessment to obtain an accurate, comprehensive understanding of child functioning (Mash and Hunsley 2005). The complexity of child behavior, the common behavioral variations seen across settings as well as the identified impact of both informant attributions and perspectives on reporting necessitate the use of multiple informants to obtain a comprehensive and accurate understanding of behavior (De Los Reyes and Kazdin 2005; Dirks et al. 2012; Kraemer et al. 2003). However, variable and often limited concordance or agreement across raters is widely acknowledged in the literature (Achenbach et al. 1987; De Los Reyes and Kazdin 2005). This is especially relevant for youth with autism spectrum disorder (ASD) whose complex clinical presentations tend to be shaped by their environment (Ozonoff et al. 2005). Youth with ASD represent an incredibly complex population with a wide range of adaptive and functional abilities necessitating specialized, and often individualized, interventions (National Research Council 2001). These enduring service needs frequently warrant significant and increasing service usage (Cidav et al. 2013). The reliance on informant report (as opposed to youth self-report) is especially prevalent for youth with ASD given concerns regarding the validity of self-reports related to deficits associated with ASD (e.g., difficulty with communication, understanding emotion; Clark et al. 2014; Tavernor et al. 2013). Most commonly, parents and teachers serve as key informants for children’s behaviors and ASD symptomology. Based on this common practice, the current paper examines concordance on standardized behavioral measures between these two groups.
There is a growing literature examining informant concordance for youth with ASD. Overall, the research indicates moderate agreement between informants (mean weighted r = .38; Stratis and Lecavalier 2015) that is comparable to agreement observed for typically developing youth (Achenbach et al. 2005, 1987; De Los Reyes et al. 2015). Recent work has also examined factors related to concordance in cross-informant comparisons. Further examination reveals variability in concordance across domains, with overall higher concordance for externalizing problems than internalizing problems or social skills (Stratis and Lecavalier 2017). Similar variability has been shown across informant pairs, with evidence of lower concordance between parent–teacher pairs compared to parent–parent or parent–child (Stratis and Lecavalier 2015). Notably, child factors also appear to impact informant concordance. Stratis and Lecavalier (2015) highlight the moderating role of child age, cognitive abilities, and diagnosis (intellectual disability versus ASD) in their recent meta-analysis on cross-informant agreement. ASD symptom severity has also been found to moderate parent–teacher concordance, with higher ASD severity associated with greater concordance (Azad et al. 2015), although not uniformly (see McDonald et al. 2016; Stadnick et al. 2017). Although these findings highlight the importance of considering key child characteristics, the majority of this work has focused on ratings of psychopathology and not child adaptive functioning more broadly. However, major service decisions such as eligibility, intervention targets and response to treatment evaluations are typically made based on general child functioning and abilities, highlighting the need to explore concordance of informant ratings in this area.
Only a handful of studies to date have specifically examined parent–teacher concordance in ratings of child adaptive functioning. This work has suggested generally moderate to high correlations (r’s = .42–.83) between teacher and parent ratings on the original version of the Vineland Adaptive Behavior Scale ([VABS; Sparrow et al. 1984]; Szatmari et al. 1994; Voelker et al. 2000). Further research has observed similarly moderate to high correlations across parent and teacher ratings on the Second Edition of the VABS ([VABS-II; Sparrow et al. 2005], r’s = .42–.83; Lane et al. 2013). However, data examining significant mean differences across parent and teacher ratings of adaptive behaviors are inconsistent, with some suggesting systematic differences (e.g., Barnhill et al. 2000; Foley Nicpon et al. 2010) and others suggesting minimal to no mean differences between informants (Lane et al. 2013). More recent work by McDonald et al. (2016) suggests the presence of differences varies by domain, with significant differences in parent–teacher ratings of adaptive skills but not psychiatric symptoms. Additionally, these ratings are typically cross-sectional and allow for evaluation of concordance at only one point in time, despite the fact that adaptive functioning is often used to examine child progress and response to treatment. There is also inconsistency regarding which informant tends to rate children as more impaired, although there is more evidence of parents consistently rating children as more impacted than teachers (Lopata et al. 2016; McDonald et al. 2016; Szatmari et al. 1994; Voelker et al. 2000). Importantly, ASD severity emerged as a key factor impacting concordance, with lower concordance regarding broad functioning for children who are more severely impacted by autism (Hundert et al. 1997; Rapin et al. 1999; Szatmari et al. 1994; Voelker et al. 2000). Overall, the nascent and conflicting nature of this work suggest there is a critical need to better understand the rate of concordance for ratings of child adaptive functioning, especially among informants who are key to the receipt of school based services, namely teachers and caregivers.
The educational system is the primary service system accessed by school-age children with ASD, with as many as 90% of youth with ASD served in public school settings (Brookman-Frazee et al. 2009; U.S. Department of Education 2015). Within school settings, youth access multidisciplinary services (e.g., occupational therapy, speech therapy, mental health) to address their significant and often complex service needs. Currently, schools utilize a variety of assessment approaches and these practices often rely on both parent and teacher informant ratings of child functioning as indicators of both service eligibility and progress. Despite its importance in determining eligibility for and types of school-based services needed, little work to date has examined the concordance in parent and teacher reports within the context of youth receiving ongoing services for ASD in public school settings.
Though the current literature provides a preliminary understanding of informant concordance of ratings of youth with ASD, important gaps remain. As mentioned, the majority of existing data pertain to concordance in informant ratings of symptoms of psychopathology, rather than work focused on child adaptive functioning more broadly. Further, researchers have only recently begun to examine concordance in functioning specifically pertaining to ASD with a need for further studies specifically focusing in this area. These data are also predominantly cross-sectional and drawn from relatively small samples, thereby restricting the ability to speak to patterns of agreement in the larger population, including changes across time. Finally, there is limited consistency in the methodologies used to examine informant concordance, which creates difficulties in interpreting and synthesizing results across studies (De Los Reyes and Kazdin 2005; Youngstrom et al. 2000). This is especially notable in the work examining broad adaptive functioning in youth with ASD, which has primarily relied on mean differences and, to a lesser extent, correlational analyses as indices of informant agreement (see Lane et al. 2013). However, recent theoretical and methodological work within the psychopathology literature points to more rigorous and meaningful methods to examine informant concordance that may provide guidance for further work with youth with ASD. For example, Youngstrom et al. (2000) approach incorporates multiple metrics of concordance, including informant agreement and disagreement that serve to complement one another, with agreement pertaining to whether informants agree on functioning pattern (e.g., higher self-help versus communication abilities) and disagreement pertaining to informants concordance on functioning level (e.g., overall mild versus severely impaired). The use of multiple metrics allows for more rigorous and robust examination of concordance and has been replicated in further investigations of discrepancy (e.g., Fung and Lau 2010; Lau et al. 2004).
The current study seeks to extend the cross informant literature in ASD by examining parent–teacher concordance for ratings of adaptive functioning and ASD-specific symptomatology across time, using multiple metrics in a large sample of youth with ASD receiving school-based services. Specifically, the current study has three aims: (1) to examine the discrepancies between parent and teacher ratings (i.e., disagreement) as well as overall agreement regarding symptom patterns (i.e., agreement); (2) to examine the impact of child characteristics on informant agreement and disagreement; (3) to examine the longitudinal consistency of agreement and disagreement, including the impact of child characteristics in changes over time. We hypothesized that concordance between parent and teacher ratings of child adaptive functioning would be consistent with the moderate rates observed in prior research. We also hypothesized that child characteristics such as ASD severity and child cognitive abilities would significantly impact parent–teacher concordance, consistent with previous research (e.g., Stratis and Lecavalier 2015). Finally, given the paucity of longitudinal literature examining informant agreement over time, this was an exploratory aim.
Methods
Procedures
Data for this project were drawn from a larger effectiveness trial of a school-based intervention for children with ASD. The study took place in a large urban county in Southern California.
Participants
The current sample included data from a subset of 246 children enrolled in the larger effectiveness trial. For child inclusion, criteria included youth receiving school-based, special education services under the primary educational classification of autism, resulting in a total sample of 305 children in the larger study. Children were nested within teachers, with a total of 102 teachers, each reporting on approximately two child participants. Autism diagnoses were confirmed using the Severity Scale of Autism Diagnostic Observation Scale, Second Edition (ADOS-2; Lord et al. 2012; see below), with 99% being classified as Autism or Autism Spectrum. Additional inclusion criteria for this study were corresponding parent and teacher responses for at least one time point with enough data to calculate raw subscale scores for the outcome measures of interest (see below). Data from the larger study not part of the current sample were excluded due to either missing and/or insufficient corresponding teacher or parent data (i.e., questionnaires were not completed or only partially completed by both parents and teachers, impeding raw score calculation), resulting in exclusion of 59 children from the larger study. Differences in demographic and clinical characteristics between children included in the current study and those excluded were examined. Results from these bivariate analyses indicated significantly fewer Hispanic/Latino youth (41.5 versus 76.5%; t(222) = − 2.82, p < .01) were included in the current sample than participated in the larger study overall. Youth in the current sample were on average 5.58 years old at entry into the study (SD 2.38, range 3–12) and 80.5% male. Teacher and parent–child dyad demographics are presented in Table 1.
Measures
Students in the current sample were administered a cognitive assessment and a standardized ASD diagnostic assessment by trained members of the research team when they enrolled in the study at the beginning of the school year (Time 1). Parents reported demographic information upon enrollment. Additionally, parents and teachers completed standardized questionnaires about each child’s behavior at the beginning (Time 1) and end (Time 2) of the school year. The average length of time between Time 1 and Time 2 was 7.15 months (SD 1.35).
Agreement Evaluation Measures
Vineland Adaptive Behavior Scales, Second Edition
The Vineland Adaptive Behavior Scales, Second Edition (VABS-II; Sparrow et al. 2005) measures personal and social skills, has been validated with children with developmental disabilities, and is applicable to children from birth through 18 years, 11 months. Standardization included national samples of children with and without disabilities. The Parent and Teacher Rating forms were utilized. The VABS-II assesses functioning levels in several developmental domains that are consistent across informant ratings forms, including Communication, Socialization, and Motor Skills, which were used in the current study. Inter-rater reliability on the VABS-II has been reported at 0.74 (Sparrow et al. 2005).
Pervasive Developmental Disorder Behavior Inventory
The Pervasive Developmental Disorder—Behavior Inventory (PDD-BI; Cohen et al. 2003) is a rating scale designed to assess symptoms of ASD in children ages 2–12 years old. The Parent and Teacher ratings forms were utilized. The PDD-BI yields five composite scales measuring maladaptive and adaptive behaviors, including the following utilized in this study: repetitive/ritualistic problem (REPRIT), social approach/withdrawal problem (AWP) and receptive/expressive social communication abilities composites (REXSCA). The PDD-BI has good reliability, construct, developmental and criterion-related validity (Cohen et al. 2003).
Student Characterization Measures
Autism Diagnostic Observation Schedule, Second Edition
ASD severity was assessed using the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al. 2012), a standardized protocol for observation of social and communicative behavior associated with ASD. It has been shown to have high reliability and discriminant validity (Lord et al. 2012). The ADOS-2 largely operationalizes the process of informing the diagnosis of ASD. The ADOS-2 was administered in the school setting by project staff trained to research reliability on the measure. This study utilizes the ASD severity score (range 1–10, where 10 is most severe). The severity score can be used for comparison across age ranges (i.e., modules) in addition to indicating ASD severity (Gotham et al. 2009; Lord et al. 2012).
Mullen Scales of Early Learning
Students received the Mullen Scales of Early Learning: AGS Edition (MSEL; Mullen 1995) if they could not achieve a basal on the verbal scale of the Differential Ability Scales. The MSEL is designed for children from birth to 68 months of age. T-scores, percentile ranks, and age equivalents can be computed for five scales separately (Gross Motor, Visual Reception, Fine Motor, Expressive Language, and Receptive Language). For these analyses, we used the Early Learning Composite (ELC; M = 100, SD 15) as an assessment of cognitive functioning. Construct, concurrent, and criterion validity are all verified by independent studies and the technical manual for the MSEL (Mullen 1995).
Differential Ability Scales, Second Edition
Students received the Differential Ability Scales, Second Edition (DAS-II; Elliott 2007) if they were over 68 months of age and functioning at least at the 2 year 6 month level, or over 2 years 6 months of age and reached a ceiling on the MSEL. The DAS is designed for students from 2 years 6 months to 17 years 11 months. The Core Cognitive tasks were administered, which include the Verbal, Nonverbal/Spatial, and Nonverbal (Fluid Reasoning) Subtests. T-scores, percentile ranks, and age equivalents can be computed for each subtest separately. For these analyses, we used the General Conceptual Ability (GCA; M = 100, SD 15) as an assessment of cognitive functioning. Construct, concurrent, and discriminative validity are all verified by independent studies and the technical manual for the DAS (Elliott 2007).
Data Analyses
A common-items approach was used to examine cross-informant agreement and disagreement such that only items and corresponding subscales consistent across parent and teacher measures were included in our analyses. Specifically, the Communication, Social and Motor Composite Scales from the VABS-II and the Repetitive/Ritualistic Problem (REPRIT), Social Approach/Withdrawal Problem (AWP) and Receptive/Expressive Social Communication Abilities (REXSCA) Composite Scales from the PDD-BI were included. Per current recommendations (e.g., De Los Reyes and Kazdin 2005) as well as an existing and increasingly replicated approach (Fung and Lau 2010; Lau et al. 2004; Youngstrom et al. 2000), cross-informant concordance was evaluated using two metrics that serve to complement one another: standardized difference scores and q correlations. Standardized difference scores were used as an index of disagreement and reflect the extent to which informants match reporting on level of functioning (Youngstrom et al. 2000). For the difference scores, raw subscale scores of parent and teacher ratings were first standardized and the standardized parent score was subtracted from the corresponding teacher reported score. A positive standardized difference score indicates teachers endorsed more items than parents whereas a negative difference score indicates the parent endorsed more items than teachers. A difference score of zero indicates cross-informant agreement at the subscale level but not necessarily at the individual item level. As an index of agreement, a Pearson correlation between informants at the subscale levels, interrater q correlations, were used and reflect the extent to which informants agree on overall pattern of functioning. Given the limited number of subscales that comprise the VABS-II Motor Composite, we were unable to calculate a q correlation for this scale.
The goal of the current study was to examine parent–teacher agreement on standardized measures of adaptive behavior (VABS-II) and autism symptomology (PDD-BI), and to identify child characteristics that may impact agreement across informants as well as examine concordance across time. For our initial analyses (Aim 1), we began by examining bivariate correlations between variables of interest and mean differences between parent and teacher ratings using paired t tests. For subsequent analyses (Aim 2), we utilized hierarchical linear regressions to examine the impact of child characteristics on parent–teacher agreement (q correlations) and disagreement (standardized difference scores). Specifically, age and gender were first entered as covariates in all models to account for the use of raw, unnormed data. In separate regression models, relevant predictor variables were subsequently were entered as predictors of agreement and disagreement scores for the subscales of interest at both time points. Finally, to examine change over time (Aim 3), we examined mean differences between disagreement and agreement between time points using paired t tests. We also examined the impact of child characteristics on concordance at Time 2 after controlling for concordance at Time 1.
Results
Aim 1: Preliminary Analyses Examining Agreement
Overall, agreement between parents and teachers on child adaptive behavior and ASD symptomology was moderate, but varied. Results indicated significant mean differences in parent and teacher report across all subscales on the VABS-II at both time points, with consistently higher parent ratings than teachers. For the PDD-BI, there is more variability across subscales, with parents rating their children as being lower functioning in terms of their approach and withdrawal behaviors but higher functioning in terms of their receptive/expressive social communication as compared to teacher ratings. Pearson correlations between parent and teacher reports on corresponding scales of the VABS-II and PDD-BI were in the moderate to high range for both time points (Pearson correlation range .34–.81). When examining concurrent concordance at Time 1 and 2 using paired t tests, teachers and parents also showed significant differences in ratings of child functioning. See Table 2 for full results.
Aim 2: Multivariate Analyses Examining Factors Impacting Concurrent Agreement Across Time
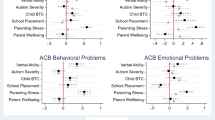
Our results suggest a significant impact of cognitive abilities and ASD severity on parent–teacher concordance that vary by specific area of child functioning and measure. Regression models for the VABS-II indicate that cognitive ability scores were significantly negatively associated with Time 2 standardized differences scores for the social domain, such that higher cognitive ability scores were associated with lower parent–teacher disagreement (β = − 0.23, p < .01). In a similar pattern, cognitive scores were positively associated with q correlations for the social domain across both time points such that higher cognitive functioning was associated with higher agreement (Time 1 β = 0.29, p < .01; Time 2 β = 0.44, p < .01). ASD severity as measured by the ADOS-2 was not significantly related to parent–teacher concordance on the VABS-II. Our results suggest a limited impact of ASD severity but a significant impact of child cognitive abilities on concordance such that increased cognitive abilities were associated with higher parent–teacher concordance (lower disagreement and higher agreement) regarding children’s adaptive behaviors.
For the PDD-BI, there was evidence of a significant impact of cognitive abilities on agreement, with significant negative associations between child cognitive abilities and q correlations for regarding repetitive/ritualistic (β = − 0.25, p < .01) and social approach/withdrawal (β = − 0.19, p < .05) behaviors at Time 2. These results suggest decreases in parent–teacher agreement regarding repetitive/ritualistic and social approach/withdrawal symptoms as cognitive abilities increase and that disagreement may similarly increase as cognitive abilities increase. In terms of ASD severity, ADOS scores were significantly negatively associated with standardized difference scores for social approach/withdrawal behaviors at Time 1 (β = − 0.17, p < .05) such that increased autism severity was associated with decreases in disagreement regarding social approach/withdrawal behaviors. ADOS scores were also negatively associated with q correlations for the receptive/expressive social communication domain (β = − .27, p < .01), such that parents and teachers showed less agreement on the PDD-BI for children with higher ADOS severity scores. Full results are reported in Table 3.
Aim 3: Multivariate Analyses Examining Consistency in Concordance and Factors Impacting Change Across Time
When comparing q correlations (agreement) and standardized difference scores (disagreement) across time points, significant mean differences were observed between standardized differences scores at Time 1 and Time 2 for the VABS-II social domain [t(112) = 2.42, p < .05] and the PDD-BI receptive/expressive social communication domain [t(122) = 3.37, p < .01], with higher mean levels of disagreement at Time 2. No other significant differences were observed for other standardized difference scores or q correlations scores. These results suggest limited changes in parent–teacher concordance over time, with the exception of the social and social communication domains where disagreement increased across time.
Similar to the concurrent findings, results from the longitudinal regression models indicate that cognitive abilities were predictive of q correlations for ratings of social abilities for the VABS-II (β = 0.20, p < .01). Consistent with concurrent results for the PDD-BI, cognitive abilities were predictive of decreases in q correlations for repetitive/ritualistic behaviors (β = − 0.23, p < .01) such that increased cognitive abilities predict lower parent–teacher agreement over time. ASD severity was not significantly predictive of changes in disagreement or agreement for either the VABS-II or PDD-BI. Again, these results suggest that higher levels of cognitive abilities are predictive of changes in concordance between parents and teachers over time. Full results can be found in Table 4.
Discussion
Consistent with our Aim 1 hypotheses, parent–teacher concordance was moderate but variable, with higher agreement (as indicated by q correlations) observed on ratings of communication abilities. The largest disagreements (as indicated by standardized difference scores) were noted for social and receptive/expressive social communication abilities. Across domains, parents consistently rated children higher than teachers, including greater adaptive abilities as well as greater ASD specific impairments than teachers. In terms of Aim 2, parent–teacher concordance was impacted by child characteristics, namely ASD severity and cognitive abilities. Specifically, higher ASD severity was associated with higher concordance regarding social approach/withdrawal behaviors and lower concordance regarding receptive/expressive social communication abilities. Higher cognitive abilities were associated with higher concordance regarding adaptive behaviors such as social abilities but lower concordance regarding ASD-specific behaviors, including restrictive/ritualistic and social approach/withdrawal behaviors. Finally in terms of Aim 3, parent–teacher agreement and disagreement was generally consistent across time. Similar to Aim 2, cognitive abilities were predictive of increased agreement regarding social abilities but lower agreement regarding repetitive and restrictive behaviors over time.
Overall, our Aim 1 findings are consistent with the broader literature suggesting moderate inter-rater agreement that varies as a function of specific domain, with lower agreement observed for adaptive or social skills versus psychiatric symptoms (McDonald et al. 2016; Stratis and Lecavalier 2015). Specifically, our current results mirror those of McDonald et al. (2016) noting low-to-moderate agreement on adaptive skills, with significant variability across constituent domains of adaptive skills. Contextual variations common to cross-informant ratings may also account for these differences (Kanne et al. 2009; De Los Reyes et al. 2015). Specifically, the lower agreement noted with social skills versus communication abilities may stem from parents and teachers generally having limited overlap in reference for reporting on social skills, with teachers likely having larger opportunity to observe social interactions in the classroom compared to parents. Indeed, these findings support the conclusion of Murray et al. (2009) that contextual factors significantly contributed to their variable pattern in parent–teacher ratings of specific social skills.
The higher parent ratings regarding ASD symptomatology observed in this study is consistent with several previous studies suggesting that parents tend to rate children’s autism symptomatology and challenging behaviors as more impaired (Foley Nicpon et al. 2010; Kessler et al. 2005; Lopata et al. 2016; Murray et al. 2009; Posserud et al. 2006; Stadnick et al. 2017). However, our finding that parents reported higher ratings of adaptive behaviors is inconsistent with prior work (Lane et al. 2013; McDonald et al. 2016; Szatmari et al. 1994; Voelker et al. 2000). Further examination of this literature reveals that the much of this work failed to examine key factors known to impact informant ratings. Our results add the larger literature underscoring the importance of examining factors such as child characteristics when interpreting informant reports. Additionally, our results support data suggesting that there is variability across domains in which parents rate children as more impaired. In particular, data suggest that teachers rate children as more socially impaired (Jepsen et al. 2012) and that parents tend to under report social deficits (Overton et al. 2007). Together, these findings underscore the importance of considering specific domains of interest as well as moderating factors such as child characteristics when interpreting cross-informant reports.
In terms of the effect of child characteristics, our Aim 2 and 3 findings suggest a differential impact of cognitive abilities on concordance, with a negative impact on ratings of ASD symptomatology and a positive impact on ratings of adaptive behaviors. A potential explanation for these findings is that adaptive abilities are easier to assess among youth who are higher functioning and likely have more salient communicative and social abilities, whereas ASD specific symptomatology may be more nuanced or subtle among these youth, making it more difficult for parents and teachers to agree upon. Interestingly, this pattern of findings is consistent with the broader literature noting decreased agreement across informants regarding more subtle symptoms such as internalizing symptoms compared to more observable or severe externalizing symptoms (see Stratis and Lecavalier 2015).
We observed a similar pattern across measures with ASD severity such that there was evidence of higher concordance for ratings of social approach/withdrawal behaviors but lower concordance for receptive/expressive social communication behaviors for youth with more severe ASD symptomatology. These findings are somewhat inconsistent with findings noting generally higher agreement for youth who are more severely affected by autism (Rapin et al. 1999; Szatmari et al. 1994; Voelker et al. 2000). However, and as is the case with cognitive abilities, it may be that social approach behaviors are more overt and therefore easier to for informants to agree on compared to receptive/expressive social communication abilities which may be more subtle and thus more difficult to see agreement across informants. Across analyses, we controlled for the impact of gender and age on concordance. Our results suggest that age had a limited impact on concordance, specifically agreement on repetitive behaviors and communication abilities. The limited impact of age aligns with prior research supporting a variable impact of age on concordance (see Stratis and Lecavalier 2015). Interestingly, the addition of ASD severity and cognitive ability to our regression models resulted in additional variance accounted for by our models, thereby suggesting an additional and possibly more prominent impact of ASD severity and cognitive ability.
The issue of context is important to consider when interpreting these findings. Many of the receptive/expressive social communication abilities queried on these assessments are often very context specific. Therefore, differences in opportunities for interaction or structure at school compared to home may contribute to variable demonstrations of social communication abilities among highly impacted children, thereby resulting in lower concordance between teachers and parents. For example, a parent may use a child’s interaction with his siblings or cousins, whom he or she is likely to be more familiar with, as a reference point to answer questions regarding social skills, whereas a teacher can draw from the broader and likely less-controlled context of seeing the child interact on the playground. For higher functioning children, these abilities may more easily generalize across settings. In addition to data suggesting variable rating pattern for specific social skills (Murray et al. 2009), this notion is supported by findings suggesting that the influence of ASD severity is context specific, where severity impacts teacher’s but not parent’s ratings of children’s social skills (Azad et al. 2015). In sum, these findings add to the broader literature recommending ongoing consideration of key child characteristics when integrating informant report. For school professionals making treatment determination and progress evaluations, this may involve ongoing assessment and incorporation of child cognitive abilities or autism severity into treatment decisions.
Finally, the limited changes in parent–teacher concordance over time (Aim 3) support the growing consensus that informant differences likely map onto meaningful behavioral differences across contexts (De Los Reyes et al. 2015; Dirks et al. 2012). That is, the stability seen over time in informant ratings reflect the importance of considering context when understanding and characterizing children’s behavior. In this sense, these differences may actually be clinically meaningful versus simply a bias that should be minimized (e.g., Bennett et al. 2010). As Dirks et al. (2012) suggest, incorporation of the contextual factors would greatly inform ongoing treatment planning or progress monitoring. For example, and as our data suggest, it may be important to incorporate treatment goals centered around improving the generalization of social approach or social communication skills across settings, especially among youth with more severe ASD specific symptoms or higher cognitive abilities. Similarly, efforts to examine, identify and communicate the unique contextual factors (e.g., variability in environmental structure, individual versus group settings) resulting in these meaningful differences may also be key treatment considerations in promoting behavior generalization. Increased parent–teacher collaboration, including ongoing discussion of observations of child functioning and factors contributing to behaviors across settings, may be especially clinically meaningful in order increase the incorporation of contextual differences into practice.
The current study has several strengths that extend the broader literature. This study represents one of the first to utilize multiple rigorous and meaningful methods of examining cross-informant evaluations of child functioning among a large, diverse sample of youth with ASD, including adaptive functioning and ASD-specific symptomatology. Additionally, our data are unique in that they speak to a longitudinal pattern of parent–teacher concordance and include an examination of how identified child characteristics impact this concordance over time. This type of evaluation is key to ongoing efforts to improve assessment of child functioning and progress that may serve to improve provision of services for these clinically complex and challenging youth. However, several limitations and considerations when interpreting findings of the current study should be noted. Our inclusion criteria required children have corresponding parent and teacher responses and may have resulted in a selective sample that is not truly representative of the broader population. That is, our sample may include youth who may have more involved or engaged caregivers and/or teachers given their willingness to participate in a multi-year, longitudinal study. Additionally, the time elapsed between Time 1 and 2 (M = 7.15, SD 1.35) may be related to our current results, with more immediate or protracted time frame resulting in a different pattern of concordance. Thus, the time between measures used in evaluation of concordance should be considered. Given the current sample, our results only speak to parent–teacher concordance for school-aged youth. As such, patterns of concordance may vary for older youth and/or young adults, where contextual differences or developmental differences (e.g., increased autonomy or time spent away from parents) may serve to further impact cross-informant concordance. However, currently little is known regarding cross-informant concordance for older youth or young adults with ASD. Finally, we did not include a comparison group of children without ASD receiving school-based services to examine whether our current pattern of results generalize to other populations, including youth with other developmental disabilities.
Overall, the findings from the current study have important implications for ongoing assessment and treatment of youth with ASD. Specifically, our results underscore the importance of including cross-informant reports in understanding general child functioning. These data also expand upon the current literature by highlighting the significant impact of child characteristics such as ASD severity and cognitive abilities as well as demonstrating the importance of considering contextual influences when interpreting informant concordance. Further exploration into the impact of contextual differences on informant ratings, including whether incorporation of these contextual factors contribute to more meaningful treatment goals or outcomes, is needed. Finally, efforts examining how to best handle cross-informant differences and providing guidance for community providers tasked with synthesizing and incorporating these data and making key treatment decisions are critical to improve outcomes for this growing population of youth.
References
Achenbach, T. M., Krukowski, R. A., Dumenci, L., & Ivanova, M. Y. (2005). Assessment of adult psychopathology: Meta-analyses and implications of cross-informant correlations. Psychological Bulletin, 131(3), 361–382. https://doi.org/10.1037/0033-2909.131.3.361.
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101(2), 213–232. https://doi.org/10.1037/0033-2909.101.2.213.
Azad, G. F., Reisinger, E., Xie, M., & Mandell, D. S. (2015). Parent and teacher concordance on the social responsiveness scale for children with autism. School Mental Health. https://doi.org/10.1007/s12310-015-9168-6.
Barnhill, G. P., Hagiwara, T., Myles, B. S., Simpson, R. L., Brick, M. L., & Griswold, D. E. (2000). Parent, teacher, and self-report of problem and adaptive behaviors in children and adolescents with Asperger. Diagnostique, 25(2), 147–167. https://doi.org/10.1177/1362361399003003004.
Bennett, T., Szatmari, P., Georgiades, S., Thompson, A., Duku, E., Bryson, S., … Zwaigenbaum, L. (2010). Maternal depression appears to influence reporting of offspring autism symptoms. Comprehensive Psychiatry, 51(6), e2.
Brookman-Frazee, L., Baker-Ericzén, M., Stahmer, A., Mandell, D. S., Haine, R. A., & Hough, R. L. (2009). Involvement of youths with autism spectrum disorders or intellectual disabilities in multiple public service systems. Journal of Mental Health Research in Intellectual Disability, 2(3), 201–219. https://doi.org/10.1080/19315860902741542.Involvement.
Cidav, Z., Lawer, L., Marcus, S., & Mandell, D. S. (2013). Age-related variation in health service use and associated expenditures among children with autism. Journal of Autism and Developmental Disorders, 43(4), 924–931. https://doi.org/10.1007/s10803-012-1637-2l.
Clark, B. G., Magill-Evans, J. E., & Koning, C. J. (2014). Youth with autism spectrum disorders: Self- and proxy-reported quality of life and adaptive functioning. Focus on Autism and Other Developmental Disabilities, 30(1), 57–64. https://doi.org/10.1177/1088357614522289.
Cohen, I. I. L., Schmidt-Lackner, S., Romanczyk, R., & Sudhalter, V. (2003). The PDD Behavior Inventory: A rating scale for assessing response to intervention in children with pervasive developmental disorder. Journal of Autism and Developmental Disorders, 33(1), 31–45. https://doi.org/10.1023/A:1022226403878.
De Los Reyes, A., Augenstein, T. M., Wang, M., Thomas, S. A., Drabick, D. A. G., Burgers, D. E., … Rabinowitz, J. (2015). The validity of the multi-Informant approach to assessing child and adolescent mental health. Psychological Bulletin, 141(4), 858–900. https://doi.org/10.1037/a0038498.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131(4), 483–509. https://doi.org/10.1037/0033-2909.131.4.483.
Dirks, M. A., De Los Reyes, A., Briggs-gowan, M., Cella, D., & Wakschlag, L. S. (2012). Embracing not erasing contextual variability in children’s behaviour. Journal of Child Psychology and Psychiatry, 53(5), 558–574. https://doi.org/10.1111/j.1469-7610.2012.02537.x.Embracing.
Elliott, C. D. (2007). Differential ability scales (Second). San Antonio: Harcourt Assessment.
Foley Nicpon, M., Doobay, A. F., & Assouline, S. G. (2010). Parent, teacher, and self perceptions of psychosocial functioning in intellectually gifted children and adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(8), 1028–1038. https://doi.org/10.1007/s10803-010-0952-8.
Fung, J. J., & Lau, A. S. (2010). Factors associated with parent-child (dis)agreement on child behavior and parenting problems in Chinese immigrant families. Journal of Clinical Child and Adolescent Psychology, 39(3), 314–327. https://doi.org/10.1080/15374411003691693.
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(5), 693–705. https://doi.org/10.1007/s10803-008-0674-3.
Hundert, J., Morrison, L., Mahoney, W., & Vernon, M. L. (1997). Parent and teacher assessments of the developmental status of children with severe, mild/moderate, or no developmental disabilities. Topics in Early Childhood Special Education, 17(4), 419–434.
Jepsen, M. I., Gray, K. M., & Taffe, J. R. (2012). Agreement in multi-informant assessment of behaviour and emotional problems and social functioning in adolescents with autistic and Asperger’s disorder. Research in Autism Spectrum Disorders, 6(3), 1091–1098. https://doi.org/10.1016/j.rasd.2012.02.008.
Kanne, S. M., Abbacchi, A. M., & Constantino, J. N. (2009). Multi-informant ratings of psychiatric symptom severity in children with autism spectrum disorders: The importance of environmental context. Journal of Autism & Developmental Disorders, 39(6), 856–864. https://doi.org/10.1007/s10803-009-0694-7.
Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 617–627. https://doi.org/10.1001/archpsyc.62.6.617.
Kraemer, H. C., Measelle, J., Ablow, J. C., Essex, M. J., Boyce, W. T., & Kupfer, D. (2003). A new approach to integrating data from multiple sources in psychiatric assessments and research: Mixing and matching contexts and perspectives. American Journal of Psychiatry, 160, 1566–1577. https://doi.org/10.1176/appi.ajp.160.9.1566.
Lane, B. R., Paynter, J., & Sharman, R. (2013). Parent and teacher ratings of adaptive and challenging behaviours in young children with autism spectrum disorders. Research in Autism Spectrum Disorders, 7(10), 1196–1203. https://doi.org/10.1016/j.rasd.2013.07.011.
Lau, A. S., Garland, A. F., Yeh, M., McCabe, K. M., Wood, P. A., & Hough, R. L. (2004). Race/ethnicity and inter-informant agreement in assessing adolescent psychopathology. Journal of Emotional and Behavioral Disorders, 12(3), 145–156. https://doi.org/10.1177/10634266040120030201.
Lopata, C., Donnelly, J., Jordan, A., & Thomeer, M. (2016). Brief Report: Parent-teacher discrepancies on the developmental social disorders scale (BASC-2) in the assessment of high-functioning children with ASD. Journal of Autism and Developmental Disabilities, 46(9), 3183–3189. https://doi.org/10.1007/s10803-016-2851-0.
Lord, C., DiLavore, M., Risi, P. C., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule (second) edition. Torrance, CA: Western Psychological Services.
Mash, E. J., & Hunsley, J. (2005). Evidence-based assessment of child and adolescent disorders: Issues and challenges. Journal of Clinical Child & Adolescent Psychology, 34(3), 362–379. https://doi.org/10.1207/s15374424jccp3403_1.
McDonald, C. A., Lopata, C., Donnelly, J. P., Thomeer, M. L., Rodgers, J. D., & Jordan, A. K. (2016). Informant discrepancies in externalizing and internalizing symptoms and adaptive skills of high-functioning children with autism spectrum disorder. School Psychology Quarterly, 31(4), 467–477. https://doi.org/10.1037/spq0000150.
Mullen, E. (1995). Mullen Scales of Early Learning. Circle Pines, MN: AGS Publishing.
Murray, D. S., Ruble, L. a, Willis, H., & Molloy, C. a. (2009). Parent and teacher report of social skills in children with autism spectrum disorders. Language, Speech, and Hearing Services in Schools, 40(2), 109–115. https://doi.org/10.1044/0161-1461(2008/07-0089).
National Resource Council. (2001). Educating children with autism. In C. Lord & J. P. McGee (Eds.). Washington, DC: National Research Council: Division of Behavioral and Social Sciences. Retrieved from https://scholar.google.com/scholar?q=National+Research+Council+Educating+children+with+autism&btnG=&hl=en&as_sdt=0%2C5.
Overton, T., Fielding, C., & De Alba, R. G. (2007). Differential diagnosis of Hispanic children referred for autism spectrum disorders: Complex issues. Journal of Autism and Developmental Disorders, 37(10), 1996–2007. https://doi.org/10.1007/s10803-006-0349-x.
Ozonoff, S., Goodlin-Jones, B., & Solomon, M. (2005). Evidence-based assesment of autism spectrum disorders in children and adolescents. Journal of Clinical Child & Adolescent Psychology, 34(3), 559–568. https://doi.org/10.1207/s15374424jccp3403.
Posserud, M. B., Lundervold, A. J., & Gillberg, C. (2006). Autistic features in a total population of 7-9-year-old children assessed by the ASSQ (Autism Spectrum Screening Questionnaire). Journal of Child Psychology and Psychiatry and Allied Disciplines, 47(2), 167–175. https://doi.org/10.1111/j.1469-7610.2005.01462.x.
Rapin, I., Steinberg, M., & Waterhouse, L. (1999). Consistency in the ratings of behaviors of communicatively impaired autistic and non-autistic preschool children. European Child and Adolescent Psychiatry, 8(3), 214–224. https://doi.org/10.1007/s007870050132.
Sparrow, S., Balla, D., & Cicchetti, D. (1984). Vineland adaptive behavior scales. In C. Pines (Ed.). American Guidance Service.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland adaptive behavior scales: (Vineland II), survey interview form/caregiver rating form. Livonia, MN: Pearson Assessments.
Stadnick, N., Chlebowski, C., & Brookman-Frazee, L. (2017). Caregiver-teacher concordance of challenging behaviors in children with autism spectrum disorder served in community mental health settings. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-017-3101-9.
Stratis, E. A., & Lecavalier, L. (2015). Informant agreement for youth with autism spectrum disorder or intellectual disability: A meta-analysis. Journal of Autism and Developmental Disorders, 45(4), 1026–1041. https://doi.org/10.1007/s10803-014-2258-8.
Stratis, E. A., & Lecavalier, L. (2017). Predictors of parent–teacher agreement in youth with autism spectrum disorder and their typically developing siblings. Journal of Autism and Developmental Disorders, 47, 2575–2585. https://doi.org/10.1007/s10803-017-3173-6.
Szatmari, P., Archer, L., Fisman, S., & Streiner, D. L. (1994). Parent and teacher agreement in the assessment of pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(6), 703–717. https://doi.org/10.1007/BF02172281.
Tavernor, L., Barron, E., Rodgers, J., & Mcconachie, H. (2013). Finding out what matters: Validity of quality of life measurement in young people with ASD. Child: Care, Health and Development, 39(4), 592–601. https://doi.org/10.1111/j.1365-2214.2012.01377.x.
U.S. Department of Education. (2015). Chapter 2: Elementary and secondary education enrollments. Retrieved from: https://nces.ed.gov/fastfacts/display.asp?id=84.
Voelker, S. L., Shore, D. L., Lee, C. H., & Szuszkiewicz, T. A. (2000). Congruence in parent and teacher ratings of adaptive behavior of low-functioning children. Journal of Developmental and Physical Disabilities, 12(4), 367–376.
Youngstrom, E., Loeber, R., & Stouthamer-Loeber, M. (2000). Patterns and correlates of agreement between parent, teacher, and male adolescent ratings of externalizing and internalizing problems. Journal of Consulting and Clinical Psychology, 68(6), 1038–1050. https://doi.org/10.1037/0022-006X.68.6.1038.
Acknowledgments
This work was conducted at the Child and Adolescent Services Research Center. This study was supported by the U.S. Department of Education Grant (R324A130349; PI: Aubyn C. Stahmer) and an NIMH Career Development Grant (K01MH109574; PI: Suhrheinrich). Additionally, Drs. Stahmer and Suhrheinrich are investigators with the Implementation Research Institute (IRI), at the George Warren Brown School of Social Work, Washington University in St. Louis, through an award from the NIMH (5R25MH08091607). The authors would like to acknowledge the participating schools, teachers, and families.
Author information
Authors and Affiliations
Contributions
KD participated in data acquisition, performed the statistical analyses, interpretation of the data, and drafted the manuscript. JS participated in the design and coordination of the study, data acquisition, and helped to draft the manuscript. SR participated in the design and coordination of the study, data acquisition, and helped to draft the manuscript. AS conceived of the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare they have no conflicts of interests.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Dickson, K.S., Suhrheinrich, J., Rieth, S.R. et al. Parent and Teacher Concordance of Child Outcomes for Youth with Autism Spectrum Disorder. J Autism Dev Disord 48, 1423–1435 (2018). https://doi.org/10.1007/s10803-017-3382-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-017-3382-z