
Abstract
This study assessed the effectiveness of an attention intervention program (Computerized Progressive Attentional Training; CPAT) in improving academic performance of children with ASD. Fifteen 6–10 year olds with ASD attending a mainstream and a special school were assigned to an experimental (CPAT; n = 8) and active control (computer games; n = 7) group. Children were assessed pre- and post-intervention on measures of behavioural symptoms, cognitive skills and academic performance. The intervention was conducted in school twice a week for 8 weeks. Children in the CPAT group showed cognitive and academic improvements over and above the active control group, while children in both groups showed improvements in behaviour. Results suggest that attention training is a feasible approach to improving academic performance in this population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) or autism is a neurodevelopmental disorder characterized by difficulties in social interaction and communication, repetitive and stereotyped interests and behaviours (American Psychiatric Association 2013). ASD is a heterogeneous disorder with complex aetiology (Mandy and Lai 2016), and although impairments in attention are not found amongst its core symptoms, atypical attention is often linked to autism in research, and even associated with the development of ASD symptoms (Keehn et al. 2013).
Attention Functioning in Autism
Atypical attentional processes have been noted in individuals with autism from early infancy. One such example is sustained attention (i.e. the ability to remain focused on task over time), which was found to be poorer in children and adolescents with autism in comparison to typically developing (TD) controls (Chien et al. 2015, 2014; Murphy et al. 2014). In a behavioural study measuring sustained attention, participants had to report whenever a specific sequence of numbers appeared within a serial visual processing stream (Chien et al. 2015). Differences in sustained attention were apparent in participants with autism as they showed fewer hits and correct rejections and more misses in comparison to TD children within the same IQ range (IQ < 115) (Chien et al. 2015). Similar findings were also reported in a previous study using a continuous performance task (CPT) where children with autism showed worse performance in focused and sustained attention and increased ADHD-like (attentional) symptoms (Chien et al. 2014). Poor performance in sustained attention was also found to be accompanied by reduced brain activation in relevant brain regions in autism compared to controls including lower activation in inferior prefrontal, medial prefrontal, striato-thalamic, and lateral cerebellar regions (Murphy et al. 2014). Even when behavioural differences are not present in sustained attention, brain activation still differs in ASD (Belmonte and Yurgelun-Todd 2003a; Ciesielski et al. 1990; Murphy et al. 2014). While contradicting results were also reported indicating intact sustained attention in ASD (Sanders et al. 2008), this may be attributed to scenarios in which the demand for sustained attention is lower (such as in the context of sustained attention to preferred objects).
Evidence for impaired selective-spatial attention (i.e. the ability to select relevant information and suppress irrelevant stimuli) has also been documented (Burack 1994; Plaisted et al. 1999), with early brain activation differences found for participants with autism (Belmonte and Yurgelun-Todd 2003a; Ciesielski et al. 1990). Belmonte and Yurgelun-Todd (2003a) used functional magnetic resonance imaging (fMRI) while participants performed a task consisting of two oddball streams, presented side-by-side. Participants had to attend to one or the other stream according to target colour. Typically, brain activation patterns represent the locus of spatial attention in such tasks so that activity in ventral visual cortex is enhanced for the attended stream and suppressed for the unattended one (Belmonte and Yurgelun-Todd 2003b). In contrast, brain activation patterns in adults with ASD indicated no spatial attention modulation of ventral visual areas (i.e., there was no enhancement or suppression). This was also accompanied by performance difference where the ASD participants showed reduced selection of targets in the attended stream and reduced compensatory suppression of items in the unattended stream (Belmonte and Yurgelun-Todd 2003a).
Finally, perhaps the most frequently documented attention-related difficulty in autism is in executive control, which is often linked to autism as a primary or secondary deficit (Geurts et al. 2009; Hill 2004; Pennington and Ozonoff 1996). Executive control (EC) comprises a large set of functions such as working memory, set shifting, inhibition, cognitive flexibility, reasoning and planning, all of which are needed for goal-directed behaviours. Specifically, set shifting or flexibility was found to be problematic in children with ASD (Happé et al. 2006; Verte et al. 2006). Cognitive flexibility or set-shifting includes processes such as disengaging attention from stimuli and redirecting it towards different locations. Indeed, atypical disengagement of attention is documented in infants with ASD as early as the first year of life (Elsabbagh et al. 2009; Landry and Bryson 2004; Zwaigenbaum et al. 2005). Inhibition and working memory also appear to be considerably delayed in autistic children in early ages, but may recover when entering adulthood (Luna et al. 2007). While some studies have found no problems in inhibition and working memory in autism (Dawson et al. 2002; Luna et al. 2007; Yerys et al. 2007), increased task complexity and consequently increased demand for executive control tend to bring out such differences. For instance, Rinehart et al. (2002) measured inhibition in children with autism and TD controls using a Stroop-like task. Levels of cognitive load were systematically increased, gradually adding congruency, conditionality and choice to the task. Results showed that only with increased levels of cognitive load the ASD group showed a decrease in performance (Rinehart et al. 2002).
Academic Performance in Autism
Academic attainment may vary considerably across children on the autism spectrum with a substantial percentage showing additional learning disabilities. In fact, in a review of ten empirical studies on the prevalence of learning disabilities among children with autism by Emerson et al. (2010), a very wide range of prevalence rates was reported from 15 to 84%. However, eight out of the ten reviewed studies show a prevalence of comorbidity of autism and learning disabilities of above 40%. Overall, poor performance in a range of academic tests such as maths, reading and writing is well documented in ASD (Keen et al. 2016). Nevertheless, while difficulties in acquiring academic skills are common among individuals with ASD, not all people with autism struggle academically (Estes et al. 2011). Evidence for difficulties in maths for instance, can be accompanied by reports of average performance in individuals with high functioning autism (HFA) and in some cases performance advantage (Chiang and Lin 2007). Reading skills also seem to be heterogeneous, as children with autism can show average reading ability but they may have difficulties in reading comprehension, and variability in results is large from floor to ceiling levels (Nation et al. 2006). Writing skills in HFA are reported to be poor, with frequent writing learning disabilities (Whitby and Mancil 2009).
While attention represents a core cognitive process, critical for the development of a number of skills, its importance in the context of classroom settings and academic attainment is of particular interest. Recent research (Erickson et al. 2015) highlights the importance of selective and sustained attention in supporting learning in a classroom setting since early infancy. In particular, selective attention has been found to play an important role in the development of both literacy and numeracy (Stevens and Bavelier 2012). Furthermore, Stern and Shalev (2013), found that poor performance in reading and reading comprehension was related to difficulties in sustained attention. Yet, another function of attention—executive attention—was linked to children’s ability in maths (Bull and Scerif 2001). Evidence linking difficulties in academic skills to attentional difficulties in ASD come from studies by May et al. (2013, 2015). Specifically, poor maths performance in children with ASD was found to be related to problems in attention switching in a visual search task (May et al. 2013). In a follow-up study, May et al. (2015) also found that attention switching correlated with both maths and reading performance in ASD. In fact, children with autism might show some similarities in learning and attentional profile to children with ADHD (Mayes and Calhoun 2007), and children with learning disabilities (LD) (Calhoun and Mayes 2005). In these studies, all clinical groups (ASD, ADHD, LD) were reported to have difficulties in attention and processing speed, which relate to poor performance in academic tests, particularly writing (Calhoun and Mayes 2005; Mayes and Calhoun 2007).
Thus, the behavioural and brain atypicalities seen in the performance of ASD participants in different attention tasks might not only have implications for the severity of ASD symptoms (Keehn et al. 2013), but also for skills needed in learning new abilities, and academic attainment in school settings. Improvement of these attention skills in ASD is therefore of crucial importance in promoting successful learning for children with ASD in a school environment.
Cognitive Interventions in Autism
A growing number of studies utilising computer-based training programs were carried out with children with autism. These programs typically target specific cognitive functions supporting social interactions such as emotion and face recognition (Golan et al. 2010), language and literacy (Pennington 2010), and social skills (Bernardini et al. 2012). However, attempts at targeting more domain-general processes have also been carried out (Hilton et al. 2014; Vries et al. 2015). Working memory and cognitive flexibility were separately taught using a computerized program in children with ASD (Vries et al. 2015). In this case, marginal post training effects and generalization occurred, with improvements in working memory and near-transfer from working memory training to attention, and cognitive flexibility training showing improvements in flexibility (Vries et al. 2015). Hilton et al. (2014) also tested cognitive training for executive function and motor skills in children with autism, using an exergame (i.e. videogame that uses body movement) and found improvements in working memory, metacognition, strength and agility. While certainly not all prior computer-based intervention studies have proven successful as some failed to generalize to naturalistic settings (e.g. Golan and Baron-Cohen 2006; Wass and Porayska-Pomsta 2014), results tend to be overall positive, showing improvements of trained skills and transfer effects (Bernardini et al. 2012; Golan et al. 2010; Pennington 2010), even when more domain-general processes such as working memory and attention are targeted (Vries et al. 2015). However, thus far comprehensive attempts to train a variety of basic attention functions are sparse, especially when applied in a school setting with the aim to impact academic attainment. One attempt to train cognitive flexibility and executive function in a school setting was carried out by Kenworthy et al. (2014) using the “Unstuck and On Target” (UOT) intervention. Using a behavioural protocol to train executive abilities and flexibility, the researchers found post-training improvements in problem-solving, flexibility, and planning/organizing as well as behaviour in classroom, for children with ASD taking part in the UOT training group, in comparison to a social skills intervention group.
The notion of the potential benefit of attention training is not unique to ASD. Posner and Rothbart (2005) argued that attentional training, through repetition can change brain functionality, and bring generalized improvements not only to the attentional network, but also to intelligence and consequently, academic performance. A computerized attentional training program has been used with children with attention difficulties in a school setting, showing long-term improvements in academic and attention skills (Rabiner et al. 2010). In fact, a number of studies in different populations support the notion that attention can be modified with training (Gagnon and Belleville 2012; Kinnealey et al. 2012; Rabiner et al. 2010; Sampanis et al. 2015; Shalev et al. 2007; Wass et al. 2012).
One attention-training program that has been shown in the past to have generalised training effects in different populations is the Computerised Progressive Attentional Training (CPAT) program developed by Shalev et al. (2007). A study assessing the effectiveness of CPAT for 6–13 year old children with attention deficits resulted in a decreased level of inattention symptoms as well as improved non-trained academic skills (Shalev et al. 2007). Similarly, a study assessing CPAT in sub-acute stroke patients demonstrated improvements in both specific attention functions (particularly sustained attention) and transfer to other cognitive domains, such as language, memory and number skills which were not directly trained (Sampanis et al. 2015). As CPAT attempts to train different attention functions—sustained, selective-spatial and executive attention, all of which could exhibit atypicalities in ASD, it may be particularly appropriate in order to train attention in children with ASD, especially as its previous uses demonstrated transfer across different cognitive domains as well as to non-trained academic skills.
While various intervention programs for ASD have been studied (Bernardini et al. 2012; Golan et al. 2010; Hilton et al. 2014; Pennington 2010; Vries et al. 2015), to our knowledge none of them has specifically targeted attention training in primary-aged children with ASD in a school setting with the aim of improving academic skills. Moreover, there is a growing need of research and interventions developed for and with schools, considering staff and school resources for effective program implementation (Kasari and Smith 2013; Parsons et al. 2013). Therefore, in the present study, the CPAT program developed by Shalev et al. (2007) was carried out in two school settings (mainstream and special education) with children with ASD, in an attempt to evaluate its viability for such population. In particular, we ask whether CPAT is an appropriate program to use with children with ASD and whether any changes triggered by training specific attention functions can transfer to non-trained academic skills and cognition.
Methods
The study took place at two different times over the school years of 2015–2016, in two primary schools in the UK (one mainstream and one special). 15 children (6–10 years old) across the two schools with a diagnosis of ASD took part and were divided into two groups, one undergoing the CPAT intervention and the other engaging in standard computer games (active control; see details below). To measure the effects of attention training, pre- and post-intervention assessments were taken in the two groups which included an intelligence test (Computerized Progressive Matrices, CPM; Raven et al. 2008), academic tests in maths, reading and copying, as well as the Childhood Autism Rating Scale (CARS; Schopler et al. 1980) to measure the severity of autism, and semi-structured interviews with class teachers and teaching assistants (TAs) to get their views on children’s performance. The entire study protocol took 2 months to complete. The intervention protocol and data collection were administered by a principal researcher (PR) and three research assistants (RAs), using personal and school laptops. Pupils were blind in regards of the main purpose of the study, and were all told that playing the computer games may help them improve in school. School staff and parents were told that all children were undergoing a computerized attention training. The possibility of using the CPAT with the active control group was offered to the participating schools following the completion of the study, providing the program as well as training the school staff on its application. Institutional ethical approval for the study was obtained from the Science, Technology, Engineering and Mathematics Ethic Review Committee of the University of Birmingham. Written consent was obtained from parents and/or legal guardians of all participants included in the study.
Participants
Participants were recruited from the two aforementioned schools. All participants had a diagnosis of autism and a statement of special educational needs (SEN) and none of them had an additional diagnosis (such as ADHD). Diagnostic criteria and ASD statements were checked and reviewed before children could take part in the study. A total of 15 children participated in the study, seven from the mainstream school and eight children from the special school (catering only for students with ASD). Pupils from the mainstream school came from different school years (i.e. 6–10 years old: two children in Year 1, one child in Year 3, two in Year 4 and two in Year 5) whereas pupils from the special school all attended the same classroom (i.e. 7–8 years old). In each school setting pupils were assigned either to an active control (computer games; CG) or to a training (CPAT) group. Participants were paired and matched in age (chronological age and cognitive age equivalent from the CPM, Raven et al. 2008) gender and intelligence (from the CPM; Raven et al. 2008) and randomly assigned to active control or training group. Thus, overall the CPAT group was comprised of eight children (two females) and the CG group included seven children (one female, see Table 1) across schools. To eliminate possible bias both groups were treated as intervention groups and this information was conveyed to teachers, parents and participants. One child (female) in the active control group did not participate in the computer games sessions, and instead had education as usual (also missing post-intervention assessments for maths and copying). The age [t(13) = 0.47, p = 0.646], age equivalent [t(13) = − 0.772, p = 0.454] and the non-verbal intelligence [t(13) = − 0.73, p = 0.48] did not differ statistically between the groups.
The Intervention Protocol (CPAT, Shalev et al. 2007)
Attention training was employed using the CPAT, which was developed based on Tsal et al. (2005) four-functions of attention model, which proposes that deficits in attention can be present in four functions within the human brain: sustained attention (responsible for maintaining attention for a prolonged time), selective-spatial attention (focusing on relevant information while ignoring adjacent distracting stimuli), executive attention (solving conflicts, inhibition of irrelevant information) and orienting attention (directing and reorienting attention). In this study, three training tasks from the CPAT protocol were used, each separately focusing on either, sustained, selective-spatial or executive attention. The original orienting task (Shalev et al. 2007) was not included in this study as the task included characters in Hebrew and had proven to be too demanding for children with ADHD of similar age to the sample of the current study (Shalev et al. 2007). However, the function of orienting is included to some extent in both the selective spatial and executive attention training tasks (especially as levels of difficulty increase). Tasks were developed in a fun and interactive manner to be used with children from 6 years of age and above who show difficulties in attention (Shalev et al. 2007).
The first of the three training tasks is The Computerized Continuous Performance Task (CCPT), which was developed to improve the function of sustained attention, that is, to be able to maintain the focus of attention on a given task especially during monotonous activities. The Conjunctive Search Task (CST, based on Treisman and Gelade 1980) was designed to improve selective-spatial attention, and the Shift Stroop-like Task (ST, based on Navon 1977), was designed to improve the function of executive attention and cognitive control. In addition, orienting of attention was trained as a part of the CST, whereby children had to disengage from the distractors and reorient attention towards the target, and also in higher levels within the ST task, when participants had to switch between the global and local levels of the figures (either between or within trials). Snapshots of the tasks are presented in Fig. 1. These training tasks were designed with progressive levels of difficulty which are tuned to the individual performance of the trainee. All the training tasks use easy to understand, displaying visual and auditory feedbacks. The tasks and different levels of difficulty have been previously tested with children with ADHD (Shalev et al. 2007), children with foetal alcohol spectrum disorder (Kerns et al. 2010) and with patients after stroke (Sampanis et al. 2015). In all these different clinical groups the CPAT program produced positive outcomes.

Example of displays from the three tasks from the CPAT. To the left, the Shift Stroop-like task (executive attention): in this task, participants were instructed to look for the large (global) smiley face (level 1) pressing the keyboard letter L if it was present, and A when it was abstent. In level 2, participants had to attend to the small (local) smiley faces, and in advanced leves they had to switch and attend to both large and small smiley faces, according to pre exposed cues. Middle: Conjunctive Search Task (selective attention). In this task participants had to decide if the display contained a target (red smiley boy), pressing L if present and A if target was absent (the display depicts level 1 where visual load is still low). Right: The Computerized Continuous Performance Task (sustained attention). In this task, participants had to respond to the appearance of a red car (target) while mantaining focus and inhibiting responses to other appearing objects (level 1). The car was only present in 30% of the trials. In advanced levels participants only had to respond when the car appeared inside a black box, and ignore its appearance anywhere else on the screen
In the present study, participants in the CPAT group had an average of 13 training sessions (12–14) of approximately 45 minutes, twice a week across a 2-month period. Sessions occurred in a distraction-free room, inside the school and were scheduled always at the same time and day of the week, and started as soon as children finished the activity they were working on in the classroom, in the pre-scheduled time set. Experimenters provided one-to-one supervision to each child. Each training task was divided into blocks of different number of trials. The CST and ST had 40 trials per block, while the CCPT had 80 trials per block for low levels of difficulty, or 160 trials for high levels of difficulty. All participants started at the lowest level of difficulty for each training task. Participants then progressed to higher levels of difficulty according to pre-specified criteria within the program, based on maintaining high levels of accuracy and individual improvements in reaction time. The shift between levels of difficulty in each task was automatically controlled by the program. Training sessions had an average of six blocks from the three training tasks (4–9). This number varied according to children’s age and individual differences. Generally, younger children performed fewer blocks per session. Also, each child took a different amount of time to finish blocks, according to their individual speed in responding to the tasks, which led to different number of blocks they could perform in a 45-minute session. In the CST and ST feedback was highly structured and immediate, with an auditory beep for incorrect answers and immediate positive visual feedback appearing on the screen for correct responses with average latency (“very good”) and correct responses showing improvements in reaction time (“excellent”). The CCPT did not show immediate visual positive feedback to maintain high demand of sustained attention. At the end of each block, feedback was translated into points that reflected participants’ performance, including the number of correct and incorrect answers and quantity of positive feedback received (in accordance with Shalev et al. 2007 and; Sampanis et al. 2015).
Active Control Protocol (Computer Games)
For the active control group, three readily available computer games were used: Plants vs. Zombies, Bejewelled 3 and Pacman. Participants in this group took part in a similar number of sessions as the CPAT group (i.e. 13 sessions) which were of the same length, frequency and format as the CPAT group. The control games also had feedback and had different levels of difficulty. Thus, both intervention groups used interactive games with positive feedbacks and rewards (stickers, reward game of their choice at the end of the session), over a 2-month period, twice a week in the mainstream and special school. Importantly, the active control group had the same one-to-one interaction with the experimenters as the training group.
Pre- and Post-intervention Measures
To assess the outcome of the attention training (CPAT) performance was measured in a number of domains (see detailed description below) before and after the intervention for both the CPAT and active control group. These included severity of autism symptoms (CARS), cognitive ability (Raven CPM), and children’s academic performance in maths, reading and copying. The views of the class teaching staff were also captured via semi-structured interviews.
Assessments were carried out between 1 and 2 weeks before and after the intervention, with an average of 3–4 sessions needed for completion of all assessments (with a frequency of two sessions per week). The assessments took place in the same rooms as the intervention (intervention rooms had sometimes to be changed due to limited room availability in schools but alternated between meeting room, library, computer room or empty classrooms). The PR and RAs had individual sessions with each child and were randomly assigned to work with different children to avoid possible bias. Results were compared within and across the training and control groups.
CARS
To assess behavioural symptoms of autism the classroom teachers filled in the Childhood Autism Rating Scale (CARS; Schopler et al. 1980, 1988) for the participating pupils. CARS is a behaviour observation scale where the child’s behaviour is scored against 15 different dimensions, each question corresponding to an ASD symptom. CARS gives a total score measure ranging from non-autistic to severe autism (from a minimum of 15 to a maximum of 60). Each dimension is scored in a scale from 1 to 4. While originally scores below 30 were thought to correspond to the non-autistic range (Schopler et al. 1988), more recent studies point towards a cut-off score of 25 (Chlebowski et al. 2010; Tachimori et al. 2003). Scores above 37 indicate severe autism (Schopler et al. 1988). The reliability has been well documented, showing good internal consistency (alpha = 0.94, n = 537), high inter-rater agreement (correlations ranging from 0.55 to 0.93, M = 0.71, n = 280), and test–retest stability over a 1 year period is 0.88 for the total score (n = 91; Schopler et al. 1988; CARS manual). High concordance between the CARS and the DSM-III-R and DSM-IV diagnostics is also documented (Perry et al. 2005; Bebko et al. 1996).
Raven CPM
The Raven’s—educational: Coloured Progressive Matrices (CPM) was developed to provide brief non-verbal screening measure of general ability. Using a set including visual patterns and shapes, it measures nonverbal skills that involve making meaning out of confusion and the ability to form nonverbal constructs that aid handling complex information (Raven et al. 2008). The test is sensitive to intellectual differences, and demonstrates good test–retest reliability (0.80; Raven et al. 1990). It is regarded as a measure of fluid intelligence, especially for children with learning difficulties and disorders of language ability, such as ASD (Carver 1990; Cotton et al. 2005; Raven et al. 2008).
The CPM consists of 36 items, divided in three sets of 12 each: set A, Aʙ, and B. The sets are formed by visual shapes constituted by different patterns that need to be matched, requiring reasoning by analogy, and the ability to take this as a consistent way of thinking and method of inference for upcoming items (Raven et al. 2008). Children can score a maximum of 36 in the raw score, which is converted into standard score, according to points obtained, and chronological age from normative data. The test also provides percentile ranks and age equivalents. In this study, the PR and RAs administered the CPM individually, prior and after training, following the administration procedure prescribed by Raven et al. (2008), with no time limitations.
Academic Assessment
In order to asses academic performance and the potential impact the intervention has on it, children in both groups completed two series of short tests in maths, reading comprehension and passage copying, one before and one after the intervention program. The tests were the same for all children, prior and post training, and children did not receive any feedback on their performance. The tests were selected from an online database of tests used by schools in the UK. Children had 10 minutes to complete each test, the maths test had a total of 11 questions to be completed, reading comprehension had 17 questions and children had three paragraphs of 143 words in total to copy. These academic assessments were chosen for this study because they are commonly used by schools in the UK, providing high ecological validity. Our objective was to evaluate if performance of children improved within the school, using instruments utilized to measure academic attainment by schools. The academic assessments were timed to closely match tests in a school environment, as many aspects of academic performance are also timed in schools (e.g. time to finish tests and complete activities). The tests scores were converted into accuracy rates (percentage correct out of total number of questions) and the copying was scored using the number of words written per minute (total number of words divided by the time provided).
Semi-structured Interviews
Four different class teachers and two TAs took part in individual semi-structured interviews (three class teachers from different classrooms from the mainstream school, one class teacher and two TAs from the same classroom from the special school, see Table 2). The interviews were carried out at the same time as the pre- and post-intervention assessments. Teachers and TAs were asked about social, academic and personal performance of children participating in the project, as well as attention skills prior and after the training program. All interviewees were blinded to the existence of a control group, and were told that the pupils who participated in the research project would go through a computerised training on attention skills.
Prior to the start of the study, it was briefly explained to them what the project consisted of (i.e. rationale, duration and timeline). They were asked about their expectations from the project and asked to describe how they perceived the children in school: social aspects, personal skills, academic performance, attention and concentration in class. The same questions about the children were asked a week after the end of training (see Appendix 1 for a blank copy of the interview schedule). Interviews were recorded using an audio recorder and additional written notes were kept. Written consents were obtained for the audio recordings.
Data Analysis
A two-way repeated measures ANOVA using time (pre vs post) as within subject factor and group (training vs control) as between subjects factor was used to analyse pre and post data. Significance level was set at p < 0.05. Effect sizes are reported as partial eta squared \((\text{n}_{\text{p}}^{2})\) for ANOVAs and Cohen’s d (same group size) or Hedges g (different group size) for t-tests. For Raven CPM (which is a standardised measure) we also conducted an analysis of the reliability of the change following the intervention using Reliable Change Indices (RCI; Jacobson and Truax 1991). All data are reported as mean ± standard error of the mean (across subjects) (SEM). CARS was reported using total scores; Raven CPM was reported and analysed using standard scores; maths and reading were reported in accuracy (percentage correct out of total questions); copying was reported and analysed using copying rate (the average number of words copied per minute). The qualitative data from the interviews were analysed using thematic analysis (Braun and Clark 2006). Thematic analysis is a widely used method to identify, analyse and report patterns in qualitative data, organising and describing the data in detail, providing flexibility for interpretation of many aspects of the research (Braun and Clark 2006). This study utilized both quantitative and qualitative data, although the qualitative data were analysed using a Chi square test of independence to verify significant differences between the groups. This decision was taken as a mixed method analysis combining quantitative and qualitative data is considered ideal in order to come to conclusions about human behaviour and effectiveness of interventions, complementing and enhancing the credibility of the research findings (Hesse-Biber 2010).
Results
Baseline Measures
Scores were distributed normally in all pre and post measures, apart from the maths pre-test (Shapiro–Wilk; control group: p = 0.039; CPAT group: p = 0.044). Importantly, the groups did not significantly differ in any of the assessments prior to the commencement of the intervention (Table 3: CPM: t(13) = − 0.730, p = 0.48, g s = 0.35; maths accuracy: t(13) = − 1.14, p = 0.27, g s = 0.56; reading accuracy: t(13) = − 0.78, p = 0.45, g s = − 0.38; copying rate: t(13) = − 1.40, p = 0.18, g s = 0.68; CARS: t(13) = 1.02, p = 0.32, g s = − 0.5). Mean and SEMs of the measures are presented by group in Table 3.
School membership (whether children were attending the mainstream or the special school) also did not affect pre-intervention baseline measures (CPM: t(13) = − 0.01, p = 0.99; maths: t(13) = 1.39, p = 0.19, reading: t(13) = 0.97, p = 0.35 or copying: t(13) = − 0.13, p = 0.99), although CARS scores were higher in the mainstream (33.07 ± 2.06) in comparison to the special school (26.62 ± 1.01; t(13) = 2.92, p = 0.012).
Pre Versus Post Intervention Analyses
CPM Standard Score
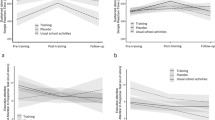
CPM scores varied in our sample, ranging from extremely low to average, high average and superior, in both control and training groups. All children from both groups completed all of the CPM test questions on both pre- and post-intervention assessments. A two-way ANOVA was carried on CPM scores with time (pre vs. post training) as a within subject factor and group (CPAT vs. CG) as a between subject factor. There was a main effect of time [F(1,13) = 7.08, p = 0.020, \({\text{n}}_{{\text{p}}}^{2}\) = 0.353], where pre CPM scores were significantly lower (89.55 ± 4.53) in comparison to the post CPM scores (97.5 ± 5.17). The interaction between group and time was marginally significant [F(1,13) = 3.78, p = 0.074, \({\text{n}}_{{\text{p}}}^{2}\) = 0.225]. Further analysis of simple effects revealed a significant increase in the CPM scores from pre to post assessment for the CPAT group (pre = 86.25 ± 6.73; post = 100 ± 5.98; t(7) = − 3.67, p = 0.008, Cohen’s d = − 1.32), but not for the CG group (pre = 92.86 ± 5.86; post = 95 ± 8.72; t(6) = − 0.45, p = 0.67, Cohen’s d = 0.011; see Fig. 2a). To further assess the likelihood of change in this measure following the intervention, we conducted a Reliable Change Indices (RCI) analysis on the CPM scores (Jacobson and Truax 1991). RCI is an appropriate measure for small samples which clinically examines significant improvements at the individual level. 6 out of the 8 children in the CPAT group showed a RCI above the cut-off point of 1.96 (considered to indicate a reliable change), while only two out of seven children from the CG group exhibited a RCI above the cut-off. In addition, one child in the CG group showed a reliable decrease in scores. Individual change from pre to post assessment for each participant is depicted in Fig. 3a. The data shows that while in the control group both improvement and deterioration were recorded, in the CPAT all participants exhibited improvement.

Performance before and after intervention for the CPAT and CG groups. a Standard scores from the cognitive assessment (CPM) for pre- and post-intervention tests, for the CPAT (black) and CG (grey) groups. b Scores (accuracy) from the maths assessment for pre- and post-intervention tests, for the CPAT (black) and CG group (grey). c Scores (accuracy) from the reading assessment for pre- and post-tests, for the training (black) and control group (grey). d Number of copied words per minute (copying rate) from the copying assessment for pre-and post-tests, for the training (black) and control group (grey)

Individual change performance (post minus pre intervention scores) for participants from the CPAT and CG groups. Participants are numbered individually, from 1 to 16. a Change scores for the cognitive assessment (CPM) showing individual performance for the training (CPAT—black) and control groups (CG—grey). b Change scores for the maths assessment, for all participants in the training (CPAT—black) and control (CG—grey) groups. c Individual change scores for the reading assessment, showing all participants in the training (CPAT—black) and control (CG—grey) groups. d Individual change scores for the copying assessment for all participants in the training (CPAT—black) and control (CG—grey) groups
Academic Assessments
Maths
Data analysis was conducted over the percent correct (correctly answered questions out of total test questions) for each participant. One child (CH7) from the control group was excluded from data analysis since she did not perform the test in the post assessment.
A two-way ANOVA was carried on maths accuracy with time (pre vs. post training) as a within subject factor and group (CPAT vs. CG) as a between subject factor. There was a main effect for time [F(1,12) = 13.92, p = 0.003, \({\text{n}}_{{\text{p}}}^{2}\) = 0.537], showing that post-test scores were generally higher than pre-test scores (pre: 38.92 ± 9.17 and post: 53.13 ± 8.92). More importantly, there was a significant interaction between time and group [F(1,12) = 6.43, p = 0.026, \({\text{n}}_{{\text{p}}}^{2}\) = 0.349]. There was a significant improvement in math scores for the CPAT group (pre = 27.8 ± 10.14; post = 51.7 ± 9.98; t(7) = − 4.52, p = 0.003; d = − 1.60), but not for the CG group (pre = 47.4 ± 14.1; post = 54.5 ± 15.8; t(5) = − 0.866, p = 0.426, d = − 0.18; see Fig. 2b). There were no significant differences in the number of attempted answered questions between the pre- and post-tests, and across CPAT and CG group (average of ten questions attempted out of the total 11). Individual change from pre to post assessment for each participant is depicted in Fig. 3b. Again, the data demonstrate that while in the control group both improvement and deterioration were recorded, in the CPAT group all participants showed improvement.
Reading Comprehension
A two-way ANOVA was carried on reading accuracy (% correct out of the total 17 questions in the test) with time (pre vs. post training) as a within subject factor and group (CPAT vs. CG) as a between subject factor. Again, there was a main effect of time [F(1,13) = 8.54, p = 0.012, \({\text{n}}_{{\text{p}}}^{2}\) = 0.397], showing that post training reading scores were generally higher than pre training scores (pre: 35.63 ± 4.74 and post: 47.45 ± 5.15). Again, the interaction between time and group approached significance [F(1,13) = 3.95, p = 0.068, \({\text{n}}_{{\text{p}}}^{2}\) = 0.233]. There was a significant improvement in reading scores for the CPAT group (pre = 39.34 ± 6.19; post = 59.19 ± 5.34;t(7) = − 4.28, p = 0.004, d = − 1.53) but not for the CG group (pre = 31.9 ± 7.3; post = 35.7 ± 9.2;t(6) = − 0.553, p = 0.60, d = − 0.17; see Fig. 2c). Here too, there were no significant differences in attempted answered questions between pre and post assessment between the groups (average of 10 questions answered out of 17). Individual change from pre to post assessment for each participant is depicted in Fig. 3c. The data once again show a variable picture for the control group with both improvements and deteriorations. In contrast, for the CPAT group a more unified picture of improvement emerges.
Copying
Word copying performance was analysed by calculating the copying rate (words copied per minute). One participant (CH7) from the control group was excluded from the analysis, as she did not perform the post intervention assessment of this test. The copying rate was submitted to a two-way ANOVA on number of copied words per minute with time (pre vs post training) as a within subject factor and group (CPAT vs CG) as a between subject factor. There was a main effect of time [F(1,12) = 7.78, p = 0.016, \({\text{n}}_{{\text{p}}}^{2}\) = 0.393], showing that post-training scores were generally higher than pre-training scores (pre: 3.7 ± 0.6 and post: 4.6 ± 0.5). More importantly, there was a significant interaction between time and group [F(1,12) = 11.97, p = 0.005, \({\text{n}}_{{\text{p}}}^{2}\) = 0.499]. For the CPAT group there was a significant improvement in copying rate as a function of time (pre = 2.7 ± 0.46; post = 4.9 ± 0.59; t(7) = − 7.37, p < 0.001; d = − 1.6). In contrast, there was no evidence for improvement in the copying rate for the CG group (pre = 4.6 ± 1.2; post = 4.4 ± 0.9; t(5) = 3.29, p = 0.755; d = 0.09; See Fig. 2d). Individual change from pre to post assessment for each participant is depicted in Fig. 3d. Here again, a similar pattern appears whereby the control group shows both improvements and deteriorations while the CPAT group shows primarily improvement.
CARS
A two-way ANOVA was carried on CARS scores with time (pre vs. post training) as a within subject factor and group (CPAT vs. control) as a between subject factor. There were no significant main effects or interaction for either factor. Thus, as expected, it appears that CARS scores did not differ between the groups [F(1,13) = 1.43, p = 0.252, \({\text{n}}_{{\text{p}}}^{2}\) = 0.1] or the passing of time in general [F(1,13) = 0.71, p = 0.415, \({\text{n}}_{{\text{p}}}^{2}\) = 0.052].
Interviews
A thematic analysis of the pre-intervention interviews shows that before training, teachers reported difficulties in social interactions, learning academic skills and concentration for all children who participated in the study (both for CG and CPAT groups). In the post-intervention interviews for both CG and CPAT groups, teaching staff noted improvements in confidence and independence, increased social interactions and a general improved mood and enthusiasm. In order to investigate potential changes following the intervention, teachers’ and TAs’ accounts were subjected to thematic analysis (Braun and Clarke 2006; interviews were organised and divided in themes covering different topics and patterns, and compared between CPAT and CG groups). Specifically, the common themes were identified and grouped into improvements in: attention, academic and behavioural changes. Quotes from the interviews can be found in Appendix 2.
CPAT Group
Generally, teaching staff perceived children who took part in the CPAT program as showing academic progress in maths and English, and as being able to concentrate in tasks for longer periods of time, requiring less prompting. They were also perceived to be more confident and independent, although this was not unique to the CPAT group. Some teachers and TAs also reported more ‘seeking’ behaviours where children seemed to look more for social interactions following training. Behavioural changes were coded from the post intervention interview transcripts with school staff. Results from the pre- and post-intervention assessments, and fragments from the interviews were organised in recurrent themes (attention, academic and behavioural changes) individually and summarized in Table 4. Some extracts from the interviews can be found in Table 4 but a more detailed account of the staff quotations can be found in Appendix 2.
Control Group
Overall, teaching staff reported positive changes in behaviour, confidence, independence and some progress in academic areas for some of the children in the control group. The same improvements in attention and concentration were not commonly found in the reports from teaching staff for the control group. Quotes from the interviews are listed in Table 5.
As detailed in Tables 4 and 5, the interviews revealed that improvements in academic skills and attention were more frequently reported for participants in the CPAT group, even though all evaluators believed that all children were taking part in an attention-training program. Positive changes were reported in both control and CPAT groups concerning personal skills such as confidence, independence and motivation. To verify this, a Chi square test of independence was performed on the frequency teaching staff reported positive changes in attention, academic performance and behaviour, in order to examine the relation between attention improvements and group (CPAT and CG), academic improvements and group, and behavioural improvements and group. The relation between attention improvement and group was marginally significant, with more reports of improvements in attention within the CPAT group (87.5%, 7 out of 8) in comparison to the CG group (33.3%, 2 out of 6; Pearson Chi-Square χ2 = 4.38, df = 1, p = 0.036; Fisher’s exact test p = 0.091). The relation between academic improvement and group was significant (Pearson Chi-Square χ2 = 7.47, df = 1, p = 0.006; Fisher’s exact test p = 0.015). Children who underwent CPAT training had significantly more reports of improved academic performance (8 out of 8, 100%) in comparison to children in the CG group (2 out of 6, 33.3%). Behaviour improvement was not significantly different between the two groups (p = 1), as teaching reported similar improvements in behaviour in children from both groups. In general, the qualitative data analyses corroborated the pattern that was observed in the quantitative data analyses.
Discussion
Summary
Previous studies have shown that children with ASD are characterized with atypical attention performance, and as attention functioning is thought to be linked to academic performance, in the present study we attempted to train attention in primary-aged children with ASD using a previously developed attention training protocol (CPAT; Shalev et al. 2007). We assessed the potential efficacy of CPAT in improving academic attainment of children with ASD by obtaining measures of non-verbal cognition, academic skills, autistic symptomatology as well as semi-structured interviews with teaching staff before and after the training protocol was employed in two schools (one mainstream and one special). Importantly, the functions we measured were not trained within the intervention protocol, which only included simple visual attention tasks (sustained-, selective-spatial- and executive attention). Furthermore, we also included an active control group of children with ASD that underwent a similar protocol of intervention with readily available computer games, using the same format and the same length and frequency of sessions (as well as a one-to-one interaction with an experimenter). This enabled us to verify that any changes observed following attention training could not be attributed to the mere passage of time and/or to the children involvement in an engaging computer-based activity during the school day. Overall, the data indicated promising comprehensive improvements for the children in the CPAT intervention group, which were over and above any improvements obtained in the control group in attention and academic performance.
Intervention Effect: Quantitative Measures
Particularly, improvements in the CPAT group were evident in a variety of academic tests including maths, reading comprehension and copying speed. Following the CPAT intervention, children with ASD were able to score higher in a time-limited maths test, were more successful in performing a time-limited reading comprehension test and were also able to increase their copying rate (words per minute) of a given text. Furthermore, scores in a non-verbal cognitive assessment (Raven CPM) also improved for the CPAT group following training. Although the small sample size used here should be kept in mind (Button et al. 2013) all of these improvements were either significant or approaching significance at the ANOVA level and all were significant at the simple effects level. This was also supported by an RCI analysis on the cognitive assessment measure where most of the participants in the CPAT group showed indication of a reliable change in performance. Finally, individual change across the different measures appeared to follow a consistent pattern whereby participants in the control group show both improvements and deterioration in performance while the participants in the CPAT group all show improvements across all measures. Thus, our findings give further support to the growing body of interventions utilizing technology in order to improve or teach new skills to children with ASD, including academic, social and cognitive skills (Bernardini et al. 2012; Bosseler and Massaro 2003; Chabani and Hommel 2014; Ganz et al. 2014; Golan et al. 2010; Hetzroni and Shalem 2005; Hilton et al. 2014; Knight et al. 2013; Pennington 2010; Vries et al. 2015).
While clear academic and cognitive improvements were observed following the attention training, we found no evidence of change in autistic symptomatology. Total scores from the CARS did not change from the pre- to post-intervention assessment and remained equivalent across the two groups (CPAT and CG). It is worth noting that the CARS is designed to be used by trained clinicians while in this study it was used by class teachers in the two schools. It was also the case that overall CARS scores were relatively low for children with ASD, even more so in the special school. We hypothesise that this is associated with the fact that non-clinicians were completing the forms and therefore based their report on the relative expression of the behaviours in the participants compared to the rest of the school environment. As such, the teacher from the special school judged the behaviours of the participants in this study relative to other ASD children in the school (possibly with more severe ASD and/or learning disabilities) who may well exhibit more extreme autistic behaviours, which resulted with lower scores compared to the mainstream school. It is also noteworthy that while the CARS is widely used for screening and diagnostic purposes as well as a treatment outcome measure, it was not designed to measure behavioural changes (Aman et al. 2004). It is therefore possible that it is not a sensitive tool for such a purpose. Nevertheless, the lack of change in autistic symptomatology may also be related to the dissociation between attention atypicality in autism and core symptoms (similarly to Eaves and Ho 2004 who did not find any differences in CARS scores post-intervention) so that while attention improvement can benefit academic performance it did not affect autistic symptoms. This differential effect provides further support to the efficiency of the CPAT in improving attention and to its specificity.
Intervention Effect: Qualitative Measures
The academic and cognitive improvements we observed were also reflected in the thematic analysis of the semi-structured interviews we conducted with teachers and TAs in the two participating schools. Teachers and TAs reported improvements in attention and academic performance, which were more frequently reported for children in the CPAT group. Teaching staff evaluations from the interviews match quite closely the academic tests results in maths and English (reading and writing) for both the CPAT and control group (in the CPAT group teaching staff reported consistent academic improvements for all children whereas such improvement was reported only for one-third of the children in the CG group). Teachers also attributed attentional improvements to children from the CPAT but also to children from the CG group (at least to some degree). This may represent a placebo effect as staff in the schools were informed that all children were taking part in an attention training program. Nevertheless, close examination of the interview reports may suggest some degree of improvement in sustained attention for the CPAT group, which is not consistently mentioned for the CG group. For example, behaviours mentioned for children in the CPAT (but not the CG) group include improving concentration in tasks and in the classroom, being able to concentrate for longer periods of time and showing more self-regulation (less prompting needed) when completing routine classroom tasks.
It is also worth noting that the thematic analysis of the interviews did highlight some behavioural changes (albeit in both groups). In particular, teachers and TAs noted that children in both groups seemed more confident, showed high self-esteem and even demonstrated more socially oriented behaviour. Indeed, these behavioural changes may be attributed to the general aspects of the intervention protocol (across both groups); namely, the participation in a special activity with a dedicated member of staff on a regular basis as a tool for engagement and interaction (Blatchford et al. 2009). Interestingly, the indication that children in the study were showing more socially oriented behaviour may point to an improvement in social interactions, but perhaps not substantial enough to be measured by CARS.
Attention Training as a Domain General Approach to Improving Cognition
The improvements found in maths, reading, copying and non-verbal intelligence following the attention training, are in accordance to previous reports using the CPAT with children with ADHD (Shalev et al. 2007), children with foetal alcohol spectrum disorder (Kerns et al. 2010) and adult stroke patients (Sampanis et al. 2015), where trained attention skills showed transfer effects for non-trained skills. When used with children with ADHD and with children with foetal alcohol spectrum disorder, the CPAT brought improvements for non-trained academic skills (reading, maths and copying; Kerns et al. 2010; Shalev et al. 2007). Similarly, when the CPAT intervention was utilised with sub-acute stroke patients, improvements were documented in a range of non-trained cognitive domains (e.g., language, memory and number skills; Sampanis et al. 2015). Our results are also in accordance with findings regarding improvement in school performance following a different computerized attention-training program, when used with TD children (Rabiner et al. 2010). While it is possible that training with CPAT affected speed of processing in general, which then manifested in better performance in timed tests (c.f. Sampanis et al. 2015 for consideration of general improvement in sustained attention) we note that we found no obvious evidence for such an effect here. First, performance tended to improve both in the timed academic tests and in the non-timed cognitive assessment and furthermore, the number of attempted questions per test did not differ before and after the intervention. It is therefore less likely that a general speed of processing change is the sole reason for improved performance in our study. Thus, the improvements we report in academic skills and cognitive ability following attention-training support the notion that cognitive training of attention has direct impact on learning and general cognition, and can therefore transfer beyond the trained attentional skills.
Another important aspect to consider here is the high comorbidity between ADHD and ASD symptoms and diagnosis. In a recent review, Antshel et al. (2016) pointed out behavioural, biological and cognitive overlaps between the disorders, and ADHD tends to be the second most common diagnosis comorbid to ASD after social-anxiety disorder (Simonoff et al. 2008). It is therefore still a possibility that the effect of CPAT intervention we document in our participants with ASD is also mediated by comorbidity with ADHD-like symptoms in our cohort. Indeed, although none of our participants had a diagnosis of ADHD, it is difficult to ascertain whether any attention difficulties CPAT has helped to improve, are primarily associated with ASD or are independent of it.
CPAT as a Feasible Intervention Tool for ASD
Importantly, our findings also support the notion that using CPAT as an intervention within a school setting is feasible. Parsons et al. (2013) and Kasari and Smith (2013) highlighted the importance of the implementation of intervention programs for ASD in real world settings, such as schools. While the CPAT intervention was challenging to implement due to school breaks, children missing classroom time, need of trained staff and private and quiet training rooms, it was still successfully conducted in the two participating schools. Frequent 1 or 2 week breaks took place in both schools (i.e. regular school holidays), which required a break in training sessions. Still, children did not show any major differences in performance on the training sessions after the breaks, indicated by similar number of completed blocks in sessions occurring before and after the break. It is also worth noting that we have found no differences in performance (and outcome) across the mainstream and the special school. This further supports the feasibility of the implementation of CPAT in varied school contexts.
Several further promising points regarding the feasibility and suitability of CPAT for children with ASD in school are worth mentioning. First, all children in the CPAT group were able to increase the number of blocks they completed in each session (from 4 initially to 7–9 blocks ultimately) and second the levels of difficulty they have reached varied from 2 to 6 (most of the children reached the third level of difficulty in all training tasks). This implies that participants were able to perform the training tasks repeatedly and that they improved their performances within the training sessions themselves. Thus, it appears that participants were able to engage with the program in the way intended so that their performance in each level improved before moving on to the next level of difficulty. Importantly, the levels of difficulty participants reached in the current study are not substantially different than previous uses of the CPAT in different populations. Finally, one more important indicator was the fact that no dropouts were recorded in the CPAT groups, and that teachers and TAs reported high motivation in the children when taking part in the training sessions, concomitant to the schools’ active participation in the project and its inclusion in the weekly routine. As such, these indicators suggest a good level of compliance and satisfaction that should be investigated more systematically in future studies.
A related issue is the way this study utilized positive feedback and rewards across the two groups, promoting engagement and motivation for both CPAT and CG groups. Improvements in children’s independence and self-esteem, as well as high motivation to participate in the program were noted by all class teachers and TAs in the interviews with respect to children in both groups. Previous studies utilising CPAT have highlighted the importance of the tight schedule of online feedbacks embedded within the program which helps the participant to associate the effort they make and the impact it has on performance as well as driving motivation (Geurts et al. 2008; Kerns et al. 2010; Shalev et al. 2007). Motivation is an important prerequisite of successful interventions, as motivational incentives tap into reward mechanisms that can aid attentional control (Padmala and Pessoa 2011). Interestingly, in ASD, evidence points to reduced socially-driven motivation, with non-social reward playing a more effective role (Chevallier et al. 2012; Mundy 1995). In our study a combination of social and non-social motivational tools were used, such as on-screen feedbacks and points acquired, verbal praise, reward games and stickers, making it difficult to discern what type of motivational tool was more effective in this population. Nevertheless, high motivation or the type of feedback in itself could not explain improvements found in the training group, as these were similar across the CPAT and the CG groups.
Limitations and Future Directions
It is important to note, however, that the present study investigated a relatively small-sized cohort (eight and seven children for the CPAT and CG, respectively) which may have impacted on the statistical analyses we have carried out. For instance, although no statistical differences were found for the baseline measures across the two groups such differences may in fact be present in our data. Also, long-term effects of training were not investigated. It is therefore imperative that future studies will continue to investigate the feasibility and efficacy of CPAT (or other attention training protocols) in a larger cohort as well as the long-term effects of training. Testing a larger cohort will also enable to identify specific pre-requisites that facilitate improvement. For instance, looking at the individual change data (Fig. 3) may highlight the potential of some participants to improve more than others. It is therefore important to identify the potential causes for these individual differences. Another factor that should be considered is utilizing a double-blind design to avoid any possible bias scoring post-tests as experimenters in this study were aware of the group assignment at the end of training; however, all possible measures were taken to ascertain children from both groups were treated equally. Parents’ evaluations should also be considered for future research, in order to investigate if the effects of training are limited within the school setting or if training and transfer effects are also noted at home. We also recommend that future studies focus on older children (8 years old and above), with no serious behavioural difficulties, as they might benefit more with the CPAT due to the ability to comply with the programme structure and complete more blocks of each task per session.
Conclusion
In conclusion, the results found in this study regarding the application of a computerized progressive attentional training program (CPAT) in schools are promising. Not only in terms of its effective use in both a mainstream and a special school, but also the near- and far-transfer of attention training to academic and non-verbal cognitive performance of children with ASD. At the same time, the program was engaging and motivating for the children, bringing improvements in a personal level for both the CPAT and CG groups due to highly structured routine and use of rewards and positive feedback.
References
Aman, M. G., Novotny, S., Samango-Sprouse, C., Lecavalier, L., Leonard, E., Gadow, K. D., … Chez, M. (2004). Outcome measures for clinical drug trials in autism. CNS Spectrums, 9(1), 36–47.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. (5th edn). Arlington, VA: American Psychiatric Publishing.
Antshel, K. M., Zhang-James, Y., Wagner, K., Ledesma, A., & Faraone, S. V. (2016). An update on the comorbidity of ASD and ADHD: A focus on clinical management. Expert Review of Neurotherapeutics, 16(3), 279–293.
Bebko, J. M., Perry, A., & Bryson, S. E. (1996). Multiple method validation study of facilitated communication: II. Individual differences and subgroup results. Journal of Autism and Developmental Disorders, 26, 19–42.
Belmonte, M. K., & Yurgelun-Todd, D. A. (2003a). Functional anatomy of impaired selective attention and compensatory processing in autism. Cognitive Brain Research, 17(3), 651–664.
Belmonte, M. K., & Yurgelun-Todd, D. A. (2003b). Anatomic dissociation of selective and suppressive processes in visual attention. NeuroImage, 19(1), 180–189.
Bernardini, S., Porayska-Pomsta, K., Smith, T. J., & Avramides, K. (2012). Building autonomous social partners for autistic children. In International Conference on Intelligent Virtual Agents, 46–52. Berlin Heidelberg: Springer.
Blatchford, P., Bassett, P., Brown, P., & Webster, R. (2009). The effect of support staff on pupil engagement and individual attention. British Educational Research Journal, 35(5), 661–686.
Bosseler, A., & Massaro, D. W. (2003). Development and evaluation of a computer-animated tutor for vocabulary and language learning in children with autism. Journal of Autism and Developmental Disorders, 33(6), 653–672.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
Bull, R., & Scerif, G. (2001). Executive functioning as a predictor of children’s mathematics ability: Inhibition, switching, and working memory. Developmental neuropsychology, 19(3), 273–293.
Burack, J. A. (1994). Selective attention deficits in persons with autism: Preliminary evidence of an inefficient attentional lens. Journal of Abnormal Psychology, 103(3), 535.
Button, K. S., Ioannidis, J. P. A., Mokrysz, C., Nosek, B. A., Flint, J., Robinson, E. S. J., & Munafò, M. R. (2013). Power failure: Why small sample size undermines the reliability of neuroscience. Nature Reviews Neuroscience, 14(5), 365–376.
Calhoun, S. L., & Mayes, S. D. (2005). Processing speed in children with clinical disorders. Psychology in the Schools, 42, 333–343.
Carver, R. P. (1990). Intelligence and reading ability in grades 2–12. Intelligence, 1, 449–455.
Chabani, E., & Hommel, B. (2014). Visuospatial processing in children with autism: No evidence for (training-resistant) abnormalities. Journal of Autism and Developmental Disorders, 44(9), 2230–2243.
Chevallier, C., Kohls, G., Troiani, V., Brodkin, E. S., & Schultz, R. T. (2012). The social motivation theory of autism. Trends in Cognitive Sciences, 16(4), 231–239.
Chiang, H. M., & Lin, Y. H. (2007). Mathematical ability of students with Asperger syndrome and high-functioning autism a review of literature. Autism: The International jouRnal of Research and Practice, 11(6), 547–556.
Chien, Y. L., Gau, S. F., Shang, C. Y., Chiu, Y. N., Tsai, W. C., & Wu, Y. Y. (2015). Visual memory and sustained attention impairment in youths with autism spectrum disorders. Psychological Medicine, 45(11), 2263–2273.
Chien, Y. L., Gau, S. S. F., Chiu, Y. N., Tsai, W. C., Shang, C. Y., & Wu, Y. Y. (2014). Impaired sustained attention, focused attention, and vigilance in youths with autistic disorder and Asperger’s disorder. Research in Autism Spectrum Disorders, 8(7), 881–889.
Chlebowski, C., Green, J. A., Barton, M. L., & Fein, D. (2010). Using the childhood autism rating scale to diagnose autism spectrum disorders. Journal of Autism and Developmental Disorders, 40(7), 787–799.
Ciesielski, K. T., Courchesne, E., & Elmasian, R. (1990). Effects of focused selective attention tasks on event-related potentials in autistic and normal individuals. Electroencephalography and Clinical Neurophysiology, 75(3), 207–220.
Cotton, S. M., Kiely, P. M., Crewther, D. P., Thomson, B., Laycock, R., & Crewther, S. G. (2005). A normative and reliability study for the Raven’s Coloured Progressive Matrices for primary school aged children from Victoria, Australia. Personality and Individual Differences, 39(3), 647–659.
Dawson, G., Munson, J., Estes, A., Osterling, J., McPartland, J., Toth, K., & Abbott, R. (2002). Neurocognitive function and joint attention ability in young children with autism spectrum disorder versus developmental delay. Child Development, 73(2), 345–358.
Eaves, L. C., & Ho, H. H. (2004). The very early identification of autism: Outcome to age 41/2–5. Journal of Autism and Developmental Disorders, 34(4), 367–378.
Elsabbagh, M., Volein, A., Holmboe, K., Tucker, L., Csibra, G., Baron-Cohen, S., & Johnson, M. H. (2009). Visual orienting in the early broader autism phenotype: Disengagement and facilitation. Journal of Child Psychology and Psychiatry, 50(5), 637–642.
Emerson, E., Baines, S., Allerton, L., & Welch, V. (2010). Health inequalities and people with learning disabilities in the UK: 2010. Durham: Improving Health & Lives: Learning Disabilities Observatory.
Erickson, L. C., Thiessen, E. D., Godwin, K. E., Dickerson, J. P., & Fisher, A. V. (2015). Endogenously and exogenously driven selective sustained attention: Contributions to learning in kindergarten children. Journal of Experimental Child Psychology, 138, 126–134.
Estes, A., Rivera, V., Bryan, M., Cali, P., & Dawson, G. (2011). Discrepancies between academic achievement and intellectual ability in higher-functioning school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 41(8), 1044–1052.
Gagnon, L. G., & Belleville, S. (2012). Training of attentional control in mild cognitive impairment with executive deficits: Results from a double-blind randomised controlled study. Neuropsychological Rehabilitation, 22(6), 809–835.
Ganz, J. B., Boles, M. B., Goodwyn, F. D., & Flores, M. M. (2014). Efficacy of handheld electronic visual supports to enhance vocabulary in children with ASD. Focus on Autism and Other Developmental Disabilities, 29(1), 3–12.
Geurts, H. M., Corbett, B., & Solomon, M. (2009). The paradox of cognitive flexibility in autism. Trends in Cognitive Sciences, 13(2), 74–82.
Geurts, H. M., Luman, M., & Van Meel, C. S. (2008). What’s in a game: The effect of social motivation on interference control in boys with ADHD and autism spectrum disorders. Journal of Child Psychology and Psychiatry, 49(8), 848–857.
Golan, O., Ashwin, E., Granader, Y., McClintock, S., Day, K., Leggett, V., & Baron-Cohen, S. (2010). Enhancing emotion recognition in children with autism spectrum conditions: An intervention using animated vehicles with real emotional faces. Journal of Autism and Developmental Disorders, 40(3), 269–279.
Golan, O., & Baron-Cohen, S. (2006). Systemizing empathy: Teaching adults with Asperger syndrome or high-functioning autism to recognize complex emotions using interactive multimedia. Development and Psychopathology, 18(2), 591–617.
Happé, F., Booth, R., Charlton, R., & Hughes, C. (2006). Executive function deficits in autism spectrum disorders and attention-deficit/hyperactivity disorder: Examining profiles across domains and ages. Brain and Cognition, 61(1), 25–39.
Hesse-Biber, S. N. (2010). Mixed methods research: Merging theory with practice. New York: Guilford Press.
Hetzroni, O. E., & Shalem, U. (2005). From logos to orthographic symbols: A multilevel fading computer program for teaching nonverbal children with autism. Focus on Autism and Other Developmental Disabilities, 20(4), 201–212.
Hill, E. L. (2004). Executive dysfunction in autism. Trends in Cognitive Sciences, 8(1), 26–32.
Hilton, C. L., Cumpata, K., Klohr, C., Gaetke, S., Artner, A., Johnson, H., & Dobbs, S. (2014). Effects of exergaming on executive function and motor skills in children with autism spectrum disorder: A pilot study. American Journal of Occupational Therapy, 68(1), 57–65.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. Journal of consulting and clinical psychology, 59(1), 12.
Kasari, C., & Smith, T. (2013). Interventions in schools for children with autism spectrum disorder: Methods and recommendations. Autism, 17, 254–267.
Keehn, B., Müller, R. A., & Townsend, J. (2013). Atypical attentional networks and the emergence of autism. Neuroscience & Biobehavioral Reviews, 37(2), 164–183.
Keen, D., Webster, A., & Ridley, G. (2016). How well are children with autism spectrum disorder doing academically at school? An overview of the literature. Autism: The International Journal of Research and Practice, 20(3), 276–294.
Kenworthy, L., Anthony, L. G., Naiman, D. Q., Cannon, L., Wills, M. C., Luong-Tran, C., … Wallace, G. L. (2014). Randomized controlled effectiveness trial of executive function intervention for children on the autism spectrum. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 55(4), 374–383.
Kerns, K. A., MacSween, J., Vander Wekken, S., & Gruppuso, V. (2010). Investigating the efficacy of an attention training programme in children with foetal alcohol spectrum disorder. Developmental neurorehabilitation, 13(6), 413–422.
Kinnealey, M., Pfeiffer, B., Miller, J., Roan, C., Shoener, R., & Ellner, M. L. (2012). Effect of classroom modification on attention and engagement of students with autism or dyspraxia. American Journal of Occupational Therapy, 66(5), 511–519.
Knight, V., McKissick, B. R., & Saunders, A. (2013). A review of technology-based interventions to teach academic skills to students with autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(11), 2628–2648.
Landry, R., & Bryson, S. (2004). Impaired disengagement of attention in young children with autism. Journal of Child Psychology and Psychiatry, 45, 1115–1122.
Luna, B., Doll, S. K., Hegedus, S. J., Minshew, N. J., & Sweeney, J. A. (2007). Maturation of executive function in autism. Biological Psychiatry, 61(4), 474–481.
Mandy, W., & Lai, M. C. (2016). Annual research review: The role of the environment in the developmental psychopathology of autism spectrum condition. Journal of Child Psychology and Psychiatry, 57(3), 271–292.
May, T., Rinehart, N., Wilding, J., & Cornish, K. (2013). The role of attention in the academic attainment of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(9), 2147–2158.
May, T., Rinehart, N. J., Wilding, J., & Cornish, K. (2015). Attention and basic literacy and numeracy in children with autism spectrum disorder: A one-year follow-up study. Research in Autism Spectrum Disorders, 9, 193–201.
Mayes, S. D., & Calhoun, S. L. (2007). Learning, attention, writing, and processing speed in typical children and children with ADHD, autism, anxiety, depression, and oppositional-defiant disorder. Child Neuropsychology, 13(6), 469–493.
Mundy, P. (1995). Joint attention and social emotional approach behaviour in children with autism. Development and Psychopathology, 7(1), 63–82.
Murphy, C. M., Christakou, A., Daly, E. M., Ecker, C., Giampietro, V., Brammer, M., & Rubia, K. (2014). Abnormal functional activation and maturation of fronto-striato-temporal and cerebellar regions during sustained attention in autism spectrum disorder. American Journal of Psychiatry, 171(10), 1107–1116.
Nation, K., Clarke, P., Wright, B., & Williams, C. (2006). Patterns of reading ability in children with autism spectrum disorder. Journal of autism and developmental disorders, 36(7), 911–919.
Navon, D. (1977). Forest before trees: The precedence of global features in visual perception. Cognitive Psychology, 9, 353–383.
Padmala, S., & Pessoa, L. (2011). Reward reduces conflict by enhancing attentional control and biasing visual cortical processing. Journal of cognitive neuroscience, 23(11), 3419–3432.
Parsons, S., Charman, T., Faulkner, R., Ragan, J., Wallace, S., & Wittemeyer, K. (2013). Commentary–bridging the research and practice gap in autism: The importance of creating research partnerships with schools. Autism: The International Journal of Research and Practice, 17(3), 268–280.
Pennington, B. F., & Ozonoff, S. (1996). Executive functions and developmental psychopathology. Journal of Child Psychology and Psychiatry, 37(1), 51–87.
Pennington, R. C. (2010). Computer-assisted instruction for teaching academic skills to students with autism spectrum disorders: A review of literature. Focus on Autism and Other Developmental Disabilities, 25(4), 239–248.
Perry, A., Condillac, R. A., Freeman, N. L., Dunn-Geier, J., & Belair, J. (2005). Multi-site study of the Childhood Autism Rating Scale (CARS) in five clinical groups of young children. Journal of Autism and Developmental Disorders, 35(5), 625–634.
Plaisted, K., Swetteham, J., & Rees, L. (1999). Children with autism show local processing in a divided attention task and global precedence in a selective attention task. Journal of Child Psychology and Psychiatry, 40, 733–742.
Posner, M. I., & Rothbart, M. K. (2005). Influencing brain networks: Implications for education. Trends in Cognitive Sciences, 9, 99–110.
Rabiner, D. L., Murray, D. W., Skinner, A. T., & Malone, P. S. (2010). A randomized trial of two promising computer-based interventions for students with attention difficulties. Journal of abnormal child psychology, 38(1), 131–142.
Raven, J., Raven, J. C., & Court, J. H. (2008). Raven’s Educational: Coloured Progressive Matrices and Crichton Vocabulary Scale Manual. London: NCS Pearson.
Raven, J. C., Court, J. H., & Raven, J. (1990). Section 2: Coloured Progressive Matrices (with US Norms) Manual for the Raven’s Progressive Matrices and Vocabulary Scales. Oxford: Oxford Psychologist Press.
Rinehart, N. J., Bradshaw, J. L., Tonge, B. J., Brereton, A. V., & Bellgrove, M. A. (2002). A neurobehavioral examination of individuals with high-functioning autism and Asperger’s disorder using a fronto-striatal model of dysfunction. Behavioral and Cognitive Neuroscience Reviews, 1(2), 164–177.
Sampanis, D. S., Mevorach, C., Shalev, L., Mohammed, S., & Humphreys, G. W. (2015). Reducing cognitive deficits after stroke through computerized progressive attentional training (CPAT): A pilot study. Physical Medicine and Rehabilitation—International, 2(7), 1058
Sanders, J., Johnson, K. A., Garavan, H., Gill, M., & Gallagher, L. (2008). A review of neuropsychological and neuroimaging research in autistic spectrum disorders: Attention, inhibition and cognitive flexibility. Research in Autism Spectrum Disorders, 2(1), 1–16.
Schopler, E. C., Reichler, R., & Renner, B. (1988). The Childhood Autism Rating Scale (CARS). Los Angeles: Western Psychological Services.
Schopler, E. C., Reichler, R. J., DeVellis, R. F., & Daly, K. (1980). Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). Journal of Autism and Developmental Disorders, 10, 91–103.
Shalev, L., Tsal, Y., & Mevorach, C. (2007). Computerized progressive attentional training (CPAT) program: Effective direct intervention for children with ADHD. Child Neuropsychology, 13(4), 382–388.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929.
Stern, P., & Shalev, L. (2013). The role of sustained attention and display medium in reading comprehension among adolescents with ADHD and without it. Research in Developmental Disabilities, 34(1), 431–439.
Stevens, C., & Bavelier, D. (2012). The role of selective attention on academic foundations: A cognitive neuroscience perspective. Developmental Cognitive Neuroscience, 2, S30-S48.
Tachimori, H., Osada, H., & Kurita, H. (2003). Childhood autism rating scale-Tokyo version for screening pervasive developmental disorders. Psychiatry and Clinical Neuroscience, 57, 113–118.
Treisman, A. M., & Gelade, G. A. (1980). Feature-integration theory of attention. Cognitive Psychology, 12(1), 97–136.
Tsal, Y., Shalev, L., & Mevorach, C. (2005). The diversity of attention deficits in ADHD the prevalence of four cognitive factors in ADHD versus controls. Journal of Learning Disabilities, 38(2), 142–157.
Verte, S., Geurts, H. M., Roeyers, H., Oosterlaan, J., & Sergeant, J. A. (2006). Executive functioning in children with an autism spectrum disorder: Can we differentiate within the spectrum? Journal of Autism and Developmental Disorders, 36(3), 351–372.
Vries, M., Prins, P. J., Schmand, B. A., & Geurts, H. M. (2015). Working memory and cognitive flexibility-training for children with an autism spectrum disorder: A randomized controlled trial. Journal of Child Psychology and Psychiatry, 56(5), 566–576.
Wass, S. V., & Porayska-Pomsta, K. (2014). The uses of cognitive training technologies in the treatment of autism spectrum disorders. Autism: The International Journal Of Research and Practice, 18(8), 851–871.
Wass, S. V., Scerif, G., & Johnson, M. H. (2012). Training attentional control and working memory: Is younger, better? Developmental Review, 32(4), 360–387.
Whitby, P. J. S., & Mancil, G. R. (2009). Academic achievement profiles of children with high functioning autism and Asperger syndrome: A review of the literature. Education and Training in Developmental Disabilities, 44(4), 551–560.
Yerys, B. E., Hepburn, S. L., Pennington, B. F., & Rogers, S. J. (2007). Executive function in preschoolers with autism: Evidence consistent with a secondary deficit. Journal of Autism and Developmental Disorders, 37(6), 1068–1079.
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari, P. (2005). Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience, 23(2), 143–152.
Acknowledgments
We thank the research assistants Anjli Pattni, Marianna Ruiz and Polly Brayfield for their hard work assisting the conduction of the intervention and assessments. Mayra Muller Spaniol was supported by the Coordination for the Improvement of Higher Education Personnel (CAPES; BEX: 2903/13-0).
Funding
This work was conducted during a scholarship supported by the International Cooperation Program CAPES at the University of Birmingham. Financed by CAPES—Brazilian Federal Agency for Support and Evaluation of Graduate Education within the Ministry of Education of Brazil, BEX: 2903/13-0.
Author information
Authors and Affiliations
Contributions
MMS was the principal researcher, participated in the study design, coordination, performed the measurements, performed the statistical analysis, interpretation of the data and drafted the manuscript; LS conceived of the study, participated in the design and interpretation of the data; LK participated in the design and coordination of the study; CM conceived of the study, participated in the design of the study, interpretation of the data and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that there is no conflict of interest.
Research Involving Human Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Appendices
Appendix 1
Interview with Teachers
Preamble
Talk about:
-
Project—aimed at improving basic attentional processes involved in school activities
-
Academic assessment (content they are seeing in class—maths, reading, writing and copying)
-
CARS
-
Preferences for break activities
Pre interview
-
What do you think are their difficulties regarding academic, social, attentional and personal domains?
-
What are your expectations from the training?
Post interview
-
How are they doing academically, socially, personally now?
-
How is their attention in the classroom?
-
Any other comments about the project?
Appendix 2
Quotes from the interviews:
CPAT
“CH11 and CH14 improved in maths, one level up since the beginning of the project” (ST). “CH11 is better at doing tasks, it is easier to get him to work on tasks, and attention has improved” (TA1). “He pays attention to details a lot more” (TA2). “CH14. shows improvement in work boxes, she used to flip, but now seems more attentive and more interested in doing the tasks.” (TA1).
“CH16. still shows some disruptive behaviours, not as much after the project. Making progress in maths, better concentration but still needs some prompting sometimes. Can do more now on his own” (ST). “CH16 has improved; it’s easier to get him to focus in activities” (TA1).
“CH12 has improved concentration and attention skills, he used to get distracted. Maths improved, numbers, English improved, he is progressing really well” (ST). “He is aware of his own behaviour, and is showing better listening skills now” (TA2).
“CH3 is more confident and independent… He does things by himself now. CH3 is showing progress in numeracy, improved focus and concentration but still has good and bad days” (MT1).
“CH1 shows greater academic achievement; more likely to go and talk to people; more focus and attention to the task. More independent and confident, can do tasks on her own and asks questions, better communication and social interactions” (MT2).
“CH5 is concentrating in tasks a bit more, for longer. CH5 is making academic progress; he can concentrate in tasks in class for longer, before it used to be 2 min” (MT3).
“CH6 made some academic progress, just not as much as one could possibly hope for. He’s not quite there yet, so inconsistent, some days are better than others. Lower levels of learning, numbers need to keep going back to adding, taking away, and number recognition. Talks to himself more. Has many social interactions, but always on his terms”. (MT1).
Control
“CH8 is more participative in class, still shows difficulties in doing tasks independently and needs prompting. He is progressing academically in maths but not so much in literacy” (MT3).
“CH4 understands pure maths but has difficulties with shapes and meaning of words and mathematical problems. He is more confident and independent. Shows more stereotyped behaviours, has problems concentrating and still needs prompting to do tasks” (MT1).
“CH9 still needs prompting to pay attention…Same academic performance” (ST). “Attention slips a bit” (TA1). “He gained a lot of confidence, good computer skills, important for life: learning to interact with the computer” (TA2).
“CH10 and CH15 have always been good” (TA1). “CH10 shows good behaviour, progressing in maths, English, good concentration” (ST). “CH15’s behaviour got worse, he is expressing more, communicating more (started to hit). Can concentrate in maths, English not so much, depends on the task needs prompting. Keeps good academic progress not major jump” (ST).
“CH13 improved behaviour in activities, completely different during activities” (TA1). “He can sit and work through tasks but not major progress academically” (ST).
Across Groups
Interestingly, there was a direct comparison between two boys, one from the CPAT and one from the control group, who were from the same classroom, according to MT3: “CH5 is concentrating in tasks a bit more, for longer….CH5 (CPAT) is more focused than CH8 (control). CH8 gets more distracted, still needs prompting and has difficulties in doing tasks independently. CH5 is making academic progress, he can concentrate in tasks in class for longer, before it used to be 2 min”. In particular, TA2 mentioned that all children were showing “smiles on their faces: children have been very enthusiastic to participate” (TA2).
Rights and permissions
About this article

Cite this article
Spaniol, M.M., Shalev, L., Kossyvaki, L. et al. Attention Training in Autism as a Potential Approach to Improving Academic Performance: A School-Based Pilot Study. J Autism Dev Disord 48, 592–610 (2018). https://doi.org/10.1007/s10803-017-3371-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-017-3371-2