
Abstract
This study documents the relation between an autism spectrum disorder (ASD) diagnosis, increases in intervention, and changes in parent–child interaction quality. Information about intervention and observations of interaction were collected before diagnosis and a half year after diagnosis for 79 low-risk toddlers who had screened positive for ASD risk during a well-baby checkup. Children diagnosed with ASD (n = 44) were 2.69 times more likely to increase intervention hours. After ASD diagnosis, the relation between intervention and interaction quality was complex: although increases in intervention and interaction quality were only modestly related, the overall amount of intervention after diagnosis was associated with higher quality interactions. Moreover, lower quality interactions before diagnosis significantly increased the likelihood that intervention would increase post-diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is strong consensus (National Research Council 2001) that early intervention, especially when it targets specific deficits, leads to better outcomes for children with autism spectrum disorder (ASD). This consensus is supported by several studies demonstrating that early intervention can decrease developmental delay (Dawson et al. 2010) and atypical behavior (Boyd et al. 2011; Eikeseth et al. 2007) and increase critical skills including joint engagement (Lawton and Kasari 2012), communication (Kaiser et al. 2000; Landa 2007; Minjarez et al. 2011), symbolic play (Kasari et al. 2006), and imitation (Landa et al. 2011).
Early detection of ASD is an essential prelude to early intervention and especially enrollment in ASD-specific intervention. Fortunately, substantial research now demonstrates that it is possible to screen low risk toddlers in community settings (Robins et al. 2014; Wetherby et al. 2008; Yama et al. 2012) and subsequently diagnose ASD reliably at age two (Lord and Luyster 2006; Woolfenden et al. 2012). However, it is not yet clear whether early diagnosis prompts parents to seek or increase intervention. To date, the literature on early ASD intervention has focused primarily on intervention efficacy, not on whether children’s enrollment in intervention changes after receiving a diagnosis. Retrospective studies sampling large populations of parents using surveys (e.g., Goin-Kochel et al. 2007; Green et al. 2006; Howlin and Moore 1997; Miller et al. 2012) provide a broad picture of interventions—which ones are used, how parents feel about them, etc.—but do not focus on the period just after an early diagnosis. These surveys suggest that parents initially report high levels of stress in reaction to an ASD diagnosis (Howlin and Moore 1997; Keenan et al. 2010) and high variability in how they select and access services after a diagnosis of ASD (Goin-Kochel et al. 2007; Miller et al. 2012). Of particular note are recent findings that often parents find it difficult to enroll in the services recommended by professionals, including early interventions related specifically to ASD (Kogan et al. 2008), especially when income and proximity affect access to specialized services (Irvin et al. 2012; Mandell and Novak 2005).
The current study was designed to take a prospective look at how early diagnosis was associated with increases in early intervention hours and changes in the quality of parent–child interactions. In particular, we sought to gather information about interventions and interactions in a community-based sample in order to position the study within an ecological perspective (Bronfenbrenner and Morris 2007) that retains the complex connections between the child and the multiplicity of influences that shape the early developmental landscape (Adamson et al. 2016). To this end, we recruited parent-toddler dyads from a low-risk, community-based sample who were participating in an ongoing early screening and diagnosis project, selecting dyads with children who screened positive for risk of ASD on the Modified Checklist for Autism in Toddlers, Revised, with Follow-Up (M-CHAT-R/F; Robins et al. 2009) during a well-baby 18- or 24-month pediatric checkup. Our design included three visits for all the participants: a clinical ASD evaluation and two laboratory visits, one just prior to the evaluation and one approximately 6 months after it. The clinical evaluation—offered to all participants in the screening project who were at risk for ASD—concluded with an extensive report containing diagnostic information; about half the toddlers in our study were diagnosed with ASD and half were not, although almost all had notable developmental difficulty. During the laboratory visits, we systematically observed parent–child interaction and parents provided information about the child’s current participation in intervention.
This design allowed us to address two research questions concerning the effects of the early diagnosis of ASD. First, we asked whether parents whose at-risk children received an ASD diagnosis would be more likely to enroll their children in early intervention services than parents whose at-risk children did not receive an ASD diagnosis. We anticipated that overall enrollment in intervention services would almost always be modest both before and a half year after diagnosis and that most toddlers would receive far fewer than the 25 h of combined intervention per week minimum recommended by the National Research Council (NRC 2001; see also Myers and Johnson 2007; National Autism Center 2015). This expectation is in line with the National Early Intervention Longitudinal Study that found that the median amount of time spent weekly in early intervention is only 1.5 h (see Hebbeler et al. 2007). Nevertheless, we expected that many parents who learned that their child is diagnosed with an ASD would promptly seek hours of intervention. In part, this may occur as a direct response to the suggestions they received about targeted services during the child’s diagnostic evaluation. However, we also expect that obtaining targeted services soon after the diagnosis will often be difficult (Kogan et al. 2008), particularly if parents rely solely on public funding. Thus, we hypothesized (hypothesis 1) that receiving an ASD diagnosis after screening would be associated with an increase in intervention hours during the interval between the clinical evaluation and their second laboratory visit. Given that this interval is relatively brief and our expectation that the overall total of intervention hours, even if they increase, will usually be low, we focused primarily on how many hours of intervention a child received rather than the specific type of intervention. However, we did note whether the interventions were specifically tailored to the needs of a child with ASD in order to determine how often children diagnosed with ASD were able to access such interventions shortly after diagnosis.
Second, we asked whether an increase in the amount of early intervention post-diagnosis was associated with positive changes in parent–child communication in the next 6 months. Previous research indicates that ASD has pervasive negative effects on parent–child interactions (Adamson et al. 2012; Sigman and Ruskin 1999). Such early difficulties interacting, especially those that limit a toddler’s joint engagement during interactions, may, as Charman (2004) cogently argued, play a pivotal role in affecting the subsequent development of language and social understanding. However, it remains unclear whether the small increases in interventions that are likely to occur soon after a toddler in a community-based sample is diagnosed with ASD will result in improvements in early interactions, since most studies that report success rely on high-dosage, intensive autism-specific interventions (see Kaiser et al. 2000; Kasari et al. 2006; Landa 2008). Overall, we anticipated that increased intervention relatively soon after diagnosis would be disappointingly infrequent in our community-based sample. However, when increases did occur, even relatively small increases would be associated with modest but measurable positive changes when parents actively pursue and are successful in changing the services that their child is receiving. Thus, we hypothesized (hypothesis 2) that even small increases in intervention may lead to improvements in key aspects of parent–child interactions, leading to discernible if relatively small improvements of the child’s joint engagement during interactions, the parent’s scaffolding of communication, the sustaining of shared topics, and the fluency and connectedness of the parent–child interaction.
Method
Participants
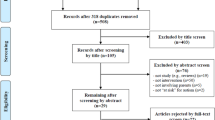
Participants were recruited from one site, metropolitan Atlanta, in an ongoing multi-site project investigating early ASD screening using the M-CHAT(-R)/F (Chlebowski et al. 2013; Robins et al. 2014). At this site, 110 children who screened at-risk on the M-CHAT(-R)/F also participated in our longitudinal study of early communication development. Of these, 79 (49 boys) met our inclusion criteria: two observation sessions completed (27 completed only one), intervention information recorded (two had none), no more than 13 months elapsed between the clinical evaluation and the subsequent observation session (one excluded), and clinical evaluation completed before the second observation (one excluded).
The mean age of the mothers was 34.1 years (SD = 7.1, range = 19.7–55.1). Most mothers had attended some college: only four had not completed high school, 12 had completed high school, 19 had some college or a technical or associate’s degree, 22 had completed college, and 22 had a graduate or professional degree. Of the 79 children, 37 identified as non-Hispanic White, 28 as non-Hispanic Black or African American, three as Asian, five as mixed race or other, and six as Hispanic (one of African descent).
Of the 79 children, 44 (30 boys) were diagnosed with ASD. Diagnoses for the other 35 children (19 boys) included global developmental delay (n = 16, eight boys), developmental language disorder (n = 7, four boys), epilepsy (n = 1, a boy), and visual impairment (n = 1, a girl). In addition, six children (four boys) had concerns that did not lead to a specific clinical diagnosis and four (two boys) were characterized as typically developing.
Procedure
As part of the ASD screening project, all children in the current study were invited for a free clinical ASD evaluation. These evaluations incorporated standardized assessments for developmental disorders including the Mullen Scales of Early Learning (Mullen 1995) and ASD-specific assessments including the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2000) and the Autism Diagnostic Interview-Revised (ADI-R; Le Couteur et al. 2003) or the Toddler ASD Symptom Interview (TASI; Barton et al. 2012); final diagnosis was made by clinical best estimate using all available information from the evaluation session. Parents received an extensive written report containing test results, description of the child’s strengths and weaknesses, diagnosis, and recommendations for intervention and support services. No intervention services were provided to participants as part of this study or any related study.
As part of the early communication study, participants took part in two laboratory visits—the first (T1) occurred just before the evaluation session and the second (T2) approximately a half year thereafter—that included systematic observations of parent–child interaction. Mean ages of the children at these two sessions were 24.1 and 31.9 months (SDs = 3.1 and 2.5), the time from T1 to the evaluation session averaged 0.6 months (SD = 1.0), and the time from the evaluation session to T2 averaged 7.8 months (SD = 2.6).
Assessing Intervention Change Status
Before each session parents completed a form detailing the intervention services their children were receiving. For each service, parents were asked to indicate the type of service, the provider, and the hours per week; at the visit, the research coordinator reviewed the form to ensure that it was complete. Based on this information, we assigned children to either a no-change group or an increased-intervention group. For children in the no-change group, the number of hours per week either increased by less than 1 h (0.125–0.75 h, n = 7), stayed the same (n = 23), or actually decreased (0.125–2 h; n = 9). Hours per week for children in the increased-intervention group increased by exactly 1 h (n = 15) or more than 1 h (n = 25; from 1.5 to 5 h for 13, from 5.5 to 15 h for 9, and from 20 to 45 h for 3). We also coded each service as funded either by a private source or a public source (e.g., the state’s birth-to-three program, Babies Can’t Wait) and whether the service was autism-specific or general. An intervention was considered autism-specific if was explicitly tailored to the developmental needs of children with ASD; in our sample, this included participation in early special education programs specifically designed for young children with ASD in school settings and therapies targeting ASD that were informed by either applied behavior analysis or by Floortime techniques.
Observing the Quality of Parent–Child Interactions
All participants were observed twice with the same parent using the Communication Play Protocol (CPP; Adamson et al. 2001, 2009). Participating in the CPP were 74 mothers, 4 fathers, and 1 grandmother. This protocol produces 30 min of semi-naturalistic observations of interaction in a laboratory playroom during which the parent (as supporting actress) is asked to perform a Communication Play with the child (the star). The Play consists of six 5-min scenes that probe three communicative contexts (social interacting, requesting, and commenting). The CPP is video-recorded using two cameras situated behind one-way mirrors.
Interactions in each of the six CPP scenes were rated using five 7-point Likert scale items that are particularly relevant targets for early interventions for toddlers diagnosed with ASD or with other developmental disorders. The items were designed to span the range of possibilities one might observe in a sample of 18–30-month-old typically developing children as well as samples of young children with developmental difficulties, including ASD (Adamson et al. 2012).
Two items characterized the quantity and quality of the child’s joint engagement so that we could assess how well the child actively sustained attention to a shared activity. One of the items, coordinated joint engagement, focused on the child’s active and repeated coordination of attention both to shared objects and events and the partner, and the second, supported joint engagement, focused on periods during which the child attended to shared objects and events but not also on the partner. A rating of 1 was assigned when there were no episodes of coordinated (or supported) joint engagement during the 5-min scene. The mid-point rating of 4 usually indicated that the child had spent about a third of the scene (or approximately 1½ min total), in coordinated (or supported) joint engagement. However, the sheer amount of time was adjusted by the quality of engagement. For example, a 4 would be selected both if the child spent less than a third of the scene in joint engagement and the quality was very high (e.g., the child eagerly and spontaneously joined in a shared activity), or if the child spent more than a third of the scene in joint engagement and it was of relatively low quality (e.g., the child appeared minimally invested in the shared activity, responding primarily to prompts from the parent). A rating of 7 indicated that the child was frequently engaged in coordinated (or supported) joint engagement and the episodes were richly textured and varied in content.
The rating item parent scaffolding captured how well a partner supports the child’s activities and provides opportunities for learning about shared objects and events and about communicating, including language. A rating of 1 was assigned when the partner provided minimal support for the child’s communication and actions on objects; a mid-point rating of 4 was assigned when the partner provided moderate levels of support; and a rating of 7 was assigned when the partner continually supported and extended the child’s actions.
In addition, two rating items—sustainability of shared topics and fluency and connectedness of the interaction—assessed the quality of the parent–child dyadic exchange. To rate the sustainability of shared topics, the observer attended to how long a dyad focused on a shared topic. A rating of 1 was assigned when shared topics during a scene were fleeting; a mid-point rating of 4 indicated that the dyad maintained topics for a moderate duration (e.g., sustaining a conversation or play for a few turns); and a rating of 7 was given when the dyad sustained topics throughout the scene. The rating item fluency and connectedness assessed the overarching flow and cohesion of the parent–child interaction. Observers attended to the balance between partners’ contributions, how well the partners negotiated shifting the floor, and how smoothly the interaction progressed. A rating of 1 indicated that the dyad did not establish an interaction. The mid-point rating of 4 indicated that interactions were established but they were largely dominated by one partner, lacked smoothness, or were not strongly cohesive. A rating of 7 indicated that parent and child often sustained a fluid and balanced interaction during which exchanges flowed easily and smoothly for several turns with both partners contributing to the progression of their exchange.
Ratings were made by research staff who were trained to apply the rating battery reliably and were blind to the child’s diagnosis, the child’s participation in intervention, and the study’s hypotheses. They were not trained to diagnose ASD and other developmental disorders, and they had not observed the clinical evaluations that were part of the study protocol. The CPP was divided into two 3-scene segments and assigned to an observer who rated all 17 items for a 5-min CPP scene before moving onto another scene. This typically entailed viewing both camera views of the scene three times. To check agreement, at least 15 % of each observer’s corpus was independently rated by a second observer (stratified by diagnostic group; observers did not know which of their sessions were double coded). Agreement was assessed with weighted kappas (Cohen 1968). The range of weighted kappas for ratings within 1 point on the 7-point rating scale was .78–.95, suggesting that observers were about 90 % accurate and often much better (see Bakeman and Quera 2011).
Results
Intervention Hours at T1 and T2
At T1, 38 of the 79 children (48 %) were receiving some intervention (i.e., hours per week > 0); for them, the median was 1.1 h per week and the mean was 2.2 h (SD = 2.4, range = 0.5–13.5). At evaluation, 44 of the 79 children (56 %) received an ASD diagnosis. The children diagnosed with ASD were somewhat more likely to have reported services at T1 than children not diagnosed with ASD (52 % vs. 43 %), but not significantly so: OR = 1.46, 95 % CI [0.60, 3.57], p = .41. By T2, 35 of the 44 diagnosed with ASD (80 %) and 21 of the 35 not diagnosed with ASD (60 %) were receiving services. Of those receiving services at T2, the median was 2.0 h per week for both groups, a non-significant difference (Mann–Whitney p = .88); the mean was higher for the ASD than the non-ASD group (6.3 vs. 4.3 h, SD = 10.3 vs. 5.1, range = 0.75–47 vs. 0.63–19), but this just reflects a positively skewed distribution (e.g., two children with hours in the 40 s in the ASD group).
At T2, as would be expected by definition, all 40 children in the increased-intervention group were receiving services; for them, the median of total hours of intervention was 2.75 h and the mean was 7.1 (SD = 9.9, range = 1.0–47). Comparable statistics for the 16 children in the no-change group receiving services (of 39) were a median of 1.33 h and a mean of 1.7 h (SD = 1.0, range = 0.63–3.5).
Diagnosis and Change in Intervention Hours
Of the 79 children in our study, 40 increased their hours of intervention by at least 1 h from T1 to T2 (51 %). More were in the ASD group: of those who received an ASD diagnosis 27 of 44 increased their hours (61 %), compared to 13 of 35 of those not receiving an ASD diagnosis (37 %); OR = 2.69, 95 % CI [1.08, 6.71], p = .034 (see Fig. 1). Thus, supporting our first hypothesis, the parents in this at-risk sample whose children received an ASD diagnosis at the evaluation visit were 2.69 times more likely to seek increased intervention than parents who did not receive an ASD diagnosis, a moderately sized effect (per Bakeman and Quera 2011, who suggested labeling odds ratios of 1.25–2 weak, 2–3 moderate, and 3 or over strong).

Number of children whose hours of intervention increased by 1 h or more from T1 to T2, separately for children who did, and did not, receive an ASD diagnosis
Intervention Services for Children Diagnosed with ASD
At T1, 21 of the children subsequently diagnosed with ASD were not receiving intervention services (48 %), but at T2, only 9 were not (20 %). Children who were receiving intervention services often received more than one type of therapy: 30 % at T1 and 74 % at T2 (see Table 1 for percentages receiving specific therapies and Fig. 2 for information about the various combinations of services). At both T1 and T2, children were most likely to be enrolled in standard interventions for children with developmental difficulties (DD) with the most likely service being speech therapy (34 % at T1, 57 % at T2) followed by occupational therapy (14 % at T1, 50 % at T2). Only two children were receiving ASD-specific interventions at T1, but 12 were at T2 (including the two from T1). Because ASD-specific interventions are considered optimal for toddlers diagnosed with ASD (Myers and Johnson 2007), Fig. 2 places all children receiving ASD-specific services in one bar; other bars indicate children receiving no services and children who received only standard-DD services. Figure 2 also indicates whether the source of funding for a child’s service was public, private, or a combination of public and private. It is particularly noteworthy that all but one (11 of 12) of the children receiving ASD-specific therapy at T2 were relying in part or totally on private funding, an odds ratio that is more than 20 times greater than the ratio for children who did not receive ASD-specific services (8 of 23 did); OR = 20.6, 95 % CI [2.24, 190], p = .008.

Intervention services received by children diagnosed with ASD grouped by none, standard-DD services, and ASD-specific services at T1 and T2 (due to rounding percentages may not sum exactly to 100 %). ASD ASD-specific, ST speech therapy, OT occupational therapy, PT physical therapy, CI combined intervention, sch school-based services, oth other services, and none no services
Increased Intervention Hours and the Quality of Interaction for Children Diagnosed with ASD
Our second hypothesis concerned whether an increase in intervention hours would affect the quality of parent–child interaction for children diagnosed with ASD. As a preliminary analysis, we asked whether demographic characteristics differed between the no-change and increased-intervention groups. Mothers of children in the increased-intervention group were older: their mean age was 35.4 vs. 31.0 (SD = 6.2 vs. 7.4); t(42) = 2.13, p = .039. Children in the increased-intervention group were somewhat more likely to be female and their mothers were somewhat more likely to have completed college and be non-Hispanic white, but not significantly so; ps = .79, .68, and .25, respectively.
Descriptive statistics for the ASD-diagnosed group for the five CPP rating items of interaction quality are given in Table 2. Mean scores were ordered at both T1 and T2 as shown in Table 2: the highest ratings tended to be given to supported joint engagement, the lowest to coordinated joint engagement, with scaffolding in the middle. As shown in the table, means for all items increased from T1 to T2 (with the exception of sustainability of topic in the no-change group). Scores on the five items were inter-correlated: the lowest correlations were between scaffolding and coordinated joint engagement (r = .44) at T1 and between supported and coordinated joint engagement at T2 (r = .42); the highest correlations were between scaffolding and fluency at T1 (r = .78) and between scaffolding and sustainability at T2 (r = .82), with a median correlation of .69.
The five CPP rating items were analyzed with an intervention change status (increased intervention vs. no-change) by time mixed design analysis of variance, with time as the repeated measure. If increased intervention led to greater improvement, as per hypothesis 2, we would expect time by intervention-change-status interactions. Additionally, we would expect main effects for time because children’s CPP ratings usually increase as they age (Adamson et al. 2012). Analysis of variance results are shown in Table 3.
As expected, and as reflected in Tables 2 and 3, all time main effects were statistically significant, with effect sizes (pη2s) ranging from .19 to .40. However, our second hypothesis—that increased intervention would be associated with greater improvement in the quality of child-parent interaction—received only minimal support. The only statistically significant interaction was for sustainability (pη2 = .14): mean sustainability ratings increased from T1 to T2 for the increased-intervention group but remained essentially static for the no-change group (see Table 2). For all other items, however, the interactions were not statistically significant (pη2s = .012–.054). Additionally, for intervention change status, one effect was significant (pη2 = .17), one marginal (pη2 = .085), and three not statistically significant (pη2s = .040–.051; see Table 3).
Exploratory Analyses Involving Quality of Interaction for Children Diagnosed with ASD
One unexpected finding was that means for all five rating items at T1, and for 4 of 5 at T2, were higher in the no-change group than in the increased-intervention group (see Table 2). Moreover, the differences between the no-change and increased-intervention group means were greater at T1 than T2 (again, see Table 2). These observations led us to ask how children with ASD in the increased-intervention group might have been more difficult interactive partners prior to diagnosis than children with ASD in the no-change group. One possibility is that children in the increased-intervention group might be more severely affected by ASD, a hypothesis consistent with the observation (Beurkens et al. 2013) that ADOS autism severity scores (Gotham et al. 2009) were inversely related to patterns of parent–child interactions in children with ASD aged 4–14. ADOS severity scores were calculated from the ADOS assessment that was performed at the time of the diagnostic evaluation shortly after the T1 observation following the procedure established by Gotham et al. (2009). In our ASD group, the severity scores ranged from 1 through 10, with a mean of 6.18 (SD = 2.12); scores tended to be marginally higher in the increased-intervention group; M = 6.63 vs. 5.47, t(42) = 1.81, η2 = .072, p = .078. Additionally, we asked whether children in the increased-intervention group might have scored differently on the Mullen Scales of Early Learning, but in fact the total Mullen score was essentially the same in both groups; M = 57.5 vs. 57.7 for the no-change and increased-intervention groups, respectively; t(42) < 1, η2 ~ 0, p = .96.
Given our focus on the relation between the quality of parent–child interaction and intervention, we next asked whether increases in intervention after diagnosis might be related to the quality of parent–child interaction prior to diagnosis in addition to the ADOS severity score at the time of diagnosis. To address this question, we used logistic regression, modeling the increase in intervention (no-change group coded 0, increased-intervention group coded 1) as an outcome predicted by the ADOS severity score and the rating items at T1. (Higher ADOS severity scores were associated with lower T1 rating item scores—rs = −.25, −.40, −.13, −.26, and −.47; ps = .10, .007, .42, .088, and .041, for supported joint engagement, sustainability, scaffolding, fluency, and coordinated joint engagement, respectively; entering both in the regression controls for the other.)
As just stated, we know that higher ADOS severity scores were marginally more likely in the increased-intervention group (p = .078). Lower scores for the rating items were also more likely in the increased-intervention group (rs = −.29, −.45, −.31, −.42, and −.46; ps = .060, .002, .042, .005, and, .002, for supported joint engagement, sustainability, scaffolding, fluency, and coordinated joint engagement, respectively). Results of the logistic regressions (Table 4) suggest that the quality of interaction but not ASD severity is associated with increased intervention after an ASD diagnosis. When controlling for the rating item, higher ADOS severity scores increased the likelihood that parents would obtain increased hours of intervention (all partial odds ratios exceeded 1), but none were statistically significant and only the effects for supported joint engagement and scaffolding achieved the criterion for being labeled weak. When controlling for the ADOS severity score, lower scores for each rating item increased the likelihood that parents would obtain increased hours of intervention (the odds ratios for the rating items were reciprocated to transform values less than 1 to values greater than 1). But, unlike the results for ADOS severity, the quality of parent–child interaction was associated with increased intervention. The effect for supported joint engagement was weak; for scaffolding moderate and marginal; and for sustainability, fluency, and coordinated joint engagement strong and statistically significant (The high odds ratio for coordinated joint engagement reflects the limited range of these scores, 1.00–2.83 in the no-change group and 1–1.83 in the increased-intervention group).
The analyses just reported cast the ADOS severity score at the time of the diagnostic evaluation and the rating items at T1 as predictors of whether parents would obtain increased hours of intervention. In our second exploratory analysis, we considered the rating items at T2 as an outcome predicted, not by intervention change status, but by the absolute number of hours of intervention reported at T2. Because the number of hours of intervention at T2 is skewed (median = 1.5, M = 5.0, range = 0–47), we computed Spearman rank-order correlations, and because we thought that the distinction between the intervention change status groups remained meaningful, we computed correlations separately for the two groups. In the no-change group, correlations were inconsequential for four of the five rating items (ρs = –.02 to .11, ps = .68–.94) and weak and statistically insignificant for coordinated joint engagement (ρ = .14, p = .58; per Cohen (1988) we label correlations .1–.3 weak, .3–.5 moderate, and .5 or above strong). In the increased-intervention group, correlations were weak and statistically insignificant for four of the five items (ρs = .15 to .22, ps = .27–.45), but moderate and statistically significant for scaffolding (ρ = .39, p = .046). Scattergrams and regression lines for the rating items are portrayed in Fig. 3; it is noteworthy that, even though the rating item means for the increased-intervention group are only somewhat less than the means for the no-change group at T2 (see Table 2), the ranges are generally greater for the increased–intervention group. The positive regression lines in Fig. 3 suggest a weak to, for scaffolding, moderate effect of hours of intervention on parent–child interaction, at least for those parents who obtained increased intervention soon after receiving an ASD diagnosis for their child. Additionally, the absolute number of hours of intervention reported at T2 correlated only weakly with the ADOS severity score (ρ = .18, p = .24) and even less with the Mullen total score (ρ = 03, p = .86).

Scattergrams for rating items at T2 with hours of interventions per week at T2—triangles represent children in the no-change group and circles children in the increased-intervention group—along with regression lines for the increased-intervention group and correlations for the increased intervention and no-change groups. Correlations (ρ) are Spearman rank-order correlations. Accordingly, hours are represented with their ranks: Ranks below 10 represent 0 hours (all in the no-change group by definition), in the teens mainly 1 h, in the 20 s from 1.5–2.5 h, in the 30 s from 3 to 9.5 h, 40–42 from 12–19.5 h, with ranks of 43 and 44 for 40 and 47 h
As a third exploratory analysis, we again considered the rating items at T2 as an outcome, this time predicted by whether children received an ASD-specific intervention compared to children who received only standard-DD interventions (n = 12 vs. 23; groups were compared with t tests). Means for the ASD-specific group, compared to the standard-DD group, were essentially the same or slightly higher than the standard-DD group, but with small effect sizes (η2s = ~ 0–.037) and no differences were statistically significant (ps = .27–.94).
Discussion
This study documents the changes in intervention that occur when low-risk 18- to 24-month-old toddlers who are screened for ASD during a well-baby checkup are subsequently diagnosed with ASD. Our findings indicate that early diagnosis prompted many parents, especially those who had access to private services, to increase the child’s intervention hours—albeit often by only a few hours—during the half year after the diagnosis. Our results also suggest that there are significant associations between intervention use and the quality of early parent–child interactions. Parents were more likely to increase intervention hours if they were experiencing lower quality dyadic interactions before an ASD diagnosis. Moreover, although there was only minimal support for our hypothesis that increases in services would be associated with increases in the quality of dyadic interactions, our findings suggest that when intervention increases, the absolute number of intervention hours was associated with higher quality interactions.
To gather data about diagnosis, intervention, and interactions, we coordinated across two on-going research programs, one an ASD-detection project that uses gold standard screening and diagnostic methods in a large, diverse, community-based sample of low-risk 18- to 24-month old children and the other a project that systematically observes the development of communication in young children, including those diagnosed with ASD and other developmental difficulties. This approach allowed us to use systematic observational protocols and state of the art diagnostic methods to explore from an ecological perspective (Bronfenbrenner and Morris 2007) how very early screening and diagnosis might influence interventions and interactions in a community-based sample. Thus, the study provides a valuable complement to randomized control trials that address questions about the efficacy of specific early interventions on parent–child interactions with samples of toddlers who are at high-risk for ASD (Zwaigenbaum et al. 2015a). However, it is important to note that our study did augment resources available in the community in ways that supported early screening and diagnosis. As part of our project, the toddlers in our study were screened for ASD during a routine well-baby checkup using the M-CHAT-R (which is a procedure that is fortunately becoming an increasingly common occurrence; see Zwaigenbaum et al. 2015b). Moreover, toddlers who screened positive were given free comprehensive ASD evaluations, which allowed us to skirt the complex concerns about the limited availability of diagnostic services for toddlers who screen positive for ASD (see Swanson et al. 2014, for a cogent discussion of this problem and possible solutions). Moreover, and most importantly, our coordination of diagnostic and observational research allowed us to study interventions and interactions in a diverse sample of low-risk toddlers who were diagnosed with ASD months and even years earlier than many previous studies.
Our most striking finding is that an ASD diagnosis clearly prompted many parents to increase the amount of intervention during the half year following the diagnostic evaluation. This is especially noteworthy since about half of the parents whose 2-year olds screened positive for ASD risk had already begun to access early intervention and therapeutic services before their child was diagnosed with ASD. However, the number of hours in intervention was very low prior to diagnosis, and there was only a weak relationship between whether a toddler was already receiving services and their subsequent diagnosis. These results are consistent with recent findings (Monteiro et al. 2016) that most children who were referred to a regional autism clinic for a diagnostic evaluation were already receiving intervention services. Unfortunately, they also noted that, like the toddlers in our sample, most of the children in their sample were dependent on publicly funded services and thus were likely to be receiving far less than the optimal number of hours of services.
Importantly, we were also able to document that receiving an ASD diagnosis may be a powerful impetus toward intervention, including ASD-specific interventions. Compared to toddlers who were not diagnosed with ASD, toddlers diagnosed with ASD were significantly more likely to increase participation in intervention. As is customary during the evaluation session and in the subsequent written report, parents—regardless of their child’s diagnosis—received individualized recommendations related to obtaining services. However, we did not directly offer intervention services or actively guide parents through the complex process of locating programs and securing resources (see, e.g., Wise et al. 2010). Nonetheless, at our second observation, only nine children of the 44 diagnosed with ASD (20 %, down from 48 %) were not receiving any services. Moreover, the number of parents who adopted multiple treatment approaches rose markedly from eight prior to diagnosis to 28 after diagnosis. This finding, along with the high prevalence of standard therapies such as speech language therapy and the relatively low enrollment in ASD-specific interventions, is consistent with other studies (e.g., Bowker et al. 2011; Irvin et al. 2012) that examined the use of services for children with ASD.
Finding an increase in intervention during the months after an ASD diagnosis was all the more remarkable given the challenges parents faced accessing services for children under 3 diagnosed with ASD at the time (early 2010s) and place (a large city) of our study. The paucity of available resources, both financial and programmatic, undoubtedly affected the types and intensity of services. During the discussions with parents during our second observation session, we often heard how limitations in resources presented barriers when they were actively trying to gain additional services and to use them consistently. In this regard, it is noteworthy that all but one of the toddlers enrolled in an ASD-specific service were relying in whole or in part on private funding. Especially poignant was one parent’s comment that although she had attempted to enroll in new interventions including an ASD-specific school program, her child had yet to receive any services because they were still trying to gain public assistance.
Difficulties securing optimal services were also reflected in the low intensity of intervention most children received. Thus, despite notable increases in intervention, a half year after diagnosis 77 % of the children diagnosed with ASD were receiving less than 5 h, and 89 % less than 10 h, of intervention per week. These findings are consistent with previous ones (Hebbeler et al. 2007), suggesting that the context of the current study was not particularly resource poor. Moreover, the duration of these services was likely often quite short since it often took many weeks to arrange a new service. Thus we were not surprised that our second hypothesis—that there would be a positive relationship between an increase in intervention and increase in the quality of parent–child interactions—received only minimal support; only 1 of our 5 rating items, sustainability, increased significantly more for the increased intervention group than the no-change group. Nevertheless, there were several intriguing indications that there is an association between early interventions and interactions during the months after diagnosis.
Our observations of quality of parent–child interaction were intentionally focused on aspects of early dyadic communication that are affected by ASD, rather than on specific child actions, such as deictic gestures, that are also affected by ASD (Özçaliskan et al. 2015, on-line). Thus all of our ratings depended to some extent on contributions from both partners. The child’s actions are emphasized most in the rating of coordinated joint engagement since the child must actively attend to the partner. The parent’s actions are focal to the rating of supported joint engagement (which does not require active child attention to the parent) and scaffolding (which assessed how well the parent was able to augment and expand the child’s communication). The quality of the parent and child co-constructed dyadic interaction is most central to the ratings of sustainability and the fluency and connectedness of communication. The rating items performed as expected based on previous studies that used them to document the quality of interactions between parents and typically developing toddlers (Adamson et al. 2012; Hirsh-Pasek et al. 2015) and to compare interactions across diagnostic groups including ASD (Adamson et al. 2012). The rating items were strongly correlated, suggesting that they were indeed characterizing related aspects of how well a parent and child were able to engage together and sustain connected and fluent interactions. Moreover, we replicated previously published findings. It is particularly striking how similar the mean ratings at our second observational sessions (when children with ASD were, on average, 31 months old) were to those for 30-month-old children with ASD in Adamson et al. (2012): Ms = 4.4 for supported joint engagement in both samples; 3.8 and 3.5 for sustainability, 3.3 and 3.5 for scaffolding, 2.8 and 2.9 for fluency, and 1.6 and 1.5 for coordinated joint engagement for our current and previous samples, respectively. Thus, as in another ASD sample, ratings in the current ASD sample were markedly lower than the comparable ratings for interactions between parents and 30-month-old typically developing children (Ms were 5.9, 5.3, 4.3, 5.6, and 3.0; Adamson et al. 2012).
Given the early age of diagnosis in our study and our longitudinal design, we were able to observe changes in the quality of interaction for toddlers diagnosed with ASD. In typically developing toddlers, toddlerhood is a period of notable positive change, especially for fluency and connectedness, as symbols infuse communication (Adamson et al. 2012). It appears to be so as well for 2-year olds diagnosed with ASD in a diverse, community-based, low-risk sample. All five ratings increased significantly from 24 to 31 months with fluency and connectedness once again showing the strongest improvement.
Documenting that the quality of parent–child interactions often improves early in the developmental course of ASD has important implications. Most fundamentally, it displays the potential for positive change during the stressful period just after diagnosis. In addition, it prompts difficult questions about why there is variability in how much improvement occurs during this period. In the current study, we focused primarily on the impact of increased interventions on parent–child interactions. Dividing our sample using the binary distinction of whether the child’s intervention hours increased or remained the same in the months after diagnosis did not shed much light on the link between increased intervention and improved quality of interactions: our hypothesis that increased intervention would be associated with greater improvement in interaction quality received only modest support with only one of the five ratings (sustainability) improving significantly more for the increased intervention group. One likely explanation is that a longer time frame is needed to see the effects of increased intervention on interactions. Thus an important next step will be to continue to trace the development of dyadic interactions in relationship to intervention.
In addition, the results of our exploratory analyses of the relation between interactions and increases in intervention produced two sets of provocative findings. First, our results suggest that the quality of interactions before ASD is diagnosed may influence whether intervention increases in the months after diagnosis. The pattern of findings across rating items is especially intriguing. Items that focus on the child’s contribution to joint engagement and on the dyad’s success at sustaining topics and fluent and connected interactions—not the items that focused primarily on how well the parents support communication—were most strongly related to increased intervention. This pattern suggests that parents were especially sensitive to the child’s difficulties contributing to communicative exchanges. It is also interesting to note that the severity of ASD as assessed during the ADOS or the child’s cognitive level as assessed by the Mullen where the child interacts with a skilled clinician was not as good a predictor of intervention increase as difficulties in interaction assessed during parent–child interaction during the CPP. The ADOS severity scores only marginally predicted whether interventions would increase by our second observation; Mullen scores were virtually identical for children who did and who did not increase intervention hours. Moreover, in a logistic regression analysis using both the ADOS severity scores and the rating items, only the rating items were associated with significant increases in intervention.
Second, when we examined the relation between variation in the intensity of intervention and the ratings of parent–child interaction after an ASD diagnosis, we found an association between the number of hours in intervention and the quality of interactions for children who experienced increased intervention, but not for those whose intervention hours did not increase after diagnosis. The lack of effect for the no-change group is not surprising since the variability in intensity was minimal and included all nine children who were not in intervention. Although the number of hours of intervention in the increased intervention group was quite low (recall that 77 % reported 5 h per week or less), there was enough variability in number of hours per week to ask whether intervention intensity and the quality of interaction were related. Our findings suggest that they may be; the five correlations between number of hours and ratings of quality were all positive, although only scaffolding was of moderate strength and statistically significant.
It is important to emphasize that our study of intervention use and interactions after early diagnosis of ASD in a low-risk community-based sample differs both in aim and analyses from studies of the efficacy of specific interventions. In particular, our measure of intervention relied solely on parents’ reports of interventions they were currently using and so we do not have information about if and how interventions specifically focused on improving parent–child interactions. In addition, in future studies it will be important to probe more fully how financial resources and diagnosis influence access to interventions. Compared to children in our non-ASD group, children diagnosed with ASD were more likely to have increased services since our first laboratory session and much more likely to be receiving ASD-specific interventions. In part this disparity likely reflects the match between diagnosis and intervention. But it also may also reflect differences in both access and parents’ sense of urgency. With regard to access, it is noteworthy that enrollment in ASD-specific interventions was heavily dependent on private funding. In future research, it will be important to probe further to determine whether differences in diagnosis affect children’s eligibility for more hours and different types of intervention. Finally, we think it would be helpful to gain more information about parents’ characteristics. Here we were limited to basic demographic information of age, race, and education, and found that only age was correlated significantly with increased intervention after an ASD diagnosis. Thus, we are left with intriguing questions about how parental characteristics as diverse as depression, support systems within the community, knowledge and beliefs about early development, and parenting efficacy might mediate the relationship between intervention services and parent–child interaction.
In summary, our findings indicate that the early diagnosis of ASD in low-risk toddlers who screen positive for ASD risk during well-baby checkups in community pediatric settings often prompts increases in interventions. The number and type of interventions parents are able to access within the months after the diagnosis of ASD are most often far from optimal; children are most likely not receiving high intensity ASD-specific interventions. Moreover, there appears to be a complex relation between intervention and the quality of dyadic interactions. In part this is due to increases in the quality of dyadic interactions that occur as the development of language affects dyadic communication processes. But the relation is also complex because the severity of early interactive difficulties appears to influence whether parents rapidly secure increased interaction as well as how the intensity of interactions they do secure may be related to the quality of interactions they experience with their children. Further research—research that clarifies more fully what transpires when toddlers are diagnosed with ASD after community-based ASD screening—is needed, not only to enrich our understanding of how early diagnosis affects parent–child interactions and intervention use, but also to enhance the design of programs that can help parents rapidly obtain effective intervention services after an early diagnosis.
References
Adamson, L. B., Bakeman, R., Deckner, D. F., & Nelson, P. B. (2012). Rating parent-child interactions: Joint engagement, communication dynamics, and shared topics in autism, Down syndrome, and typical development. Journal of Autism and Developmental Disorders, 42, 2622–2635.
Adamson, L. B., Bakeman, R., Deckner, D. F., & Romski, M. (2009). Joint engagement and the emergence of language in children with autism and Down syndrome. Journal of Autism and Developmental Disorders, 39, 84–96.
Adamson, L. B., Kaiser, A., Tamis-Lemonda, C., Owen, M., & Dimitrova, N. (2016). The developmental landscape of language acquisition and intervention. Manuscript submitted for publication.
Adamson, L. B., McArthur, D., Markov, Y., Dunbar, B., & Bakeman, R. (2001). Autism and joint attention: Young children’s responses to maternal bids. Journal of Applied Developmental Psychology, 22, 439–453.
Bakeman, R., & Quera, V. (2011). Sequential analysis and behavioral methods for the behavioral sciences. Cambridge: Cambridge University Press.
Barton, M., Boorstein, H., Herlihy, L., Dumont-Mathieu, T., & Fein, D. (2012). Toddler ASD Symptom Interview. Self-published.
Beurkens, N. M., Hobson, J. A., & Hobson, R. P. (2013). Autism severity and qualities of parent-child relations. Journal of Autism and Developmental Disorders, 43, 168–178.
Bowker, A., D’Angelo, N. M., Hicks, R., & Wells, K. (2011). Treatments for autism: Parental choices and perceptions of change. Journal of Autism and Developmental Disorders, 41, 1373–1382.
Boyd, B., McDonough, S., Rupp, B., Khan, F., & Bodfish, J. (2011). Effects of a family-implemented treatment on the repetitive behaviors of children with autism. Journal of Autism and Developmental Disorders, 41, 1330–1341.
Bronfenbrenner, U., & Morris, P. A. (2007). The bioecological model of human development. In R. M. Lerner (Ed.), Handbook of child psychology (Vol. 1, pp. 793–828). Hoboken, NJ: Wiley.
Charman, T. (2004). Why is joint attention a pivotal skill in autism? In U. Frith & E. L. Hill (Eds.), Autism: Mind and brain (pp. 68–87). Oxford: Oxford University Press.
Chlebowski, C., Robins, D. L., Barton, M. L., & Fein, D. (2013). Large-scale use of the modified checklist for autism in low-risk toddlers. Pediatrics, 131, 1121–1127.
Cohen, J. (1968). Weighted kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychological Bulletin, 70, 213–220.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. New Jersey: Lawrence Erlbaum Associates.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greeson, J., et al. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125, 17–23.
Eikeseth, S., Smith, T., Jahr, E., & Eldevik, S. (2007). Outcome for children with autism who began intensive behavioral treatment between ages 4 and 7. Behavior Modification, 31, 264–278.
Goin-Kochel, R. P., Myers, B. J., & Mackintosh, V. H. (2007). Parental reports on the use of treatments and therapies for children with autism spectrum disorders. Research in Autism Spectrum Disorders, 1, 195–207.
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 693–705.
Green, V. A., Pituch, K. A., Itchon, J., Choi, A., O’Reilly, M., & Sigafoos, J. (2006). Internet survey of treatments used by parents of children with autism. Research in Developmental Disabilities, 27, 70–84.
Hebbeler, K., Spiker, D., Bailey, D., Scarborough, A., Mallik, S., Simeonsson, R., & Singer, M. (2007). Early intervention for infants and toddlers with disabilities and their families: Participants, services, and outcomes. Final report of the National Early Intervention Longitudinal Study (NEILS).
Hirsh-Pasek, K., Adamson, L. B., Bakeman, R., Owen, M. T., Golinkoff, R. M., Pace, A., et al. (2015). The contribution of early communication quality to low-income children’s language success. Psychological Science, 26, 1071–1083.
Howlin, P., & Moore, A. (1997). Diagnosis in autism: A survey of over 1200 patients in the UK. Autism, 1, 135–162.
Irvin, D. W., McBee, M., Boyd, B., Hume, K., & Odom, S. L. (2012). Child and family factors associated with the use of services for preschoolers with autism spectrum disorder. Research in Autism Spectrum Disorders, 6, 565–572.
Kaiser, A. P., Hancock, T. B., & Nietfeld, J. P. (2000). The effects of parent-implemented enhanced milieu teaching on the social communication of children who have autism. Journal of Early Education and Development, 4, 423–446.
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47, 611–620.
Keenan, M., Dillenburger, K., Doherty, A., Byrne, T., & Gallagher, S. (2010). The experiences of parents during diagnosis and forward planning for children with autism spectrum disorder. Journal of Applied Research in Intellectual Disabilities, 23, 390–397.
Kogan, M. D., Strickland, B. B., Blumberg, S. J., Singh, G. K., Perrin, J. M., & vanDyck, P. C. (2008). A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005–2006. Pediatrics, 122, 1149–1158.
Landa, R. (2007). Early communication development and intervention for children with autism. Mental Retardation and Developmental Disabilities Research Reviews, 13, 16–25.
Landa, R. J. (2008). Diagnosis of autism spectrum disorders in the first 3 years of life. Nature Clinical Practice Neurology, 4, 138–147.
Landa, R. J., Holman, K. C., O’Neill, A. H., & Stuart, E. A. (2011). Intervention targeting development of socially synchronous engagement in toddlers with autism spectrum disorder: A randomized controlled trial. Journal of Child Psychology and Psychiatry, 52, 13–21.
Lawton, K., & Kasari, C. (2012). Brief report: Longitudinal improvements in the quality of joint attention in preschool children with autism. Journal of Autism and Developmental Disorders, 42, 307–312.
Le Couteur, A., Lord, C., & Rutter, M. (2003). The Autism Diagnostic Interview-Revised (ADI-R). Western Psychological Service: Los Angeles, CA.
Lord, C., & Luyster, R. (2006). Early diagnosis of children with autism spectrum disorders. Clinical Neuroscience Research, 6, 189–194.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (2000). Autism Diagnostic Observation Schedule (ADOS). Los Angeles, CA: Western Psychological Service.
Mandell, D. S., & Novak, M. (2005). The role of culture in families’ treatment decisions for children with autism spectrum disorders. Mental Retardation and Developmental Disabilities Research Reviews, 11, 110–115.
Miller, V. A., Schreck, K. A., Mulick, J. A., & Butter, E. (2012). Factors related to parents’ choices of treatment for their children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6, 87–95.
Minjarez, M. B., Williams, S. E., Mercier, E. M., & Hardan, A. Y. (2011). Pivotal response group treatment program for parents of children with autism. Journal of Autism and Developmental Disorders, 41, 92–101.
Monteiro, S. A., Dempsey, J., Broton, S., Berry, L., Goin-Kochel, R. P., & Voigt, R. G. (2016). Early intervention before autism diagnosis in children referred to a regional autism clinic. Journal of Developmental and Behavioral Pediatrics, 37, 15–19.
Mullen, E. M. (1995). Mullen Scales of Early Learning. Circle Pines, MN: American Guidance Circle.
Myers, S. M., & Johnson, C. P. (2007). Management of children with ASD. Pediatrics, 120, 1162–1182.
National Autism Center. (2015). Findings and conclusions: National Standards Project, Phase 2. MA: Randolph.
National Research Council. (2001). Educating Children with Autism. Committee on Educational Interventions for Children with Autism. In C. Lord & J. P. McGee (Eds.), Division of Behavioral and Social Sciences and Education. Washington, DC: National Academy Press.
Özçalışkan, S., Adamson, L. B., & Dimitrova, N. (2015, on-line). Early deictic but not other gestures predict later vocabulary in both typical development and autism. Autism.
Robins, D. L., Casagrande, K., Barton, M., Chen, C. A., Dumont-Mathieu, T., & Fein, D. (2014). Validation of the Modified Checklist for Autism in Toddlers, Revised with Follow-up (M-CHAT-R/F). Pediatrics, 133, 37–45.
Robins, D.L., Fein, D., & Barton, M. (2009). The Modified-Checklist for Autism in Toddlers-Revised with Follow-up (M-CHAT-R/F). Self-published.
Sigman, M., & Ruskin, E. (1999). Social competence in children with autism, Down syndrome and other developmental delays: A longitudinal study. Monographs on the Study for Research in Child Development, 6, 1–114.
Swanson, A. R., Warren, Z. E., Stone, W. L., Vehorn, A. C., Dohrmann, E., & Humberd, Q. (2014). The diagnosis of autism in community pediatric settings: Does advanced training facilitate practice change? Autism, 18, 555–561.
Wetherby, A. M., Brosnan-Maddox, S., Peace, V., & Lewton, L. (2008). Validation of the Infant Toddler Checklist as a broadband screener for autism spectrum disorders from 9 to 24 months of age. Autism, 12, 487–511.
Wise, M. D., Little, A. A., Holliman, J. B., Wise, P. H., & Wang, J. (2010). Can state early intervention programs meet the increased demand of children suspected of having autism spectrum disorders. Journal of Developmental and Behavioral Pediatrics, 31, 469–476.
Woolfenden, S., Sarkozy, V., Ridley, G., & Williams, K. (2012). A systematic review of the diagnostic stability of autism spectrum disorder. Research in Autism Spectrum Disorders, 6, 345–354.
Yama, B., Freeman, T., Graves, E., Yuan, S., & Campbell, M. K. (2012). Examination of the properties of the Modified Checklist for Autism in Toddlers (M-CHAT) in a population sample. Journal of Autism and Developmental Disorders, 42, 23–34.
Zwaigenbaum, L., Bauman, M. L., Choueiri, R., Kasari, C., Carter, A., Granpeesheh, D., et al. (2015a). Early intervention for children with autism spectrum disorder under 3 years of age: Recommendations for practice and research. Pediatrics, 136(Supplement 1), S60–S81.
Zwaigenbaum, L., Bauman, M. L., Fein, D., Pierce, K., Buie, T., Davis, P., et al. (2015b). Early screening of autism spectrum disorder: Recommendations for practice and research. Pediatrics, 136(Supplement 1), S41–S59.
Acknowledgments
This study was funded by grants from the National Institute of Child Health and Human Development (R01HD035612; R01HD039961) and Autism Speaks (Targeted Research Award #8368). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health. Portions of this study were presented at the 2012 international meeting of the American Speech-Language-Hearing Association, Atlanta, GA and the 2014 International Meeting for Autism Research, Atlanta, GA. The authors thank Brooke Nelson, Ann Grossniklaus, Amber Shoaib, Glencora King, Benjamin Brandon, Diana Volkov, Courtney Cadle, Ashleigh Kellerman, Pamela Rutherford, and Deborah Deckner for their help conducting sessions and coding the corpus. Finally, we acknowledge with gratitude the parents and children who participated in our longitudinal study.
Author Contributions
K. Suma led the conceptualization of the study and contributed to its design, to the data collection, analysis and interpretation, and, with L. Adamson, drafted the manuscript’s introduction, methods, and discussion. L. Adamson also collaborated on the study conceptualization and design, directed the project that generated the ratings of social interaction, and contributed to the interpretation of the findings. R. Bakeman conducted the data analysis, drafted the results section, and contributed to the manuscript writing. D. Robins directed the ASD screening and diagnosis of the study participants and contributed to the study design and manuscript writing. D. Abrams assisted in conceptualizing the study, reviewing the literature, and revising the manuscript. All authors approved the final manuscript as submitted.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Diana L Robins is co-holder of the copyright for the M-CHAT and M-CHAT-R and co-owner of M-CHAT, LLC, which receives royalties from companies that incorporate the M-CHAT into commercial products. All other authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All parents provided informed consent for themselves and their child’s participation prior to their inclusion in this study.
Rights and permissions
About this article

Cite this article
Suma, K., Adamson, L.B., Bakeman, R. et al. After Early Autism Diagnosis: Changes in Intervention and Parent–Child Interaction. J Autism Dev Disord 46, 2720–2733 (2016). https://doi.org/10.1007/s10803-016-2808-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-016-2808-3