
Abstract
The purpose of this pilot study was to evaluate the efficacy of the interview skills curriculum (ISC), a manualized 12-week group-delivered intervention for young adults with autism spectrum disorder (ASD). This intervention aims to increase social–pragmatic skills essential to a successful job interview. Twenty-eight adults (18–36 years) were randomly assigned to one of two groups: ISC or waitlist control. Results revealed that the experimental group showed larger gains in social–pragmatic skills observed during a mock job interview than the control group. Treatment effects on distal outcomes, including social adaptive behaviors and depressive symptoms were not significant, although the respective effect sizes were medium/large. Results indicate that a brief, low-intensity treatment can improve the job-interview performance of young adults with ASD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The current prevalence of autism spectrum disorders (ASD) is estimated at 1 case per 88 (CDC 2012). With more than 70 % of individuals with autism being under age 14, there is clearly a significant challenge on the horizon with respect to serving an ever-expanding population of adults with ASD (Gerhardt and Lanier 2011). One consequence of this vast increase in identified individuals is a much larger proportion of the ASD population with IQ estimates within the normal range. Whereas this ‘high functioning’ cohort of adolescents and young adults may have strengths in intelligence and verbal ability, positive outcomes are not guaranteed for this group. Howlin et al. (2004) surveyed 68 adults with ASD and found that outcome was highly variable even for those in the normal IQ range and that neither verbal nor performance IQ were strong predictors of outcome. Compounding this finding is that individuals who have cognitive and linguistic skills within the normal range are likely to have limited access to services and have recently been found to be three times as likely to have no daytime activities compared to adults with ASD who have an intellectual disability (Taylor and Seltzer 2011).
The social communication deficits of ASD typically identified in childhood appear to persist into adulthood and may impact a number of outcomes (Howlin 2000; Sigman and McGovern 2005; McGovern and Sigman 2005). Challenges with verbal communication include use of shorter utterances, poor reporting of events, and difficulty engaging in conversation have been described for adults with ASD (Howlin et al. 2000) whereas nonverbal communication weaknesses include effective use of eye gaze, gestures, and facial affect (Szatmari et al. 1989). Impairments in adaptive social skills in the presence of normal intellectual ability have been reported for adolescents and young adults with ASD (Klin et al. 2007; Venter et al. 1992). Thus, the domain of social communication may serve as a critical target area to improve adult outcomes.
Bleak outcomes for high functioning adults with ASD span across the social, employment, and mental health domains. Social outcomes for adults with ASD indicate low rates of independent living, and friendships; even for those with normal IQ—more than half report having no friends (Howlin et al. 2004; Liptak et al. 2011; Orsmond et al. 2013). Recent work utilizing the National Longitudinal Transition Study-2 (NLTS2), a prospective study that has followed over 11,000 youth with disabilities into adulthood, has characterized social participation of young adults with ASD (Orsmond et al. 2013). After adjusting for factors such as family income, communication ability, and involvement in work and school, this study reports high levels of isolation experienced by young adults with ASD relative to those with other disabilities (Orsmond et al. 2013).
Occupational outcomes for young adults with ASD also indicate a significant challenge for this population with approximately one half reporting having ever worked for pay following high school (Roux et al. 2013). Overall high rates of unemployment for young adults with ASD have been reported in a Canadian study (Jennes-Coussens et al. 2006) and in a survey of 200 young adults in Florida (CARD 2008). For those with jobs, rates of competitive employment are low (Howlin et al. 2004), employment status is typically low (Barnard et al. 2001; Mawhood and Howlin 1999), and young adults with ASD report earning significantly lower wages than young adults from other disability groups (Roux et al. 2013).
The third challenging outcome area for young adults with ASD is that of mental health. Estimated rates of co-existing psychiatric disorders in individuals with ASD who have normal intelligence have varied substantially, from 9 to 89 % with depression, often associated with severe anxiety, as the most common psychopathology in adults with ASD (Howlin 2000). A preliminary study of adults with AS found that 32 % reported having a co-morbid mental health problem and 15 % had planned or attempted suicide (Barnard et al. 2001). Converging research indicates a strong association between higher cognitive ability and the presence of increased rates of depression (Shtayermman 2007; Sterling et al. 2008).
Reported connections among these domains provide valuable insight for intervention planning. Chadsey-Rusch (1992) reported that social skills are related to positive employment outcomes. Not surprisingly loneliness and lack of quality friendships correlate with depression (Whitehouse et al. 2009). While connections amongst these domains requires further inquiry, the implication of these findings for treatment is that improvement in one domain may fuel resultant improvement in another having an overall additive effect on positive outcomes.
These data highlight the social, employment, and mental health challenges facing adults with ASD and firmly establishes the need for evidence-based interventions addressing these outcomes. Because of the limited research on social skills interventions for adults with ASD, we must turn to the child and adolescent literature to examine the current evidence in this area. Williams-White et al. (2007) conducted a systematic review of group intervention research for school-age children and adolescents with ASD. Their evaluation of 14 studies identified a number of promising intervention strategies including those to increase social motivation, social initiations, to improve appropriate social responding, reduce interfering behaviors, and promote skill generalization. Of the 14 studies, only five used a comparison group and none used random assignment. Studies generally reported positive effects via qualitative and observational data. Data from quantitative outcome measures, however were inconsistent. Some studies showed small to moderate improvements (Cotter 1997; Provencal 2003) and others showed no improvement (Ozonoff and Miller 1995; Webb et al. 2004).
While a burgeoning body of evidence for social skills interventions aimed at children and adolescents with ASD is available (Laugeson et al. 2012, Williams-White et al. 2007), there is a tragic dearth of research with the adult populations in this area. The Interagency Autism Coordinating Committee (IACC 2012) in the Department of Health and Human Services recently addressed the concern of a lack of tested interventions to address core symptoms of ASD as well as adaptive behavior by emphasizing the need for adult treatment research to be a high priority on the nation’s research agenda.
Reports of social skills groups for adults with ASD indicate improvements in social skills related to conversation and the development of relationships (Hillier et al. 2007; Howlin and Yates 1999; Mesibov 1985). These programs, however, were administered without comparison groups thus firm conclusions cannot be drawn about the nature of described effects. Turner-Brown et al. (2008) conducted a quasi-experimental study with 11 adults with high functioning ASD to evaluate feasibility and utility of an adaptation of the Social Cognition and Interaction Training (SCIT) developed for adults with psychotic disorders (Roberts et al. 2004). Following the 18-week group intervention, participants in the SCIT-A condition demonstrated significant improvement in theory-of-mind skills as measured by the Hinting Task (Corcoran et al. 1995) compared to those who did not receive the treatment. Although not significant, the treatment group showed an increase in perceived social communication skills relative to controls. No changes were observed on a behavioral observation utilizing role-play scenarios wherein the participants engaged in a set of 3-min conversations on predetermined topics. Although this study is limited by lack of randomization and small group size, it demonstrates feasibility and promise as a group-delivered treatment to target social skills for adults with HFA.
In the first RCT evaluating a behavioral intervention for adults with ASD, Gantman et al. (2012) tested an adaptation of the UCLA PEERS Program (Laugeson and Frankel 2010) with seventeen young adults ranging in from 18 to 23 years of age. Young adults and their caregivers attended separate concurrent sessions. After 14 weekly sessions, the PEERS treatment group showed significant improvement relative to controls on both social skills and the development of social relationships as indicated by several self- and parent-report measures. This study provides initial support for the effectiveness of the PEERS for Young Adults Program, however two primary limitations in measurement are important to note. First diagnosis of ASD was not confirmed with a standardized measure such as the ADOS. Second, behavioral observations to document acquisition of new social skills were not included. In spite of these limitations, this study represents positive movement toward strong efficacy research on interventions for adults with ASD.
The limited evidence available points to the need for additional research using rigorous research designs with increased sample sizes. Research is sorely needed that incorporates self report but also extends evaluation efforts by including comprehensive standardized measures to accurately characterize the sample studied and detect change as a result of the intervention. Specifically, use of measures targeting the constructs of mental health and adaptive behavior are critical. Further, blinded assessment of behavioral observations should be incorporated to provide an objective, unbiased analysis of skills acquired as a result of participation in the intervention.
The purpose of this pilot study was to evaluate the efficacy of the interview skills curriculum (ISC), a manualized 12-week group-delivered intervention for young adults with ASD. This intervention aims to increase social–pragmatic skills essential to a successful job interview. We hypothesized that adults who receive ISC would show significant gains in targeted social and pragmatic skills between baseline and 6-month follow up. Further, it was hypothesized that participants would improve in their social adaptive behavior skills and would report improvements in depressive symptoms.
Methods
Participants
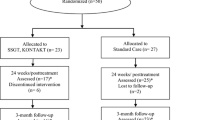
A total of 33 adults were evaluated for participation in the study from August 2012 to January 2013. The study was conducted in Tallahassee, Florida and participants were recruited primarily from the Florida State University Center for Autism and Related Disabilities (CARD). All CARD clients in Tallahassee and surrounding communities that were in the age range for this study were mailed a letter describing the project along with a form where they could indicate interest in study participation. In addition, staff of local organizations serving adults with ASD was provided with recruitment information that they could share with their clients with ASD. Individuals were eligible to participate if they: (1) had previously been given a clinical diagnosis of ASD (including Autistic Disorder, Asperger’s Syndrome, Pervasive Developmental Disorder-Not Otherwise Specified) meeting DSM-IV-TR (APA 2000) diagnostic criteria for an ASD, (2) ranged in age from 18 to 36 years, (3) demonstrated an verbal IQ above 70, and (4) possessed a special or regular high school diploma or a high school GED or equivalent. Individuals at any stage of employment or unemployment were considered for participation. Participants’ clinical diagnoses were confirmed using the Autism Diagnostic Observation Schedule (ADOS-2; Lord et al. 2012). As shown in Fig. 1, 33 young adults signed consent and were evaluated for eligibility. Four individuals were excluded from the study because they did not meet criteria for an ASD on the ADOS-2. An additional participant completed baseline assessments but declined to participate prior to randomization. Twenty-eight adults diagnosed with ASD were pairwise matched according to their performance on the Stanford-Binet Intelligence Scale-Abbreviated Battery (SB5-ABIQ 5th Ed; Roid 2003) and randomly assigned to either treatment or waitlist control condition. Twenty-four participants completed the study.

Participant recruitment, enrollment, randomization, and retention
Descriptive information on the participants’ demographic characteristics, cognitive and adaptive abilities, and ASD symptoms is presented separately for the experimental and control group (Table 1). The sample included 27 males and one female. Participants ranged in age from 18 to 36 years (M = 24.5, SD = 5.2). All participants except one met diagnostic criteria for Autistic Disorder (n = 16) or ASD (n = 11) on the ADOS-2. The one remaining participant met diagnostic cutoff scores on both the Reciprocal Social Interaction and the Communication subscales, but missed the combined cutoff score by one point. Because the evaluator’s clinical impression confirmed the ASD diagnosis, we decided to retain the participant in the sample. At baseline, participants completed a descriptive survey, eliciting information about various social, educational, and occupational activities and experiences (Adult Living Interview). Responses revealed that four participants were employed full-time, and one participant was employed part-time when entering the study. Although four of the five employed participants reported working within their field of interest, three stated plans to improve their employment situation during the next year (e.g., changing from part-time to full-time employment, changing fields). Occupations included a self-employed attorney, a computer analyst, an administrative secretary, and service occupations related to food preparation or janitorial duties. In addition, eleven young adults were currently enrolled in a formal college or university program (n = 10), or completing coursework in preparation for the General Educational Development (GED) test (n = 1). Two of the eleven adults enrolled in an educational program also held part-time positions, one as a math tutor and the other as an administrative office assistant. Table 2 includes information on the participants’ educational attainment, employment history, living situation, social activities, and future plans, presented separately for individuals classified as unoccupied, student, or employed. Statistical tests revealed a significant association between participants’ current educational/occupational classification and their level of educational attainment, Χ 2(2) = 10.1, p < .01, Cramer’s V = .60 (large effect size). Finally, it is notable that out of the 16 individuals who reported having ever been employed, almost half (n = 7) reported having lost employment due to difficulties following company policies or practices (n = 3), difficulty getting along with others (n = 1), or difficulty keeping up with demands (n = 1). With one exception, all participants stated a desire to work, and 14 reported plans to improve their employment situation during the next year.
Overview and Timeline
Data for this randomized clinical trial were collected at a single project site between 2012 and 2013. Two waves of data were collected. Baseline assessments occurred during two individual sessions. During the first session, assessments were conducted to confirm diagnosis of ASD and to provide baseline characteristics of the sample. An experienced diagnostician working within the FSU Autism Institute completed the evaluation. Measures included: (1) the Stanford-Binet Intelligence Scale-Abbreviated Battery (SB5-ABIQ 5th Ed; Roid 2003); (2) the ADOS-2 (Lord et al. 2012); (3) Vineland-II Adaptive Behavior Scales (VABS-II; Sparrow et al. 2004), and the depression scale of the Health Questionnaire-9 (PHQ-9; Spitzer et al. 1999). On a separate day, participants completed a mock job interview.
Once the initial assessments were completed, pairs of participants were matched on their performance on the SB5-ABIQ and randomly assigned to one of two groups: treatment or waitlist control. Because it is important to have group equivalence on nonverbal intelligence, we used a matched random assignment process which is preferred to stratifying when possible (Shadish et al. 2002). Those randomized to the treatment group participated in one of two (Fall or Spring) 12-week offerings of the ISC. Those randomized to waitlist control did not receive intervention during the study period but were invited to participate in an ISC class following exit assessments for the study. Throughout the study, staff and students involved in administering assessments or coding observations were kept blind to the participant’s group assignment. After the last intervention session was completed, participants completed a series of exit assessments. Exit assessments included some but not all measures administered at baseline. The time lag between baseline and exit assessments varied substantially between participants, but was well matched between the experimental (M = 5.42 months, SD = 2.16, range 2.4–10.2) and control group (M = 6.13 months, SD = 1.97, range 2.9–8.0). Information on subjects’ completion of the allocated intervention, measures and attrition is displayed in Fig. 1 (CONSORT Flow Diagram).
Intervention Procedures
ISC is a manualized 12-week, low-intensity group-delivered intervention aimed at increasing social–pragmatic skills with an emphasis on those essential to a successful job interview. In 2007–2008 Dr. Amy Wetherby and Dr. Lindee Morgan co-directed a service grant from the Able Trust to conduct a Job Interview Class to help prepare teens and young adults with ASD for success in their job interview experiences. Twenty-seven teens and young adults participated in a year-long program with a number of positive outcomes. Notably, 78 % (14 out of 18 in the job market) secured employment by the end of or shortly following participation in he class.
ISC was developed as a result of the Able Trust project. ISC is a manualized intervention protocol that has been developed as a 3-month treatment package presented in a group setting utilizing weekly meetings (90 min per session). Meeting topics are organized to reflect portions of the interview process in a logical, structured format. Primary curriculum topics include: (1) Character, attitude, and persona, (2) Small talk, non-verbal communication, and hygiene, and (3) Interview questions, closing the interview, and follow-up. Each curriculum topic lasted approximately four sessions. Due to the social communication challenges faced by individuals with ASD, additional topics infused into the curriculum include: non-verbal communication; emotional regulatory strategies, and self-advocacy. Meeting content is presented in a variety of formats including discussion, role-play, video feedback, peer review, and games. Mock job interviews were conducted twice (pre- and post-treatment) in order for each participant to practice interviewing skills and to serve as a context in which the skills taught in the ISC could be measured.
The ISC treatment sessions were delivered by the second author, Allison Leatzow, an educator and former job coach with extensive experience working with adolescents and adults with ASD. Allison has worked as an Autism Consultant with FSU CARD since 2006, was the lead instructor for the Able Trust Project, and is one of the developers of the ISC. Delivery of treatment fidelity (Resnick et al. 2005) was monitored monthly by the first author to document whether the instructor implemented ISC with the group as intended. Participants who completed the study were provided with a DVD copy of their mock job interviews a $200 gift card intended for the purchase of job interview clothing.
Measures
Descriptive Measures
ASD Severity
The ADOS-2 (Lord et al. 2012) is a semi-structured standardized assessment for individuals referred because of possible autism. The Reciprocal Social Interaction, Communication, Play or Imagination/Creativity, and Stereotyped Behaviors and Restricted Interests algorithm subtotals from the ADOS were used as ratings of autism symptoms. The ADOS was used at baseline as a measure to confirm the diagnosis and to describe the participants.
Cognitive Functioning
To assess cognitive abilities, the Stanford-Binet Intelligence Scale-Abbreviated Battery (SB5-ABIQ 5th Ed; Roid 2003) was administered (i.e., the Nonverbal Reasoning and Verbal Knowledge) to derive the ABIQ. These subtests are normed for use with the age range of individuals included in this project and have strong psychometric properties documenting good reliability (alpha coefficients of .95 nonverbal and .96 verbal), excellent stability, and validity. The scores derived from the SB5-ABIQ have been found to be significantly correlated with several common full-scale IQ batteries (Newton et al. 2008). Because the SB5-ABIQ is normed on ages 2–85 years and has separate measures for verbal and nonverbal subtests, it is ideally suited for the heterogeneity of cognitive level in individuals with ASD.
Demographic and Social Interview
The Adult Living Interview is a 23-item interview adapted from an adult survey developed by the Florida Center for Autism and Related Disabilities (CARD 2008). This survey was originally developed to assess outcomes of young adults with ASD and focuses on issues related to employment, educational attainment, transportation, housing, and social life. For the purposes of this study, the survey was adapted to be utilized as an interview protocol and was administered at baseline and following treatment.
Outcome Measures
Mock Job Interviews/Social Pragmatic Scale
Mock job interviews were conducted pre- and post-treatment and served as the primary source of data collection. Five volunteer professionals unknown to the research participants conducted video-recorded mock interviews with scripted questions tailored to match participant career interests. Interviews were video-recorded for the purposes of conducting video review with project participants and for coding and data analysis. Interviewers were counterbalanced so that participants had a different interviewer each time. Interviews were be tailored for either entry-level or professional positions and consisted of a standardized set of questions presented in a flexible, naturalistic format.
A trained undergraduate coder blind to group assignment and interview timing scored mock interviews. Interviews were scored using the Social Pragmatic Scale (Morgan 2011), an 8- item observational tool developed for the purposes of this project. Each item was scored using a 4-point Likert scale and included items related to greetings, appearance, social interaction, and communication. Inter-observer reliability was evaluated by two coders, who independently reviewed 20 % of the video-recorded mock interviews. Intra-class correlations revealed good to excellent inter-observer agreement, ICC = .75.
Adaptive Behavior
The Vineland Adaptive Behavior Scales-II (VABS; Survey Interview Form; Sparrow et al. 2004) was selected to evaluate adaptive behavior because it yields information about abilities in the home and the community and is routinely used to assist in the diagnosis of developmental delay, mental retardation, and autism (Paul et al. 2004). It provides a standard score in four domains—Communication, Daily Living, Social, and Motor, and an Adaptive Behavior Composite. Confidence levels are reported for subdomain, domain, and Adaptive Behavior Composite standard scores. The validity of the VABS has been well established for populations with ASD (Perry and Factor 1989). The VABS was used as an outcome measure to be administered at both baseline and 6-month follow up utilizing parent rating forms.
Depressive Symptoms
The Patient Health Questionnaire-9 (PHQ-9; Spitzer et al. 1999) is a nine-item depression scale of the Patient Health Questionnaire that was used to assess symptoms to make a tentative evaluation of depression and to derive a severity score to monitor change over time. The PHQ-9 is based directly on the DSM-IV diagnostic criteria for major depressive disorder and has been used in research to document change in treatment for depression (Lowe et al. 2004) and was administered pre and post-treatment.
Data Analysis
Analyses were performed on the intent-to-treat basis. As indicated in Fig. 1, one participant allocated to the experimental condition, and three participants allocated to the control condition did not complete their allocated treatment. Although the small sample size did not allow us to impute missing data, analyses included all available data, including those from participants who failed to complete the allocated treatment. In addition, we conducted exploratory analyses to identify any systematic differences between the four participants who dropped and the 24 participants who completed the study. These exploratory analyses were independent-samples t tests for continuous variables (e.g., chronological age, ADOS scores, Abbreviated Battery IQ scores, PHQ baseline scores, baseline performance on the mock interview) and Chi square tests for categorical variables (e.g., educational attainment, ethnicity/race, diagnostic classification, living situation, educational/occupational classification). Results revealed no significant differences by attrition status, p > .10.
The main goal of this analysis was to evaluate the effect of ISC on gains in the participants’ performance during the Mock Interview between baseline and exit. In addition, we aimed to evaluate treatment effects on two distal outcomes, generalized social behaviors assessed using the Vineland and depressive symptoms assessed using the Patient Health Questionnaire. Consistent with recommendations for clinical trials (Fitzmaurice et al. 2004; Carter et al. 2011), change between baseline and exit assessments were quantified as residual gain scores. One advantage of this approach is that it can provide considerably more power to detect treatment effects than other statistical methods (see NICHD ECCRN and Duncan 2003 for a comparison of different approaches). Residual gain scores were obtained by regressing the Time 1 measure of each variable onto the later measure of the same variable. The residual errors for each subject were then used as the criterion scores quantifying change. In the context of the current study, residual gain scores answer whether a participant randomized to ISC is expected to change more than a participant in the control condition, given that they have the same initial value. Linear regression analysis revealed that baseline performance on the mock interview reliably predicted participants’ performance at exit, B = .71, SE B = .15, t(23) = 4.8, p < .001. Fifty-one percent of variability in the participants’ performance at exit can be accounted for by baseline variation in that variable. Similarly, 72 % of variation in participants’ social subscale scores on the Vineland (B = .99, SE B = .13, t(23) = 7.6, p < .001), and 81 % of variability on the depression subscale of the Patient Health Questionnaire (B = .81, SE B = .08, t(23) = 9.8, p < .001) could be attributed to baseline variation in the same variable.
Results
Preliminary Analyses
Prior to evaluating the primary hypotheses, potentially confounding variables were examined. To check that the experimental and control groups were not different at baseline, independent-samples t-tests for continuous variables (e.g., Abbreviated Battery IQ scores) and Chi square tests for categorical variables (e.g., educational attainment) were performed as appropriate. Measures considered for this analysis included baseline measures of primary outcome variables (i.e., mock interview scores, VABS social subscale scores, PHQ depression scores), socioeconomic characteristics (e.g., ethnicity/race), and baseline variables potentially associated with outcomes (e.g., chronological age, ASD symptom severity, Abbreviated Battery IQ scores, VABS scores, educational attainment, educational/occupational classification). Results from these analyses revealed no significant differences between the experimental and control groups on any of the evaluated measures, p > .10. The corresponding effect sizes are reported in Tables 1 and 3.
Evaluating Treatment Effects on Proximal Outcomes
To test the main effect of treatment group allocation on participants’ performance during the mock interview, we specified a series of t tests comparing scores between the experimental and control group. Results revealed a significant main effect of treatment group allocation on gains in participants’ performance during the mock interview from baseline to exit, t(23) = 2.14, p < .05. The effect size associated with this treatment effect was Glass’s delta = .87, which is conventionally considered to be a large effect. Detailed results from this analysis are reported in Table 3. Due to the relatively small sample size, we used a nonparametric Mann–Whitney U test to confirm this key finding. Distributions of residual gain scores for the experimental and control condition were similar, as assessed by visual inspection. Results showed that the median residual gain score was significantly higher in the experimental (.80) than in the control (−1.06) condition, U = 34.5, z = −2.17, p < .05.
Evaluating Treatment Effects on Distal Outcomes
For this analysis, we considered two distal outcomes, the social composite of the Vineland Adaptive Behavior Scale and the depression scale of the Patient Health Questionnaire. To test the main effect of treatment group allocation on participants’ scores on both measures, we specified a series of t tests comparing scores between the experimental and control group. Results revealed that the Vineland social composite score of participants randomized to the experimental group increased from 78.46 (SD = 10.95) to 81.67 (SD = 13.38) between baseline and exit assessments. In contrast, the Vineland social composite score of participants randomized to the control group remained rather stable, 79.17 (SD = 8.65) and 79.42 (SD = 9.75), respectively. Although this treatment effect was not statistically significant, t(23) = 1.26, p = .23, the Glass’s delta coefficient revealed a large effect size (Glass’s delta = 1.09). It is notable that variability of gain scores in the experimental condition (SD = 7.97) was significantly larger than in the control condition (SD = 2.83), F(11,11) = 7.9, p < .01. Increased variability in the experimental group may indicate that distal treatment effects may only be evident in some but not other participants. Detailed results from this analysis are reported in Table 3.
Results also revealed that self-reported depressive symptoms of participants randomized to the experimental group decreased from 7.69 (SD = 5.79) to 5.42 (SD = 3.90) between baseline and exit assessments. In contrast, the depressive symptoms of participants randomized to the control group remained rather stable, 7.86 (SD = 6.56) and 7.92 (SD = 6.01), respectively. Although this treatment effect was not statistically significant, t(23) = 1.20, p = .24, the Glass’s delta coefficient revealed a medium effect size (Glass’s delta = −.55).
Discussion
The results of this study provide preliminary evidence supporting the efficacy of ISC for young adults with ASD. Specifically, adults randomly assigned to the experimental group showed larger gains in social–pragmatic skills observed during a mock job interview than adults assigned to the control group. Due to the small sample size, results from analyses evaluating distal outcomes are inconclusive. That is, treatment effects on social adaptive behaviors and depressive symptoms were not significant, although the respective effect sizes were medium/large. These findings are encouraging and suggest that a brief, low-intensity treatment can improve the job-interview performance of young adults with ASD.
Due to the fact that the bulk of research on adults with ASD has been descriptive in nature, mention of characteristics of this sample is warranted prior to a discussion of treatment results. Forty-three percent of study participants reporting being unoccupied (e.g. neither enrolled in school or employed) at baseline. This figure is much higher than previously reported rates of about 24 % for high functioning adults with ASD (Renty and Roeyers 2006; Taylor and Seltzer 2011). Just over half of this sample reported participation in work and/or education at baseline. It is notable that out of the 16 individuals who reported having ever been employed, almost half reported having lost employment due to difficulties following company policies or practices, getting along with others, or keeping up with demands. In addition, greater than half of the sample reported living with parents and 64 % reported experiencing depressive symptoms. Although this sample is without intellectual disability, these data describe a group of young adults with ASD that continues to experience significant struggles and are consistent with recent longitudinal research findings reporting on outcomes of adults with ASD (Howlin et al. 2004; Orsmond et al. 2013; Roux et al. 2013).
Participants who were randomized to ISC demonstrated significant improvement in interview skills in comparison to IQ-matched control participants. This finding is unique within the small body of adult intervention literature in that studies have either lacked inclusion of a behavioral observation to evaluate intervention effects (e.g. Gantman et al. 2012) or studies have included such a measure with no observed effect (Turner-Brown et al. 2008). This treatment effect is important because it provides evidence of generalization of learning acquired during the intervention sessions to a novel context requiring interactions with unfamiliar communicative partners.
Vineland social composite results demonstrated improvement for participants randomized to the experimental group whereas the control group’s performance on this measure remained stable. Although this treatment effect was not statistically significant, the large effect size (Glass’s delta = 1.09) provides substantive information as to the potential for change. The lack of significance is not surprising given the relatively small sample size and variability present in the treatment group indicating that an intervention effect on this measure may only be evident select participants. Research indicating that individuals with autism show significant impairment on the Vineland in the presence of normal intelligence (Klin et al. 2007) and evidence that those with higher functioning ASD become increasingly impaired with age, suggest adaptive skills as a priority area for treatment (Klin et al. 2007). Give the large effect size we detected, we are encouraged about this preliminary result that may be validated in further study of the ISC.
Self-report of depression symptoms via the Patient Health Questionnaire indicated reduction, albeit nonsignificant, in depressive symptoms for participants in the ISC condition. It is possible that participation in ISC and increased access to peers contributed to these reported improvements. Due to consistent reports of very high levels of mental health concerns of adults with ASD, particularly that of depression in those with IQ in the normal range (e.g. Sterling et al. 2008) our detection of a medium effect size for participants of ISC is encouraging and warrants further evaluation.
Along with the encouraging results reported here, several limitations should not be overlooked. First, these effects represent measurement of skills shortly following the 12-week ISC intervention. In order to evaluate stability of gains, longer-term follow up and assessment of participants is required. Information on participants’ other treatments and services being received was not collected nor did we collect detailed information on changes in social behavior and relationships following study participation. Inclusion of a protocol for evaluating change in social and employment status would provide relevant information regarding effects of treatment as well as a mechanism for the intervention to bolster individualized support to participants.
In summary, the results of this study provide support for the ISC as an effective program for young adults with ASD by demonstrative positive, short-term effects on interview skills. Such demonstrable change may be critical to influence longer-term adult outcomes in a positive direction and future research to document these potential effects is warranted. Specifically, future research should seek to establish whether short-term treatment effects generalize to distal measures of social adaptive functioning and mental health and whether these changes are mediated by short-term changes in job interview skills. Ultimately whether ISC has the potential to influence young adults ability to procure employment should also be evaluated.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revision). Washington, DC: American Psychiatric Association.
Barnard, J., Harvey, V., Potter, D., & Prior, A. (2001). Ignored or ineligible? The reality for adults with autism spectrum disorders. London: National Autistic Society.
Carter, A. S., Messinger, D. S., Stone, W. L., Celimli, S., Nahmias, A. S., & Yoder, P. (2011). A randomized controlled trial of Hanen’s ‘More than Words’ in toddlers with early autism symptoms. Journal of Child Psychology and Psychiatry, 52(7), 741–752.
Centers for Autism and Related Disabilities. (2008). Adult Living Survey. Miami, FL (Unpublished survey).
Centers for Disease Control and Prevention. (2012). Prevalence of autism spectrum disorders—Autism and developmental disabilities monitoring network, 14 sites, United States, 2008. Surveillance Summaries, MMWR, 61(SS03), 1–19.
Chadsey-Rusch, J. (1992). Toward defining and measuring social skills in employment settings. American Journal of Mental Retardation, 96, 405–418.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Erlbaum.
Committee, Interagency Autism Coordinating. (2012). Strategic plan for autism spectrum disorder research: 2012 update. Bethesda, MD: National Institutes of Health, Office of Autism Research Coordination.
Corcoran, R., Mercer, G., & Frith, C. D. (1995). Schizophrenia, symptomatology and social inference: Investigating “theory of mind” in people with schizophrenia. Schizophrenia Research, 17(1), 5–13.
Cotter, M. W. (1997). Improving the social behavior of high-functioning children with autism: A social skills support group intervention. Unpublished doctoral dissertation, University of Alabama.
Early Child Care Research Network, N.I.C.H.D., & Duncan, G. J. (2003). Modeling the impacts of child care quality on children’s preschool cognitive development. Child Development, 74, 1454–1475.
Fitzmaurice, G. M., Laird, N. M., & Ware, J. H. (2004). Applied longitudinal analysis. Hoboken, NJ: Wiley-Interscience.
Gantman, A., Kapp, S. K., Orenski, K., & Laugeson, E. A. (2012). Social skills training for young adults with high-functioning autism spectrum disorders: A randomized controlled pilot study. Journal of Autism and Developmental Disorders, 42, 1094–1103.
Gerhardt, P., & Lanier, I. (2011). Addressing the needs of adolescents and adults with autism: A crisis on the horizon. Journal of Contemporary Psychotherapy, 41, 37–45.
Hillier, A., Fish, T., Cloppert, P., & Beversdorf, D. Q. (2007). Outcomes of a social and vocational skills support group for adolescents and young adults on the autism spectrum. Focus on Autism and Other Developmental Disabilities, 22(2), 107–115.
Howlin, P. (2000). Outcome in adult life for more able indivdiuals with autism or Asperger syndrome. Autism, 4, 63–83.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45(2), 212–229.
Howlin, P., Mawhood, L., & Rutter, M. (2000). Autism and developmental receptive language disorder—A follow-up comparison in early adult life. II: Social, behavioural, and psychiatric outcomes. Journal of Child Psychology and Psychiatry, 41, 561–578.
Howlin, P., & Yates, P. (1999). The potential effectiveness of social skills groups for adults with autism. Autism, 3(3), 299–307.
Jennes-Coussens, M., Magill-Evans, J., & Koning, C. (2006). The quality of life of young men with Asperger syndrome. Autism, 10(4), 403–414.
Klin, A., Saulnier, C. A., Sparrow, S. S., Cicchetti, D. V., Volkmar, F. R., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal of Autism and Developmental Disorders, 37(4), 748–759.
Laugeson, E. A., & Frankel, F. (2010). Social skills for teenagers with developmental and autism spectrum disorders: The PEERS treatment manual. New York: Routledge.
Laugeson, E. A., Frankel, F., Gantman, A., Dillon, A. R., & Mogil, C. (2012). Evidence-based social skills training for adolescents with autism spectrum disorders: The UCLA PEERS program. Journal of Autism and Developmental Disorders, 42, 1025–1036.
Liptak, G. S., Kennedy, J. A., & Dosa, N. P. (2011). Social participation in a nationally representative sample of older youth and young adults with autism. Journal of Developmental and Behavioral Pediatrics, 32, 277–283.
Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism Diagnostic Observation Schedule-II. Los Angeles, CA: Western Psychological Services.
Lowe, B., Unutzer, J., Callahan, C. M., Perkins, A. J., & Kroenke, K. (2004). Monitoring depression treatment outcomes with the Patient Health Questionnaire-9. Medical Care, 42(12), 1194–2001.
Mawhood, L., & Howlin, P. (1999). The outcome of a supported employment scheme for high functioning adults with autism or Asperger syndrome. Autism, 3(229), 254.
McGovern, C., & Sigman, M. (2005). Continuity and change from early childhood to adolescence. Journal Child Psychology and Psychiatry, 46(4), 409–419.
Mesibov, G. (1985). Social skills training with verbal autistic adolescents and adults: A program model. Journal of Autism and Developmental Disorders, 14, 395–404.
Morgan, L. (2011). Social Pragmatic Scale. Unpublished manual, Florida State University, Tallahassee, FL.
Newton, J. H., McIntosh, D. E., Dixon, F., Williams, T., & Youman, E. (2008). Assessing giftedness in children: Comparing the accuracy of three shortened measures of intelligence to the Stanford-Binet Intelligence Scales, 5th edition. Psychology in the Schools, 5(6), 523–536.
Orsmond, G. I., Shattuck, P. T., Cooper, B. P., Sterzing, P. R., & Anderson, K. A. (2013). Social participation among young adults with an autism spectrum disorder. Journal of Autism and Developmental Disorders, 43, 2710–2719.
Ozonoff, S., & Miller, J. N. (1995). Teaching theory of mind: A new approach to social skills training for individuals with autism. Journal of Autism and Developmental Disorders, 25, 415–433.
Paul, R., Miles, S., Cicchetti, D., Sparrow, S., Klin, A., Volkmar, F., et al. (2004). Adaptive behavior in autism and pervasive developmental disorder-not otherwise specified: Microanalysis of scores on the Vineland Adaptive Behavior Scales. Journal of Autism and Developmental Disorders, 34, 223–228.
Perry, A., & Factor, D. C. (1989). Psychometric validity and clinical usefulness of the Vineland Adaptive Behavior Scales and the AAMD Adaptive Behavior Scale for an autistic sample. Journal of Autism and Developmental Disorders, 19(1), 41–55.
Provencal, S. L. (2003). The efficacy of a social skills training program for adolescents with autism spectrum disorders. Unpublished doctoral dissertation, University of Utah.
Renty, J., & Roeyers, H. (2006). Quality of life in high-functioning adults with autism spectrum disorder. Autism, 10(5), 511–524.
Resnick, B., Inguito, P., Orwig, D., Yahiro, J. Y., Hawkes, W., Werner, M., et al. (2005). Treatment fidelity in behavior change research: A case example. Nursing Research, 54(2), 139–143.
Roberts, D. L., Penn, D., & Combs, D. R. (2004). Social cognition and interaction training. Unpublished Treatment Manual.
Roid, G. H. (2003). Stanford-Binet Intelligence Scales (5th ed.). Itasca, IL: Riverside.
Roux, A. M., Shattuck, P. T., Cooper, B. P., Anderson, K. A., Wagner, M., & Narendof, S. A. (2013). Postsecondary employment experiences among young adults with an autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 52(9), 931–939.
Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and quasi-experimental designs for generalized causal inference. Boston: Houghton Mifflin.
Shtayermman, O. (2007). Peer victimization in adolescents and young adults diagnosed with Asperger’s syndrome: A link to depressive symptomatology, anxiety symptomatology, and suicidal ideation. Issues in Comprehensive Pediatric nursing, 30, 87–107.
Sigman, M., & McGovern, C. W. (2005). Improvement in cognitive and language skills from preschool to adolescence in autism. Journal of Autism and Developmental Disorders, 35(1), 15–23.
Sparrow, S., Balla, D., & Cicchetti, D. (2004). Vineland-II Adaptive Behavior Scales. Circle Pines, MN: American Guidance Service.
Spitzer, R., Kroenke, K., & Williams, J. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Journal of the American Medical Association, 282, 1737–1744.
Sterling, L., Dawson, G., Estes, A., & Greenson, J. (2008). Characteristics associated with the presence of depressive symptoms in adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 38(6), 1011–1018.
Szatmari, P., Bartolucci, G., & Bremner, R. (1989). Asperger’s syndrome and autism: Comparison of early history and outcome. Developmental Medicine and Child Neurology, 1(6), 709–720.
Taylor, J. L., & Seltzer, M. M. (2011). Employment and post-secondary educational activities for young adults with autism spectrum disorders during the transition to adulthood. Journal of Autism and Developmental Disorders, 41, 566–574.
Turner-Brown, L. M., Perry, T. D., Dichter, G. S., Bodfish, J. W., & Penn, D. L. (2008). Brief report: Feasibility of social cognition and interaction training for adults with high functioning autism. Journal of Autism and Developmental Disorders, 38, 1777–1784.
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up study of high-functioning autistic children. Child Psychology and Psychiatry and Allied Disciplines, 33(3), 489–507.
Webb, B. J., Miller, S. P., Pierce, T. B., Strawser, S., & Jones, W. P. (2004). Effects of social skill instruction for high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19, 53–62.
Whitehouse, A. J., Durkin, K., Jaquet, E., & Ziatas, K. (2009). Friendship, loneliness and depression in adolescents with Asperger’s syndrome. Journal of Adolescence, 32, 309–322.
Williams-White, S., Keonig, K., & Scahill, L. (2007). Social skills development in children with autism spectrum disorders: A review of intervention research. Journal of Autism and Developmental Disorders, 37, 1858–1868.
Acknowledgments
Preparation of this article was supported by a Pilot Treatment Grant (#7454, PI Lindee Morgan) from Autism Speaks. We are deeply grateful for the study participants and their families. We also wish to acknowledge the support and assistance of Holly Dickinson, Lauren Propst, Kim McShane, Kathy Watkins, Steve Barnes, Shirley Nicoll, Karen Robins, Marisa Laughrey, Sarah Richter, Joy Moore, Susan Baldino, Jazmin Caton, Michael Landing, Bryan Schultz, Patricia Armstrong, and Amy Wetherby.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morgan, L., Leatzow, A., Clark, S. et al. Interview Skills for Adults with Autism Spectrum Disorder: A Pilot Randomized Controlled Trial. J Autism Dev Disord 44, 2290–2300 (2014). https://doi.org/10.1007/s10803-014-2100-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2100-3