
Abstract
With the approaching release of the DSM V in 2013, there has been much debate about the proposal to remove the diagnostic label of Asperger’s disorder from the new DSM. This study explored how health and education professionals perceive the conditions of autism and Asperger’s disorder and their views on the proposed diagnostic changes. Analysis of the 547 participant responses confirmed an increase stigma is associated with the label of autism, with autism considered to be a more severe than the condition of Asperger’s disorder. Approximately half of the participants reported being opposed to proposed diagnostic changes and of the remaining participants, 22 % supported the proposed changes and 28 % expressed uncertainty.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The classification of mental health disorders has been well documented over the years with many nomenclatures being developed. Whilst initially this labelling of mental health disorders was aimed at improving the accuracy of statistical data collected in relation to mental illness, it resulted in mental health disorders being incorporated in the International Statistical Classifications of Diseases and Related Health Problems—Version 6 (World Health Organisation 1992) and the first formal Diagnostic and Statistical Manual of Mental Disorders (DSM) in 1952 (American Psychiatric Association 2000). Over time, the DSM’s categorical description of mental illness symptoms has become one of the key mental health diagnostic guides for those in research, medical, psychological, forensic and social welfare fields (Kupfer et al. 2008). The importance of this labelling system has also extended beyond researchers and clinicians, to general community members with DSM diagnostic labels of anxiety, ADHD and depression being routinely mentioned in community discussions and media reports. Diagnostic labels can be influential in accessing services and funding, such as Australian’s access to psychological therapy through the Medicare system being dependent on diagnosis of specific mental health conditions (Fletcher et al. 2011; MacCulloch 2010) and access to support services in education settings generally relying on children having specific diagnostic labels (Skellern et al. 2005). Within the context of autism and Asperger’s disorder, Australian families with children under 7 years of age diagnosed with pervasive developmental disorders are currently eligible for up to $12,000 of private therapy services (Australian Government 2008).
Given this dependency on the labelling system for mental health disorders in western society and the fact that there has been nearly 60 years of diagnostic labelling, it could be assumed that reviewing and updating of the DSM would be a relatively straight forward process. However unlike the clarity that exists in diagnosing physical ailments, the interpretation of what a mental illness is and how it is defined is subjective. Social norms as well as evolving research recommendations can change the diagnostic criteria for mental illness. Historical evidence suggests that new disorders can be identified, previously defined disorders can be split into new subtypes, two or more previously defined disorders can be merged into one disorder and disorders can be removed from diagnostic manuals (Rogler 1997).
A current example of changes to the labelling of mental health conditions is found in the proposal to change the Pervasive Developmental Disorder criteria in the DSM. The currently used DSM IV-TR description of Pervasive Developmental Disorders includes the conditions of Autistic Disorder (autism), Asperger’s Disorder, Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS), Rett’s Disorder and Childhood Disintegrative Disorder. Of these five conditions, autism, Asperger’s disorder and PDD-NOS have specific areas of diagnostic commonality in relation to impairments in social interaction skills and restricted patterns of stereotyped behaviours or interests (American Psychiatric Association 2000).
Since the inclusion of Asperger’s disorder in the DSM in 1994, there has ongoing controversy about the Asperger’s disorder label (Ghaziuddin 2010). Questions have been raised about the distinctiveness of Asperger’s disorder from autism (Macintosh and Dissanayake 2006; Sanders 2009) and the increasing diagnostic rates of pervasive developmental disorders since the introduction of Asperger’s disorder into the DSM and increasing diagnostic rates of pervasive developmental disorder conditions (Wing et al. 2011). Consequently, a proposal to combine the conditions of autism, Asperger’s disorder, childhood disintegrative disorder and PDD-NOS into the one diagnostic label of Autistic Disorder (Autism Spectrum Disorder) was first officially circulated by the American Psychiatric Association in 2009. The current revised proposal gives preference to the label of Autism Spectrum Disorder and includes a severity rating scale (American Psychiatric Association 2011). It is suggested that this new condition will be introduced in the DSM V, which is due for release in 2013 (American Psychiatric Association 2011), with the view that it may reduce some of the confusion caused by the current range of diagnostic terms describing pervasive developmental disorders (Wallis 2009).
This convergence of diagnostic categories essentially removes the term of Asperger’s disorder from the official diagnostic criteria (Swedo 2009) and has resulted in debate (Ghaziuddin 2010; Lecavalier et al. 2009; Wing et al. 2011) reflecting the previously documented arguments for and against the use of categorical diagnostic labels in society (Corrigan 2007). In the arguments against the use of diagnostic labels, linguistic and social psychology advocates suggest that labels produce negative evaluations, stereotypes and stigma’s (Corrigan 2007; Eiser and Mower-White 1976), whilst self-reported client-based studies have proposed diagnostic labels can be beneficial by “providing orientation for those afflicted and their relatives” (Angermeyer and Matschinger 2003, p. 304).
In the ensuring debate on the proposed DSM changes associated with Asperger’s disorder, concern has been raised that the negative connotations associated with the term of ‘autism’ in the proposed new label of ‘Autism Spectrum Disorder’, will discourage families of those with milder symptoms of autism spectrum conditions from seeking a diagnosis under the new label (Wallis 2009). Despite the paucity of literature exploring the stigma associated with the conditions of autism and Asperger’s disorder, research (Kite et al. 2011) has suggested that the term Asperger’s disorder currently has a relatively positive perception in society (Wallis 2009). This positive perception is founded on reports that link Asperger’s disorder and ‘geniuses’ such as “Bill Gates, Albert Einstein and Thomas Jefferson” (Hough 2006, p. 166). The relatively positive perception of Asperger’s disorder is in contrast to the link between the condition of autism with language delays and intellectual disability (Gillberg and Enlers 1998). The stigma and stereotyping of autism is potentially compounded by media reports of children diagnosed with autism engaging in volatile behaviour such as head banging and running away (Earley 2009), as well as reports of schools placing children diagnosed with autism in “cages” (Doherty 2009, p. 1) to protect them from bullying and leaving the school grounds.
Reports of diagnostic labels giving rise to differing levels of stigma and stereotyping are relatively common. For example, jurors have reported experiencing a greater negative affect from the label of psychopath than the term of conduct disorder (Bocaccini et al. 2008) and community members have reported experiencing an increased sense of fear and negative affect from the label of schizophrenia than that of depression (Angermeyer and Matschinger 2003). Further to this, research on the impact of labels on professional perceptions have found that when “a diagnostic label is revealed to a teacher before the teacher meets the child with a disability, it may create unnecessary worries and elicit misconceptions” (Huang and Diamond 2010, p. 178). These concerns have been found in studies involving student teachers, in which they have indicated a reluctance to have children with behavioural labels in mainstream education systems (Stinnett et al. 1999) as well as studies of experienced teaching staff, in which they have reported an increased sense of discomfort when presented with a child with a diagnostic label (Huang and Diamond 2010). It is not surprising then that professionals’ familiar with Asperger’s disorder, including psychiatrists and paediatricians, have expressed some concern about the possibility of negative connotations associated with the new label (Ghaziuddin 2010; Lenne and Waldby 2011).
In contrast, some people diagnosed with Asperger’s disorder have commented that they already embrace the Autism Spectrum Disorder term and do not have any concerns with the proposed changes (Autism Support Group 2010; Wallis 2009). This identification with the Autism Spectrum label possibly reflects the positive aspects that having a diagnostic label can provide, with the label providing an orientation point to make sense of difficulties, forming a basis for improved understanding, increasing the desire to seek appropriate supports and in providing a guide around possible outcomes (Elfant 1985; Holm-Denoma 2008).
Whilst specialist committees have been consulted in the development of the new DSM criteria (American Psychiatric Association 2010) and a range of individual comments have been made about the proposed changes in the media, on websites and recently in journal articles, there is currently a lack of research exploring the views held about these proposed changes. Given the increasing growth in interest in the topic of Asperger’s disorder, with a Google search in early 2012 indicating over 9½ million topics on the subject, the current research aimed to explore the views of the proposed diagnostic changes. More specifically, the study explored views held about the proposed DSM diagnostic changes and differences between the conditions of autism and Asperger’s disorder. This study constitutes a section of a larger project exploring the perception of Asperger’s disorder, with only the views held by health and educational professionals reported here.
Method
Participants
A total of 547 Australian health and education professionals returned the questionnaire. The majority of participants were female (90 %), with an average age of 45 years (SD 11.64). The 376 health professionals consisted of 126 psychologists, 75 speech pathologists, 61 nurses, 43 social workers and 71 other health professionals. The ‘other health professional’ group consisted of a range of medical and allied health professionals who did not have enough participants within their particular professional field to form their own occupational group in this study. The remainder of the participants were made up of 171 education professionals.
Questionnaire
The questionnaire for the larger research project consisted of six sections, with this study focusing on the results from Section 6. This section asked participants if they thought there was a difference between the conditions of autism and Asperger’s disorder, with participants responding using a Yes/No answer. Participants who responded ‘yes’ were invited to rate on a scale of 0 (no impact) to 5 (extreme impact) the extent that they felt a diagnosis of Asperger’s disorder would firstly impact on the child and then on the family. Participants were then invited to answer the same questions about the perceived impact on the child and family in relation to the diagnosis of autism.
A short description of the proposal to combine autism and Asperger’s disorder into the one diagnostic category in the new DSM was then presented, with the introductory statement stating;
There is currently a major review of the criteria for diagnosing mental illness and disabilities. One of the proposed changes is to combine autism and Asperger’s syndrome into the one category, called Autistic Disorder (Autism Spectrum Disorder).
This was followed by a question asking participants if they thought autism and Asperger’s should be combined into the one diagnosis, responding using a Yes/No/Don’t know format. The use of the terminology Autistic Disorder (Autism Spectrum Disorder) was consistent with the initial proposal released in 2009 for the DSM changes (American Psychiatric Association 2009), when the questionnaire was initially designed. A free text narrative option was available for participants to explain their reasons for supporting, objecting to or expressing uncertainty about the proposed changes in the diagnostic criteria.
Procedure
The same procedure as described in Kite and Tyson (2011a, b) was used, with ethics approval obtained, then an email sent inviting participation in the study by accessing a link to an online questionnaire. Paper versions of the questionnaire were also distributed to three private education settings, three medical centres and through the Specific Learning Difficulties Association of South Australia.
Results
Perceived Differences Between Autism and Asperger’s Disorder
Of the 547 health and education professionals who participated in this research, 491 responded to the question “Do you think there is a difference between autism and Asperger’s disorder”; with 93.4 % of participants indicating that they thought there was a difference between the conditions of autism and Asperger’s disorder. Across the health professionals, between 96 and 97 % of the social workers, speech pathologists and nurses and just over 90 % of the psychologists indicated that there was a difference between the conditions. No significant difference in response rates were found using Pearson’s Chi square test of contingencies across the various groups, χ2 (2, 491) = 4.897, p = .298).
The 456 participants who positively endorsed that there were differences between the conditions of autism and Asperger’s disorder were invited to answer questions relating to the perceived severity of these conditions. These participants indicated that they viewed the conditions of autism and Asperger’s disorder to have a relatively severe impact on the child (M = 4.52, SD = .78 and M = 4.19, SD = .82 respectively) and the child’s family (M = 4.67, SD = .59 and M = 4.35, SD = .70 respectively), with significantly negatively skewed results. Due to the marked violation of the normality assumption in the data from the extreme negative skewing, the Wilcoxon signed rank non-parametric procedure was used to compare the results. The analyses found participants perceived the condition of autism to have a significantly greater impact on the child than Asperger’s disorder (z = 9.10 (corrected for ties), p < .001, two tailed) and on the family (z = −10.61 (corrected for ties) p < .001, two tailed). The effect sizes were considered to be large (r = .41 and r = .48 respectively).
Proposed Diagnostic Changes
The participants were requested to indicate either ‘yes, no or don’t know’ response to a question asking if they thought the diagnostic labels of Asperger’s disorder and autism should be combined. Overall the results indicated that 50.2 % of participants objected to the proposed change, 22.6 % supported the change and 27.6 % indicated that they did not know if the conditions should be combined. There was no association between the education and health professionals’ response towards change (χ2 (2, 496) = 0.20, p = .91).
To further explore participants’ reasons for supporting or opposing the proposed DSM diagnostic changes, participants were invited to provide a free text description of their reasons for their responses about the proposed changes.
Content analysis using an a priori coding system was used to examine the frequency of selected comments made by participants in their free text comments. The a priori coding method, in which the coding categories were established before examining the data (Bernard and Ryan 2010), was used as a repetitive range of reasons have been proposed by professionals and in online computer based social networks for supporting or objecting to the proposed diagnostic changes. Drawing from established literature, the reasons suggested for objecting to the proposed changes; include the conditions being perceived to have different needs, different management and support strategies, different prognosis and associated needs into adulthood (Admin 2011), different severity levels between the conditions (Admin 2011; Ghaziuddin 2010; Kite et al. 2011; Wallis 2009), different causes (Isus 2011) and a negative stigma (Kite et al. 2011; Wallis 2009), as well broad comments identifying the conditions as just being different (Admin 2011; Henrysdad 2010).
The literature based arguments in favour of changes in the diagnostic criteria include; the conditions being described as being part of the same condition (Lopez-Duran 2010), opportunities for improved service access (Bubbles 2011; William and Mary 2011), decreased confusion between the labels (Wallis 2009) and increased recognition of the condition (Julie 2011). Given the documented reoccurrence of these comments by individuals expressing their views on the proposed change, yet the current lack of exploration of these views across larger population groups, it was decided by the principal author that developing an a priori coding method based on the previously documented arguments would assist in establishing a clearly defined coding system that was relevant to the current debate (Sproule 2010).
From reviewing the previously mentioned literature, seven codes were identified as potential reasons for objecting to the proposed diagnostic changes and four codes were identified as potential reasons to support the diagnostic changes. These eleven codes are displayed in Tables 1 and 2 respectively, with a selection of key words associated with the described codes. These associated words formed the basis of the codebook to guide the coding system. After developing the coding system an initial review of approximately 5 % of the free text comments was made by the principal author to review the validity of the selected codes for analysing the comments. From this review, it was considered that the overall eleven coding categories were appropriate with additional key words added to the final code framework e.g. cognitive as well as intellectual and intelligence under the characteristics code.
Whilst a range of labels have been reported to be used in describing the conditions of autism and Asperger’s disorder previously (Attwood 1998; Ghaziuddin 2010; Kite et al. 2011; Wallis 2009), the vast array of terms used in this study included; autism, the spectrum, spectrum, autism family, Asperger, Asperger’s, aspergers, Asperger Syndrome, ASD, Autism Spectrum, Autism Spectrum Disorder (Atypical), Autism Spectrum Disorder, spectrum scale, autistic, High Functioning Autistic, AS, Pervasive Developmental Disorder, PDD-NOS, Autistic Disorder, HFA, LFA, Aspbergers and Austism. Some participants also appeared to have developed their own language using terms of ASDian people and Aspergains. Given the range of terminology used by participants to describe autism and Asperger’s disorder in their free text responses, it was decided by the principle author that the coding would be conducted manually rather than through the use of computer based coding systems. The manual coding method was considered to enable increased flexibility around the range of terms, spelling and grammar used by participants (Sproule 2010).
To increase reliability of the coding, the principal author and a second independent rater, who was unfamiliar with the research topic, used the coding system to identify the frequency of codes across the data set. Cohen’s kappa indicated that the inter-rater scores had an adequate to high level of reliability, with the scores across all codes being 0.74 or above. Given the satisfactory level of inter-rater reliability the coding of the principal author was used for the analyses. Table 1 displays the code headings and frequencies of the responses reported as a percentage of the total responses.
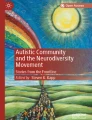
As displayed in Table 1 the most frequently occurring comments against the proposed diagnostic changes related to the perception of autism and Asperger’s disorder being different conditions, having different characteristics and intervention needs. The high frequency in responses relating to differences between the conditions is in contrast to the low frequency of responses about the conditions having different causes and prognosis. Due to the extremely low frequency of responses for the codes relating to different causes and prognosis, it was decided by the authors to remove the two lowest frequency scores before examining the responses provided by the specific groups. This resulted in five codes being considered, with the frequency of responses provided by each group displayed graphically, using a percentage scale in Fig. 1.

Frequency (expressed as %) of responses made within the groups objecting to the proposed DSM changes
As displayed in Fig. 1, the health and education professionals’ tend to use a combination of broad comments about the conditions being different as well as making more specific comments relating to the conditions having different characteristics and intervention needs. What was notable was that many of the professional participants struggled to clearly articulate the nature of the differences between the conditions. This is evident in the following extract of comments from participants:
-
P(231): There is quite a difference between the two and I feel this should remain distinct. (Speech Pathologist)
-
P(962): Since AS is on the autism spectrum, it is different from other ASD. (Social Worker)
-
P(619): I feel the conditions are different, although they share similar behaviours (Teacher)
-
P(289): Asperger’s syndrome and autism have their unique features. It is just like you can’t combine ADHD and ODD together (Psychologist)
Given the professional debate that has occurred over the past decade around the similarities and differences between these conditions (Cuccaro et al. 2007; Ghaziuddin 2005; Macintosh and Dissanayake 2006), it is not considered surprising that participants in this study found it difficult to explicitly clarify the differences between the conditions, despite their clear objection to the proposed diagnostic changes.
The frequency of participant responses to the four coded reasons for supporting changes in the DSM diagnostic criteria are displayed in Table 2 and graphically displayed in Fig. 2.

Frequency (expressed as %) of responses made within the groups for supporting changes in the DSM
As reported in Table 2 and graphically displayed in Fig. 2 the high frequency of responses relating to the conditions of autism and Asperger’s disorder being the same or part of the same condition was consistent across the health and education groups. Even though only 22.2 % of the participants in this study indicated having outright support for the proposed changes in the diagnostic criteria, the ease by which the health and education professionals used the ‘spectrum’ term in their comments highlights the general acceptance that has occurred over the past few years in this terminology and is consistent with the increasing use of the spectrum terminology within articles and publications (Macintosh and Dissanayake 2006; Paxton and Estay 2007). This ease in the use of the spectrum terminology is evident in the following extracts:
-
P(162) Aspergers could be at one end of the spectrum, that is, high functioning autism and low functioning autism at the other (psychologist)
-
P(77) The spectrums that are proposed for classification systems better reflects clinical presentations (psychologist)
-
P(349) Aspergers is on part of the spectrum (teacher)
-
P(270) Because it is a spectrum disorder (speech pathologist)
-
P(381) My understanding is that Asperger’s syndrome is on the spectrum of autism (social worker)
The second most frequent comment made by participants in their support for the proposed changes to the DSM related to the changes being viewed to be beneficial in streamlining and gaining services for clients with Asperger’s disorder. Given the previously documented need for increased support services for those with Asperger’s disorder in education settings (Brewin et al. 2008; Little 2003) it is not surprising that education professionals have highlighted a hope that the diagnostic change will result in the potential for increased services. The following extracts from education professionals reflect the hope associated around the streamlining of services:
-
P(378) There would probably be more help for Asperger’s if both are under the same umbrella. There is probably more help given to Autistic children.
-
P(449) The Asperger children may be helped by being able to access formal support which is accorded to autistic children. (teacher)
-
P(484) People with Asperger’s syndrome have a lot of difficulty accessing services that are available for those with Autism. Combining them into one diagnosis would enable more people to receive help and support in schools and for adults who find it extremely difficult to receive support (teacher)
Access to increased support from the new label may not, however, automatically be the case as the Australian Government’s Early Intervention for Autism program currently provides access to the same level of funding for the conditions of autism, Asperger’s disorder and PDD-NOS for children up to 7 years of age (Australian Government 2008). Hence, the health professionals subsequent lower frequency of responses in relation to increasing access to services may reflect greater knowledge about current service access, resulting in a less optimistic view of the new label increasing service access.
In the free text comments, only four health professionals and two education professionals who indicated that they did know if the changes in the diagnostic criteria should occur responded with a free text comment. Due to the small number of comments provided, it was decided that no meaningful information relevant to the current research area could be obtained by analysing these comments.
General Discussion
Overall the results of this study indicate that, despite participants perceiving a difference between the conditions of autism and Asperger’s disorder, they are divided in whether the two conditions, should be combined into the proposed new diagnostic label of Autism Spectrum Disorder. In this study, approximately half of the participants did not support the proposed diagnostic changes, with the remaining participants divided between supporting the changes (22) and not being able to form a clear opinion (28 %). The most frequently occurring comments made by the health and educational professionals against the proposed diagnostic changes related to the perception of autism and Asperger’s disorder being different conditions, with different characteristics and intervention needs. The most frequent comment in support of the diagnostic change overwhelmingly related to the conditions being viewed as being the same/within the same spectrum. This was followed by educational professionals’ demonstrating a perception of greater service access being possible from the diagnostic label change.
In general, the divide between support for, arguments against and uncertainty about the proposed changes, are relatively consistent with the debate that has been apparent in computer chat services and in media articles, since early 2009 when the proposed changes to the DSM-IV-TR Pervasive Developmental Disorder criteria were circulated for public review and comment (American Psychiatric Association 2009). In the present study, the most frequent reasons given by health and educational professionals objecting to and supporting the proposed diagnostic changes are considered to reflect the ongoing literature debate about the differences (Ghaziuddin 2005, 2008) and similarities (Barbaro and Dissanayake 2007; Cuccaro et al. 2007; Macintosh and Dissanayake 2006) between the two conditions. These arguments about the positive and negative aspects associated with using diagnostic labels are consistent with the pro-con debate that has existed around diagnostic label use since Rosenhan’s article on being sane in insane places was published in the 1970’s (Rosenhan 1973).
In the current study the finding that the condition of autism has a greater impact on the child and family than that of Asperger’s disorder is consistent with the concerns raised about the autism label having a more negative connotation attached to it than that of the Asperger’s disorder label. This research result is consistent with Kite et al.’s (2011) focus group findings relating to differing perceptions being attached to these conditions, with Asperger’s disorder being viewed more favourably through links to high achievers in society (Hough 2006). These findings are also consistent with previous research identifying that differing DSM disorders can give rise to differing perceptions and levels of stigma (Angermeyer and Matschinger 2003; Bocaccini et al. 2008).
Whilst the amalgamation of autism and Asperger’s disorder into the one condition of Autism Spectrum Disorder, potentially may eliminate biased perceptions between the labels of autism and Asperger’s disorder, the introduction of the severity scale associated with the proposed new Autism Spectrum Disorder label does indicate the need for continuing judgement about the severity and impact of the condition. The proposed severity scale being divided into three levels, with level 1 being deemed to require support, level 2 requiring substantial support and level 3 requiring very substantial support (American Psychiatric Association 2011), aims to have diagnostic clinicians identify and rank client needs. Whilst this system may eliminate differences in perceptions being based on the broad label of ‘Asperger’s disorder’ and ‘autism’, it will require accurate diagnostic methods to ensure the appropriateness of the severity level. It is also possible that this severity scale may need reviewing during a person’s life span, as despite Autism Spectrum conditions being considered to be lifelong, challenges in social communication and restricted interests and repetitive behaviours may alter in severity levels across time. This could occur during key developmental times in primary school, adolescents and early adulthood, as social demands and expectations change (Attwood 1998; Paxton and Estay 2007). This area of monitoring the severity level will become more important if access to support in education settings and disability services become linked to the severity scale, with this currently being unknown at this time.
Even though the proposed changes in the diagnostic criteria are predominately designed to reflect an overall desire to develop “more useful diagnostic categories” (Regier et al. 2009, p. 648), the issue of reducing the current level of confusion between the labels used to described the current pervasive developmental disorders has also been raised by those reviewing the diagnostic criteria (Wallis 2009). While a range of terminology describing autism and Asperger’s disorder has previously been mentioned in articles and books (Attwood 1998; Paxton and Estay 2007; Rosenberg et al. 2009; Wallis 2009), the 24 different methods participants used to label, spell and represent autism and Asperger’s disorder in their free text comments in this study highlights the current range of terms associated with autism and Asperger’s disorder.
In conclusion, this study has provided some research evidence for the assumption that autism is viewed more negatively than the condition of Asperger’s disorder and that the professional divide that has been played out over the past couple of years in the literature about the proposed changes to the DSM-V has extended across professionals working in the health and education areas.
In considering limitations of this study, it is important to mention that the question presented to participants about the proposed diagnostic changes used the terminology of Autistic Disorder (Autism Spectrum Disorder), which was consistent with the initial proposal released in 2009 for the DSM changes (American Psychiatric Association 2009), when the questionnaire was initially designed. Given the subsequent revised terminology of Autism Spectrum Disorder (American Psychiatric Association 2010) for the new DSM label, one could question if this change in terminology may have impacted on the participants’ responses. This seems unlikely, however, given that the Autism Spectrum terminology remained the same and the revised definition relating to ‘autism’ remained consistent.
Another potential limitation of this study was the inclusion of this question at the end of a questionnaire that explored more generally the perception of Asperger’s disorder. Given the initial part of the questionnaire was about Asperger’s disorder, the participants completing this section of the questionnaire may have been biased towards Asperger’s disorder, with their results reflecting this bias. Due to the preliminary and exploratory nature of this research it is considered that further research could extend on the current findings through using the developing a quantitative questionnaire to further compare reasons for supporting or not supporting the proposed changes.
References
Admin. (2011, July 6). Asperger’s, autism and the new DSM. Retrieved December 27, 2011.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders. Washington: American Psychiatric Association.
American Psychiatric Association. (2009). Asperger’s disorder. Retrieved 30 April 2009.
American Psychiatric Association. (2010). DSM-V: The future manual. Retrieved 18 June.
American Psychiatric Association. (2011). DSM-5 Development. Retrieved September 1, 2011 from http://www.dsm5.org>Home>ProposedRevision.
Angermeyer, M. C., & Matschinger, H. (2003). The stigma of mental illness: Effects of labelling on public attitudes towards people with mental illness. Acta Psychiatrica Scandinavica, 108, 304–309.
Attwood, T. (1998). Asperger’s syndrome: A guide for parents and professionals. London: Jessica Kingsley Publishers.
Australian Government. (2008). Helping children with autism. Canberra: FaHCSIA.
Autism Support Group. (2010). Proposed changes to autism diagnosis in DSM-V. Retrieved 20 July 2010.
Barbaro, J., & Dissanayake, C. (2007). A comparative study of the use and understanding of self-presentational display rules in children with high functioning autism and Asperger’s disorder. Journal of Autism and Developmental Disorders, 37, 1235–1246.
Bernard, H. R., & Ryan, G. W. (2010). Analyzing qualitative data systematic approaches. London: SAGE Publications.
Bocaccini, M. T., Murrie, D. C., Clark, J. W., & Cornell, D. G. (2008). Describing, diagnosing and naming psychopathy: How do youth psychopathy labels influence jurors. Behavioural Science and the Law, 26, 487–510.
Brewin, B. J., Renwick, R., & Fudge Schormans, A. (2008). Parental perspectives of the quality of life in school environments for children with Asperger syndrome. Focus on Autism and other developmental disabilities, 23(4), 242–252.
Bubbles. (2011). Autism and Asperger’s in teh DSM-V: Thoughts on clinical utility. Retrieved September 2011.
Corrigan, P. W. (2007). How clinical diagnosis might exacerbate the stigma of mental illness. Social Work, 52(1), 31–39.
Cuccaro, M. L., Nations, L., Brinkley, J., Abramson, R. K., Wright, H. H., Hall, A., et al. (2007). A comparison of repetitive behaviors in Aspergers disorder and high functioning autism. Child Psychiatry and Human Development, 37, 347–360.
Doherty, E. (2009, 26 April). Kids ‘Cage’ Anger. The Advertiser, pp. 1, 4.
Earley, D. (2009, May 2). Rein reveals autism ordeal. The Advertiser.
Eiser, J. R., & Mower-White, C. J. (1976). The persuasiveness of labels: Attitude change produced through definition of the attitude continuum. European Journal of Social Psychology, 4(1), 89–92.
Elfant, A. B. (1985). Psychotherapy and assessment in hospital settings: Ideological and professional conflicts. Professional Psychology: Research and Practice, 16(1), 55–63.
Fletcher, J., Pirkis, J., King, K., Christo, J., Bassilios, B., Burgess, P., et al. (2011). Psychologists’ experiences with the Better Access initiative: A pilot study. Australian Psychologist, 46, 153–162.
Ghaziuddin, M. (2005). A family history study of Asperger’s syndrome. Journal of Autism and Developmental Disorders, 35, 177–182.
Ghaziuddin, M. (2008). Defining the behavioural phenotype of Asperger syndrome. Journal of Autism and Developmental Disorders, 38(1), 138–142.
Ghaziuddin, M. (2010). Brief report: Should the DSM V drop Asperger syndrome? Journal of Autism and Developmental Disorders, 40, 1146–1148.
Gillberg, C., & Enlers, S. (1998). High functioning people with Autism and Asperger’s syndrome: A literature review. In E. Schopler, G. B. Mesibov, & L. J. Kunce (Eds.), Asperger syndrome or high-functioning autism? (pp. 79–100). New York: Plenum Press.
Henrysdad. (2010). Autism and Asperger’s in teh DSM-V: Thoughts on clinical utility. Retrieved September 21, 2011.
Holm-Denoma, J. M. (2008). Patients’ affective reaction to receiving diagnostic feedback. Journal of Social and Clinical Psychology, 27(6), 555–575.
Hough, H. (2006). Letters to the editor. Journal of Child and Adolescent Psychiatric Nursing, 19(4), 166–169.
Huang, H., & Diamond, K. E. (2010). Early childhood teacher’s ideas about including children with disabilities in programmes designed for typically developing children. International Journal of Disability, Development and Education, 56(2), 169–182.
Isus. (2011). Autism and Asperger’s in the DSM-V: Thoughts on clinical utility. Retrieved September 21, 2011.
Julie. (2011). Bye Bye Asperger’s syndrome. Retrieved November 1, 2011 from http://psychcentral.com/blog/archives/2009/11/05/bye-aspergers-syndrome.
Kite, D., & Tyson, G. (2011a). Implicit theories of characteristics and causes of Asperger's disorder. Manuscript submitted for publication.
Kite, D., & Tyson, G. (2011b). Management and treatment strategies for Asperger's disorder- How effective are they perceived to be? Manuscript submitted for publication.
Kite, D., Tyson, G., & Gullifer, J. (2011). Exploring the perception of Asperger’s disorder. Unpublished Manuscript submitted for publication.
Kupfer, D. J., Regier, D. A., & Kuhl, E. A. (2008). On the road to the DSM-V and ICD-11. European Archives of Psychiatry and Clinical Neuroscience, 258, 2–6.
Lecavalier, L., Gadow, K. D., DeVincent, C. J., Houts, C., & Edwards, M. C. (2009). Deconstructing the PDD clinical phenotype: Internal validity of the DSM-IV. Journal of Child Psychology and Psychiatry, 50(10), 1246–1254.
Lenne, B. S., & Waldby, C. (2011). Sorting out autism spectrum disorders: Evidence-based medicine and the complexities of the clinical encounter. Health Sociology Review, 20(1), 70–83.
Little, L. (2003). Maternal perceptions of the importance of needs and resources for children with Asperger syndrome and nonverbal learning disorders. Focus on Autism and Other Developmental Disabilities, 18(4), 257–266.
Lopez-Duran, N. (2010). Autism and Asperger’s in the DSM-V: Thoughts on clinical utility. Retrieved September 21, 2011,
MacCulloch, T. (2010). Constructions of truth, gate-keeping and the power of diagnostic labels. Issues in Mental Health and Nursing, 31, 151–152.
Macintosh, K., & Dissanayake, C. (2006). Social skills and problem behaviours in school aged children with high-functioning autism and Asperger’s disorder. Journal of Developmental Disorders, 36, 1065–1076.
Paxton, K., & Estay, I. A. (2007). Counselling people of the autism spectrum: A practical manual. London: Jessica Kingsley Publishers.
Regier, D. A., Narrow, W. E., Kuhl, E. A., & Kupfer, D. J. (2009). The conceptual development of DSM-V. American Journal of Psychiatry, 166(6), 645–650.
Rogler, L. H. (1997). Making sense of historical changes in the diagnostic and statistical manual of mental disorders: Five propositions. Journal of Health and Social Behavior, 38, 9–20.
Rosenberg, R. E., Daniels, A. M., Law, K. J., Law, P. A., & Kaufmann, W. E. (2009). Trends in autism spectrum disorder. Journal of Autism and Developmental Disorders, 39, 1099–1111.
Rosenhan, D. L. (1973). On being sane in insane places. Science, 179, 250–258.
Sanders, J. L. (2009). Qualitative or quantitative differences between Asperger’s Disorder and autism? Historical considerations. Journal of Autism and Developmental Disorders, 39, 1560–1567.
Skellern, C., Schluter, P., & McDowell, M. (2005). From complexity to category: Responding to diagnostic uncertainties of autism spectrum disorders. Journal of Paediatrics and Child Health, 41, 407–412.
Sproule, W. (2010). Content analysis. In M. Walter (Ed.), Social research methods (2nd ed., pp. 323–350). Melbourne: Oxford University Press.
Stinnett, T. A., Bull, K. S., Koonce, D. A., & Aldridge, J. O. (1999). Effects of diagnostic label, race, gender, educational placement and definitional information on prognostic outlook for children with behavior problems. Psychology in Schools, 36(1), 51–59.
Swedo, S. (2009). Report of the DSM-V neurodevelopmental disorder work group. Retrieved 9/12/2009.
Wallis, C. (2009). A powerful identity, a vanishing diagnosis. The New York Times.
William & Mary. (2011). Asperger’s, autism and the new DSM. Retrieved December 1, 2011 from http://www.wm.edu/offices/deanofstudents/services/disabilityservices/facultyresource.
Wing, L., Gould, J., & Gillberg, C. (2011). Autism spectrum disorders in the DSM-V: Better or worse than the DSM-IV? Research in Developmental Disabilities, 32, 768–773.
World Health Organisation. (1992). ICD-10 international statistical classification of diseases and related health problems. Geneva: author.
Acknowledgments
The Nursing and Allied Health Scholarship and Support Scheme (NAHSSS) funded through the Department of Health and Ageing provided support for participation in the Doctor of Clinical Psychology course. The views expressed in this article do not necessarily represent those of the NAHSS, its Administrator, Services for Australian Rural and Remote Allied Health (SARRAH) and/or the Australian Government Department of Health and Ageing.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kite, D.M., Gullifer, J. & Tyson, G.A. Views on the Diagnostic Labels of Autism and Asperger’s Disorder and the Proposed Changes in the DSM. J Autism Dev Disord 43, 1692–1700 (2013). https://doi.org/10.1007/s10803-012-1718-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1718-2