
Abstract
Self-perception in high-functioning children and adolescents with Autism Spectrum Disorder (ASD) was examined by comparing parent- and self-reports on the Autism Spectrum, Empathy, and Systemizing Quotients (AQ, EQ and SQ). Participants were 20 youths with ASD and 22 typically developing controls. Both parents and participants in the ASD group reported more autistic traits (higher AQ) and less empathy (lower EQ) than the control group. SQ ratings did not differ between groups. Comparisons of self- and parent-reports indicated that youths with ASD reported significantly fewer autistic traits and more empathic features than their parents attributed to them. There were no discrepancies between parent- and self-reports in the control group. Implications regarding the use of self-report in ASD are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism Spectrum Disorders (ASDs) are characterized by impairments in social interaction and communication as well as repetitive and stereotyped patterns of behaviours and interests (American Psychiatric Association 2000). The autism spectrum includes Autistic Disorder, Asperger’s Disorder and Pervasive Developmental Disorders—Not Otherwise Specified. The clinical presentation of the symptoms of ASD is heterogeneous across individuals and, over time, can vary within the same person (Hill and Frith 2003). As such, it is vital that health care professionals have access to accurate information about their clients’ current symptoms and characteristics so that they can provide valid diagnoses, develop individualized treatment plans and monitor progress and change across time. Further, researchers in the field of ASD must be able to precisely characterize the individuals and groups that they study.
Self-report measures are valuable and common assessment tools in clinical research and practice, especially in the evaluation of older children, adolescents and adults. These instruments provide reports of subjective experience that cannot be obtained through any other means. However, the reliability of self-report data are sometimes questioned, not only because of the potential for measurement error associated with all assessment tools, but also due to the possibility of bias on the part of respondents (Baldwin 2000). In addition, when characterization information is obtained directly from individuals with disorders that affect their psychological and cognitive functioning, there are concerns about the degree to which they are aware of, or have insight into, their symptoms. Some investigators have suggested that impaired introspection, or self-awareness, may be associated with ASD (e.g., Frith 1989). If this is the case, there are important considerations regarding the use of self-report tools in clinical practice and research settings where people with ASD are assessed. The primary goal of this research project was to provide clinicians and researchers with information about the self-perception of autism related symptoms in ASD. This knowledge is necessary to assess the suitability of self-report symptom measures for individuals with ASD.
It has been well established that theory of mind (ToM) deficits are common in individuals with ASD (Tager-Flusberg 2007). ToM is conceptualized as the ability to attribute mental states to the self and others (Premack and Woodruff 1978). As a result of these attributions, individuals with intact theory of mind are able to understand the motivations, and predict the actions, of others. It has been proposed that impaired ToM is a central deficit in ASD and that many symptoms characteristic of the autism spectrum can be explained by an impaired ability to comprehend the minds of others (Perner et al. 1989). Nearly all previous research that has examined ToM in ASD has focused on knowledge of others’ minds. However, Frith and Happé (1999) described evidence that suggested some individuals with ASD experience a lack of awareness of their own mental states. They hypothesized that if the mechanisms that underlie the ability to ascribe mental states to others are the same as those required for attributing and reflecting on one’s own mental state, then “self-knowledge is likely to be impaired just as is the knowledge of other minds” (p. 7).
Consistent with this notion, Green et al. (2000) reported that only half of the parents of a sample of boys with Asperger’s Disorder (ASP) believed their sons to have some awareness of their “autistic handicap”. The experimenters rated even fewer boys with ASP (15%) to have an accurate perception of their disability. Further, Green et al. (2000) found that 30% of participants with ASP reported that they did not have a handicap or any differences relative to others. Similarly, Koning and Magill-Evans (2001) observed that, although a group of adolescent boys with ASP had some awareness of their social skills deficits, they assessed themselves as having more social skills than their parents and teachers reported them to possess. Knott et al. (2006) described similar findings; self-reports by children and adolescents with ASD indicated greater levels of social skills and social competence relative to parent-reports.
In this study, we examined how individuals with ASD perceive their autism-related traits and behaviors relative to how another person, a parent, perceives them. As is the case in previous literature, we use the terms “self-perception”, “self-awareness” and “insight” interchangeably to refer to the degree to which agreement exists between an individuals’ self-report of autism related traits and behaviors and parental perceptions of the same traits and behaviors. We consider individuals with greater agreement between self- and parent-perceptions to be more accurate in their self-perceptions and to possess greater levels of self-awareness and insight.
We examined self-perception of traits and behaviors associated with the autism spectrum by comparing self- and parent-reports of children and adolescents with ASP or high-functioning autism (HFA; hereafter referred to as the ASD group) on three measures that characterize traits that have been associated with the autism spectrum: the Autism Spectrum Quotient (AQ; Baron-Cohen et al. 2001), the Systemizing Quotient (SQ; Baron-Cohen et al. 2003) and the Empathy Quotient (EQ; Baron-Cohen and Wheelwright 2004). The AQ has been widely used in studies of ASD and measures the degree to which an individual exhibits traits that are associated with the autism spectrum (Baron-Cohen et al. 2001). The SQ evaluates an individual’s interest in analyzing or constructing systems (Baron-Cohen et al. 2003), such as curiosity about how machines work or interest in numbers and patterns. The EQ measures the extent to which an individual can comprehend the intentions and predict the behaviours of others, as well as their ability to experience emotions as a result of perceiving the emotions of others (Baron-Cohen and Wheelwright 2004). Previous studies have demonstrated significant differences between the self-report ratings of adults with ASD and control participants on the AQ, EQ and SQ (Baron-Cohen et al. 2003; Baron-Cohen and Wheelwright 2004; Baron-Cohen et al. 2001). Typically, adult participants with ASD report more systemizing and less empathic characteristics, as well as more traits and behaviours associated with the autism spectrum, than do controls.
The only previous data that addressed self- versus other-report on these measures were reported by Baron-Cohen et al. (2001)) in their initial study of the AQ. In a subsample (22/58) of ASD participants, parents attributed slightly more autistic traits to their adult children than the adults with ASD attributed to themselves. The mean parent score was 2.8 points higher, but no statistical analyses of these data were reported. It has been suggested (Baron-Cohen and Wheelwright 2004) that there is a need to complete additional studies of these measures by comparing scores for the same individuals across raters. However, to our knowledge, no further comparisons of self and other ratings on the AQ have been reported and there have been no studies of self- and other-ratings utilizing the EQ and SQ measures.
Our main hypothesis was that we would observe significant differences between self- and parent-ratings on the AQ, EQ and SQ for the ASD group, but not for the control group. Specifically, we expected that parents of children with an ASD would rate their children as having more autism-related traits and behaviors than the children themselves acknowledged. For the control group, we hypothesized that parent-ratings would not differ from self-ratings for any of the three scales. As indicated previously, the primary objective of this study was to provide researchers and clinicians with additional information regarding the appropriateness of self-report measures for evaluating symptoms and behaviours in high-functioning children and adolescents with an ASD.
Methods
Participants
In total, 42 children and adolescents participated in this study. Also, for each youth participant, one parent or guardian completed questionnaires relating to their child’s behaviour. The 20 participants in the Autism Spectrum Disorder (ASD) group met full criteria for autism based on the Autism Diagnostic Interview—Revised (Lord et al. 1994), while the other 22 were classified as typically developing controls. All participants in the ASD group had received a diagnosis of Asperger’s Disorder or Autistic Disorder based on DSM-IV criteria, as well as best clinical estimate by a clinician or team of clinicians with autism expertise. For both groups, participants were excluded if they had an estimated IQ of less than 75 (Wechsler Abbreviated Scale of Intelligence; WASI; Wechsler 1999), a history of a traumatic brain injury, significant neurological disorder, or systemic condition that might affect the central nervous system. Control participants were also excluded if they had a past or present diagnosis of any psychiatric disorder (including an ASD). Some participants did not complete all three questionnaires examined in the current study (the AQ, EQ and SQ). As such, we compared the age, sex and estimated full scale IQ of the ASD and control groups for both the entire sample (see Table 1) as well as the smaller sub-samples that completed each measure. There were no significant differences between groups for any of these comparisons.
Materials
Three questionnaires were used to assess parent- and self-reports of autism related characteristics. The AQ (Baron-Cohen et al. 2001) assesses the extent to which individuals express traits associated with the autism spectrum. Some sample AQ items are as follows: “I prefer to do things the same way over and over again” and “I find social situations easy”. The AQ is comprised of 50 questions and all items are included in the overall score. The SQ (Baron-Cohen et al. 2003) measures the degree to which individuals are interested in constructing and analyzing systems. Two examples of SQ items are: “If I had a collection (e.g., CDs, coins, stamps), it would be highly organized” and “When I learn about historical events, I do not focus on exact dates”. The EQ (Baron-Cohen and Wheelwright 2004) assesses whether individuals can understand the intentions of others and predict their behavior, while also measuring their ability to experience emotions as a result of perceiving the emotions of others. Some sample EQ items are as follows: “I am good at predicting how someone will feel” and “I often find it difficult to judge if something is rude or polite”. The SQ and EQ both contain 60 questions, of which 20 are unscored filler items.
For each question on all three measures there are four response options: strongly or definitely agree, slightly agree, slightly disagree, and definitely or strongly disagree. For the AQ, EQ and SQ, half of the items are worded such that an “agree” response indicates a high score, whereas for the other half a “disagree” response is a high score. For the AQ, one point is given for each response that represents endorsement of an autism related trait, regardless of whether the modifier is “slightly” or “definitely”. For the EQ and SQ, however, one point is given for responses that indicate a “slight” endorsement of the trait being measured (i.e., empathy or systematizing, respectively) and two points if the response is a “strong” endorsement. For the AQ, EQ and SQ, an item score of zero is given if an answer does not represent endorsement of an autism-related, empathic or systematizing trait, respectively.
Comparisons of individuals with ASD and control participants have shown differences on the self-report versions of the AQ (Baron-Cohen et al. 2001), EQ (Baron-Cohen and Wheelwright 2004) and SQ (Baron-Cohen et al. 2003), as well as for parent-reports on the adolescent version of the AQ (Baron-Cohen et al. 2006). On the adult (self-report) version of the AQ, a group of individuals with ASP or HFA scored significantly higher than a group of control participants (Baron-Cohen et al. 2001), indicating a higher level of autism related traits. Similarly, parents of adolescents with ASD rated their children as significantly higher on the AQ, as compared to parents of typically developing adolescents (Baron-Cohen et al. 2006). On the SQ (Baron-Cohen et al. 2003), adults with ASP or HFA reported significantly higher self-report scores than comparison participants, indicating more interest in analyzing and constructing systems. Baron-Cohen and Wheelwright (2004) found that adults with ASP or HFA had significantly lower EQ scores than controls, indicating that they rated themselves as having fewer empathic traits (Baron-Cohen et al. 2003).
Baron-Cohen et al. (2001) suggested that a cut-off score of 32 or higher on the AQ can discriminate adults who have clinically significant levels of autistic traits. For the parent-report adolescent version of the AQ, a cut-off score of 30 or higher has been suggested (Baron-Cohen et al. 2006). On the EQ, Baron-Cohen and Wheelwright (2004) showed that a score of 30 or below differentiates individuals with HFA or ASP from control participants. With respect to the SQ, Baron-Cohen et al. (2003) observed that individuals with HFA or ASP scored significantly higher (M = 35.7, SD = 15.3) than a group of control participants (M = 29.7, SD = 10.2), but a cutoff score for differentiating those with an ASD from controls was not suggested.
Baron-Cohen et al. (2001) reported that, for the AQ, two-week test-retest reliability was r = .70. They also demonstrated that control participants scored higher than adults with ASP/HFA on only 2 of the AQ’s 50 items. Further, 79.3% of individuals with ASP/HFA and only 2% of controls scored above the AQ’s recommended cutoff score of 32. Baron-Cohen et al. (2001) interpreted these data to indicate that the AQ possesses reasonable face and construct validity, as well as strong test-retest reliability. With respect to the EQ, Baron-Cohen and Wheelwright (2004) reported that 81.1% of adults with ASP/HFA and 12.2% of controls scored below the EQ’s recommended cutoff score of 30. They also showed that control participants scored lower than individuals with ASP/HFA on only 2 of the EQ’s 40 scored items. Further, twelve-month test-retest reliability was r = .97. The authors also reported a high Cronbach’s alpha coefficient (.92) for the EQ. Baron-Cohen and Wheelwright concluded that these data provide evidence of reasonable construct and external validity and strong test-retest reliability for the EQ.
For the SQ, less psychometric data are available. Baron-Cohen et al. (2003) reported a reasonable Cronbach’s alpha coefficient of .79 for this measure. Recently, Ling et al. (2009) reported a similar alpha coefficient of .80 for the SQ. However, Ling et al. (2009) noted that when they removed a number of items from the SQ, the Cronbach’s alpha statistic increased to .815. They interpreted this to mean that some SQ items may not be measuring the same construct as the broader scale.
Although a parent-report version of the AQ exists (Baron-Cohen et al. 2006), it was necessary to adapt the SQ and EQ to enable parent-report. This was done in the same manner by which the AQ was adapted for this purpose. All items retained their original meanings and were only modified to reflect a third-person, rather than a first-person, perspective (i.e., “I” was changed to “my child” or “he/she”). Both self- and parent-ratings were focused on the child’s behaviour. For the purposes of this study AQ, SQ and EQ items were not adapted specifically for use with youth participants. However, participants rarely expressed difficulty comprehending items and examiners were available to answer questions regarding the meaning of items.
Procedures
Participants completed the AQ, SQ and EQ measures as part of larger test batteries that examined social and cognitive functioning. These studies were conducted in Bloomington, Indiana or Halifax, Nova Scotia. All data were obtained in accordance with study protocols approved by the Indiana University Human Subjects Committee or the IWK Health Centre Research Ethics Board and the Dalhousie Research Ethics Board. For participants older than 18 years, written, informed consent was obtained. For those younger than 18 years, parental consent and participant assent was acquired. Following consent procedures, participants’ general level of cognitive ability was estimated using the WASI (Wechsler 1999). None of the participants performed below the inclusion cutoff (i.e., 75) on the WASI. Based on WASI scores and general conversational skills, all participants were considered to be capable of completing the questionnaires.
The AQ (Baron-Cohen et al. 2001), SQ (Baron-Cohen et al. 2003) and EQ (Baron-Cohen and Wheelwright 2004) were completed by each participant and by a parent or legal guardian. Most participants completed these measures in the laboratory; however, some filled out the questionnaires at home. Participants were encouraged to obtain clarification from the experimenters if they did not understand the meaning of any items. Each questionnaire was scored by two different researchers to ensure accuracy.
Results
A 2 × 2 repeated measures Analysis of Variance (ANOVA) was completed for each of the three measures (AQ, EQ and SQ), with group (ASD and control) and rater (parent and self) as independent variables. We completed the following post-hoc t-tests when appropriate. Self- and parent-ratings were compared within the ASD and control groups, using paired sample t-tests, for each scale. Independent samples t-tests were used to compare the two groups on self-ratings and parent-ratings for each scale. Finally, we examined relationships between parent- and self-ratings on each measure within the ASD and control groups separately using Pearson correlations.
Autism Spectrum Quotient Findings
For the AQ, repeated measures ANOVA revealed a significant between-subjects main effect of group [F(1, 36) = 91.8, p < .001], with participants in the ASD group having higher AQ scores than those in the control group. A significant within-subjects main effect of rater [F(1, 36) = 31.2, p < .001] was also noted, with higher parent- versus self-ratings. In addition, an interaction between the group and rater variables was observed [F(1, 36) = 56.6, p < .001].
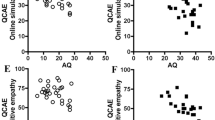
Follow-up t-tests revealed that AQ scores were higher for the ASD group than the control group for both self [t(36) = 4.8, p < .001] and parent [t(36) = 11.9, p < .001] scores (see Table 2). Parent- and self-ratings differed for the ASD group [t(17) = −6.9, p < .001], with parents reporting significantly more autism symptoms than the children. However, parent and self AQ scores did not differ for the control group [t(20) = 2.1, p > .05, see Fig. 1].

Mean self and parent AQ ratings for ASD and control groups (+SE), * p < .001. Maximum = 50. A cutoff of 32 has been suggested to differentiate ASD and control participants
Empathy Quotient Findings
For the EQ ratings, repeated measures ANOVA also showed a significant main effect of group [F(1, 35) = 66.2, p < .001], with participants in the ASD group having lower EQ scores than those in the control group. There was also a significant main effect of rater [F(1, 35) = 9.2, p < .005], with lower overall parent-ratings relative to self-ratings. In addition, there was a significant group by rater interaction [F(1, 35) = 24.9, p < .001].
Follow-up t-tests indicated significant differences between ASD and control group ratings for both self [t(36) = −3.6, p < .001] and parent [t(35) = −10.6, p < .001] scores. In both cases, EQ scores were lower for the ASD group than the control group (see Table 2). Consistent with the AQ results, parent- and self-ratings differed on the EQ for the ASD group [t(17) = 5.3, p < .001], with parents rating their children as having fewer empathic characteristics relative to self-ratings by the children. There was no difference between the self and parent EQ scores for the control group [t(18) = −1.5, p > .05, see Fig. 2].

Mean self and parent EQ ratings for ASD and control groups (+SE), * p < .001. Maximum = 80. A cutoff of 30 has been suggested to differentiate ASD and control participants
Systemizing Quotient Findings
In contrast to the findings for the AQ and EQ, repeated measures ANOVA of the SQ ratings did not reveal main effects of rater [F(1, 37) = 1.4, p > .05] or group [F(1, 37) = .02, p > .05], nor a significant interaction [F(1, 37) = .10, p > .05].
Relationships Between Parent- and Self-Report Scores
Pearson correlations were calculated to determine whether relationships existed between self- and parent-scores within the ASD or control groups on the AQ, EQ or SQ. For the ASD group, there were no significant relationships between self- and parent-ratings for any of the measures [AQ (r(17) = .45, EQ (r(18) = −.02, SQ (r(19) = .17; all p > .05]. However, there were significant associations between self and parent scores in the control group for the AQ [r(21) = .71, p < .001] and EQ [r(19) = .54, p < .05], but not the SQ [r(20) = .37, p > .1].
Relationships Between Discrepancy Scores and Demographics
Pearson correlations were also examined to determine whether discrepancy scores between parent- and self-ratings were associated with demographic variables, including the age, estimated full scale IQ, and estimated verbal and performance IQ of the participant. For each measure, a discrepancy score was calculated by subtracting the self-report score from the parent-report score for each participant. We then examined the relationships between the discrepancy scores and each of the demographic variables for the two groups separately. There were no significant correlations (all p > .05) between any of these variables and discrepancy scores on the AQ or EQ for either the control or ASD groups.
For the SQ, however, discrepancy scores were related to several demographic variables. Within the ASD group, there were significant correlations between positive SQ discrepancies, which indicate higher parent than child ratings, and lower estimated full scale IQ [r(17) = −.53, p < .05] and lower estimated verbal IQ [r(17) = −.54, p < .05]. Similarly, for the control group, positive SQ discrepancies were related to lower estimated full scale IQ [r(19) = −.60, p < .01], lower estimated verbal IQ [r(19) = −.46, p < .05], lower estimated performance IQ [r(19) = −.48, p < .05] and younger age [r(19) = −.55, p < .05].
Discussion
The goal of the present study was to examine how children and adolescents with ASD perceive themselves relative to how others perceive them. To investigate this question, we collected parent- and self-reports on three measures of autism-related traits (the AQ, EQ and SQ) for a group of youths with an ASD and typically developing controls. Consistent with previous studies (e.g., Baron-Cohen and Wheelwright 2004; Baron-Cohen et al. 2001) we found higher AQ scores and lower EQ scores for the ASD group relative to controls. Not only was this the case for parent-ratings, but also for self-ratings, suggesting that youths with an ASD have some awareness of their expression of autistic and empathic traits. However, as hypothesized, we also found that parent- and self-ratings differed significantly within the ASD group for both the AQ and EQ, while there were no differences between parent- and self-ratings for the control group. Specifically, children and adolescents with an ASD rated themselves as having fewer autistic features and more empathic traits than did their parents. This finding supports the notion that children and adolescents have limitations in their self-perception of autism-related traits.
In contrast to previous findings (Baron-Cohen et al. 2003), the ASD and control groups did not differ on the SQ. This finding held for both self- and parent-ratings, with the two groups generating nearly identical ratings. Importantly, there were no differences between parent- and self-ratings on the SQ for the control group or the ASD group. This finding is in sharp contrast to the large discrepancies between parent- and self-ratings for the ASD group on the AQ and EQ and may suggest that self-perception is not uniformly impaired for all behaviours and traits.
However, we interpret the SQ findings with caution for the following reasons. We found significant associations between SQ discrepancy scores (parent vs. self) and age and IQ for the control group and between SQ discrepancy scores and IQ for the ASD group. Furthermore, self and parent scores for the SQ were not correlated for either group. However, after controlling for age, there were significant correlations between parent and self SQ scores for the control group. The same was true after controlling for IQ. In contrast, for the ASD group, the correlation between parent and self SQ ratings was not significant after controlling for age and IQ. Although the mean score of the SQ ratings did not differ for the ASD participants and their parents, the fact that these scores were not correlated suggests that youth and parent ratings were not in agreement on this measure. Recall that there were also significant associations between parent and youth AQ and EQ scores for the control group, but no such relationships for the ASD group. This pattern of findings held when we controlled for age and IQ.
The significant association between the magnitude of the parent versus self SQ discrepancy and age for the control group, with younger children showing lower SQ scores, suggests that this measure is sensitive to developmental effects. This was not the case for the AQ and EQ. These results suggest that if the SQ is used in future studies with children and adolescents that revisions to the content may be necessary. Furthermore, lower IQs were associated with larger discrepancies in the direction of children with lower IQ reporting fewer systemizing features than parents. It is possible that the questions on the SQ are more difficult to answer than those on the AQ and EQ and this may have contributed to less accurate or more variable responses by the youths in our study. Although Ling et al. (2009) reported that adult SQ scores are independent of intelligence, a standard measure of IQ was not employed. In contrast to the SQ findings, our data did not reveal relationships between the AQ and EQ discrepancy scores and IQ or age. The current findings suggest that further work is needed to define the construct measured by the SQ, as well as its relationship with IQ and age.
Together, the AQ and EQ findings show that, although individuals with an ASD reported higher scores on the AQ and lower scores on the EQ than did controls, they rated themselves as more similar to typically developing children and adolescents than did their parents. Also of considerable interest was the finding that parent and self AQ and EQ scores were positively correlated in the control group, but not in the ASD group. This provides further evidence of a discrepancy between parent and self assessments for those with an ASD. In contrast to these discrepancies, parent- and self-reports for the ASD group were similar on the SQ. As discussed above, these results may suggest that self-perception in children and adolescents with ASD is not impaired in some areas. However, the lack of correlation between parent- and self-ratings on the SQ in our ASD group casts some doubt on this interpretation.
Our current findings are in keeping with those of previous studies. For example, Koning and Magill-Evans (2001) and Knott et al. (2006) found that participants assessed themselves as possessing greater levels of social skills or competence than reported by others. Similarly, Green et al. (2000) found that many youths with ASD in their sample underestimated their degree of “disability”. Our results are also similar to data published with respect to the Positive Illusory Bias that has been reported in children with Attention-Deficit Hyperactivity Disorder (ADHD). Despite the fact that individuals with ADHD experience difficulties across a number of domains of functioning (e.g., academic, social and behavioural), they often rate their own competence in these areas very highly (Owens et al. 2007). Our results suggest that children and adolescents with an ASD may also be prone to a positive illusory bias, at least with regard to their autism-related symptoms.
The results described above have important implications for our understanding of ToM deficits in ASD. As indicated earlier, although most previous research on ToM in ASD has centered around impairments in knowledge of others’ minds, some researchers (e.g., Frith and Happé 1999) have suggested that self-knowledge may also be affected. Our findings of discrepancies between self- and parent-ratings of symptoms are consistent with the notion of impaired theory of own mind in ASD. It is interesting to consider how awareness of one’s own mind may be related to knowledge about others’ minds. Interpretation of our own behaviors and characteristics, and the degree to which we do or do not possess certain traits (as rated on the AQ, EQ, and SQ), likely requires awareness and knowledge of what is “typical”. For example, to decide whether I agree or disagree with the item “I am good at predicting how someone will feel”, I need to know what “good” means in this context and then be able to compare myself to others. Without knowledge of how good others are at predicting how someone will feel, I may be poor at judging my own skill in this area. Future research is needed to address the question of how the understanding of own and other minds are related and whether the same mechanisms underlie both of these processes.
Understanding Discrepancies Between Raters
We recognize that the nature of the discrepancies between parent- and self-reports on the AQ and EQ may not be due entirely to poor self-perception on the part of the youths with ASD. Years of experience learning about and living with a child with an ASD is likely to lead parents to be more knowledgeable of, observant of, and sensitive to autism related traits. As such, the parents of our ASD sample may have assigned higher ratings to some of the ASD associated traits exhibited by their children than parents of control participants assessing the same behaviours. However, in light of previous findings (Green et al. 2000; Knott et al. 2006; Koning and Magill-Evans 2001), the discrepancy observed between self- and parent-reports identified in this current study likely reflects poorer self-perception to a greater extent than over-reporting by parents. Furthermore, it is important to keep in mind that parents and youths did not differ on the SQ. The lack of difference on this measure suggests that discrepancies between self- and parent-reports were not simply due to a systematic bias in under-reporting by the ASD youths or over-reporting by their parents.
To address the question of the relative contributions of parent- versus self-perceptions to the AQ and EQ discrepancies, it would be valuable to obtain ratings of individuals with an ASD from a third source, such as a teacher or peer. Teacher reports may be particularly useful due to educators’ broad normative experience with typical and atypical child development. Additional information could also be obtained through behavioural observation. Such data could be compared to both parent- and self-ratings in order to parse out parental and child contributions to the discrepancy in rating autism related characteristics. Furthermore, it will be important to examine self- and other-ratings in adults with an ASD in order to determine if poor self-perception is also present later in development.
Clinical Implications
The role of insight into autism symptoms, and self-perception more generally, in ASDs has received only minimal attention in previous research (Capps et al. 1995; Vickerstaff et al. 2007). Our results provide valuable information about the use of self-report measures to assess individuals with ASD and may indicate the need for an appraisal of an individual’s self-awareness before self-report tools are considered a reliable means for measuring current symptoms and level of functioning. The findings of this study also provide the basis for a discussion about whether impairments in self-perception should be the target of treatment. In 1973, Kanner suggested that for his patients with the best outcomes, awareness of differences resulted in “a conscious effort to do something about them” (p. 209). The argument that awareness and accurate perception of symptoms might facilitate positive treatment outcomes in ASD is supported by empirical evidence that better insight or awareness of psychiatric symptoms is associated with good clinical outcomes in some clinical populations (e.g., Obsessive Compulsive Disorder; Himle et al. 2006; Storch et al. 2008).
Counter to this argument, the results of several studies suggest that greater awareness of differences, or poorer self-perceived competence, is associated with negative mood and depression in individuals with ASD (e.g., Butzer and Konstantareas 2003; Vickerstaff et al. 2007). It is possible that individuals with ASD who have intact self-perception experience depression because they are aware of their differences and cognizant of the challenges they face as a result (Capps et al. 1995; Sterling et al. 2008). There is a high rate of depression in ASD populations (Vickerstaff et al. 2007), which is particularly concerning in light of the many negative outcomes, including suicidality (Lainhart and Folstein 1994), that have been associated with depression in individuals with ASD. More research will be necessary to determine whether there are associations between awareness of ASD symptoms (i.e., level of self-perception) and presence of internalizing disorders. If relationships exist between intact self-perception and co-morbid psychopathology, it may be important to identify those children with ASD who have greater self-awareness at an early age so that prevention of internalizing disorders can be a target of treatment. Such findings will subsequently guide clinical decisions about whether improving perception of one’s ASD traits should be a target of intervention and, if so, how the negative affective symptoms that may be associated with improved self-perception in ASDs can be prevented or managed.
Limitations
An important shortcoming of the current study is a lack of inclusion of a ToM measure, which would have allowed us to examine associations between theory of others’ minds and self-perception. ToM measures should be included in future studies of self-perception. Furthermore, we recognize that the construct of self-perception is not yet fully understood. That is, in the current study, we consider the discrepancy between self- and parent-report as a representation of self-perception. We realize this is only one way to measure this construct and that other experimental and clinical measures must be developed and applied in order to thoroughly examine how individuals with an ASD perceive themselves and their autistic traits. Furthermore, this study was focused solely on traits associated with ASD. Thus, we do not know how youths with an ASD perceive other clinical symptoms, such as anxiety, depression, and attention. It will be important to examine parent- and self-report of other behaviours and traits to establish the parameters of impaired self-perception in ASD.
Further, the measures employed in this study, the AQ, EQ and SQ, were originally developed for use with adult samples. Youth participants rarely indicated that they did not understand questions contained within these questionnaires and examiners were available to provide clarification of the meaning of items. As such, we believe that participants adequately comprehended these questionnaires. However, it would be useful to test this assumption empirically in a sample of youth participants in the future. Further, it may be that the cutoff scores originally proposed for these tools are not as useful when interpreting data obtained from child and adolescent participants.
Lastly, our sample had a wide age range. Although ASD and control groups were closely matched on overall age, we are aware that there could be developmental changes in self-perception abilities during childhood and adolescence. We did examine the relationships between parent and child discrepancies on the AQ, EQ and SQ and participant demographics and found only one significant relationship, between age and the SQ parent-child discrepancy score in the control group. It will be important for future research to examine the relationship between self-perception and age in ASD, particularly in light of evidence of previous research that shows adults with an ASD rate themselves much higher on the AQ and SQ, and lower on the EQ than did the youths in the current study.
Summary
Overall, the current results provide evidence for poor self-perception of autism-related traits in children and adolescents with an ASD. Although not addressed by the current study, this difficulty may be due to the same mechanisms that underlie commonly reported difficulty with understanding minds of others. Finally, results indicate that reliance on self-report for clinical and research characterization of those with an ASD should be considered carefully, particularly with regard to autistic traits, as poor awareness of autism-related traits may lead to an under-reporting of autism symptoms and over-reporting of social competency.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, text revision (4th ed.). Washington, DC: American Psychiatric Association.
Baldwin, W. (2000). Information no one else knows: The value of self-report. In A. A. Stone, J. S. Turkkan, C. A. Bachrach, J. B. Jobe, H. S. Kurtzman, & V. S. Cain (Eds.), The science of self-report: Implications for research and practice (pp. 3–7). Mahwah, NJ: Lawrence Erlbaum Associates.
Baron-Cohen, S., & Wheelwright, S. (2004). The empathy quotient: An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. Journal of Autism and Developmental Disorders, 34(2), 163–175.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The Autism-Spectrum Quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31(1), 5–17.
Baron-Cohen, S., Richler, J., Bisarya, D., Gurunathan, N., & Wheelwright, S. (2003). The systemizing quotient: An investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. In U. Frith & E. Hill (Eds.), Autism: Mind and brain (pp. 161–186). New York, NY: Oxford University Press.
Baron-Cohen, S., Hoekstra, R. A., Knickmeyer, R., & Wheelwright, S. (2006). The Autism-Spectrum Quotient (AQ)—adolescent version. Journal of Autism and Developmental Disorders, 36(3), 343–350.
Butzer, B., & Konstantareas, M. M. (2003). Depression, temperament and their relationship to other characteristics in children with Asperger’s disorder. Journal on Developmental Disabilities, 10(1), 67–72.
Capps, L., Sigman, M., & Yirmiya, N. (1995). Self-competence and emotional understanding in high-functioning children with autism. Development and Psychopathology, 7(1), 137–149.
Frith, U. (1989). Autism: Explaining the enigma. Oxford: Blackwell.
Frith, U., & Happé, F. (1999). Theory of mind and self-consciousness: What is it like to be autistic? Mind & Language, 14(1), 1–22.
Green, J., Gilchrist, A., Burton, D., & Cox, A. (2000). Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. Journal of Autism and Developmental Disorders, 30(4), 279–293.
Hill, E. L., & Frith, U. (2003). Understanding autism: Insights from mind and brain. In U. Frith & E. L. Hill (Eds.), Autism: Mind and brain (pp. 1–19). New York, NY: Oxford University Press.
Himle, J. A., Van Etten, M. L., Janeck, A. S., & Fischer, D. J. (2006). Insight as a predictor of treatment outcome in behavioral group treatment for obsessive compulsive disorder. Cognitive Therapy and Research, 30(5), 661–666.
Kanner, L. (1973). Childhood psychosis: Initial studies and new insights. Oxford: V. H. Winston.
Knott, F., Dunlop, A.-W., & Mackay, T. (2006). Living with ASD. Autism, 10(6), 609–617.
Koning, C., & Magill-Evans, J. (2001). Social and language skills in adolescent boys with Asperger syndrome. Autism, 5(1), 23–36.
Lainhart, J. E., & Folstein, S. E. (1994). Affective disorders in people with autism: A review of published cases. Journal of Autism and Developmental Disorders, 24(5), 587–601.
Ling, J., Burton, T., Salt, J., & Muncer, S. J. (2009). Psychometric analysis of the systemizing quotient (SQ) scale. British Journal of Psychology, 100(3), 539–552.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview—revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(5), 659–685.
Owens, J., Goldfine, M., Evangelista, N., Hoza, B., & Kaiser, N. (2007). A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clinical Child and Family Psychology Review, 10, 335–351.
Perner, J., Frith, U., Leslie, A. M., & Leekam, S. R. (1989). Exploration of the autistic child’s theory of mind: Knowledge, belief, and communication. Child Development, 60(3), 689–700.
Premack, D., & Woodruff, G. (1978). Does the chimpanzee have a theory of mind? Behavioral and Brain Sciences, 1(4), 515–526.
Sterling, L., Dawson, G., Estes, A., & Greenson, J. (2008). Characteristics associated with presence of depressive symptoms in adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 38(6), 1011–1018.
Storch, E. A., Merlo, L. J., Larson, M. J., Marien, W. E., Geffken, G. R., Jacob, M. L., et al. (2008). Clinical features associated with treatment-resistant pediatric obsessive compulsive disorder. Comprehensive Psychiatry, 49(1), 35–42.
Tager-Flusberg, H. (2007). Evaluating the theory-of-mind hypothesis of autism. Current Directions in Psychological Science, 16(6), 311–315.
Vickerstaff, S., Heriot, S., Wong, M., Lopes, A., & Dossetor, D. (2007). Intellectual ability, self-perceived social competence, and depressive symptomatology in children with high-functioning autistic spectrum disorders. Journal of Autism and Developmental Disorders, 37(9), 1647–1664.
Wechsler, D. (1999). Wechsler abbreviated scale of intelligence (4th ed.). San Antonio, TX: The Psychological Corporation.
Acknowledgments
This project was supported by a Health Research Project Grant (PSO 2007-3410) from the Nova Scotia Health Research Foundation to S. A. Johnson. Data for this study were collected, in part, in the Clinical and Cognitive Neuroscience Laboratory of Dr. Julie C. Stout at Indiana University. Some of these findings were presented in poster format at the International Meeting for Autism Research (IMFAR) in May, 2008 in London, England and at the Annual Convention of the Canadian Psychological Association in June, 2008 in Halifax, Nova Scotia. We thank Jodie Baker and Alison Murton for their assistance with data collection. J. H. Filliter is supported by funding from the Killam Trusts, the Natural Sciences and Engineering Research Council of Canada, and the Autism Research Training Program.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Johnson, S.A., Filliter, J.H. & Murphy, R.R. Discrepancies Between Self- and Parent-Perceptions of Autistic Traits and Empathy in High Functioning Children and Adolescents on the Autism Spectrum. J Autism Dev Disord 39, 1706–1714 (2009). https://doi.org/10.1007/s10803-009-0809-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-009-0809-1