
Abstract
The effectiveness of a social skills training group for adolescents with Asperger syndrome and high-functioning autism (AS/HFA) was evaluated. Parents of six groups of adolescents (n = 46, 61% male, mean age 14.6) completed questionnaires immediately before and after the 12-week group. Parents and adolescents were surveyed regarding their experience with the group. Significant pre- to post-treatment gains were found on measures of both social competence and problem behaviors associated with AS/HFA. Effect sizes ranged from .34 to .72. Adolescents reported more perceived skill improvements than did parents. Parent-reported improvement suggests that social skills learned in group sessions generalize to settings outside the treatment group. Larger, controlled studies of social skills training groups would be valuable.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
As individuals with autism spectrum disorders enter adolescence and adulthood, their interest in social interactions often increases (Kanner, Rodriguez, & Ashenden, 1972; Schopler & Mesibov, 1983). However, persistent social skill deficits may impede them from forming relationships. High-functioning autistic adolescents, in particular, become more keenly aware of the difficulties they encounter when interacting with peers. At a time when “fitting in” is of overriding importance, these young people may find themselves isolated, rejected or even bullied at school. They can be at risk for low self-esteem, depression and anxiety disorders. As they approach adulthood, lack of social competence may also become a barrier to vocational opportunities (Howlin, 2000; Krasny, Williams, Provencal, & Ozonoff, 2003).
Several centers have developed social skills interventions to address the needs of adolescents with autism, but few have reported on their efforts. Most reports of social skills interventions are case series describing training on an individual basis (Rogers, 2000). Such interventions have focused on different aspects of social skills deficits in autism, grouped by Gresham, Sugai, and Horner (2001) into deficits in acquisition, performance and fluency of social skills. Interventions that have addressed deficits in acquisition of social knowledge include “social stories” (Gray, 1994a), “comic strip conversations” (Gray, 1994b), and “hidden curriculum” (Bieber, 1994), which make explicit the unspoken rules and meanings in social situations via stories and pictures. Interventions targeting inadequate or inappropriate performance of social behaviors include “social autopsies” (Bieber, 1994), where problem-solving and positive reinforcement are used to enhance social learning. Interventions that help increase fluency of appropriate social behaviors through exposure and practice include “social scripts,” where adolescents may carry cards with responses they may use in the course of different interactions (Barnhill, 2002). In addition, interventions specifically targeting theory of mind have been developed, where role plays, pictures and games have been used to teach perspective-taking (Howlin, Baren-Cohen, & Hadwin, 1999; Ozonoff & Miller, 1995).
Gresham et al. (2001) identified a number of strategies to promote skill acquisition, generalization and maintenance, including teaching social skills in a natural setting, using active modeling of behaviors, and coaching and reinforcement procedures. Delivering social skills training in a group format may facilitate the use of these strategies by allowing adolescents to practice social skills through interacting with their peers, with guidance from group leaders. Fun group activities may also increase adolescents’ motivation to spend time with their peers and to develop friendship skills. A few group social skills interventions have been evaluated; three groups tailored to the adolescent age group are described here.
Mesibov (1984) was one of the first to describe a social skills training group, implemented with 15 verbal autistic adolescents and adults (ages 14–35). This open-ended program combined individual teaching with weekly group sessions that involved open discussion, skills practice, role-playing and a “joke time.” Feedback from participants and their families was positive, but no objective measures of improvement were used.
Two systematic studies of social skills training for adolescents were found. Ozonoff and Miller (1995) reported on a 4-1/2 month training program for high-functioning autistic adolescents that taught theory of mind, as well as conversation skills, through role play and other activities. The five adolescents in the treatment group made gains on several theory of mind tasks, where the four adolescents in the control group made no gains. However, there was no change on parent and teacher ratings of social competence for either group, suggesting that skills learned in the group did not generalize to other settings.
Sloman and Leef (2004) reported on an 8- to 10-week group for 9–14-year-olds with Asperger syndrome that ran concomitantly with a group for parents. This group was similar to the one described here, with a new social skill taught each week using role-play exercises, followed by a recreational time. Significant pre- to post-treatment gains were found on a parent-rated measure of social, emotional, and communication skills.
At the Montreal Children’s Hospital, a basic social skills training group was recently developed to meet the needs of adolescents with Asperger syndrome and high-functioning autism (AS/HFA). In the past 3 years, we have requested that parents complete rating scales before and after their children participate in the 12-week group. We wanted to know if our efforts to teach social skills to these young people had effects on their behavior. We hypothesized that participation in the group would have a specific effect on measures of social competence, but not on measures of other problem behaviors associated with AS/HFA that are not targeted by the intervention.
Methods
Subjects
Adolescents ages 13–18 were referred to the group from psychiatry and community clinics across the McGill University network. Criteria for inclusion in the group were: a diagnosis of an autism spectrum disorder by a child psychiatrist, adequate language skills for participation in activities as described below, and willingness to attend. This was a clinical sample, not recruited for research. Formal tests of intelligence and language were not performed. Most adolescents were in a regular school, but this information was not always recorded. Adolescents were initially screened with their parents to discuss what gains they and their families hoped would be achieved in the group. If adolescents were able to talk about their interests and to verbalize some goals for participation, they were considered suitable for the group.
Intervention
The group curriculum combined psychoeducational and experiential methods of teaching social skills, with emphasis on learning through role play. Each group enrolled 7–8 adolescents. The groups were led by a social worker and psychologist experienced in working with adolescents in psychiatry, and, for one group, included a psychiatric resident as a third co-leader. Group leadership required 2 h per week for each clinician for 14 weeks (assessments, planning and preparation, group time, feedback sessions).
The groups met weekly for 12 weeks. Meetings were 1-1/2 h in duration and were held in the late afternoon, following the usual school day. Meetings were held in the conference room of the child and adolescent psychiatry clinic. At the first meeting, the group rules were explained. These rules include: keeping what is said confidential, arriving on time, attending every week, participating in all activities, and a “no tolerance for violence” policy. Each group meeting followed a standard sequence of activities, as follows:
-
(1)
Check-in: Each member discusses events and problems from their week. Other members are encouraged to ask questions and offer suggestions.
-
(2)
Review of last week’s skill: Leaders ask if members had a chance to practice the previous skill.
-
(3)
Introduction of new skill: Members are asked to talk about their ideas on a particular social skill. Members may be given a card describing the new skill.
-
(4)
Role play: Members practice the new skill in pairs, one pair at a time, while the rest of the group watches and gives feedback.
-
(5)
Snack break: Members are encouraged to interact with one another during the break.
-
(6)
Activity: Group games such as charades are played.
-
(7)
Closing: Members are encouraged to say goodbye to each other.
Many of the exercises used to teach new skills were adapted from the book: Skillstreaming the Adolescent (Goldstein & McGinnis, 2000). This book was developed for use with youths with behavioral issues, and not specifically for adolescents with AS/HFA. Several other skills training manuals of this type are available (Walker et al., 1983). Skills that were covered in the groups are listed in Table 1, along with examples of role play activities used to teach the skills.
The pace of introduction of new skills was flexible and dependent on the needs of group members. In the first session, members’ ideas, and sometimes misconceptions, about AS/HFA were solicited and addressed. The group program includes a trip to a semi-formal restaurant, where dining etiquette skills are practiced. At the last (12th) session, the group celebrates with an activity of their choice, which has most often been a pizza party. Group members are invited to return for “alumni” parties twice a year. They are again encouraged to interact with other members, familiar and unfamiliar, at these parties. The group program has been reported in further detail elsewhere (Strulovitch & Tagalakis, 2003).
Measures
Parents were asked to complete three questionnaires immediately before and after the 12-week group: the Social Responsiveness Scale (SRS), the Aberrant Behavior Checklist (ABC), and the Nisonger Child Behavior Rating Form (N-CBRF). The reliability and validity of all three scales has been established, and all three have been used in treatment studies (McCracken & Research Units on Pediatric Psychopharmacology Autism Network, 2002; Pine, Luby, Abbacchi, & Constantino, 2006; Shea et al., 2004).
The SRS is a 65-item informant-based measure of children’s social competence, where social deficits are represented as quantitative traits rated on a 4-point Likert scale (Constantino, Przybeck, Friesen, & Todd, 2000). There are five treatment subscales: “Social Awareness” (eight items), “Social Cognition” (12 items), “Social Communication” (22 items), “Social Motivation” (11 items) and “Autistic Mannerisms” (12 items) that are sensitive to change in social deficits, and three “DSM-oriented” subscales measuring “Social Aspects” (47 items), “Language Aspects” (six items) and “Preoccupations and Mannerisms” (12 items) of autism as described in DSM-IV (John Constantino, Personal communication; see American Psychiatric Association, 2000).
The ABC is a 58-item informant-based measure of problem behaviors of people with developmental disabilities, rated on a 4-point Likert scale (Aman, Singh, Stewart, & Field, 1985). There are five subscales: “Irritability” (15 items), “Lethargy, Social Withdrawal” (16 items), “Stereotypic Behavior” (seven items), “Hyperactivity” (16 items) and “Inappropriate Speech” (four items). Alpha coefficients have ranged from 0.77 to 0.95 across subscales (Brown, Aman, & Havercamp, 2002).
The N-CBRF is a 70-item informant-based measure of emotional and behavioral problems of children and adolescents with developmental disabilities (Aman, Tasse, Rojahn, & Hammer, 1996). It has considerable overlap of content with the Aberrant Behavior Checklist (ABC), but is intended more for assessment purposes, whereas the ABC is intended to monitor treatment effectiveness. In addition, two “Social Competence” subscales, “Compliant/Calm” (six items) and “Adaptive Social” (four items), allow informants to comment on the child’s strengths. There are six “Problem Behavior” subscales: “Conduct Problems” (16 items), “Insecure/Anxious” (15 items), “Hyperactive” (nine items), “Self-Injury/Stereotypic” (seven items), “Self-Isolated/Ritualistic” (eight items) and “Overly Sensitive” (five items). Items are rated on a 4-point Likert scale. Subscales are highly correlated with analogous subscales on the Aberrant Behavior Checklist. Alpha coefficients have ranged from 0.73 to 0.93.
An adolescent feedback survey was introduced in the past year for the two most recent groups. This anonymous survey contained Likert-type scales on which adolescents could rate whether they liked the group and to what extent they felt that they had improved on skills learned in the group. Response modalities for the amount of improvement were: “none,” “a little,” “some,” and “a lot.” There were also open-ended questions about what they liked best/least and suggestions for future groups.
Parents in the first group were surveyed on their impressions regarding the group, as well. This procedure was unfortunately neglected for subsequent groups, but was reinstated in the past year for the two most recent groups. The parent survey contained Likert-type scales on which parents could rate perceived change in their child’s social behavior over the course of the group. Response modalities for the amount of change on specific skills were: “worse,” “same,” “a little better,” “better,” and “a lot better.” An expanded scale was used for the amount of overall change perceived. In addition, there were open-ended questions regarding the parent’s perception of their child’s experience in the group, and suggestions for future groups.
Data Analysis
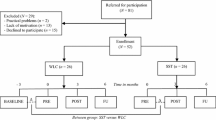
Social competence was measured using the SRS and the N-CBRF Positive Social (N-CBRF-PS) scale. Problem behaviors were measured using the ABC and the N-CBRF Problem Behavior (N-CBRF-PB) scale. The Statistical Package for the Social Sciences (SPSS version 11.0.1) was used to perform Wilcoxon matched-pairs tests to examine pre- to post-group change for total and subscale scores on these measures. Student’s t-tests for matched pairs were also performed and generally led to similar p-values but, given the small sample size and the greater robustness of non-parametric statistics, p-values associated with Wilcoxon tests are reported. The impact of age, gender and medication status (medication prescribed or not prescribed) on outcomes was evaluated using t-tests, where age was converted into a dichotomous variable (age 14 and under versus age 15 and over). Differences among scores for subjects for whom data was complete or incomplete were also examined using t-tests. The relationship between categories of overall improvement on parent feedback questionnaires and outcomes on standardized continuous measures was examined by comparing mean scale scores across response categories.
Results
Sample Characteristics
Data is available for six groups of adolescents whose parents completed questionnaires. A total of 46 adolescents (61% male) were enrolled in the groups. Special recruitment efforts were made to include at least two females in each group, explaining the somewhat low male:female ratio for a high-functioning sample. The mean age at enrollment was 14.6 years (SD 1.7), with 31 subjects age 14 years and under, and 15 subjects age 15 years and over. Seventeen adolescents (37%) were taking psychotropic medication, including atypical antipsychotics (n = 6), selective serotonin reuptake inhibitors (n = 5) or methylphenidate (n = 5).
The mean total scores before treatment on the SRS, ABC, N-CBRF-PB and N-CBRF-PS were similar to scores found in previous samples of youth with pervasive developmental disorders (see Tables 2 and 3; Brown et al., 2002; Constantino et al., 2004; Tasse, Aman, Hammer, & Rojahn, 1996).
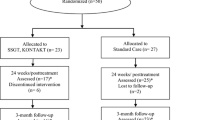
Missing Data
One participant dropped out after two meetings, and another was asked to leave the group after becoming physically aggressive during a meeting. Of the remaining 44 adolescents, complete pre- and post-group data is available on the SRS for 32 individuals, and on the ABC and N-CBRF for 30 individuals. More data is available for later groups, as different methods of ensuring that questionnaires were returned were tried with successive groups. Currently, post-group questionnaires are completed at post-group feedback meetings held with each adolescent’s parents. In the past, questionnaires sent home for completion were often not returned. No significant differences in age (mean 14.3 years vs. 15.0 years, p = .17), gender (58.6% vs. 64.7% males, p = .76) or baseline total scores on outcome measures (SRS mean 96.7 vs. 102.4, p = .58; ABC mean 41.9 vs. 51.5, p = .31; N-CBRF-PB mean 51.3 vs. 69.7, p = .11; N-CBRF-PS mean 13.9 vs. 12.5, p = .37) were found for adolescents with complete versus incomplete data sets.
Adolescents for whom parents completed feedback surveys had significantly greater improvement on the ABC total score and “Irritability” and “Hyperactivity” subscales than those for whom feedback was unavailable (ABC mean difference 22.41 vs. 3.38, p = .006; “Irritability” mean difference 6.82 vs. 0.43, p = .003; “Hyperactivity” mean difference 5.76 vs. −0.21, p = .010). Change on other outcome measures was not significantly different between these groups.
Social Competence
Supporting the hypothesis that the social skills group would have positive effects on social competence, significant improvement was found on the total scores for the SRS and the N-CBRF-PS (Table 2). The direction of change for all subscale scores suggested a robust trend towards social competence gains. Of the 12 pre- to post-treatment differences, six were statistically significant, two were not significant, and four fell just short of statistical significance. Effect sizes for subscales where improvement was statistically significant ranged from .34 to .46, and were of comparable magnitude for the SRS and the N-CBRF-PS scores. It is worth noting that of the three DSM oriented subscales of the SRS, the largest improvement was found for the DSM Social score, with an effect size roughly twice as high as that observed for the two other DSM domain scores. The post-treatment total score on the SRS still fell within the expected range for adolescents with autistic spectrum disorders. Age (14 and under vs. 15 and over), gender and medication status (usage vs. no usage of psychotropic medications) did not have significant effects on treatment outcome (data not shown).
Problem Behaviors
Significant improvements were also found on measures of problem behaviors associated with AS/HFA, including all subscales of the ABC and the N-CBRF-PB, except for the “Hyperactivity” subscale of the N-CBRF-PB (Table 3). Effect sizes ranged from .34 to .72, with the largest effects found on the “Irritability” and “Overly sensitive” subscales, and on the ABC total score. Age had a significant effect on outcome on the “Irritability” subscale, where greater improvements were found for subjects age 14 and under, compared to older subjects (mean difference 5.33 vs. 1.00, p = .045). No other effects of age, gender or medication status on treatment outcome were found.
Feedback Surveys
Thirteen adolescents (from two groups) completed anonymous feedback surveys. Ten of the adolescents reported liking the group; five of the ten reported that they “liked it a lot.” One adolescent reported disliking the group; no reason was given. The most improvement was reported for “having a conversation,” with seven adolescents reporting “a lot” of improvement and five reporting “some” improvement. Modal responses included “a little” improvement for “recognizing body language” and “making small talk,” “some” improvement for “meeting new people,” and “a lot” of improvement for “handling teasing” and “self-confidence.” All except one adolescent reported having made friends in the group.
Seventeen parents (from three groups) completed feedback surveys. Fifteen parents reported that their child seemed happy to attend the group. Ten parents reported “a little” overall improvement in their child’s social behavior, while three parents reported that it was “the same,” and three reported that it was “much better” or “very much better.” Mean pre- to post-treatment differences for adolescents whose parents reported that behavior was “the same,” “a little better” or “much/very much better” were, respectively: 12.00 vs. 6.83 vs. 20.33 for the SRS total score; −3.67 vs. −1.50 vs. −6.50 for the N-CBRF-PS; 8.00 vs. 16.67 vs. 38.00 for the ABC total score; and 2.50 vs. 8.67 vs. 49.00 for the N-CBRF-PB. Therefore, differences were generally comparable for the “same” and “a little better” groups, but much larger for the “much/very much better” group, especially on problem behavior measures. Many parents requested more parent involvement in the group, or a parallel parent group. Many also asked for continued involvement of adolescents with the group, including continued contact with other families, or independent living skills/job training for adolescents.
Discussion
The results of this preliminary study indicate that social skills groups can be an effective way of helping verbal adolescents with autism spectrum disorders to develop comfort and confidence in social interactions. This is, to our knowledge, the first study of social skills training that uses a validated, normed measure of social functioning in autism. Parent-reported improvement suggests that social skills that are learned generalized to settings outside the treatment sessions. Responses on feedback surveys suggest that adolescents perceived more improvement in their social skills than did their parents. Their willingness to attend the group (a requirement for inclusion in the group) likely translated into greater motivation to learn social skills and may have augmented their perception of gains made in the group. On the other hand, they may have been more aware of their gains than their parents might have been.
The magnitude of gains in social skills was similar on the SRS and N-CBRF-PS, indicative of a moderate effect. However, some results on SRS subscales were suggestive of specificity of treatment effects. Of the three DSM subscales, the only statistically significant gain was detected on “Social Aspects” of autism, whereas, in line with the treatment goals and expectations, no improvement was seen on the two other DSM subscales tapping into language and stereotypic features of autism. The results for all of the social subscales of the SRS were of similar magnitude, with the exception of the “Social Awareness” subscale. The lack of effect on this subscale could be due to the relative difficulty, for parents, in determining change in adolescents’ awareness of social cues versus their observable social behaviors. Alternatively, this subscale had a small number of items, and therefore may not have reliably detected a change in a small sample.
Contrary to our initial predictions, improvements were also found for a range of problem behaviors associated with autism spectrum disorders, including affect regulation problems, anxiety, self-isolation, stereotypic behaviors and self-injurious behaviors. Interestingly, the improvements for externalizing behaviors as measured by the two hyperactivity subscales or the conduct problem subscale were either non-significant or associated with smaller effect sizes. These behaviors were the least likely to improve as a result of the social skills training intervention, therefore suggesting that some, but not all, behavior problems might represent secondary targets for social skills interventions, and that the improvements reported by parents in this study do not merely results from rater biases or expectations. Moderate to large effect sizes on the ABC were comparable to pre–post effect sizes found in a study of risperidone in aggressive adolescents (Buitelaar, van der Gaag, Cohen-Kettenis, & Melman, 2001).
A greater degree of improvement found on the ABC for adolescents whose parents completed feedback surveys suggests that the available feedback may not be representative of the impressions of all parents involved. The relationship between parent-reported improvement on feedback surveys and improvement on measures of problem behaviors was generally in the expected direction, although differences between the “same” and “a little better” were difficult to detect. The magnitude of improvement associated with a response of “much/very much better” on feedback questionnaires was larger on all measures, but especially for those questionnaires tapping non-specific behavior problems. As these results were obtained on a very small sample of respondents, caution is required in interpreting these trends.
Non-specific therapeutic factors, such as supportive relationships formed with the therapists and with other group members, may also have contributed to changes in subscales tapping into adolescents’ emotional state, including “Irritability” and “Overly Sensitive”. Other authors have also found improvements in problem behaviors that were not directly targeted in social skills training (Bodfish, 2004).
This study was limited by a number of factors, including a small sample size (further reduced by missing data) and the absence of a control group. The social skills groups were offered in response to a clinical need, and subjects were not recruited for research, but were referred by treating clinicians. More accurate description of the sample (IQ, language ability) is desirable but unavailable. Formal recruitment efforts would likely be necessary to perform a larger study, particularly if randomization to treatment and control groups is desired. The absence of a control group leaves unanswered the question of whether positive results are due to test attenuation or spontaneous improvement versus to group participation. That said, some findings were suggestive of specific improvements that would appear related to the intervention, and effect sizes are larger than placebo effects in a randomized study of risperidone in autistic children performed over a similar time frame (McCracken & Research Units on Pediatric Psychopharmacology Autism Network, 2002).
Another limitation of this study is the use of only parent-report measures to test for quantitative evidence of improvement. Group participants, their peers and their teachers may have had different perceptions regarding changes in participants’ social behaviors. A measure of global adaptive functioning may also have been informative. Furthermore, it is not possible to know whether treatment gains were maintained, as follow-up data is not available.
Medication use was not monitored over the course of the group. While no differences were found between outcomes for subjects taking versus not taking medication, medication effects cannot be entirely ruled out as a confounding variable in this study.
An additional limitation of this study is that the group program was not manualized, so that programming differed slightly between groups. As well, the clinicians running the group had experience in working with adolescents and in teaching social skills, but were not initially specifically trained in techniques used with the pervasive developmental disorders population. The intervention does not incorporate many of the new social skills training techniques developed for this population. On the other hand, it is striking that moderate effect sizes on measures of social competence and problem behaviors were demonstrated despite these shortcomings. The apparent efficacy of this simple, low-cost intervention suggests that the social deficits of adolescents with AS/HFA can be readily addressed. Moreover, adolescents and parents reported general satisfaction with the treatment and identified specific gains. This finding may be somewhat discordant with previous studies of social skills training, where poor generalization of treatment effects suggested that more intensive treatment (>30 h) might be necessary (Gresham et al., 2001). More research into psychosocial interventions for these adolescents is clearly needed. Studies of manualized interventions would allow other centers to replicate the program and pool outcomes for evaluation. Equally, future studies should address whether or not the addition of a parallel group for parents enhances treatment effects.
This study is valuable in its examination of a “real-world” service-oriented program, initially developed in response to clinical needs rather than as a research initiative. Many centers seek evidence that the clinical programs they offer represent an efficient use of resources. Simply-designed effectiveness studies can be a first step toward examining efficiency. The results of this preliminary study indicate that larger, controlled studies of social skills training for verbal adolescents with autism spectrum disorders would be important.
References
Aman, M. G., Singh, N. N., Stewart, A. W., & Field, C. J. (1985). The aberrant behavior checklist: A behavior rating scale for assessment of treatment effects. Journal of Mental Deficiency, 89, 485–491.
Aman, M. G., Tasse, M. J., Rojahn, J., & Hammer, D. (1996). The Nisonger Child Behavior Rating Form: A child behavior rating form for children with developmental disabilities. Research in Developmental Disabilities, 17, 41–57.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders IV. Washington, D.C.: American Psychiatric Association.
Barnhill, G. P. (2002). Designing social skills interventions for students with Asperger syndrome. National Association of School Psychologists Communique, 31, 3.
Bieber, J. (1994). Learning disabilities and social skills with Richard Lavoie: Last one picked, first once picked on. Washington, D.C.: Public Broadcasting Service.
Bodfish, J. W. (2004). Treating the core features of autism: Are we there yet? Mental Retardation and Developmental Disabilities Research Reviews, 10, 318–326.
Brown, E. C., Aman, M. G., & Havercamp, S. M. (2002). Factor analysis and norms for parent ratings on the aberrant behavior checklist – community for young people in special education. Research in Developmental Disabilities, 23, 45–60.
Buitelaar, J. K., van der Gaag, R. J., Cohen-Kettenis, P., & Melman, C. T. (2001). A randomized controlled trial of risperidone in the treatment of aggression in hospitalized adolescents with subaverage cognitive abilities. Journal of Clinical Psychiatry, 62, 239–248.
Constantino, J. N., Gruber, C. P., Davis, S., Hayes, S., Passanante, N., & Przybeck T. (2004). The factor structure of autistic traits. Journal of Child Psychology and Psychiatry, 45, 719–726.
Constantino, J. N., Przybeck, T., Friesen, D., & Todd, R. D. (2000). Reciprocal social behavior in children with and without pervasive developmental disorders. Journal of Developmental and Behavioral Pediatrics, 21, 2–11.
Goldstein, A. P., & McGinnis, E. (2000). Skillstreaming the adolescent: New strategies and perspectives for teaching prosocial skills. Champaign: Research Press.
Gray, C. (1994a). The new social story book. Arlington: Future Horizons.
Gray, C. (1994b). Comic strip conversations. Arlington: Future Horizons.
Gresham, F. M., Sugai, G., & Horner, R. H. (2001). Interpreting outcomes of social skills training for students with high-incidence disabilities. Exceptional Children, 67, 331–344.
Howlin, P. (2000). Outcome in adult life for more able individuals with autism or Asperger syndrome. Autism, 4, 63–83.
Howlin, P., Baron-Cohen, S., & Hadwin, J. (1999). Teaching children with autism to mind-read: A practical guide. New York: John Wiley and Sons.
Kanner, L., Rodriguez, A., & Ashenden, B. (1972). How far can autistic children go in matters of social adaptation? Journal of Autism and Childhood Schizophrenia, 2, 9–33.
Krasny, L., Williams, B. J., Provencal, S., & Ozonoff, S. (2003). Social skills interventions for the autism spectrum: Essential ingredients and a model curriculum. Child and Adolescent Psychiatric Clinics of North America, 12, 107–122.
McCracken, J. T., & Research Units on Pediatric Psychopharmacology Autism Network. (2002). Risperidone in children with autism and serious behavioral problems. New England Journal of Medicine, 347, 314–321.
Mesibov, G. B. (1984). Social skills training with verbal autistic adolescents and adults: A program model. Journal of Autism and Developmental Disorders, 14, 395–403.
Ozonoff, S., & Miller, J. N. (1995). Teaching theory of mind: A new approach to social skills training for individuals with autism. Journal of Autism and Developmental Disorders, 25, 415–433.
Pine, E., Luby, J., Abbacchi, A., & Constantino, J. N. (2006). Quantitative assessment of autistic symptomatology in preschoolers. Autism, 10, 344−352.
Rogers, S. J. (2000). Interventions that facilitate socialization in children with autism. Journal of Autism and Developmental Disorders, 30, 399–409.
Schopler, E., & Mesibov, G. B. (1983). Autism in adolescents and adults. New York: Plenum Press.
Shea, S., Turgay, A., Carroll, A., Schulz, M., Orlik, H., Smith, I., & Dunbar, F. (2004). Risperidone in the treatment of disruptive behavioural symptoms in children with autistic and other pervasive developmental disorders. Pediatrics, 114, 634–641.
Sloman, L., & Leef, J. (2004). Child social interaction and parental self-efficacy: Evaluating simultaneous groups for children with Asperger Syndrome and their parents. In K. P. Stoddart (Ed.), Children, youth and adults with Asperger Syndrome (pp. 253–267). London: Jessica Kingsley Publishers.
Strulovitch, J., & Tagalakis, V. (2003). Social skills groups for adolescents with Asperger syndrome. Perspectives on Language, Learning and Education, 10, 20–22.
Tasse, M. J., Aman, M. G., Hammer, D., & Rojahn, J. (1996). The Nisonger Child Behavior Rating Form: Age and gender effects and norms. Research in Developmental Disabilities, 17, 59–75.
Walker H. M., McConnell S., Holmes D., Todis B., Walker B., & Golden, N. (1983). The Walker social skills curriculum: The accepts program. Pro-Ed, Austin.
Acknowledgments
The authors thank Micha Huynh and Sylvie Lafleur for their help in the preparation of this paper. Preliminary results of this project were presented at the Joint Annual Meeting of the American and Canadian Academies of Child and Adolescent Psychiatry in Toronto, 2005.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tse, J., Strulovitch, J., Tagalakis, V. et al. Social Skills Training for Adolescents with Asperger Syndrome and High-Functioning Autism. J Autism Dev Disord 37, 1960–1968 (2007). https://doi.org/10.1007/s10803-006-0343-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-006-0343-3