
Abstract
In this study we examined early motor, vocal, and communicative development in a group of younger siblings of children diagnosed with autism (Infant Siblings). Infant Siblings and no-risk comparison later-born infants were videotaped at home with a primary caregiver each month from 5 to 14 months, with follow-up at 18 months. As a group, Infant Siblings were delayed in the onset of early developmental milestones and spent significantly less time in a greater number of postures, suggestive of relative postural instability. In addition, they demonstrated attenuated patterns of change in rhythmic arm activity around the time of reduplicated babble onset; and they were highly likely to exhibit delayed language development at 18 months.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A diagnosis of ASD is based on a constellation of symptoms, including both the presence of certain atypical behaviors (e.g., repetitive behaviors, persistent preoccupation with parts of objects) and the relative absence of (or significant developmental delays in) others (e.g., mutual eye gaze, gestures, language, symbolic play; American Psychiatric Association 1994). Because the diagnosis involves delayed development in domains such as pointing, language, and symbolic play, clinicians must wait until well after children have reached the typical age of emergence for such behaviors before considering a diagnosis of ASD. Despite growing evidence that ASD is a genetically-based neurodevelopmental disorder (e.g., see Folstein and Rosen-Sheidley, 2001; Spence, 2001; Szatmari, Jones, Zwaigenbaum, & McLean, 1998, for reviews) and the fact that many parents report suspecting a problem prior to 12 months (e.g., Coonrod & Stone, 2004; Stone, Hoffman, Lewis, & Ousley, 1994), the general consensus is that ASD cannot be diagnosed reliably before age two (e.g., see Rogers, 2001).
This fact has led to a surge of interest in the identification of early behavioral markers of risk for a later ASD diagnosis. The data to be reported in the current paper were collected as part of an ongoing longitudinal study designed to address this issue through the identification of early indicators of an eventual ASD diagnosis. Our focus is on the later-born infant siblings of children diagnosed with autism. These infant siblings are themselves at especially high risk for an autism or ASD diagnosis (e.g., Zwaigenbaum et al., 2005; see also Zwaigenbaum et al., 2006). The larger ongoing study observes infants prospectively at monthly intervals from the ages of 5–14 months with follow-up at 3-month intervals from 18 to 36 months. In this paper, results from the monthly visits and the 18-month follow-up will be presented.
Because the goal of this research is to identify early indicators, ideal behaviors for observation would be frequently occurring, spontaneous, salient to observers, characteristic of young infants, and in areas known to be impaired in older children with ASD. This led us to focus on motor and speech/language functioning. Spontaneous motor and speech/language-related (i.e., vocalization) behaviors are frequent in young infants; and there is growing evidence from typically developing infants that the motor and oral/vocal systems are closely linked, mutually influential from birth, and exhibit developmentally significant transitional forms that are relatively easy to observe (for a review, see Iverson & Thelen, 1999). In addition, as indicated below, there is a substantial literature documenting the existence of disorders in motor and speech/language functioning in older children with ASD and some indication that infants eventually diagnosed with ASD may manifest these disorders as well.
Movement and Postural Disorders in Young Children with ASD
Movement disorders appear to be relatively common among children with ASD. Indeed, some authors have speculated that movement disturbances may be directly related to the core symptoms of ASD (e.g., Leary & Hill, 1996). For example, in older children, clumsiness (e.g., Jones & Prior, 1985), difficulty with tasks involving coordinated sequences of movements (e.g., Vernazza-Martin et al., 2005; Wing, 1969), gait abnormalities (e.g., shorter steps, slower pace, unusual arm positions; Damasio & Maurer, 1978; Teitelbaum, Teitelbaum, Nye, Fryman, & Maurer, 1998; Vilensky, Damasio, & Maurer, 1981), and reduced postural stability (Minshew, Sung, Jones, & Furman, 2004) have been reported. Other investigators have indicated that children with ASD perform worse than typically developing children of the same chronological age and like children with developmental delays and younger, mental-age-matched typically developing children on standardized measures of motor skill (Hauck & Dewey, 2001; Manjiviona & Prior, 1995).
Retrospective studies of infants eventually diagnosed with ASD have not generally focused on movement, but those that have included observations of motor behaviors have reported patterns of movement disturbance. In a retrospective video study using movement analysis, for example, Teitelbaum et al. (1998) reported that of 17 infants later diagnosed with ASD, all showed at least some abnormal movement patterns during the first year (e.g., atypical organization of body segments when rolling from prone to supine, inability to maintain balance while sitting independently). Related disturbances reported by others include hypotonia (Adrien et al., 1991, 1992), postural instability (Kroeker, 2000), and unusual posturing (Baranek, 1999). In a review of the early medical screening records of 18-month-old children eventually diagnosed with ASD, Johnson, Siddons, Frith, and Morton (1992) observed a marginal tendency for greater problems in motor development for this group relative to randomly selected children eventually identified as having learning disabilities and to typically developing children. Finally, in a chart-based case study of a single infant with autism, Dawson, Osterling, Meltzoff, and Kuhl (2000) reported numerous examples of motor difficulties beginning in the first 6 months and continuing throughout the first year. These included disturbances in muscle tone, poorly integrated movements, toe walking, and absence of a coordinated stepping pattern. Findings such as these underscore the importance of examining motor functioning for early identification of children with ASD.
Language Disorders in Young Children with ASD
Although nearly 50% of individuals with ASD develop some functional speech (Lord & Paul, 1997), language skills within this population are widely variable. Of the children who ultimately acquire some language, most experience substantial delays in language development and specific deficits in the areas of language comprehension and pragmatics (see Tager-Flusberg, Paul, & Lord, 2005, for a recent review).
Although relatively little is known about early language skills in children who eventually develop ASD, there is some evidence that bears on this issue. Using the Mullen Scales of Early Learning, Landa and Garrett-Meyer (2006) have reported that at 6 months of age, Infant Siblings of children with autism who themselves later go on to develop ASD show no significant communicative delays. By contrast, however, Zwaigenbaum et al. (2005) found that at 12 months of age, Infant Siblings later diagnosed with ASD scored significantly lower on both the expressive and receptive language subscales of the Mullen; and in a study of Infant Siblings carried out by Yirmiya and colleagues (Yirmiya et al., 2006a; Yirmiya, Gamliel, Shaked, & Sigman, 2006b), 2 of 3 infants who scored 2 or 3 on the CHAT at 36 months had significant language delays.
Finally, difficulties with syllable production have been noted in a case study from birth to 2 years of an infant later diagnosed with autism. Dawson et al. (2000) reported that at 9 months, the infant’s vocal responses were “...primarily limited to guttural sounds with few, if any, recognizable consonant or labial sounds...” (p. 302). Although these data are taken from a single infant, the relative absence of these sounds is clearly deviant from patterns reported for typically developing infants in this age range, for whom labial sounds (e.g., [b], [m]) tend to be among the most frequently produced (e.g., Davis & MacNeilage, 1995).
This difficulty with production of well-formed syllables may be explained in part by problems with oral-motor control. The infant in Dawson et al.’s (2000) case study was reported to have significant oral-motor difficulties. In a retrospective survey of parents of 160 children with ASD and parents of 40 age- and gender-matched typically developing children, Gernsbacher et al. (2002) reported that children with ASD could be reliably distinguished from comparison children on the basis of reduced report of seven common early oral-motor behaviors (e.g., raspberries, sucking liquid through a straw, puffing cheeks with air, blowing bubbles).
Vocal-Motor Links in Children with ASD
Available evidence suggests that the vocal and motor difficulties apparent in children with ASD are closely correlated. Thus, for example, production of early oral- and manual-motor behaviors is related to language outcomes in early childhood, with nonverbal children reported to produce significantly fewer of both types of behaviors than children who eventually acquire fluent speech (Gernsbacher et al., 2002). In a longitudinal study of 35 children with ASD, Stone and Yoder (2001) found that after controlling for expressive language level at 2 years, motor imitation was a significant predictor of language abilities at age 4.
In light of these findings, the goal of this research is to examine the development of early motor skills, vocalization, and vocal-motor links in Infant Siblings in comparison to infants who are also later-born but have no family history of ASD. Specifically, we will present data on the achievement of infant motor and communicative milestones, postural variability, language development, and the relationship between motor rhythmicity and babble onset. This latter phenomenon is of particular interest as an index of the development of language-motor links in light of the strong, positive correlations found in typically developing children between age of babble onset and increased production of upper limb stereotypies (waving, swinging, banging; e.g., Cobo-Lewis, Oller, Lynch, & Levine, 1996) and of increased rates of rhythmic arm activity among infants who have just begun to babble (Iverson, Hall, Nickel, & Wozniak, in press).
Method
Participants
Participants were 21 infants (6 male, 15 female) from families in which an older child had been diagnosed with autism. Families were recruited through the Autism Research Program at the University of Pittsburgh, parent support organizations, and local agencies and schools serving families of children with ASD. Prior to enrollment, all older siblings were seen at the Autism Research Program for administration of the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000) by a trained clinician. For an infant to qualify for the study, the infant’s older sibling had to score above the threshold for Autism on the ADOS.
For purposes of comparison, a sample of 18 infants (8 males, 10 females) with no family history of ASD (i.e., no first- or second-degree relatives diagnosed with ASD) was selected from a larger group participating in an ongoing longitudinal study of vocal-motor coordination in infancy being conducted by the first author. This No-risk (NR) comparison group was chosen so as to include only later-born infants from the larger sample. All participants in both samples were from full-term, uncomplicated pregnancies and came from monolingual, English-speaking households. Thirty-six infants (19 Infant Siblings, 17 NR) were of Caucasian descent, two (both Infant Siblings) were Hispanic, and one NR infant was Asian-American. Mothers and fathers of infants in both groups had attained comparable levels of education, with a majority of parents either holding college degrees or having completed some college. Mean maternal (M Sib = 35.0, SD = 4.75; M NR = 33.0, SD = 5.12) and paternal (M Sib = 36.33, SD = 3.63; M NR = 34.33, SD = 4.10) ages did not differ significantly between the two groups.
Procedure
Infants and primary caregivers were videotaped at home for approximately 45 min each month. For the Infant Siblings, data collection began when the infant was 5 months old and continued at monthly intervals to the age of 14 months, with an 18-month follow-up visit. Comparison data were obtained from the NR sample from comparable monthly visits. Observations occurred within three days of the monthly anniversary of the infant’s birth and at times when caregivers thought the infant would be most alert and playful. Sessions were divided into three segments lasting approximately 15 min each. The first and final segments consisted of naturalistic observation. Caregivers were instructed to continue their normal activities and infants were observed in contexts and activities typical of the time of day at which the visit took place. The second segment consisted of semistructured play with the primary caregiver and included play with rattles (5 min), play in a Johnny Jump-Up (5 min), face-to-face interaction (3 min), and play with toys (5 min). As infants outgrew rattles, Johnny Jump-Up, and face-to-face interaction, the toy play segment was expanded to include time previously allocated to these activities. Over the course of the session, infants were naturally observed in a variety of self-adopted postures, including independent sitting, reclining, standing, prone, supine, and on hands and knees.
Measures
MacArthur–Bates Communicative Development Inventory
At each visit beginning at 8 months, caregivers completed the MacArthur–Bates Communicative Development Inventory (CDI; Fenson et al., 1993) as a measure of early communicative and language development. In this paper, we focus on the 18-month data.
At the 18-month observation, caregivers completed either the Words and Gestures or the Words and Sentences form, depending on the child’s general language level. If the child was producing relatively few words (as indicated by the primary caregiver and observed by the experimenter) and had no two-word combinations, the Words and Gestures form was administered. This form of the CDI is organized into two parts. Part I consists of a 396-item vocabulary checklist organized into 19 semantic categories. Parents are asked to check: (a) items that their child only understands; and (b) those that s/he both says and understands. Part II of the Infant form focuses on early gestures (e.g., giving, showing, pointing) and actions (e.g., games and routines, pretend play), and parents are requested to indicate those performed by their child. If the child had a significant productive vocabulary and combinations, the Words and Sentences form was administered. This form consists of two parts: a 680-word vocabulary checklist organized into 22 semantic categories (parents indicate words that their child says) and a section on children’s use of English morphology and syntax.
For children for whom the Words and Gestures form was collected, numbers of words understood and words understood and produced were totaled separately; only data on word production are collected on the Words and Sentences form. Scores for all children were then compared to the appropriate norms (Fenson et al., 1993); scores falling at or below the 5th percentile were deemed to represent a clinically significant language delay (e.g., Dale et al., 1998).
Pervasive Developmental Disorder Screening Test-II
At the 18-month visit, caregivers of Infant Siblings completed the Pervasive Developmental Disorders Screening Test-II (PDDST-II; Siegel, 2001). The PDDST-II is a 23-item parent report measure tapping behaviors presumed to be sensitive to possible ASD (e.g., language and communication delay, perceptual fixations, repetitive behaviors). It has high sensitivity (87% of children with autism were correctly identified) and moderate specificity.
Coding
All infant rhythmic limb movements, occurrences of milestone behaviors, and posture bouts were coded from the videotapes by coders blind to group membership. Because infants were enrolled in the study over a 2-year period and rhythmic movement and posture coding is ongoing, data from different numbers of infants are available for the various analyses to be presented below. Respective n’s will be indicated as analyses are reported.
Rhythmic Limb Movements
Rhythmic limb movements were defined as movements repeated in the same form at least three times at regular, short intervals of approximately a second or less (Thelen, 1979). Each movement bout was identified and the presence of co-occurring vocalizations noted. Rhythmic movements were further classified on the basis of involved body segment(s) (e.g., both legs, right arm, head, torso) and form (see Iverson & Fagan, 2004, for details).
Milestone Onsets
Upon enrollment, primary caregivers were given a baby journal and a list of early developmental milestones to track. At each visit, the experimenter reviewed the journal with the caregiver, focusing specifically on new behaviors that had appeared since the last visit. For motor milestones (independent sitting, walking), achievement of a given milestone was credited when the caregiver reported the onset of a new behavior and occurrence of the behavior was verified by the experimenter during a given session. To identify babbling onset and first word onset, caregivers were given a small tape recorder and asked to make brief audiorecordings of their infants’ vocalizations on the day prior to each visit. Babble onset was credited at the visit during which the parent reported relatively regular production of reduplicated syllables (e.g., [babababa]) and at least two instances of such vocalizations were produced either during the observation or on the audiotape made prior to the visit. Achievement of first word onset was indicated at the visit at which the caregiver reported use of a specific word form either in different contexts or to refer to different exemplars of the referent and the word was produced by the child spontaneously during the session or on the audiotape made before the observation. Note that mama and dada were excluded from consideration as first words due to their similarity to sound patterns common in the vocalizations of young infants. Onset of showing and pointing was credited when caregivers indicated production of the gestures on the CDI.
Posture Bouts
Posture bouts were coded when infants remained in a given posture for more than 1 s; they were further classified according to posture type (e.g., prone, hands and knees, stand unsupported). For analyses presented here, only data on frequency of postural change (i.e., shift from one posture to another) will be reported.
Reliability
Intercoder reliability was assessed by having all coders independently code all behaviors described above for 18 ten-minute segments randomly chosen from observations of different Infant Siblings and NR infants. Using this procedure, mean intercoder agreement was .91 for occurrence of a rhythmic movement; 1.00 for milestone onset; .91 for rhythmic movement types; and .80 for postures. Following calculation of intercoder reliabilities, disagreements were resolved through discussion.
Results
This study was designed to examine the onset of early developmental milestones, the production of rhythmic limb movements, and postural variability in Infant Siblings and to compare these data to those obtained from NR infants. In addition, for Infant Siblings, parent report data on early language development (CDI) and ASD symptomatology at 18 months (PDDST-II) were examined. Here we focus on four aspects of the data: (a) onset of six major early developmental milestones: independent sitting, reduplicated babbling, showing, pointing, walking, and first words; (b) postural variability; (c) production of rhythmic limb movements and changes in rhythmicity in relation to babble onset; and (d) 18-month language outcomes and ASD symptoms for the Infant Siblings group only.
Milestone Onset
Data from 18 NR infants and 15–21 Infant Siblings (depending on the milestone; see Table 1) were examined with regard to age of onset of six early developmental milestones: independent sitting, reduplicated babbling, showing, pointing, first word, and walking. To determine whether Infant Siblings were delayed in milestone onset relative to NR infants, we first compared the mean ages at which infants in each group attained a given milestone. These data are presented in Table 1. Although none of these comparisons was statistically significant, the average onset ages for independent sitting, reduplicated babble, showing, walking, and first words were later for Infant Siblings than for NR infants. Onset of pointing occurred at comparable ages for the two groups.
Because inspection of the distributions for milestone onsets indicated significant skewing and substantial individual variability at the high end, especially among Infant Siblings (some of whom had not attained various milestones even by 18 months of age), we decided to evaluate differences in milestone attainment by comparing distributional patterns between groups. To do so, chi-square tests were computed separately for each of the six milestones on the distributions of Infant Siblings whose onset age fell at or below (earlier or on time) vs. above (later) the median for the NR group (and vice versa). These data are also presented in Table 1.
As is evident, the Infant Sibling group contained a higher proportion of infants who were delayed relative to the NR group in the onset of all six milestones. These differences were statistically significant in the case of independent sitting, χ2 (1, N = 39) = 2.786, P = .047, reduplicated babble, χ2 (1, N = 38) = 8.108, P = .002, showing, χ 2 (1, N = 38) = 2.880, P = .045, and first words, χ 2 (1, N = 33) = 3.696, P = .027. Comparisons for pointing and walking were not statistically significant. For purposes of later discussion, individual milestone delays are summarized in the left side of Table 2.
Postural Variability
In light of previous reports of greater postural instability in infants later diagnosed with ASD (e.g., Kroeker, 2000), we examined the mean duration (in seconds) of posture bouts (calculated by dividing the length of the session by the number of postures observed in the session) observed within a session. This was done separately for each infant for a given session. This measure takes into account the frequency with which postural changes occur and thus provides a rough index of postural stability. Data presented here are from 10 Infant Siblings and 12 NR infants at the sessions 1 month before babble onset, at babble onset, and 1 month after babble onset. This analysis revealed that on average Infant Siblings’ posture bouts were significantly shorter (i.e., posture was less stable) than those of NR infants, t(20) = −2.718, P = .013 (M Sib = 44.90, SD = 25.93, range 20.88–100.5; M NR = 114.74, SD = 77.567, range 22.06–249.08).
Rhythmic Limb Movements and Babble Onset
Previous longitudinal observation of typically developing infants has indicated that rate of rhythmic arm movement begins to increase about two months before babble onset and continues to rise through babble onset, when it peaks and eventually declines slightly (Iverson, 2005). In contrast, rate of all other limb rhythmicities (legs, torso, head, fingers) remains low and relatively unchanged throughout this period. Thus, in typically developing infants, change in limb rhythmicity around the time of babble onset appears to be specific to the arms.
In order to examine the relationship between babble onset and production of rhythmic arm movements in Infant Siblings, we focus here on data from the babble onset session and the sessions one month prior to (Pre-Babble) and one month after babble onset (Post-Babble). Data for these three sessions were available for 10 Infant Siblings and 12 NR infants. Change in limb rhythmicity surrounding babble onset was examined both in terms of change in the overall rate of rhythmic arm movements and in terms of the specificity of change using the proportions of limb movements produced by each body segment.
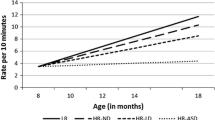
Group data on change in rate of rhythmic arm movements for Infant Siblings and NR infants are presented in Fig. 1. As is evident, for both groups of infants, rate of rhythmic arm movement increased from the Pre-Babble to the Babble Onset session and dropped following Babble Onset. This overall Session effect was significant, F(2,38) = 5.122, P = .011, η 2 = .212. As is also apparent, however, the relative difference in rate of rhythmic arm movement between the Babble Onset and Pre- and Post-Babble sessions was lower for Infant Siblings than for NR infants. This difference approached but did not quite reach significance (P = .056, Fishers Exact Test).

Change in rate of rhythmic arm activity (a) and proportions of arm and finger rhythmicities (b) in relation to reduplicated babble onset in Infant Siblings and NR infants
In light of the prior finding that for NR infants, change in rhythmic limb movement production at babble onset is specific to the arms (Iverson, 2005), specificity of change in rhythmic limb movement at babble onset was examined by computing the proportions of rhythmic movements produced by each body segment. These proportions were calculated separately for each infant for the Pre-Babble and Babble Onset sessions and averaged across infants in each group. These data are presented in the lower panel of Fig. 1.
A 2 X 2 X 2 repeated measures ANOVA with Limb (arms, fingers) and Session (Pre-Babble, Babble Onset) as the within-subjects factors and Group (Infant Sibling, NR) as the between-subjects factor revealed a highly significant main effect of Limb, F(1,20) = 72.283, P = .000, η 2 = .783; but this was qualified by a significant Limb X Session X Group interaction, F(1,20) = 6.213, P = .022, η 2 = .237. Simple effects analyses carried out to assess the source of the interaction indicated that for NR infants, there was a significant increase in the proportion of rhythmic arm movements from the Pre-Babble to the Babble Onset session (M Pre = .61, SD = .32; M Babble = .83, SD = .15, P = .007, η 2 = .313) and that, while production of finger rhythmicities decreased across the two sessions (M Pre = .15, SD = .27; M Babble = .05, SD = .11), the difference only tended toward significance (P = .138). By contrast, for Infant Siblings, the proportionate production of rhythmic arm movements was relatively unchanged across the Pre-Babble and Babble Onset sessions (M Pre = .58, SD = .23; M Babble = .53, SD = .33, P = .568), and while the proportion of finger rhythmicities actually increased (M Pre = .02, SD = .03; M Babble = .12, SD = .17), it did not do so significantly (P = .337).
Language Development and ASD Symptomatology in 18 Month-old Infant Siblings
Language data from the 14 Infant Siblings who have reached the age of 18 months are presented in the right side of Table 2. Parents of six Infant Siblings completed the Words and Sentences form of the CDI, and thus for these infants, data are only available for vocabulary production. Parents of eight Infant Siblings completed the Words and Gestures form, and for them, data on vocabulary comprehension and production are presented in the table. Note that the fact that the Words and Gestures form had to be used with parents of 18 month-olds is in itself suggestive of delay, as it is normed for use with children up to 16 months of age. Scores for these children were thus compared to the norms for 16-month-old children. Scores falling at or below the 5th percentile are considered to be indicative of a clinically significant delay.
As is apparent, of the 8 children for whom both comprehension and production data are available, 1 was delayed in vocabulary comprehension but not in production, 1 was delayed in comprehension but only mildly delayed in production, 2 were significantly delayed in production but only mildly delayed in comprehension, and 4 were experiencing clinically significant delays in both vocabulary comprehension and production. Of the six children whose parents completed the Words and Sentences form, one scored in the clinically delayed range for vocabulary production, and an additional two children gave evidence of milder delays, scoring below the 50th percentile for their age. Thus, a total of 9 of the 14 Infant Siblings had a clinically significant delay in either vocabulary comprehension or production at 18 months of age.
With regard to the PDDST-II, two children (both males) scored above the cutoff for possible ASD at 18 months and have subsequently received an independent diagnosis of PDD from a developmental pediatrician. In terms of the findings described above, one of these children never produced reduplicated babble, and thus data on the relationship between rhythmic arm movement and babble onset were not available. The other child demonstrated a pattern of change in frequency of rhythmic arm movement similar to that of the NR group (see Fig. 1) but was significantly delayed in babble onset (10 months) and also showed an increase in the proportionate production of finger (but not arm) rhythmicities at babble onset. In addition, both children were significantly delayed relative to both NR infants and other Infant Siblings in the onset of walking (15 and 16 months), pointing (14 and 13 months), and first words (18 months), and they were also among those with clinically significant language delays at 18 months (one in both comprehension and production, the other in production only). The relevance of this pattern of delay in both language and motor domains to both language delay and ASD will be discussed below.
Discussion
Group Patterns of Delay
Relative to the general population, those infants with an older sibling already diagnosed with autism are known to be at more than 200 times the risk for an eventual ASD diagnosis themselves (Ritvo et al., 1989; see Zwaigenbaum et al., 2005, for more recent figures). The data presented here suggest that even in the absence of obvious ASD symptomatology, these infants are also at risk for a number of other developmental delays and atypicalities. Specifically, relative to No Risk infants, Infant Siblings are more likely to be delayed in the onset of early developmental milestones, to be characterized by postural change and instability, to exhibit delays in both language production and comprehension at 18 months, and to demonstrate attenuated and varied patterns of change in rhythmic activity around the time of reduplicated babble onset.
Motor and Posture Development
To our knowledge, this is the first study to track the onset of major early motor milestones longitudinally and prospectively in Infant Siblings. The pattern reported here suggests that delays in motor development may be characteristic of Infant Siblings as a group. To the extent that such delays reflect relative instability in the motor system, they could have far-reaching consequences for the emergence of skills in other developmental domains. Although this topic is as yet not well-researched for motor milestones other than crawling, we do know, for example, that the onset of crawling is related to a wide variety of skills in domains such as responsiveness to referential gestures, spatial coding and search strategies, social referencing, and wariness of heights (Campos et al., 2000). It seems likely that relationships of this sort are also characteristic of other motor onsets. Furthermore, when motor development is delayed, opportunities to engage with and learn about the environment and social partners in new and different ways may be limited or hampered (see Thelen, 2004, for discussion).
A further indication that motor system instability may be characteristic of Infant Siblings as a group comes from our data on postural instability. Previous retrospective home video studies have reported that relative to comparison infants, infants later diagnosed with ASD spend more time in a larger number of postures (e.g., Kroeker, 2000), adopt atypical postures (e.g., Baranek, 1999), and exhibit difficulties with movement organization (e.g., Teitelbaum et al., 1998). Our data are consistent with these previous reports.
Communicative Milestones and Language Development
The group data presented here also reveal delays among Infant Siblings in the onset of certain early communicative milestones (reduplicated babble, showing, first words) and in the development of receptive and expressive language. With regard to early communicative milestones, it is well-documented that young children with ASD are likely to be delayed in the use of gestures such as showing, which involve a shared reference component (e.g., Charman et al., 1997), and in onset of first words (e.g., De Giacomo & Fombonne, 1998). In addition, there are data indicating that at least some infants later diagnosed with ASD produce very limited or no babble with clear syllabic organization (Dawson et al., 2000; Gernsbacher, 2004).
Finally, delayed language development at 18 months was also characteristic of Infant Siblings as a group. This result is not surprising in light of the prevalence of delayed reduplicated babble in the group and the fact that delayed babble has been shown to relate to delayed language (e.g., Oller, Eilers, Neal, & Schwartz, 1999; Stoel-Gammon, 1989). It is also very much in line with other recent studies of Infant Siblings in the second and third years that have reported delays in language using both standardized and parent report measures (Mitchell et al., 2006; Yirmiya et al., 2006a; Yirmiya et al., 2006b; Zwaigenbaum et al., 2005). Whether the Infant Siblings as a group will continue to be characterized by delay at later ages is an open question (and there is some indication that they will not; Pilowsky, Yirmiya, Shalev, & Gross-Tsur, 2003; but see Bailey, Palferman, Leavey, & Le Couteur, 1998). Rather, it is likely that there will be some children who will ‘catch up’ to their peers at later ages and some who will show persistent delays. The extent to which these delays are transient vs. persistent and their relationship to developmental outcome measures at 36 months is an issue that we will address in our continuing work.
Rhythmic Arm Movement at Babble Onset
Of the milestones considered here, reduplicated babble was the one for which delay was most pronounced (greater than 1 month) for Infant Siblings relative to NR infants, and the one for which the greatest proportion of Siblings were delayed in relation to the NR average. In addition, as a group, Infant Siblings demonstrated a less pronounced pattern of change in rate of rhythmic arm movement at babble onset and change in rhythmicity was not specific to the arms. Rather, for Infant Siblings (but not NR infants), the proportion of rhythmicities involving the arms was generally unchanged from the pre-babble to the babble onset session. Although an observed increase in proportion of finger rhythmicities for Infant Siblings was not significant, the direction of the effect is intriguing in light of prior retrospective home video studies in which infants later diagnosed with ASD produced higher rates of finger rhythmicities than did typically developing infants (Kroeker, 2000).
Why was change in rhythmic arm activity at babble onset attenuated among Infant Siblings? One possible explanation is suggested by Iverson and Thelen’s (1999) model of the development of vocal-motor coordination. There is a substantial body of work supporting the existence of couplings between the manual and oral/vocal systems from very early in development (see Iverson & Thelen, 1999, for a review). When systems of this type are coupled, they are typically termed ‘coupled oscillators;’ and it is a well-established characteristic of coupled oscillators that each tries to draw the other into its characteristic oscillation pattern. This suggests the possibility that entrainment, which occurs when the activation of one oscillator is sufficient to “pull in” the activity of the other to yield an ordered patterning of coordinated activity, may characterize the development of vocal-motor coordination (see Iverson & Fagan, 2004, for discussion and relevant data; see also Ejiri & Masataka, 2001).
Iverson and Thelen (1999) characterize the emergence of reduplicated babble as a product of the entrainment of the vocal by the motor system. Thus, in typically developing infants prior to the onset of reduplicated babbling, rhythmic arm movements are frequently occurring, stable, and well-practiced behaviors. Since these are prime conditions for entrainment, production of repetitive, rhythmically organized arm movements gradually entrains vocal activity, leading eventually to the emergence of the rhythmically organized CV sequences that comprise babbling. One would therefore expect the appearance of reduplicated babble to be accompanied by an increase in frequency of arm rhythmicity; and indeed, this is precisely what is observed in typically developing infants (e.g., Ejiri, 1998; Iverson, 2005; Thelen, 1979).
Delays in the attainment of certain motor milestones, increased postural instability, and delay in babble onset, as reported here for Infant Siblings, may be suggestive of poor internal organization and instability within the motor and vocal systems. When a system is unstable, more energy is required to maintain a particular behavioral state (Haken, 1996; Nicolas & Prigogine, 1989). The implication for entrainment is clear: once a behavior has emerged, there may be little or no remaining energy, energy that is required to capture and entrain another system. Thus, patterns of vocal-manual entrainment in Infant Siblings might be expected to vary systematically from those of NR infants. With respect to babbling emergence, more time would be required for the motor to entrain the vocal system and result in a delay in the onset of babbling. In addition, although there are no currently available data on this topic, it seems possible that babble, when it does emerge, would more likely be poorly organized and infrequent. This would in turn reduce the opportunity for mutual entrainment of the manual system by the vocal system and might therefore be expected to be accompanied by reduced rates of manual rhythmicity and less specificity with regard to the arms.
One final issue with regard to all of the group differences just discussed has to do with the degree to which these delays and atypicalities are characteristic of infants who will eventually be diagnosed with ASD or of at-risk infants more generally. Since delays in motor milestone onset are evident in children at-risk for developmental delays (e.g., gestational age less than 32 weeks, term asphyxia; Piper & Darrah, 1994) and delays in the onset of reduplicated babble and in language abilities in the second year are also present in children at risk for later non-ASD language and communication disorders (e.g., Oller et al., 1999; Stoel-Gammon, 1989), the question of specificity is an important one, and it is one to which we return below.
Individual Variations in Patterns of Delay
As or perhaps even more striking than the group differences just discussed is the fact that within the Infant Sibling group, on a child-by-child basis, the particular patterns of clinically significant delay are hugely variable. There are infants who manifest no such delays. There are infants whose only clinically significant delays are in skills directly related to language and communication. There is one infant whose delays are restricted to motor milestones; and there are five infants with clinically significant delays in both motor and language areas, although even here the delays are not across the board.
Because the current sample size is still quite restricted and because data are at present available on the Infant Siblings in this sample only through the age of 18 months, it is as yet impossible to assess the long-term predictive implications of the observed variations in these patterns of delay with confidence. Even if the task is merely to predict language delay at 18 months based on delays in achievement of early milestones, the data on Infant Siblings and No Risk infants presented here make it apparent that no single milestone onset delay will serve as a completely reliable indicator of later language delay. Somewhat surprisingly, this is even true for delayed babble onset in that, although it has reasonable positive predictive value (3 of 4 infants with delayed babble onset had later clinically significant levels of language delay) and specificity (4 of 5 infants without language delay also showed no babble onset delay), it is not especially sensitive. Of the 9 infants with some type of language delay at 18 months, only 3 were delayed in babble onset.
An alternative possibility might involve not single milestone delays as predictors but rather broad patterns of delay, in particular patterns that involve both motor and language/communication milestones. Here again, because of sample size and age limitations, the data presented are at best suggestive. While for the prediction of later language delay, use of multiple indicators of this sort provides only a slight increase over delay in babble onset in positive predictive value and sensitivity and none in specificity, this approach may prove more useful with regard to predicting ASD symptoms. Here sensitivity is perfect (i.e., both children exhibiting this pattern received a positive PDDST-II screen at 18 months) and specificity reasonably high (the pattern was absent in 9 of 12 children without a positive screen), although positive predictive value was only marginal (of 5 children with this pattern, only 2 received a positive screen).
Clinical Implications
Taken together, we believe that the results reported here, though preliminary in nature, have possible implications for developmental screening and may be relevant to the early identification of ASD. The first is that it may be useful to pay careful attention to early motor milestone attainment for Infant Siblings and for at-risk infants in general, particularly during the first year, when variation in social-communicative behaviors of the sort often taken to be indicative of an ASD diagnosis has yet to emerge. While delays in the achievement of major early motor milestones may not be specific to ASD, they are nevertheless indicative of general risk status, and given the importance of skilled movement for perception, action, and cognition (e.g., see Thelen, 2004), identifying such delays and providing appropriate intervention at an early age is critical.
Second, the fact that Infant Siblings are at risk not only for ASD but also for language delay and other mild developmental disorders (Yirmiya et al., 2006a) highlights the potential importance of tracking the emergence and production of reduplicated babble in Infant Siblings. While this may sound like a task for the specialist, Oller and colleagues (Oller, Eilers, Neal, & Cobo-Lewis, 1998; Oller et al., 1999) have demonstrated that if interviewed appropriately, caregivers can be remarkably accurate reporters of babble onset and production by their infants. This may be a useful procedure to incorporate into surveillance visits for very young Infant Siblings, as the absence of babble by 10 months is considered to be a moderately sensitive index of risk for later language delay and developmental disorder (Oller et al., 1998, 1999; Stoel-Gammon, 1989).
Finally, it remains to be seen whether and to what extent there will be a ‘profile’ of motor and language delays and deficits that is characteristic of infants later diagnosed with ASD. Given the relative costs and consequences of under- versus over-identification and the fact that infants with this pattern are already delayed in critical developmental domains, however, it is clear that there is a need for longitudinal, prospective observation of motor and vocal behaviors during the first year. The fact that these behaviors are frequently occurring and easily recognized by observers and that motor and vocal disorders are pervasive among children with ASD makes them ideal candidates for inclusion in any screening tool developed for the early identification of ASD.
References
Adrien, J. L., Faure, M., Perrot, A. Hameury, L., Garreau, B., Barthelemy, C., & Sauvage, D. (1991). Autism and family home movies: Preliminary findings. Journal of Autism and Developmental Disorders, 21, 43–49.
Adrien, J. L., Perrot, A., Sauvage, D., Leddet, I., Larmande, C., Hameury, L., & Barthelemy, C. (1992). Early symptoms in autism from family home movies. Acta Psychopaediatrica, 55, 71–75.
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, D.C.: American Psychiatric Association.
Bailey, A., Palferman, S., Leavey, L., & Le Couteur, A. (1998). Autism: The phenotype in relatives. Journal of Autism and Developmental Disorders, 28, 369–392.
Baranek, G. (1999). Autism during infancy: A retrospective video analysis of sensory-motor and social behaviors at 9–12 months of age. Journal of Autism and Developmental Disorders, 29, 213–224.
Campos, J. L., Anderson, D. I., Barbu-Roth, M. A., Hubbard, E. M., Hertenstein, M. J., & Witherington, D. (2000). Travel broadens the mind. Infancy, 1, 149–219.
Charman, T., Baron-Cohen, S., Swettenham, J., Cox, A., Baird, G., & Drew, A. (1997). Infants with autism: An investigation of empathy, pretend play, joint attention, and imitation. Developmental Psychology, 33, 781–789.
Cobo-Lewis, A. B., Oller, D. K., Lynch, M. P., & Levine, S. L. (1996). Relations of motor and vocal milestones in typically developing infants and infants with Down syndrome. American Journal on Mental Retardation, 100, 456–467.
Coonrod, E. E., & Stone, W. L. (2004). Early concerns of parents of children with autistic and nonautistic disorders. Infants and Young Children, 17, 258–268. .
Dale, P. S., Simonoff, E., Bishop, D. V. M., Eley, T. C., Oliver, B., Price, T. S., Purcell, S., Stevenson, J., & Plomin, R. (1998). Genetic influences on language delay in two-year-olds. Nature Neuroscience, 1, 324–328.
Damasio, A. R., & Maurer, R. G. (1978). A neurological model for childhood autism. Archives of Neurology, 38, 646–649.
Davis, B. L., & MacNeilage, P. J. (1995). The articulatory basis of babbling. Journal of Speech and Hearing Research, 38, 1199–1211.
Dawson, G., Osterling, J., Meltzoff, A. N., & Kuhl, P. (2000). Case study of the development of an infant with autism from birth to two years of age. Journal of Applied Developmental Psychology, 21, 299–313.
De Giacomo, A., & Fombonne, E. (1998). Parental recognition of developmental abnormalities in autism. European Journal of Child and Adolescent Psychiatry, 7, 131–136.
Ejiri, K. (1998). Relationship between rhythmic behavior and canonical babbling in infant vocal development. Phonetica, 5, 226–237.
Ejiri, K., & Masataka, N. (2001). Co-occurrence of preverbal vocal behavior and motor action in early infancy. Developmental Science, 4, 40–48.
Fenson, L., Dale, P., Reznick, S. J., Thal, D. J., Bates, E., Hartung, J. P., Pethick, S., & Reilly, J. S. (1993). The MacArthur Communicative Development Inventories: User’s guide and technical manual. San Diego: Singular Press.
Folstein, S., & Rosen-Sheidley, B. (2001). Genetics of autism: Complex aetiology for a heterogeneous disorder. Nature Reviews: Genetics, 2, 943–955.
Gernsbacher, M. A. (2004). Language is more than speech: A case study. Journal of Developmental and Learning Disorders, 8, 81–98.
Gernsbacher, M. A., Goldsmith, H. H., O’Reilly, M., Sauer, E., DeRuyter, J., & Blanc, M. (2002). Infant motor dyspraxia as a predictor of speech in childhood autism. Toronto, Ontario, Canada: Poster presented at the International Conference on Infant Studies.
Haken, H. (1996). Principles of brain functioning: A synergetic approach to brain activity, behavior, and cognition. New York: Spriger-Verlag.
Hauck, J. A., & Dewey, D. (2001). Hand preference and motor functioning in children with autism. Journal of Autism and Developmental Disorders, 31, 265–277.
Iverson, J. M. (2005). Increased manual rhythmicity precedes babble onset. Atlanta, GA: Poster presented at the Biennial Meetings of the Society for Research in Child Development.
Iverson, J. M., & Fagan, M. K. (2004). Infant vocal-motor coordination: Precursor to the gesture-speech system?. Child Development, 75, 1053–1066.
Iverson, J. M., Hall, A. J., Nickel, L., & Wozniak, R. H. (2006). The relationship between reduplicated babble onset and laterality in infant rhythmic arm movement, in press.
Iverson, J. M., & Thelen, E. (1999). Hand, mouth, and brain: The dynamic emergence of speech and gesture. Journal of Consciousness Studies, 6, 19–40.
Johnson, M. H., Siddons, F., Frith, U., & Morton, J. (1992). Can autism be predicted on the basis of infant screening tests? Developmental Medicine and Child Neurology, 34, 316–320.
Jones, V., & Prior, M. (1985). Motor imitation abilities and neurological signs in autistic children. Journal of Autism and Developmental Disorders, 15, 37–46.
Kroeker, R. (2000). Rhythmic behaviors in typically developing infants, and infants with later diagnosed autism or developmental delay. Unpublished doctoral dissertation, Department of Psychology, University of Washington.
Landa, R., & Garrett-Meyer, E. (2006). Development in infants with autism spectrum disorder: A prospective study. Journal of Child Psychology and Psychiatry, 47, 627–638.
Leary, M. R. & Hill, D. A. (1996). Moving on: Autism and movement disturbances. Mental Retardation, 34, 39–53.
Lord, C., & Paul, R. (1997). Language and communication in autism. In D. Cohen & F. Volkmar (Eds.), Handbook of autism and pervasive developmental disorders (2nd ed.). New York: John Wiley & Sons.
Lord, C., Risi, S., Lambrecht, L., Cook Jr. E. H., Leventhal, B. L., DiLavore, P. C., Pickles, A., & Rutter, M. (2000). The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223.
Manjiviona, J., & Prior, M. (1995). Comparison of Asperger syndrome and high-functioning autistic children on a test of motor impairment. Journal of Autism and Developmental Disorders, 25, 23–39.
Minshew, N. J., Sung, K., Jones, B., & Furman, K. (2004). Underdevelopment of the postural control system in autism. Neurology, 63, 2056–2061.
Mitchell, S., Brian, J., Zwaigenbaum, L., Roberts, W., Szatmari, P., Smith, I., & Bryson, S. (2006). Early language and communication development in infants later diagnosed with Autism Spectrum Disorder. Developmental and Behavioral Pediatrics, 27, S69–S78.
Nicolas, G., & Prigogine, I. (1989). Exploring complexity: An introduction. Munich: Verlag Press.
Oller, D. K., Eilers, R. E., Neal, A. R., & Cobo-Lewis, A. B. (1998). Late onset canonical babbling: A possible early marker of abnormal development. American Journal on Mental Retardation, 103, 249–263.
Oller, D. K., Eilers, R. E., Neal, A. R., & Schwartz, H. K. (1999). Precursors to speech in infancy: The prediction of speech and language disorders. Journal of Communication Disorders, 32, 223–245.
Pilowsky, T., Yirmiya, N., Shalev, R. S., & Gross-Tsur, V. (2003). Language abilities of siblings of children with autism. Journal of Child Psychology and Psychiatry, 44, 914–925.
Piper, M. C., & Darrah, J. (1994). Motor assessment of the developing infant. Philadelphia: W.B. Saunders Company.
Ritvo, E. R., Jorde, L. B., Mason-Brothers, A., Freeman, B. J., Pingree, C., Jones, M. B., McMahon, W. M., & Petersen, P. B. (1989). The UCLA-University of Utah epidemiologic survey of autism: Recurrence risk estimates and genetic counseling. American Journal of Psychiatry, 146, 1032–1036.
Rogers, S. J. (2001). Diagnosis of autism before the age of 3. In L. G. Masters (Ed.), International review of research in mental retardation (vol. 23, pp. 1–31). New York: Academic Press.
Siegel, B. (2001). Pervasive Developmental Disorder Screening Test-II. San Antonio, TX: Harcourt Assessment.
Spence, M. A. (2001). The genetics of autism. Current Opinion in Pediatrics, 13, 561–565.
Stoel-Gammon, C. (1989). Prespeech and early language development of two late talkers. First Language, 9, 207–224.
Stone, W. L., Hoffman, E. L., Lewis, S. E., & Ousley, O. Y. (1994). Early recognition of autism. Archives of Pediatric and Adolescent Medicine, 148, 174–179.
Stone, W. L., & Yoder, P. J. (2001). Predicting spoken language level in children with autism spectrum disorders. Autism, 5, 341–361.
Szatmari, P., Jones, M. B., Zwaigenbaum, L., & MacLean, J. E. (1998). Genetics of autism: Overview and new directions. Journal of Autism and Developmental Disorders, 28, 351–368.
Tager-Flusberg, H., Paul, R., & Lord, C. (2005). Language and communication in autism. In F. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (3rd Edition). New York: John Wiley & Sons.
Teitelbaum, P., Teitelbaum, O., Nye, J., Fryman, J., & Maurer, R. G. (1998). Movement analysis in infancy may be useful for early diagnosis of autism. Proceedings of the National Academy of Science, 95, 13982–13987.
Thelen, E. (1979). Rhythmical stereotypies in normal human infants. Animal Behaviour, 27, 699–715.
Thelen, E. (2004). The central role of action in typical and atypical development: A dynamic systems perspective. In I. J. Stockman (Ed.), Movement and action in learning and development: Clinical implications for Pervasive Developmental Disorders (pp. 49–73). San Diego: Elsevier Academic Press.
Vernazza-Martin, S., Martin, N., Vernazza, A., Lepellec-Muller, A. Rufo, M., Massion, J., & Assaiante, C. (2005). Goal directed locomotion and balance control in autistic children. Journal of Autism and Developmental Disorders, 35, 91–102.
Vilensky, J. A., Damasio, A. R., & Maurer, R. G. (1981). Gait disturbances in patients with autistic behavior: a preliminary study. Archives of Neurology, 38, 646–649.
Wing, L. (1969). The handicaps of autistic children—A comparative study. Journal of Child Psychology and Psychiatry, 10, 1–40.
Yirmiya, N., Gamliel, I., Pilowsky, T., Feldman, R., Baron-Cohen, S., & Sigman, M. (2006a). The development of siblings of children with autism at 4 and 14 months: Social engagement, communication, and cognition. Journal of Child Psychology and Psychiatry, 47, 511–523.
Yirmiya, N., Gamliel, I., Shaked, M., & Sigman, M. (2006b). Cognitive and verbal abilities in 24- and 36-month-old siblings of children with autism. Journal of Autism and Developmental Disorders.. doi: 10.1007/s10803-006-0163-5.
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari, P. (2005). Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience, 23, 143–152.
Zwaigenbaum, L., Thurm, A., Stone, W., Baranek, G., Bryson, S., Iverson, J. M., Kau, A., Klin, A., Landa, R., Lord, C., Rogers, S., & Sigman, M. (2006). Studying the emergence of Autism Spectrum Disorders in high-risk infants: Methodological and practical issues. Journal of Autism and Developmental Disorders. doi: 10.1007/s10803-006-0179-x.
Acknowledgments
This research was supported by a Language and Communication Pilot Study Grant from the National Alliance for Autism Research and by NIH R01 HD41607 to JMI. We thank Diane Williams, Nancy Minshew, P.J. McCarroll, and the NICHD-funded University of Pittsburgh–Carnegie Mellon Collaborative Program of Excellence in Autism Research (HD35469) for supporting assessments of older siblings and assistance with participant recruitment; Beth Whitehouse for assistance with participant recruitment; Kelly Aller, Carin Bremer, Erin Koterba, Tracy Nyerges, Meg Parladé, and Emily Reid for assistance with data collection; and members of the Infant Communication Lab for assistance with data collection, coding, and establishment of intercoder reliability. Special thanks are due to the families and infants who participated in the research. This work could not have been conducted without their dedicated and enthusiastic involvement.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iverson, J.M., Wozniak, R.H. Variation in Vocal-Motor Development in Infant Siblings of Children with Autism. J Autism Dev Disord 37, 158–170 (2007). https://doi.org/10.1007/s10803-006-0339-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-006-0339-z