
Abstract
Joint attention, a foundational nonverbal social-communicative milestone that fails to develop naturally in autism, was promoted for three toddlers with early-identified autism through a parent-mediated, developmentally grounded, researcher-guided intervention model. A multiple baseline design compared child performance across four phases of intervention: focusing on faces, turn-taking, responding to joint attention, and initiating joint attention. All toddlers improved performance and two showed repeated engagement in joint attention, supporting the effectiveness of developmentally appropriate methods that build on the parent–child relationship. A complementary qualitative analysis explored family challenges, parent resilience, and variables that may have influenced outcomes. Intervention models appropriate for toddlers with autism are needed as improved early identification efforts bring younger children into early intervention services.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The research reported here studied an approach to promoting joint attention in toddlers with autism that considers developmental foundations and builds on the existing parent–child relationship (Schertz, 2005a). Models appropriate for younger children with autism are a high priority for the field because with earlier and effective intervention, we can expect superior long-term outcomes (National Research Council, 2001; Volkmar, Lord, Bailey, Schultz, & Klin, 2004). As early identification efforts improve with effective toddler screening programs (e.g., Robins, Fein, Barton, & Green, 2001; Stone, Coonrod, & Ousley, 2000), this need becomes more urgent.
Joint attention is defined as visually coordinating attention with a partner to an external focus, showing social engagement and an awareness of the partner’s mutual interest for the purpose of “commenting” rather than “requesting” (Carpenter & Tomasello, 2000; Mundy & Stella, 2000; Schertz, 2005b). Like receptive and expressive verbal language, joint attention appears in both responding and initiating forms and is demonstrated by following another’s eye gaze or point, or by showing or pointing to objects (Kasari, Freeman, & Paparella, 2001). This important foundational competency crosses three domains of early development (Schertz & Odom, 2003) by supporting theory of mind or an awareness of others’ mental states (Baron-Cohen, 2000), language learning (Carpenter, Nagell, & Tomasello, 1998; Paparella & Kasari, 2004), and social development (Adamson & Russell, 1999). During the first year of life, precursors of joint attention are typically evident in a natural progression through face-to-face engagement in the first months, involvement with objects by mid-year and, by the last quarter of the year, response to joint attention overtures from caregivers (Adamson & Bakeman, 1991). Typically appearing in the first year as a passive response that relies heavily on caregiver support, joint attention is fully consolidated by about 18 months (Adamson & Russell, 1999).
Disruption in the development of joint attention is unique to autism, providing one of the earliest discernable markers of autism in toddlers. When compared to control groups with typical development, developmental delay, and language delay, groups with autism show difficulties with joint attention that cannot be explained by general cognitive or language differences (McArthur & Adamson, 1996; Mundy, Sigman, Ungerer, & Sherman, 1986). These findings suggest a need to study intervention models that directly target development of joint attention and to compare results with more traditional approaches that focus on symbolic communication.
In a study designed for the exclusive purpose of promoting joint attention in young children with autism, Whalen and Schreibman (2003) used naturalistic behavior modification to elicit joint attention in 4-year-olds with autism. Using physical and verbal prompts, interspersal of mastered tasks, task choice, and contingent reinforcement, their intervention resulted in moderate gains, but limited skill maintenance, which was attributed to the lack of planned parent involvement. Kasari et al. (2001) suggest that generalizability limitations may also result from a reinforcement-based, externally motivated approach to promoting what is a spontaneous, internally generated form of early communication.
Other intervention considerations surround issues of developmentally appropriate practice for toddlers (Bredekamp & Copple, 1997). In a consensus-building effort to guide practices for young children with autism, the National Research Council (2001) identified intensity of services as critical, although its importance is questioned by others (Bono, Daley, & Sigman, 2004; Prizant & Wetherby, 1998). Toddlers may be less adaptive than older children to intensive, highly structured, adult-directed, skill-based approaches and some have called for early intervention models that move beyond promoting isolated skills to considering family systems, child engagement, integrated and authentic intervention, and variable response to intervention (Bryson, Rogers, & Fombonne 2003; Howlin & Moore, 1997; Pretti-Frontczak & Bricker, 2004; Volkmar et al., 2004). Dawson and Osterling (1997) advocated a developmental approach for toddlers with autism, emphasizing early social skills and child initiation.
Relationship-based approaches (Greenspan & Wieder, 1999; Klein, 2003; Prizant, Wetherby, & Rydell, 2000) can address social-communication needs within a developmental framework. McCollum (1984) transmitted generalizable principles rather than specific skills to help parents adjust their interactive style to match infant characteristics. Cognitive-mediational approaches also use relationships to promote children’s internal learning capacity. Theories of “cognitive modifiability”, based on Vygotskian thought, emphasize transactional aspects of socially based learning to influence child motivation, self-efficacy, and desire for learning (Feuerstein, 1980; Haywood, Brooks, & Burns, 1992). Butera and Haywood (1992) advocated a cognitive model to help children with autism process the complexities of social communication.
Accommodation to a social world, an emerging challenge for toddlers, is supported by parent–child interaction in joint attention encounters. Typically, parent initiative is prominent in the early stages of joint attention development (Adamson & Bakeman, 1991) and the level of early caregiver scaffolding (i.e., support provided to enable success) relates to the infant’s later ability to initiate joint attention (Vaughan et al., 2003). Maternal responsivity was found to mediate communication development in young children with developmental delays and autism (Kaiser & Hemmeter, 1996; Mahoney & Perales, 2003; Yoder & Warren, 1999) and, if the interaction supports joint attention, parent-mediated intervention could extend through much of the child’s waking hours. Ingersoll and Dvortcsak (2006) promoted generalization and maintenance of professionally trained child skills in their group training program for parents of young children with autism. Klein (2001) placed parents in a more central role in a parent-mediated relationship-based intervention that supported early cognitive development. Compared to controls, the experimental group realized superior cognitive outcomes that were sustained in 3-year follow-up measures.
The purpose of the current study was to determine the effectiveness for toddlers with early-identified autism of a model that initiated intervention before age three, promoted joint attention by building on its developmental precursors, and used the parent–child relationship to mediate child learning. A secondary purpose was to study possible transactional influences among family factors, intervention-related variables, and intervention outcomes.
Method
Participants
The participants were three parents of toddlers with autism. Eligibility criteria were child age less than 36 months at entry and strong early markers of autism. The first three eligible families who agreed to commit to the intervention were accepted for participation. To recruit participants, pediatricians in two group practices agreed to administer the Modified Checklist for Autism in Toddlers (M-CHAT; Robins et al., 2001) at all 18- and 24-month well child checks, providing a researcher-generated letter to identified families that invited their participation in the study. Concurrently, Part C-funded early intervention providers in a multi-county area were requested to administer the M-CHAT for children they identified as having disproportionate delays in social and communication development. The researcher re-administered the M-CHAT to identified willing families by interview. Although it is a screening and not a diagnostic instrument, the M-CHAT has shown strong sensitivity (identifies 85–95% of true positives, depending on exclusion criteria) and specificity (correctly excludes 93% of children who will not be diagnosed) in field tests (Dumont-Mathieu & Fein, 2005). M-CHAT results for participants were replicated on the Pervasive Developmental Disorders Screening Test-II (PDD-ST-II; Siegel, 2001) and the researcher-developed Infant Social-Communication Questionnaire (ISCQ) (Schertz, unpublished). Diagnostic clinics in the region were reluctant to diagnose autism in children under age 3; however, the researcher administered the Childhood Autism Rating Scale (CARS; Schopler, Reichler, & Renner, 1988), resulting in scores for all children in the “severely autistic” range. Parent-initiated independent evaluations from research hospital clinics subsequently confirmed diagnoses of autism for all three children.
All parent participants were mothers and the three toddlers were boys. Child A’s mother was age 27 and a high school graduate with self-reported dyslexia and depression. Child A, age 24 months at enrollment was an only child. He received Part C-funded early intervention services limited by parent choice to one hour weekly. Child B’s mother, 32 years of age, was a college graduate with special education work experience. Child B, who entered the study at age 33 months, had a diagnosis of epilepsy. He received 7–8 h weekly of Part C-funded early intervention services and transitioned to Part B preschool services during his participation in the study. Two older siblings, both boys, had also received Part C services. Child C’s mother, age 23, was a high school graduate who reported that she had diagnoses of dyslexia, ADHD, bipolar disorder, and previous addiction to narcotics. Child C, age 22 months at entry, also had two older siblings who had received early intervention services. The family participated in Part C-funded services 2 h weekly and his mother reported that Child C had diagnoses of asthma and epilepsy. All three mothers reported pregnancy complications resulting in extended bed rest. Developmental assessment results were gathered from early intervention providers. Screening and assessment scores are presented in Table 1.
Design
A mixed methods research design can serve purposes not achievable through quantitative or qualitative methodologies carried out alone, including complementarity, defined as enhancement through exploration of overlapping or related data (Johnson & Onwuegbuzie, 2004). In the current study, complementarity of data was achieved through the combination of single subject multiple baseline and qualitative research designs. The single subject design was implemented across targeted outcomes for the purpose of documenting causal relationships between the intervention and child performance in the four levels of social-communicative competency: focusing on faces, turn-taking, responding to joint attention, and initiating joint attention. This design, replicated across the three participants, resulted in a graphic depiction of changes in child performance for each level. The inclusion of multiple participants with staggered movement from baseline into intervention conditions isolated changes attributable to the intervention from those possibly related to external factors such as maturation. A sufficient number of data points demonstrated stable patterns for baseline and intervention conditions.
Although single subject design studies typically report on structured behavioral and skill-based interventions using measures that correspond to elicited skills, this study applies the design to nonverbal social communication outcomes that are not directly “trained” through a structured reinforcement-based approach. Rather, in Heflin and Simpson’s (1998) conceptualization, this model can be classified as “relationship based” in that it fosters parent–child interaction in a planned, but open-ended format within the context of the relationship rather than through a skill-based approach that reinforces specific skills in isolation or as ends in themselves. In the current study, the intervention targeted relationship-based competencies through the open-ended medium of parent–child interaction and did not employ a specific program of reinforcement apart from that derived naturally from the interaction. Similarly, Ingersoll and Dvortcsak (2006) distinguished between “direct” and “indirect” teaching methods with direct methods including naturalistic behavioral approaches that use learning theory techniques (e.g., Kaiser & Hemmeter, 1996; Koegel & Schreibman, 1996) and indirect methods including developmental approaches that focus on parent–child interaction and emphasize parent responsivity. Using this framework, the current study employs indirect methods. In these respects, the approach aligns with those described by Greenspan and Weider (1999), Klein (2003), McCollum (1984), and Prizant et al. (2000).
To explore underlying family and intervention-related variables that may have influenced child performance and to shed light on parents’ understanding of, progress with, and response to their role in the intervention, a complementary qualitative research design was implemented using data from audiotaped parent–researcher discussions and parent notes. The qualitative analysis explored influences that may have played a role in observed changes. Data from initial parent interviews and weekly parent–researcher conversations included intervention-related concerns and other parent-identified issues. Initial interview questions included the M-CHAT items and questions that explored the children’s development, parents’ desires related to parent–child communication, and parents’ conceptions of the parent-professional role. Parents’ daily notes included descriptions of children’s participation in daily parent–child interaction.
Intervention Procedure
Intervention sessions were conducted in families’ homes. To promote interaction, parents played face-to-face games using toys that were present in the home. The Joint Attention Mediated Learning (JAML) manual (Schertz, 2005c) provided a framework for parent–child interaction. The manual’s content focused on developmental foundations of joint attention and the format was modeled on the Affective Cognitive Enabling: Mediating Learning Strategies curriculum (Kahn & Hosaka, unpublished), a curriculum targeting parent mediation of infant cognitive learning. At the end of the baseline period, the researcher provided parents with an oral and written overview of mediated learning principles (adapted from Klein (2003)) as they relate to development of joint attention and as children progressed, explanations and suggested activities were provided for each of the four intervention phases.
Phases were introduced in sequence, along with descriptions of targeted competencies and their importance. Two levels comprised each phase, the first relying on parent initiative and the second seeking more initiative from the child. Rather than rigid prescriptions, suggested activities were intended to help parents envision ideas of their own to encourage their child’s best response. Suggested activities were linked to earlier-presented mediated learning principles.
Focusing on faces strategies were aimed at increasing child tolerance for looking at faces, the single greatest difference found between 12-month-olds later identified with and without autism (Osterling & Dawson, 1994) and an avenue for the child to discern social cues. Examples included using interactive face-oriented vocal games with strong rhythms, pairing looks to the face with expressions of affection, making the parent’s face hard to avoid, imitating facial gestures, and mirror play. Turn-taking activities aimed to promote reciprocity, a component of joint attention, and included imitation of child-initiated gestures, responding to child actions as if they were intended as interactions, embedding parents’ actions into the child’s isolated repetitive play, following the child’s lead, pausing for the child’s response after the parent’s turn, and playing teasing games. Responding to joint attention strategies targeted shared attention to objects through supportive parent initiations. For example, parents were encouraged to introduce a toy after establishing eye contact, hold the toy close to their faces when offering it to the child, and use excitement or suspense to encourage the child to look between a toy and the parent’s face. Finally, initiating joint attention activities encouraged the child to engage the parent’s attention in relation to an object by expressing excitement about the child’s play with a toy or introducing “surprise” bags or wrapped packages.
Parents were requested to spend approximately one hour daily in face-to-face parent–child interaction, selecting and implementing activities in routine and planned interactions and to describe child performance in brief daily notes. Weekly sessions with the researcher included a review of parent notes, videotaping of a 10-min parent–child interaction session for data analysis, introduction of new material, joint planning for the upcoming week, and discussion of parent concerns. Dyads A and B were scheduled for once weekly and Dyad C for twice weekly sessions, but actual participation was closer to once weekly for Dyad C. The number and duration of sessions in which the families participated are presented in Table 2. Intervention was discontinued for Children B and C when they had progressed through the four phases of intervention and showed multiple instances of initiating joint attention. Intervention was discontinued for Child A after mutual agreement by his mother and the researcher that his response to the intervention had reached a plateau.
Data Collection and Analysis
Parents were informed of the four targeted outcomes before data collection began, allowing them to elicit their child’s best performance during the baseline condition. An experienced early intervention provider was trained on coding criteria to an average Kappa agreement level of .89. Naïve to the baseline or intervention condition, the coder observed each 10-s interval from weekly videotaped 10-min parent–child interaction sessions (60 segments per session) for occurrence of targeted outcomes. Focusing on faces was coded if the child looked at any part of his mother’s face during the interval. Turn-taking required the child to perform one of at least two actions as part of a full turn-taking routine completed within no more than two consecutive intervals. Responding to joint attention was credited if the child responded to the parent’s attempt to draw his attention to an object by alternating looks between the parent’s face and the object for the apparent purpose of sharing interest. Initiating joint attention was coded if the child alternated looks between the parent’s face and an object for the apparent purpose of drawing the parent’s attention to the object (i.e., “showing”). Interobserver agreement (Kappa), calculated on 25% of videotaped sessions, was .86 for focusing on faces (range = .73 to .96), .82 (range = .47 to 1.00) for turn-taking, .80 (range = .66 to .92) for responding to joint attention, and .87 (range = .73 to .92) for initiating joint attention with a mean Kappa agreement of .84.
Qualitative data were collected from initial interviews, weekly sessions, and daily parent notes. Audio-recordings yielded 257 pages of field notes for analysis. These notes were coded, organized into categories, and analyzed for emergent themes that centered on the relationship of the intervention to child progress, parent-voiced challenges, and indicators of resilience. QSR NVivo© software provided a structure for organizing and coding the qualitative data. Triangulation, achieved through convergence within and across the qualitative and quantitative data, strengthened the credibility of conclusions. For example, parent responses to a social validity questionnaire supported qualitative descriptions of child changes and parent reports of child progress converged with videotape data. All parent participants were offered an opportunity to verify and clarify qualitative data and conclusions and the one parent who accepted reported agreement with no recommendations for changes. A second experienced early intervention provider, working from six randomly selected transcripts, identified codable items and found that 97% were addressed in researcher memos, that all quotes were represented accurately, and that all associated interpretations and conclusions in the final report were supported by source data.
In fidelity of intervention measures, a comparison of weekly audio transcriptions to child outcomes confirmed that intervention phases were introduced sequentially in researcher guidance to parents. When a child showed multiple instances of the targeted outcome in a phase in each of at least two sessions, and both the parent and researcher agreed that the child was ready to move on, the phase was reinforced and a new phase introduced. To establish fidelity of parent–child mediation, daily parent notes were reviewed for indications that parents had demonstrated an understanding of and adherence to the active phase of intervention in their reports of daily parent–child activities. The percentage of notes that showed full, partial, and no fidelity was calculated and is presented in Table 2. Parents B and C showed close fidelity with weekly intervention plans while Parent A showed difficulty with conceptual understanding of turn-taking and joint attention, resulting in less adherence to the appropriate phase of intervention in reported daily activities.
Results
Quantitative
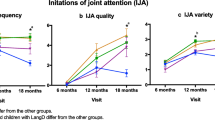
Changes in child performance were reflected as the number of 10-s intervals during weekly 10-min video segments in which the child engaged in focusing on the parent’s face, turn-taking, responding to parents’ joint attention overtures, and initiating joint attention encounters with the parent. These data are shown in Fig. 1 with child progress tracked through the ordered presentation of phases preceded by baseline conditions of increasing duration. Before the intervention was introduced, the three toddlers showed varying levels of focusing on faces and turn-taking, however none showed responding to or initiating joint attention, the ultimate goal of the intervention. With intervention, Child A’s greatest area of improvement was focusing on faces with moderate progress in turn-taking and slight progress with the two joint attention measures. Child B showed steady improvement in all phases with progress closely following the introduction of each new phase. Child C, who engaged in focusing on faces before beginning intervention, progressed rapidly through the remaining three phases and showed instances of joint attention before those phases had been formally introduced. In the intervention condition, each of the three toddlers surpassed baseline performance levels for all four targeted outcomes.

Individual child progress on targeted outcomes by phase of intervention. Note: FF = focusing on faces; TT = turn-taking; RJA = responding to joint attention; IJA = initiating joint attention; FU = follow-up
Generalization and Maintenance
In alternative settings (kitchen, back yard, and restaurant), all parents elicited the same range of child performance that had been consistently observed in previous sessions. Although parents were not asked to continue the intervention at the conclusion of the intervention phase, in 5-week post-intervention maintenance measures, each child’s performance for every phase was higher than his mean performance during baseline conditions and exceeded mean intervention condition levels for the majority of targeted competencies (see Table 3).
Social validity measures assessed the degree to which goals, techniques, and outcomes of the intervention were acceptable to the three parents. A researcher-developed five-point Likert scale questionnaire allowed for differentiated levels of response as recommended by Schwartz and Baer (1991). This approach to measurement of social validity diverges from that used in other joint attention intervention research which evaluated “normalcy” ratings (Whalen & Schreibman, 2003) but was similar to the approach used in a recent study that provided training to parents of children with autism (Ingersoll & Dvortcsak, 2006). Parent responses, summarized in Table 4, indicated parents’ support for the importance and appropriateness of intervention goals, their role in implementation, their participation in weekly sessions, activity suggestions, and level of intrusiveness. All parents predicted better long-term child competence as a result of the intervention and indicated improved confidence in their own ability to support child interaction. Parents B and C expressed satisfaction with the level of child improvement in all intervention phases while Parent A noted her son’s limited progress in joint attention phases. Another indicator of parents’ commitment to and acceptance of the intervention, participation in weekly sessions, varied across participants; however, all participated in most scheduled sessions.
Qualitative
Parents’ views of child progress, expressed in weekly discussions with the researcher and in their daily notes, mirrored trends in the quantitative data. These qualitative data coalesced into five themes, providing insight into variables possibly associated with child progress and suggesting implications for intervention and future research: (a) parent fidelity with planned intervention mediated child progress, (b) child progress in social-communication development facilitated reduced aggression, (c) physical activity motivated children to interact, (d) simplifying the presentation of the parent’s face facilitated focusing on faces, and (e) turn-taking activities based on face-to-face play promoted joint attention better than play with toys.
The researcher provided planned and sequential, but informal guidance on the four phases of intervention. To promote focusing on faces, the researcher provided explanations, possible activities, and affirmation of parent competence.
He’s learning about social skills [and] communication.... You can think of success in terms of how long he can sustain that eye contact..., keeping him engaged with you as long as he will tolerate it; moving your head toward or away from him into his line of vision..., helping him to succeed by making your face hard to avoid.... Your affective involvement [gives] meaning to looking at faces.
Parents’ internal debates and observations helped them work through issues and gain conceptual understanding and buy-in as they progressed through the phases. In the initial phase of focusing on faces, Parent B reported, “I just feel so bad for him, because it seems like I have to calm him just to get him to [look at me].... There are days when I think... he needs to have his own world for whatever reason.” Later she observed, “He will look straight at you if he is wearing sunglasses and I think in his mind it’s ‘You can’t see my eyes.... I’m getting not just more eye contact and interaction when he’s really happy, but also when he’s really mad”. Parent C described how she and her husband had encouraged looks to their faces. “When we were talking to him, we noticed that his eyes would drift downwards, and... we’d kind-of touch him right there and his eyes would go toward our eyes.” All three parents were observed to easily conceptualize the focusing on faces phase of intervention and to integrate it into parent–child interactions. This factor likely contributed to the rapid child progress observed during this phase (Note: Child C showed competency with focusing on faces during the baseline phase).
In the turn-taking phase, the researcher provided explanations and examples. “We want him to get into that reciprocal back-and-forth thinking..., to involve you in his activity [so] it’s not just about him, but it’s [also] about another person.”. Parents showed creativity in building on their children’s interests. “I found that if I keep it very light and very simple, and I don’t demand too much of him, it becomes a pleasant experience” (Parent B). “I counted his toes, then I patted the bottom of his foot, and when I did, he’d like that, so every couple of seconds, he’d stick his foot back up and I’d pat it again.” Parent C reported on an activity of stacking baby formula cans. “I had my hand sitting right there and he... let me know [when it was my turn] by giving me that little look”. Children B and C both showed strong progress in response to turn-taking intervention as seen in Fig. 1. Dialogue with Parent A showed that she had some difficulty conceptualizing and eliciting reciprocity in turn-taking, relying on a limited number of rote activities such as manipulating a busy box. It is not clear whether this factor or the severity of her child’s autism contributed to his uneven response to the intervention.
In the third and fourth phases of intervention, the researcher described the relationship of joint attention to language and clarified parameters. In one example, Parent A struggled to translate the concept of joint attention into daily interactions when she described her child nonverbally asking for help putting beads into a can. “He needs me to do it; he needs help.” The researcher clarified to distinguish this from joint attention, “Yes, he’s requesting because he can’t do it himself.” Recognizing the sharing aspect of joint attention, Parent A offered, “His books are joint attention because sometimes he’ll bring it and come over and let us sit with him and look at it.” The researcher again clarified that, “[We want] him to show you that he’s interested by looking at the book and then looking at your face.” Parent B revealed her initial skepticism that her son could engage in joint attention. “I would be surprised if he saw a novel thing and... looked at me as if to say ‘look, this is really neat’”. Later however, she reported the first observed instance of initiating joint attention. Her son brought his portable video player to her and suddenly he “looked at the video... and then at my eyes and smiled... I’m sure he was trying to show me his cartoon––for a couple of seconds, we enjoyed something together”. As illustrated in Fig. 1, Children B and C showed a strong response to the intervention in phases 3 and 4 while Child A showed only isolated instances of joint attention.
The emergence of receptive and expressive verbal language at the end of the intervention, although not included in quantitative measures because it was not a directly planned outcome, was voluntarily reported by parents and observed by the researcher. This development was notable with Children B and C, both of whom had engaged in joint attention in multiple sessions. Child A achieved a level of competency with Picture Exchange Communication System (PECS) for requesting. Parent C described the beginnings of receptive and expressive language. “[His grandmother] said, ‘See ya’ and he goes ‘Ee ya’. We asked if he wanted [a soda] and he goes [shakes head “yes”].... So I think he’s starting to comprehend what we’re asking.”
Although not assessed quantitatively, parents volunteered background information on the larger family experience that may have impacted intervention effectiveness. They also described their own challenges and resilience relative to their children’s needs. Emergent themes reflecting challenges included searching for a diagnosis, limited child response to traditional services, co-occurrence of familial disabilities, and broader family stressors. Themes of parent resilience included coming to terms with the child’s diagnosis and evolving views of the child’s potential and of their own competence and self-efficacy.
Parents related difficulties, most prominently behavioral challenges, that were associated with their children’s autism. Parent A connected her son’s tantrums to his restricted interests. “He’s so zombie into the movie lately. I don’t know how to get out of it. I turned off the TV..., then he just went into more of a fit, and he punched and hit and went all out.” Early in the intervention period, Parent B also wearied of her son’s constant demands. “In the morning I can be pretty good about it, but by [evening]..., I’m like, ‘You have to take him. I don’t want to be touched; I don’t even want to be looked at.” She also worried about empathy. “If one of the other boys gets hurt..., [he] may be interested in looking at the tears to try to figure out where they came from, but he doesn’t seem to understand that means that someone’s hurt.” Parent C expressed concern with her son’s aggression, noting that he began to engage in frequent head butting and biting beginning at approximately 18 months of age. Parent B’s initial concerns about her son’s aggressiveness abated as he progressed through the intervention. By parent report, Child C’s aggressive behaviors continued throughout the intervention period with some reduction by follow-up; however, larger family concerns may have helped to maintain his aggression. By observation and parent report, Child A’s aggressive behavior showed no signs of abatement during the intervention or follow-up phases.
During the intervention period, all participants struggled with the initial tentative nature of their child’s diagnosis (a factor that compromised the process of coming to terms) and the struggles they experienced obtaining a definitive diagnosis. Parent A reported that her doctor did not give her direct answers when she expressed initial concerns. When diagnosticians reported preferring to wait until age three to give a diagnosis of autism, she reported responding, “I’m stuck because there are a lot of things I need the diagnosis for [eligibility for services; helping her husband come to terms with their son’s difficulties].” Parent B also reported experiencing initial uncertainty about the source of developmental concerns and sought out initial and later confirming diagnoses. Parent C expressed relief at her son’s tentative early diagnosis. Although she questioned the diagnosis after seeing intervention-related improvement, the original results were confirmed. All mothers reported that their husbands followed a more difficult path in coming to terms with the diagnosis. Over the course of the intervention, two of the husbands left their families, a move that both mothers attributed to the stress of having a child with autism.
Before the research intervention began, Parent B reported that in spite of the high level of services received, “I don’t think we’re helping him [with traditional services]”. She referred to the continual need to “lower the bar” of expectations and noted a lack of progress over the two years her child had received services. This pattern was repeated with the other two dyads. All participants reported co-occurrence of learning disabilities or other developmental concerns among members of their immediate families. Parents A and C reported on their own learning disabilities and mental health concerns. Parents B and C noted developmental and medical concerns with siblings, including seizure disorders. Paternal aggression was reported by Parent C and income limitations contributed additional stressors for this family. Limited support from extended family was cited to varying degrees by all participants.
All participants were motivated to counteract these challenges. They showed an interest in learning about autism and progressed from focusing primarily on their children’s limitations toward increasing acceptance and recognition of child potential. Parent B observed, “I am getting more awareness that I am here. It’s not just because he needs something... and I feel like that is huge progress”. Parent A recognized progress with focusing on faces and Parent C expressed excitement with her child’s use of receptive and expressive language. Parents also invested in their own personal development, Parent A by teaching herself to read and participating in an autism support group; Parent B by creating a support group for families, sharing her intervention experiences at a national conference, and pursuing employment in a related field; and Parent C by learning about her children’s complicated medical issues and initiating licensed practical nurse training. All parents took firm control of their children’s services.
Discussion
This study provides evidence that in response to a parent mediated, developmentally oriented, and interaction based intervention model, two of three toddlers with early identified autism demonstrated joint attention, a typical milestone that failed to develop naturally. The third demonstrated progress with focusing on faces and turn-taking, hypothesized precursors of joint attention. Results complement Whalen and Schreibman’s (2003) study which used behavior modification to promote joint attention in older preschoolers with autism. Achievement of child outcomes in the current study may be attributable to a family centered approach that built on developmental foundations of joint attention and used the parent–child relationship as the medium for intervention, harnessing parents’ expertise and strong investment in their children’s developmental outcomes. Parents infused intervention through play and in natural family routines, an approach that had secondary benefits for parents by helping them to envision both the child’s potential and their own abilities as ongoing mediators of their children’s learning.
Results point to the possible importance of providing a developmental foundation to support both symbolic communication and its precursor, joint attention. Joint attention research indicates that face-to-face engagement, social interaction, child initiation, and responding to joint attention may provide a developmental foundation for the child to freely initiate joint attention social overtures to a partner (Adamson & Bakeman, 1991).These developmental precursors to initiating joint attention were operationalized in the current study as focusing on faces, turn-taking, and responding to joint attention. Joint attention, in turn, appears to provide a developmental foundation for verbal language (e.g., Carpenter et al. 1998; Paparella & Kasari, 2004). Attention to others’ faces, an ability that is compromised for infants later diagnosed with autism, is a necessary component of joint attention because it allows the child to ascertain the partner’s interest in their mutual focus of attention. Turn-taking, also a component of joint attention and a form of reciprocity, further supports the interactional aspects of joint attention. Turn-taking may lead most directly to joint attention if it is initially based on dyadic play rather than play with toys because it is engagement with the parent that is a greater need for children with autism than attention to objects. Initiating joint attention is typically built on a base of responding to joint attention and this appears to have occurred with the toddlers with autism in this study. Eliciting initiation of joint attention required from the parent only a receptive demeanor once this foundation had been laid.
Because of social difficulties in autism, the current study was designed to build on the already established parent–child relationship. The intervention did not train parents in specific techniques; rather, parents created activities that they believed would best encourage their child’s social participation across contexts and over time in the child’s natural environment. This encouraged parents’ leadership in the intervention while capitalizing on their expertise, intimate knowledge of the child, and strong investment in child outcomes. The interventionist assumed a supporting role, highlighting the purpose and goals of each phase, providing examples of activities that parents could adapt, and tracking changes.
The intervention addressed other difficulties inherent in more structured skill-based interventions. One concern is that joint attention is an abstract ability that is not easily “trained” (Kasari et al., 2001). The mediated learning approach addresses this concern as well as related problems of generalization and maintenance often reported in behaviorally oriented approaches. The aim of mediated learning approaches is to affect the child’s desire to learn and interact rather than to train specific skills through a system of external rewards (Klein, 2003). Parents in this study appeared to have an instinctive grasp of how to mediate learning for their children but needed guidance on the meaning and importance of joint attention for future language and social development. Parents with varying abilities were able to create opportunities to promote interactional competencies when armed with general theoretical knowledge and suggested strategies. Benefits were also observed for parents themselves, who expressed greater confidence in their child’s potential and in their role in effecting child changes. Importantly, these changes were evident irrespective of their socioeconomic and educational experiences.
The interventionist’s role is more complex in this model than in more traditional professionally implemented approaches. Interventionists must master theory and make it accessible to adult learners, provide situational coaching based on ongoing assessment of parent understanding, serve as a sounding board and source of support relative to a wide range of parent concerns, bolster parents’ confidence in the possibility of change, and recognize and affirm parents’ competence. This role relies on sharing theoretical knowledge and posing questions that can include parents in the discovery process in ways that build on existing child and parent competencies (i.e., beginning at a skill level where both parent and child can experience success). To address these needs, personnel training should focus on theory related to joint attention, family systems, and adult learning theory. The use of family case studies (e.g., McWilliam, 2000) can support understanding of complex family needs in times of crisis, parents’ potential to promote early social communication development even in the face of serious child and parent challenges, and the individualization of parent education, coaching, and support strategies.
Findings in the current study are limited by the small number of participants and by the fact that the intervention was implemented and reported by a single researcher. Also, confidence in follow-up measures is qualified by the limitation of nonrepeated measures (i.e., a single data point). A limitation with the intervention is that while many parents may prefer the flexibility and freedom of selecting or creating their own activities based on a sample of suggested activities, others (e.g., those challenged to conceptualize intervention goals) may benefit from more targeted guidance and structure relative to activity selection. Future studies are therefore needed to replicate and extend this research. Qualitative findings also suggest questions for further study: Can simplifying the presentation of the parent’s face facilitate focusing on faces? How can turn-taking activities best be designed to lead to joint attention? What is the impact of joint attention development on child aggression?
Research findings suggest implications for practitioners. First, recommended family-centered and family-guided practices (Sandall, McLean, & Smith, 2000) for young children with disabilities should take a more prominent role in early autism intervention as these findings demonstrated the potential efficacy of such approaches. Second, building intervention from the parent–child relationship is a priority as children are identified at toddler ages during which the relationship with the caregiver naturally serves as the primary medium for social-communicative learning. Third, recommendations that services for young children with autism be intense should be examined in light of current findings that joint attention can be effectively promoted for some toddlers with autism using once weekly intervention that supports developmentally grounded parent–child interaction in natural family settings. This contrasts with models that call for intensive investment of intervention resources that directly target specific skills, that are implemented by specialists, and that must be supplemented by additional resources to promote generalization to natural environments. One factor that may have influenced response to the low intensity approach in the current study is the early age at which this intervention was initiated. Fourth, developmental precursors of joint attention (e.g., focusing on faces, turn-taking, etc.) and symbolic language (e.g., joint attention) should be incorporated into intervention for children with autism to lay the groundwork for more natural development of higher level competencies. Fifth, because of the high levels of stress experienced by families who are in the initial stages of autism diagnosis, attention to larger family concerns may play an important role in a parent-implemented intervention and warrant further study. For example, future research could explore whether fathers being more actively in the intervention might facilitate their process of “coming to terms”, with resultant positive outcomes for families. Finally, relying on less formal and definitive diagnostic protocols to identify high risk for autism during the toddler years may be important to permit initiation of services before nonproductive patterns of interaction are established.
References
Adamson, L. B., & Bakeman, R. (1991). The development of shared attention during infancy. Annals of Child Development, 8, 1–41.
Adamson, L. B., & Russell, C. (1999). Emotion regulation and emergence of joint attention. In P. Rochat (Ed.), Early social cognition: Understanding others in the first months of life (pp. 281–297). Mahway, NJ: Erlbaum.
Baron-Cohen, S. (2000). Autism: Deficits in folk psychology exist alongside superiority in folk physics. In H. Tager-Flushberg, & D. J. Cohen (Eds.) Understanding other minds (pp 73–82). York: Oxford University Press.
Bono, M. A., Daley, T., & Sigman, M. (2004). Relations among joint attention, amount of intervention, and language gain in autism. Journal of Autism and Developmental Disorders, 34, 495–505.
Bredekamp, S., & Copple, C. (1997). Developmentally appropriate practice in early childhood programs (Revised edition). Washington, DC: National Association for the Education of Young Children.
Bryson, S. E., Rogers, S. J., & Fombonne, E. (2003). Autism spectrum disorders: Early detection, intervention, education, and psychopharmacological management. Canadian Journal of Psychiatry, 48, 506–516.
Butera, G., & Haywood, H. C. (1992). A cognitive approach to the education of young children with autism. Focus on Autistic Behavior, 6, 1–14.
Carpenter, M., Nagell, K., & Tomasello, M. (1998). Social cognition, joint attention, and communicative competence from 9 to 15 months of age. Monographs of the Society for Research in Child Development, 63(4, Serial No. 255), 1–142.
Carpenter, M., & Tomasello, M. (2000). Joint attention, cultural learning, and language acquisition. In A. M. Wetherby, & B. M. Prizant (Eds.), Autism spectrum disorders (pp. 31–54). Baltimore: Brookes.
Dawson, G., & Osterling, J. (1997). Early intervention in autism. In M. J. Guralnick (Ed.). The effectiveness of early intervention (pp. 307–326). Baltimore: Brookes.
Dumont-Mathieu, T., & Fein, D. (2005). Screening for autism in young children: The Modified Checklist for Autism in Toddlers (M-CHAT) and other measures. Mental Retardation and Developmental Disabilities Research Reviews, 11, 253–262.
Feuerstein, R. (1980). Instrumental enrichment: An intervention program for cognitive modifiability. Baltimore: University Park Press.
Greenspan, S., & Wieder, S. (1999). A functional developmental approach to autism spectrum disorders. Journal of the Association for Persons with Severe Handicaps, 24, 147–161.
Haywood, H. C., Brooks, P., & Burns, S. (1992). Bright start: Cognitive curriculum for young children. Watertown, MA: Charlesbridge Publishing.
Heflin, L. J., & Simpson, R. L. (1998). Interventions for children and youth with autism: Prudent choices in a world of exaggerated claims and empty promises. Part I: Intervention and treatment option review. Focus on Autism and Other Developmental Disabilities, 13, 194–211.
Howlin, P., & Moore, A. (1997). Diagnosis in autism: A survey of over 1200 patients in the UK. Autism, 2, 135–162. .
Ingersoll, B., & Dvortcsak, A. (2006). Including parent training in early childhood special education curriculum for children with autism spectrum disorders. Journal of Positive Behavior Intervention, 8, 79–87.
Johnson, R. B., & Onwuegbuzie, A. J. (2004). Mixed methods research: A research paradigm whose time has come. Educational Researcher, 33, 14–26.
Kaiser, A. P., & Hemmeter, M. L. (1996). The effects of teaching parents to use responsive interaction strategies. Topics in Early Childhood Special Education, 16, 375–407.
Kasari, C., Freeman, S. F. N., & Paparella, T. (2001). Early intervention in autism: Joint attention and symbolic play. International Review of Research in Mental Retardation, 23, 207–237.
Klein, P. S. (2001). Mediational intervention for sensitizing caregivers (MISC) in Ethiopia. In P. S. Klein (Ed.), Seeds of hope (pp. 29–93). Oslo, Norway: Unipub Forlag.
Klein, P. S. (2003). A mediational approach to early intervention: Israel. In S. L. Odom, M. J. Hanson, J. A. Blackman, & S. Kaul (Eds.), Early intervention practices around the world (pp 69–89). Baltimore: Paul H. Brookes.
Koegel, R. L., & Schreibman, L. (1996). Fostering self-management: Parent-directed pivotal response training for children with autistic disorder. In E. D. Hibbs & P. S. Jenson (Eds.), Psychosocial treatments for child and adolescent disorders (pp. 525–552). Washington, DC: American Psychological Association.
Mahoney, G., & Perales, F. (2003). Using relationship-focused intervention to enhance the social-emotional functioning of young children with autism spectrum disorders. Topics in Early Childhood Special Education, 23, 77–89.
McArthur, D., & Adamson, L. B. (1996). Joint attention in preverbal children: Autism and developmental language disorder. Journal of Autism and Developmental Disorders, 26, 481–495.
McCollum, J. A. (1984). Social interaction between parents and babies: Validation of an intervention procedure. Child: Care, Health, and Development, 10, 301–315.
McWilliam, P. J. (2000). Lives in progress. Baltimore: Brookes.
Mundy, P., Sigman, M., Ungerer, J., & Sherman, T. (1986). Defining the social deficits of autism: The contribution of non-verbal communication measures. Journal of Child Psychiatry, 27, 657–669.
Mundy, P., & Stella, J. (2000). Joint attention, social orienting, and nonverbal communication in autism. In A. M. Wetherby & B. M. Prizant (Eds.), Autism spectrum disorders (pp. 55–77). Baltimore: Brookes.
National Research Council (2001). Educating children with autism. Washington, DC: National Academy Press.
Osterling, J., & Dawson, G. (1994). Early recognition of children with autism: A study of first birthday home videotapes. Journal of Autism and Developmental Disorders, 24, 247–257.
Paparella, T., & Kasari, C. (2004). Joint attention skills and language development in special needs populations: Translating research to practice. Infants and Young Children, 17, 269–280.
Pretti-Frontczak, K., & Bricker, D. (2004). An activity-based approach to early intervention (3rd ed.). Baltimore: Paul H. Brookes.
Prizant, B. M., & Wetherby, A. M. (1998). Understanding the continuum of discrete-trial traditional behavioral to social-pragmatic developmental approaches in communication enhancement for young children with autism/PDD. Seminars in Speech and Language, 19, 329–352.
Prizant, B. B., Wetherby, A. M., & Rydell, P. J. (2000). Communication intervention issues for children with autism spectrum disorders. In A. M. Wetherby, & B. M. Prizant (eds.), Autism spectrum disorders: A transactional developmental perspective (pp. 193–224). Baltimore: Paul H. Brookes.
Robins, D. L., Fein, D., Barton, M. L., & Green, J. A. (2001). The Modified Checklist for Autism in Toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. Journal of Autism and Developmental Disorders, 31, 131–144.
Sandall, S., McLean, M. E., & Smith, B. J. (2000). DEC recommended practices in early intervention/early childhood special education. Longmont, CO: Sopris West.
Schertz, H. H. (2005a). Promoting joint attention in toddlers with autism: A parent-mediated developmental model. (Doctoral dissertation, Indiana University, 2005). Dissertation Abstracts International, 66, 3982.
Schertz, H. H. (2005b). Joint attention. In J. T. Neisworth, & P. S. Wolfe (Eds.), Autism and pervasive developmental disorders dictionary Baltimore: Brookes, (pp. 115).
Schertz, H. H. (2005c). Joint Attention Mediated Learning (JAML) manual. Unpublished manuscript.
Schertz, H. H., & Odom, S. L. (2003). Joint attention and early intervention with autism: A conceptual framework and promising approaches. Journal of Early Intervention, 27, 42–54.
Schopler, E., Reichler, R. J., & Renner, B. R. (1988). The Childhood Autism Rating Scale (CARS). Los Angeles, CA: Western Psychological.
Schwartz, I. S., & Baer, D. M., (1991). Social validity assessments: Is current practice state of the art? Journal of Applied Behavior Analysis, 24, 189–204.
Siegel, B. (2001). Pervasive Developmental Disorders Screening Test – II (PDDST-II): Stage 1 screener for primary care settings. Retrieved September 1, 2004 from http://eiiswest.nsnet.org/Referral_Package/pddst2.pdf.
Stone, W. L., Coonrod, E. E., & Ousley, O. Y. (2000). Brief report – screening tool for autism in two-year-olds (STAT): Development and preliminary data. Journal of Autism and Developmental Disorders, 30, 607–612.
Vaughan, A., Mundy, P., Block, J., Burnette, C., Delgado, C., Gomez, Y., et al. (2003). Child, caregiver, and temperament contributions to infant joint attention. Infancy, 4, 603–616.
Volkmar, F. R., Lord, C., Bailey, A., Schultz, R. T., & Klin, A. (2004). Autism and pervasive developmental disorders. Journal of Child Psychology and Psychiatry, 45, 135–186.
Whalen, C., & Schreibman, L. (2003). Joint attention training for children with autism using behavior modification procedures. Journal of Child Psychology and Psychiatry, 44, 456–468.
Yoder, P. J., & Warren, S. F. (1999). Maternal responsivity mediates the relationship between prelinguistic intentional communication and later language. Journal of Early Intervention, 22, 126–136.
Acknowledgments
This research was conducted as preparation for a doctoral dissertation. The first author would like to acknowledge the support and assistance of her advisor, Dr. Samuel L. Odom and other members of her dissertation committee including Dr. Susan Klein, and Dr. Gretchen Butera, all of Special Education department at Indiana University, and Dr. Naomi Swiezy from the Christian Sarkine Autism Treatment Center at Riley Hospital for Children. The author also thanks the three parent participants for implementing the intervention, Shelley McAllister for coding the video data, and Anne Wagner for reviewing the qualitative data.
Author information
Authors and Affiliations
Corresponding author
Appendix A
Appendix A
Joint Attention Mediated Learning (JAML) Parent Manual (excerpt)
The following pages have ideas for helping your child make progress in focusing on faces, turn-taking, and joint attention––all important to help your child communicate and interact socially with others. Each idea or learning strategy is just that––an idea. Working with the researcher, you will have other ideas that can help reach similar goals. Each strategy is connected with one or more learning principles, identified in bold after each strategy.
These learning principles show five ways to help children learn. The five learning principles are:
-
1.
Focusing: Helping your child to focus helps her look at or listen to something that can help her learn, to share attention with you by looking at what you want her to see, or by showing you what she wants you to see.
-
2.
Giving meaning: You can help your child understand the meaning of things by expressing your feelings (such as excitement) when you are sharing attention with him about an object or a happening. Giving meaning helps him to understand what parts are important to pay attention to because they are special in some way.
-
3.
Expanding: When you and your child are paying attention to something, you can help your child to expand his understanding of an object or event. You do this by providing labels, by helping him see something about an object that he had not noticed before, or by seeing how something relates to other things he knows about.
-
4.
Encouraging: Toddlers learn best when they feel successful. You can help your child experience success by making activities challenging enough but not too hard, by pointing out what he did that caused his success, by expressing affection when he is successful, and by showing him that you are confident that he can succeed.
-
5.
Organizing and planning: Helping your child experience order can boost his learning by helping him see how what he is doing relates to the larger world. If activities are structured, he can better predict what comes next. He may be more willing to do something that he does not like (but that is important for his learning) if he knows a preferred activity will come later. Also, if activities happen in a logical sequence, your child can better see the connections between things. Structure is especially helpful to promote learning for toddlers with social and communication difficulties. You can help to structure activities by
-
a.
showing your child only the part he needs to know for what you want him to learn,
-
b.
helping him to keep his attention on one thing at a time,
-
c.
reducing sights and sounds that may draw his attention away from the activity,
-
d.
helping him to understand “first ___, then ____” (to know what comes next),
-
e.
moving gradually from simple tasks to ones that are more complicated,
-
f.
helping him to see how things are organized––the relationships between things
-
g.
keeping objects in the same location; putting toys in order at the end of play
-
h.
helping him to understand the value of rules.
During play sessions, all of the time is not spent working on new and more difficult learning strategies. It is important that your child enjoy interacting with you and experience success most of the time. The targeted strategies will help him to learn new things, and these new activities should be mixed in with comfortable activities he already knows, enjoys, and is successful with. However, the purpose of the parent–child play sessions is for him to interact, so you should expect your child to interact with you during all play activities––he can be left to play with toys on his own at other times.
Children learn best when they choose their activities. You can help this to happen by following your child’s lead. You do this by joining into his play rather than asking him to switch from something he is doing to an activity you want to do. However, you can guide him toward new activities when he loses interest with an activity. The most important thing to remember is to keep him engaged in interaction with you as long as possible.
Suggested strategies for developing your child’s social-communication skills are divided into four areas: (1) focusing-on-faces, (2) turn-taking, (3) responding to joint attention, and (4) initiating joint attention. Each of these four areas is divided into two levels. With the first level, you are doing most of the work by showing your child how to do things. In the second level of each area, your child is expected to do more of the work by practicing the skills you have taught him.
Rights and permissions
About this article
Cite this article
Schertz, H.H., Odom, S.L. Promoting Joint Attention in Toddlers with Autism: A Parent-Mediated Developmental Model. J Autism Dev Disord 37, 1562–1575 (2007). https://doi.org/10.1007/s10803-006-0290-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-006-0290-z