
Abstract
Children with Autism Spectrum Disorders (ASD) and children with Obsessive Compulsive Disorder (OCD) were compared on a range of repetitive behaviours. Parents reported similar levels of sameness behaviour and repetitive movements in the clinical groups, although children with OCD engaged in more repetitive behaviour focussed around routines and rituals. Children with OCD reported more compulsions and obsessions than children with ASD; both groups reported more compulsions and obsessions than a typically developing comparison group. Types of compulsions and obsessions tended to be less sophisticated in children with ASD than those with OCD. Sameness behaviour was more prevalent in younger children with OCD, but for children with ASD, age was not significantly related to sameness behaviour, repetitive movements, compulsions, or obsessions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Repetitive behaviour is a non-specific symptom, which has historically been considered as a marker of psychopathology (Lewis & Bodfish, 1998). The term repetitive behaviour is used to refer to a wide range of behaviours that are undertaken often, in an invariant manner, and are inappropriate or odd (Turner, 1997). Such behaviour is observed in a range of psychological disorders and medical conditions (Lewis & Bodfish, 1998; Turner, 1997), with subclinical levels reported in the normal population, most commonly in young children (Evans et al., 1997; Zohar & Felz, 2001). Research into the underlying biology of repetitive behaviour has centred on neutransmitter functions, predominantly serotonin and dopamine. This research is in its infancy, and is marked by inconsistencies, but suggests that the same neural structures and chemistry are likely to underlie repetitive behaviour in a range of disorders (Militerni, Bravaccio, Faclo, Fico, & Palermo, 2002).
This study focuses on two conditions in which repetitive behaviour is a core symptom, Autism Spectrum Disorders and Obsessive Compulsive Disorder (OCD), with a view to assessing similarities and differences in repetitive behaviour to each in these disorders. This comparison is intended to provide information regarding the specificity of particular forms of repetitive behaviour in each of these disorders and, more generally, to further our understanding of this important symptom.
Autism and Asperger syndrome (AS) are part of a group of Pervasive Developmental Disorders. Repetitive behaviour has been considered a core component of these disorders since the earliest conceptions (Kanner, 1943; Asperger, 1991), and continues to be included in current diagnostic criteria, (Diagnostic and Statistical Manual of Mental Disorders Fourth Edition Text Revision (DSM IV), American Psychiatric Association, 2000). A wide range of repetitive behaviour has been observed in children with autism and AS including repetitive motor mannerisms, an obsessive desire for sameness, negative reactions to change, and a narrow range of interests that are pursued in an obsessional manner (Smith, Magyar, & Arnold-Saritepe, 2002). The behaviours appear to change in presentation over time, with a recent study finding that younger children with autism (aged 2–4 years) engaged in more motor and sensory repetitive behaviours while older children (aged 7–11 years) engaged in more complex behaviours (Militerni et al., 2002). Another recent study reported that although age was related to improvements in the social and communication domain, respectively, there were fewer improvements in the repetitive behaviour domain (Fecteau, Mottron, Berthiaume, & Burack, 2003). These behaviours do not occur exclusively in Autism Spectrum Disorders, but the co-occurrence of a range of repetitive behaviours in these disorders suggests that these behaviours form a class (Lewis & Bodfish, 1998). Higher rates of repetitive behaviour have been demonstrated to differentiate individuals with autism or AS from individuals with a variety of other conditions (Bodfish, Symons, Parker, & Lewis, 2000; Prior & Macmillan, 1973; Rojahn, Matson, Lott, Esbensen, & Smalls, 2001; Turner, 1997). Individuals with AS, autism, and Pervasive Developmental Disorder (Not Otherwise Specified) (PDD (NOS)) vary predominantly in symptom severity, and this in turn is related to intelligence level, (for example see Manjiviona & Prior, 1999; for review see Dickerson Mayes, & Calhoun, 2003; Prior et al., 1998), making it reasonable to combine children with AS, autism, and PDD (NOS) of comparable intelligence for the purpose of research. The term Autism Spectrum Disorders (ASD) will be used henceforth to refer to AS, autism, and PDD (NOS).
Repetitive behaviour, in the form of obsessions and compulsions, is a defining component of OCD, a disorder that is increasingly being recognised in children and adolescents (Robinson, 1998). The disorder appears to have a bimodal pattern of onset, with the first peak occurring around puberty, and the second occurring in early adulthood (Zohar, 1999). Age of onset has been examined retrospectively, with around one third of adults reporting that their symptoms commenced prior to 15 years of age (Pauls, Alsobrook, Goodman, Rasmussen, & Leckman, 1995). The generally accepted view is that obsessions are intrusive repetitive thoughts that trigger anxiety (Bolton, 1996). Individuals often feel compelled to perform a ritual or a compulsion, which may be temporarily relieve the anxiety (DSM IV). However, some children have compulsions in the absence of clear obsessions and most report more compulsions than obsessions, with few reporting obsessions alone (Shafran, 1998). Several authors have suggested that compulsive behaviour may initially occur for a variety of reasons, for example as a result of a neurological deficit, and that obsessions may develop later as an individual attempts to make sense of their otherwise senseless repetitive behaviour (Bolton, 1996; Robinson, 1998; Schultz, Evans, & Wolff, 1999). Research has indicated that OCD is associated with other forms of repetitive behaviour, with approximately one third of children and adolescents with OCD also meeting the criteria for a tic disorder (Riddle, 1998). To the author’s knowledge, comorbidity with other forms of repetitive behaviour, such as those typically observed in children with ASD, has not been evaluated.
The similarities in the repetitive behaviour in ASD and OCD mean that at times careful assessment is required to assist with differential diagnosis (for example see King & Scahill, 1999; Leckman et al., 1999). Another issue that has received some attention in the literature is whether secondary OCD can or should be diagnosed in individuals with ASD (for example see Reaven & Hepburn, 2003; Towbin, 2003). The DSM IV suggests that repetitive behaviour is a source of pleasure in ASD, but a source of anxiety in OCD; it promotes consideration of social and communication impairments when considering differential diagnosis, but does not provide any guidance in relation to secondary diagnosis.
Evaluation of the similarities and differences of repetitive behaviour between ASD and OCD is likely to have been hampered by several factors, including the use of different terminology. For example, children with ASD are often described as being ‘obsessed’ with a particular area of knowledge, but this differs from the obsessions in OCD in that it is enjoyed and does not appear to provoke anxiety (Szatmari, 1998). It is possible that children with ASD pursue their circumscribed interests in an obsessional manner as a response to anxiety, however the language impairments and difficulties with introspection in these children make it difficult to assess this. These factors also make it difficult to assess whether children with ASD experience their repetitive behaviour as foreign and unwanted (or ‘ego-dystonic’), a feature which is considered to be a defining component of OCD (American Academy of Child and Adolescent Psychiatry, 1998; King & Scahill, 1999).
To the author’s knowledge only one study has sought to compare repetitive behaviour in ASD and OCD. McDougle et al. (1995) administered the Yale Brown Obsessive Compulsive Scale to find that adults with ASD reported more compulsions than obsessions, and generally reported less sophisticated obsessions and compulsions than those with OCD. The study relied heavily on parental report as the majority of individuals with ASD had an intellectual disability, and a significant proportion were mute. Further, the discrepancy in intelligence between the groups may have exaggerated the differences between the two disorders. In addition, no measure of the repetitive behaviours typically observed in individuals with ASD was included, therefore limiting the comprehensiveness of the assessment.
The underlying causes of repetitive behaviour are unclear, although arousal modulation is typically suggested for ASD, and anxiety for OCD (see Bolton, 1996; Turner, 1997). Impairments in executive functioning have also been suggested as a causal factor, with impairments demonstrated in both ASD and OCD samples. The children included in this study also undertook some measures designed to assess executive functioning and parents completed a questionnaire regarding this domain. These findings are summarised briefly in the results section, but will be reported in detail in a subsequent paper. A review of the neurological, genetic and biological literature reveals other similarities between the two disorders. Volkmar, Lord, Bailey, Schultz, and Klin (2004) reviewed the relevant literature on ASD while Kirkby (2003) provided a comprehensive summary of the recent research in OCD, hence findings will not be discussed further here.
To summarise, some similarities in repetitive behaviour are apparent in childhood OCD and ASD, such that differential diagnosis may be challenging and secondary diagnosis of OCD for individuals with ASD is an unresolved issue. To date, a comparison of repetitive behaviour in children with the two disorders has not been undertaken.
Method
Participants
Participants were 54 children and adolescents aged 7–16 years. All of the participants will be referred to as children henceforth, for the sake of brevity. The ASD group consisted of 19 children (16 males, 3 females), with a mean age of 11 years (SD = 2.42). The majority of these children had a diagnosis of AS (n = 15), 2 had a diagnosis of Autistic Disorder, and 1 had a diagnosis of Pervasive Developmental Disorder (Not Otherwise Specified). The majority were not medicated at the time of the study, however 3 children were taking Dexamphetamine, and 2 were taking Ritalin. Most of the children in this group (n = 15) were diagnosed by an experienced multidisciplinary assessment team at the Royal Children’s Hospital, consisting of a paediatrician, psychologist, and speech pathologist, according to DSM IV criteria. The remaining children with ASD (n = 4) responded to advertisements in relevant newsletters and had been diagnosed by experienced psychiatrists and psychologists according to DSM IV criteria. The OCD group consisted of 17 children (8 males, 9 females), with a mean age of 12 years (SD = 2.17). At the time of the study four children in the OCD group were taking Selective Serotonin Reuptake Inhibitors and two parents indicated that their child was taking medication but did not provide further details. The majority of children in this group were also receiving some form of psychological therapy (n = 15), compared with 4 children in the ASD group. Children with OCD were referred by clinicians in the Royal Children’s Hospital network (n = 7), as well as private psychiatrists and psychologists (n = 8). Two families responded to advertisements in relevant newsletters. Again, experienced professionals had diagnosed these children, according to DSM IV criteria. For both children with ASD and OCD diagnoses were based on a clinical interview with children and parents and a range of other findings, such as language and cognitive tests. Standardised diagnostic tools were not typically used as part of this process.
The typically developing, or control group, consisted of 18 children (6 males, 12 females) with a mean age of 12 years (SD = 2.94), none of whom were receiving psychological or pharmachological treatment. Ten typically developing children were recruited from a Catholic Primary School in north west metropolitan Victoria. The school was culturally diverse and consisted of a high proportion of children for whom English was a second language. A convenience sample of eight children aged between 12 and 16 years was recruited through families known to the researcher.
Exclusion criteria from the study were presence of a comorbid neurological disorder, such as Tourette syndrome or a Tic Disorder, a comorbid Intellectual Disability or Language Disorder, or a comorbid Axis 1 disorder, such as another anxiety disorder or depression. Strategies for ensuring that the participants did not have a comorbid disorder included ensuring that referrers were aware of the selection criteria, including items regarding comorbid disorders on an information sheet completed by parents, using the results of cognitive tests to eliminate any children with an Intellectual Disability or Language Disorder, and reviewing children’s files.
Measures
Parents completed an information sheet of demographic information that included their child’s diagnosis, medication, known comorbid psychological and neurological conditions, and family psychiatric history.
Repetitive behaviour measures
Measures were selected with the intention to provide a thorough assessment of the broad range of repetitive behaviour observed in children with ASD and OCD. The Repetitive Behaviour Questionnaire (RBQ) was developed by Turner (1995) to assess repetitive behaviours in ASD. It is a comprehensive parent or teacher rated questionnaire that allows the assessor to calculate scale scores for repetitive language, sameness behaviour, and repetitive movements, as well as a total repetitive behaviour score. Information regarding the validity and reliability of this scale has not been published, but can be found in Turner’s thesis (Turner, 1995). As a complement to the RBQ, the Children’s Yale Brown Obsessive-Compulsive Scale (CY-BOCS) was chosen (Scahill et al., 1997). The initial section, which contains two comprehensive symptom checklists, one for obsessions, and one for compulsions across a range of behaviours, was administered.
Intelligence
The children were administered a short form of the WISC III consisting of the Block Design, Similarities, Vocabulary, and Coding subtests. Verbal and Performance intelligence (VIQ and PIQ) were estimated using the procedure outlined by Sattler (1992). If a child had been assessed with the WISC III in the past 2 years, parents completed a release of information consent form and the researcher obtained the results from the relevant psychologist.
Procedure
Informed consent was obtained from parents and assent was obtained from children. Parents completed the demographic information sheet, RBQ, and a questionnaire measure of executive functioning. The principal researcher (FZ) completed all of the assessments. The short form of the WISC III was administered first, followed by the executive functioning tests. The CY-BOCS was then administered. Whether or not this was administered with the child alone, with a parent present, or with a parent only, was dependent upon the family’s preference, or on clinical judgment based on the child’s developmental level and language skills. Where administration was conducted with either the child or the parent individually, information was also obtained from the other informant and was integrated into the results. The total time required to complete these measures varied significantly between participants and their families according to their age, ability to sustain their attention to the tasks, and the style in which they shared information. With most children the total time was around 2 h but ranged from approximately an hour and a half to 3 h.
Results
Given the small sample sizes in this study, effect sizes are presented in addition to significance tests. Effect sizes (ES) were calculated using Cohen’s (1988) formula: for t tests ES = d/2 where d = M 1−M 2/σ (p. 276), for F tests ES = √ [η2/(1−η2)] (p. 284). ‘Small’ effect size is 0.10, ‘medium’ is 0.25, and ‘large’ is 0.40 (Cohen, 1988). Initial data screening revealed that the results were not altered when the two children with a diagnosis of Autistic disorder and the child with a diagnosis of PDD (NOS) were excluded from the sample; therefore these children were retained as part of the ASD group. Table 1 contains descriptive characteristics for each of the groups. Because of concerns about the distribution of these scores non-parametric tests were used; these confirmed that the three groups did not differ in median age, VIQ or PIQ.
Repetitive Behaviour Measures
Table 2 documents the results of the RBQ. Although it was reported to occur at extremely low levels, repetitive language was comparable in the ASD and OCD groups, t (34) = 0.06, P = 0.95, ES = 0.02. Repetitive language was not apparent in the control group. ANOVAs for sameness behaviour, repetitive movements, and total repetitive behaviour revealed a significant difference between the groups, with post hoc tests revealing that the two clinical groups showed significantly higher levels of repetitive behaviour than the control group, P < 0.01. As there was clearly a floor effect in the control group, and because similarities and differences between the two clinical groups were the main focus of the study, t-tests were used to assess for differences between the ASD and OCD group. Independent samples t-tests revealed no significant difference between the clinical groups for total repetitive behaviour, (t (34) = 0.42, P = 0.68, ES = 0.02), sameness behaviour, (t (34) = 1.21, P = 0.23, ES = 0.21), or repetitive movements, (t (34) = −0.10, P = 0.92, ES = 0.07).
Items from the RBQ were further categorised by the various types of repetitive behaviour they reflect. The results are presented in Fig. 1. Children with ASD and OCD were rated similarly on most of the scales, with children with OCD rating higher on routines and rituals.

Variations in type of repetitive behaviour in children with ASD and OCD
Sameness behaviour occurred at significantly higher rates in younger children with OCD compared to older children with the disorder (r (17) = −0.57, P = 0.02), but there was no significant relationship between repetitive movements and age. Age was not significantly related to sameness behaviour or repetitive movements in children with ASD.
The majority of children with ASD completed the CY-BOCS interview with their parents (68.4%), usually by choice, compared with 29.4% of children with OCD and 11.1% of children in the typically developing group. Six children in the ASD group and two children in the control group did not complete the CY-BOCS with their parents. The group of children whose parents completed the CY-BOCS alone consisted of younger children (M = 8.50 years, SD = 1.16) who, having completed all of the previous tests, were eager to have a break and could not be persuaded to participate in the interview. In these circumstances information regarding obsessions and compulsions was obtained briefly from the child either before or after their parent/s completed the CY-BOCS interview. Data screening indicated that these particular children did not differ significantly in VIQ or PIQ, nor in the number of obsessions and compulsions reported during the CY-BOCS interview. Hence, these children were included in all subsequent analyses.
Table 2 presents the mean number of obsessions and compulsions endorsed by children with ASD and OCD. Again, there was a floor effect in the control group with ANOVAs revealing significant differences between each of the clinical groups and the control group, P < 0.05. However, in both cases the homogeneity of variance assumption was violated, P < 0.01. Subsequent analysis confirmed that children with OCD reported significantly more compulsions, t (34) = 3.97, P = 0.00, ES = 0.69 and obsessions, t (34) = 3.48, P = 0.00, ES = 0.60, than children with ASD.
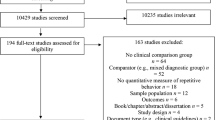
The proportion of children endorsing each type of compulsion is presented in Fig. 2. It is apparent that children with OCD were more likely than children with ASD to endorse compulsions in all areas, with the exception of those involving another person, and ordering compulsions, where the two groups were comparable.

Percentage of children with ASD and OCD endorsing various compulsions
Figure 3 presents the percentage of children in each group who endorsed each type of obsession. Children with OCD endorsed more obsessions than children with ASD for most obsession types. The number of children endorsing religious obsessions was comparable in the two groups, while children with ASD endorsed more miscellaneous obsessions than children with OCD.

Percentage of children with ASD and OCD endorsing various obsessions
Older children with OCD were significantly more likely to report obsessions than younger children with the disorder, (r (17) = 0.55, P = 0.02). Age was not significantly related to the number of compulsions and obsessions reported by children with ASD. In the ASD group the mean number of obsessions and compulsions were moderately related (r (19) = 0.50, P = 0.03), with a strong association in the OCD group (r (17) = 0.71, P = 0.00). Table 3 shows the relationship between the number of obsessions and compulsions reported during the CY-BOCS interview and the repetitive movement and sameness scores obtained from the RBQ. Repetitive language was not included due to very low rates of this behaviour being reported in both groups. Higher rates of repetitive movements were related to a greater number of obsessions in children with ASD, but no other significant relationships were apparent. Results from the typically developing group are not reported due to the generally low rates of repetitive behaviour in this group.
A number of executive functioning tests were also administered and the relationship between these results and repetitive behaviour was examined. Greater executive function impairment, as rated by parents, was related to higher rates of repetitive behaviour in the ASD and control groups, but not for the OCD group. Detailed results will be reported in a subsequent paper.
Discussion
The results of the RBQ indicate that children with ASD and OCD engage in similar levels of sameness behaviours and repetitive movements. The results from the CY-BOCS however, suggest differences in the type of behaviour observed in the two disorders. Children with OCD reported more compulsions and obsessions than children with ASD, who in turn reported more compulsions and obsessions than typically developing children. Consideration of the type of compulsions and obsessions in each disorder suggests that the compulsions in ASD tended to be less sophisticated. These results are reasonably consistent with those reported by McDougle et al. (1995) who compared the CY-BOCS results of adults with ASD and OCD.
Developmentally, sameness behaviour was more prevalent in younger children with OCD, with older children with the disorder reporting more obsessions. In children with ASD age was not significantly related to sameness behaviour, repetitive movements, obsessions or compulsions. The discrepancy between Militerni et al. (2002) finding of higher rates of motor and sensory repetitive behaviour in younger children with ASD and these results is likely to reflect the older age group included in the present study. The results of the current study and the findings reported by Fecteau et al. (2003) suggest that repetitive behaviours persist throughout development in children with ASD, although the form of these behaviours may change. Finally, the various types of repetitive behaviour assessed were not correlated in children with ASD or OCD.
Implications for Assessment and Treatment
The results of this study highlight the challenges of assessing developmental disorders and suggest similarities in the content of repetitive behaviour in children with OCD and ASD. ASD can be an important differential diagnosis when diagnosing OCD and, contrary to the suggestions of some authors (for example see Presta et al., 2003), the results of the current study suggest that differentiating between ASD and OCD based on the characteristics of repetitive behaviour is likely to be problematic. Differential diagnosis is most likely to be difficult in high functioning individuals, who do not exhibit such severe social and communication impairments. These impairments are not part of the diagnostic picture in OCD and are therefore useful in ruling out ASD (Chang & Piacentini, 2002).
The question of whether children with ASD should be diagnosed with secondary OCD has received an increasing amount of attention in the literature. A secondary diagnosis would seem to require a clinical judgement that the repetitive behaviour observed is over and above that which is expected in ASD. This would be extremely difficult given that there has been no clear consensus about the level of repetitive behaviour typically observed in ASD. Further a diagnosis of OCD requires the repetitive behaviour to be ego-dystonic and distressing, factors that are difficult to assess in children with ASD. Since a diagnosis of ASD signals the potential need to intervene with repetitive behaviours, a secondary diagnosis of OCD may add little and only serve to confuse the child and parents.
Limitations and Directions for Future Research
The study demonstrates some of the difficulties of assessing repetitive behaviour. The discrepancy between the findings from the CY-BOCS and the RBQ may, in part, be accounted for by the different presentation of these measures; semi-structured interview as opposed to questionnaire. Many parents spontaneously reported repetitive behaviour of their own during the testing, the presence of which may impact on the way they interpreted and reported similar behaviour in their children. More importantly, the CY-BOCS is not diagnostic, but rather provides a method of assessing symptom content and severity after a diagnosis of OCD has been established (Scahill et al., 1997). Caution is therefore required when interpreting reports of obsessions and compulsions from children without a diagnosis of OCD.
The present study suggests similarities in the content of repetitive behaviour in ASD and OCD, but does not provide information regarding the quality of repetitive behaviour in each of the disorders. Understanding the quality of the behaviour in each of these disorders requires direct observation. Functional analysis would be helpful in determining whether the behaviour in ASD and OCD serves similar or different functions. The present study indicates the type of repetitive behaviour observed varies with age in childhood OCD. Longitudinal analysis would enable consideration of such age effects and could inform our understanding of the way in which these disorders, and repetitive behaviour more generally, develop. Addressing the question of underlying processes also requires researchers to design measures that adequately assess factors such as ego-dystonicity, resistance, distress and impairment. Measures that are suitable for assessing repetitive behaviour in a range of disorders are likely to allow for more productive comparisons of similarities and differences between diagnostic categories.
In addition to the limitations discussed previously the small sample size affected the power of statistical analyses and limits the extent to which the results can be generalised. Further limitations include the broad range of severity that was apparent in both the ASD and OCD groups and the lack of a structured diagnostic interview. The inclusion of such an interview in future research should allow for exploration of any additional diagnoses, and may go some way towards clarifying the relationship of ASD and OCD to other disorders where clinicians have observed similarities, such as Non Verbal Learning Disorder (American Academy of Child and Adolescent Psychiatry, 1998).
In conclusion, sameness behaviour, repetitive movements, compulsions and obsessions were more prevalent in children with OCD and ASD than in typically developing children. Future research should consider the full range of repetitive behaviour in these disorders using a range of methods. Further exploration of the way in which a child’s development affects the expression of repetitive behaviour in ASD and OCD also appears warranted.
References
American Academy of Child, Adolescent Psychiatry (1998). Practice parameters for the assessment and treatment of children and adolescents with Obsessive Compulsive disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 37(10S), 27S–45S.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders. (4th ed. revised). Washington, DC: Author.
Asperger, H. (1991). Autistic psychopathy in childhood. In U. Frith, (Ed. and trans.), Autism and Asperger Syndrome. (pp. 37–92). Cambridge: Cambridge University Press. (Original work published 1944)
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30(3), 237–243.
Bolton, D. (1996). Annotation: Developmental issues in obsessive compulsive disorder. Journal of Child Psychology and Psychiatry, 37(2), 131–137.
Chang, S., & Piacentini, J. (2002). Childhood Obsessive-Compulsive and Tic disorders. In D. T. Marsh, & M. A. Fristad, (Eds), Handbook of Serious Emotional Disturbance in Children and Adolescents. (pp. 175–203). New York: John Wiley and Sons.
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences. San Diego, CA: Academic Press.
Dickerson Mayes, S., & Calhoun, S. L. (2003). Relationship between Asperger’s syndrome and high functioning Autism. In M. Prior, (Ed), Learning and Behavior Problems in Asperger Syndrome. (pp. 15–35). New York: The Guilford Press.
Evans, D. W., Leckman, J. F., Carter, A., Reznick, J. S., Henshaw, D., King, R. A., & Pauls, D. (1997). Ritual, habit, and perfectionism: The prevalence and development of compulsive-like behavior in normal young children. Child Development, 68(1), 58–68.
Fecteau, S., Mottron, L., Berthiaume, C., & Burack, J. A. (2003). Developmental changes of autistic symptoms. Autism, 7(3), 255–268.
Kanner, L. (1943). Autistic distrubances of affective contact. Nervous Child, 2, 217–250
King, R., & Scahill, L. (1999). The assessment and coordination of treatment of children and adolescents with OCD. Child and Adolescent Clinics of North America, 8(3), 577–597.
Kirkby, K. C. (2003). Obsessive compulsive disorder: Towards better understanding and outcomes. Current Opinion in Psychiatry, 16(1), 49–55.
Leckman, J. F., King, R. A., Scahill, L., Findley, D., Ort, S. I., & Cohen, D. J. (1999) Yale Approach to Assessment and Treatment. In J. F. Leckman, & D. J. Cohen, (Eds), Tourette’s Syndome – Tics, Obsessions and Compulsions Developmental Psychopathology and Clinical Care. (pp. 285–309). New York: Wiley.
Lewis, M., & Bodfish, J. W. (1998). Repetitive behavior disorders in autism. Mental Retardation and Developmental Disabilities Research Reviews, 4, 80–89.
Manjiviona, J., & Prior, M. (1999). Neuropsychological profiles of children with Asperger syndrome and Autism. Autism, 3(4), 327–356.
McDougle, C. J., Kresch, L. E., Goodman, W. K., Naylor, S. T., Volkmar, F. R., Cohen, D. J., & Price, L. H. (1995). A case-controlled study of repetitive thoughts and behavior in adults with autistic disorder and obsessive-compulsive disorder. American Journal of Psychiatry, 152(5), 772–777.
Militerni, R., Bravaccio, C., Faclo, C., Fico, C., & Palermo, M. T. (2002). Repetitive behaviours in autistic disorder. European Child and Adolescent Psychiatry, 11, 210–218.
Pauls, D., Alsobrook, J., Goodman, W., Rasmussen, S., & Leckman, J. (1995). A family study of obsessive compulsive disorder. American Journal of Psychiatry, 152, 76–84.
Presta, S., Marazziti, D., Dell’Osso, L., Pfanner, C., Pfanner, P., Marcheschi, M., Masi, G., Muratori, F., Mucci, M., Millepiedi, S., & Cassano, G. B. (2003). Obsessive-compulsive disorder in children and adolescence. Psychopathology, 36, 55–64.
Prior, M., Eisenmajer, R. Leekam, S., Wing, L., Gould, J., Ong, B., & Dowe, D. (1998). Are there subgroups within the autism spectrum? A cluster analysis of a group of children with autistic spectrum disorders. Journal of Child Psychology and Psychiatry, 39(6), 893–902.
Prior, M., & Macmillan, M. B. (1973). Maintenance of sameness behavior in children with Kanner’s syndrome. Journal of Autism and Childhood Schizophrenia, 3(2), 154–167.
Reaven, J., & Hepburn, S. (2003). Cognitive behavioural treatment of obsessive-compulsive disorder in a child with Asperger syndrome. Autism, 7(2), 145–164.
Riddle, M. (1998). Obsessive-compulsive disorder in children and adolescents. The British Journal of Psychiatry, 35(Suppl.), 91–96.
Robinson, R. (1998). Obsessive compulsive disorder in children and adolescents. Bulletin of the Menninger Clinic, 62(4 Suppl. A), A49–A64.
Rojahn, J., Matson, J. L., Lott, D., Esbensen, A. J., & Smalls, Y. (2001). The behavior problems inventory: An instrument for the assessment of self-injury, stereotyped behaviour, and aggression/destruction in individuals with developmental disabilities. Journal of Autism and Developmental Disorders, 31(6), 577–588.
Sattler, J. M. (1992). Assessment of Children. (3rd ed.) San Diego: Jerome M. Sattler, Publisher, Inc.
Scahill, L., Riddle, M., McSwiggin-Hardin, M., Ort, S., King, R., Goodman, W., Cicchetti, D., & Leckman, J. (1997). Children’s Yale-Brown obsessive compulsive scale: Reliability and validity. Journal of the American Academy of Child and Adolescent Psychiatry, 36(6), 844–852.
Schultz, R. T., Evans, D. W., & Wolff, M. (1999). Neuropsychological models of childhood obsessive-compulsive disorder. Child and Adolescent Psychiatric Clinics of North America, 8(3), 513–531.
Shafran, R. (1998). Childhood obsessive-compulsive disorder. In P. J. Graham, (Ed), Cognitive-behavioural therapy for children and families. (pp. 45–73). New York: Cambridge University Press.
Smith, T, Magyar, C., & Arnold-Saritepe, A. (2002). Autism Spectrum Disorder. In D.T. Marsh, & M.A. Fristad, (Eds) Handbook of Serious Emotional Disturbance in Children and Adolescents. (pp. 131–148). New York: Wiley.
Szatmari, P. (1998). Differential diagnosis of Asperger disorder. In E. Schopler, G.B. Mesibov, & L.J. Kunce, (Eds) Asperger Syndrome or High Functioning Autism? Current Issues in Autism. (pp. 61–74). New York: Plenum Press.
Towbin, K. E. (2003). Strategies for pharmacological treatment of high functioning autism and Asperger syndrome. Child and Adolescent Psychiatric Clinics of North America, 12, 23–45.
Turner, M. (1995). Repetitive behaviour and cognitive functioning in autism. Unpublished Ph. D. Thesis, University of Cambridge.
Turner, M. (1997). Towards an Executive Dysfunction Account of Repetitive Behavior in Autism. In J. Russell, (Ed), Autism as an Executive Disorder. (pp. 57–100). Oxford: Oxford University Press.
Volkmar, F. R., Lord, C., Bailey, A., Schultz, R. T., & Klin, A. (2004). Autism and pervasive developmental disorders. Journal of Child Psychology and Psychiatry, 45(1), 135–170.
Zohar, A. H. (1999). The epidemiology of obsessive-compulsive disorder in children and adolescents. Child and Adolescent Psychiatric Clinics of North America, 8(3), 445–460.
Zohar, A. H., & Felz, L. (2001). Ritualistic behavior in young children. Journal of Abnormal Child Psychology, 29(2), 121–128.
Acknowledgments
We gratefully acknowledge the contribution of Dr Janine Manjiviona, Margaret Richardson, Kathleen Allen, and Jasmin Scanlan from the Royal Children’s Hospital. We also thank Dr Howard Cooper and Barbara Jones for their assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zandt, F., Prior, M. & Kyrios, M. Repetitive Behaviour in Children with High Functioning Autism and Obsessive Compulsive Disorder. J Autism Dev Disord 37, 251–259 (2007). https://doi.org/10.1007/s10803-006-0158-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-006-0158-2