
Abstract
Inhibition is a key neurocognitive domain in ADHD that is commonly assessed with the stop-signal task. The stop-signal involves both “go” and “stop” trials; previous research indicates that response times are reliably slower to “go” trials during tasks with vs. without intermittent “stop” trials. However, it is unclear whether this pattern reflects deliberate slowing to maximize inhibitory success (performance adjustment hypothesis) and/or disrupted bottom-up information processing due to increased cognitive demands (dual-task hypothesis). Given the centrality of “go” responding for estimating children’s inhibitory speed, finding that children with ADHD slow differently –or for different reasons– has the potential to inform cognitive and self-regulatory theories of ADHD. The current study used a carefully-controlled experimental design to assess the mechanisms underlying stop signal-related slowing in ADHD. Children ages 8-13 with (n = 81) and without ADHD (n = 63) completed the stop-signal task and a control task that differed only in the presence/absence of “stop” trials. Using drift-diffusion modeling, Bayesian repeated-measures ANOVAs revealed a pattern consistent with the performance adjustment hypothesis, such that children adopted more cautious response strategies (BF10 = 6221.78; d = 0.38) but did not show changes in processing speed (BF01 = 3.08; d = 0.12) or encoding/motor speed (BF01 = 5.73; d = 0.07) when inhibition demands were introduced. Importantly, the ADHD/Non-ADHD groups showed equivalent effects of intermittent “stop” trials (BF01 = 4.30-5.56). These findings suggest intact self-regulation/performance monitoring in the context of adapting to increased inhibitory demands in ADHD, which has important implications for the continued isolation of potential mechanisms associated with ADHD symptoms and impairment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Attention-deficit/hyperactivity disorder (ADHD) is associated with deficits on tasks intended to assess numerous neurocognitive domains (Willcutt et al. 2005). Inhibitory control has long been considered a central neurocognitive process in ADHD, with ADHD groups typically showing medium-sized impairments relative to their typically-developing peers on common inhibition paradigms (Alderson et al. 2007; Lijffijt et al. 2005; Lipszyc and Schachar 2010; Wright et al. 2014). Though only a subset of children with ADHD may exhibit inhibitory control deficits (Fair et al. 2012; Kofler et al. 2018; Nigg et al. 2005), behavioral inhibition remains key to etiologic theories of ADHD (Barkley 1997; Sonuga-Barke et al. 2010), and may relate cross-sectionally to clinically-relevant domains of impairment, including parent-child relationship quality (Kofler et al. 2017) and social functioning (Bunford et al. 2015; cf. Tseng and Gau 2013). Recent evidence also suggests that performance on inhibition tasks may predict medication treatment response (see Molitor and Langberg 2017) and be a mediator of stimulant treatment response (Hawk et al. in press), highlighting its continued importance for understanding ADHD etiology and treatment.
Inhibitory Control and Response Speed
Inhibitory control refers to a set of interrelated cognitive processes that underlie the ability to withhold (action restraint) or stop (action cancellation) an on-going response (Logan et al. 1984) and are supported by neuroanatomical networks involving bilateral frontal, right superior temporal and left inferior occipital gyri, right thalamic, and mid-brain structures (Cortese et al. 2012). The stop-signal task (Logan et al. 1984) is arguably the most widely-used test of inhibitory control. It requires participants to respond quickly to “go” stimuli and to withhold responding when the go stimulus is followed by a “stop” cue (typically an auditory tone). Thus, participants have to balance two competing task goals (Verbruggen and Logan 2009). Importantly for the current study, a large body of research shows that reaction times (RT) to go trials are reliably slower during tasks that present intermittent stop signals than during otherwise identical tasks without these stop trials for both children with ADHD (e.g., Alderson et al. 2008) and neurotypical samples (e.g., Rieger and Gauggel 1999; Verbruggen and Logan 2009).
To date, little attention has been paid to why this slowing occurs and whether the mechanisms driving slowing are different for children with and without ADHD. Elucidating the processes driving stop-signal-related slowing has the potential to inform cognitive and self-regulatory processes in ADHD, with implications for etiological models of ADHD that have been developed in part on data from the stop-signal task. It also has methodological implications for using the stop-signal task with different diagnostic groups. Perhaps counterintuitively, the speed of children’s responses to non-inhibitory go trials is critical for estimating the (unobservable) speed of children’s stop processes (Logan et al. 1984), which is used frequently as evidence for inhibition deficits in ADHD (Alderson et al. 2007; Lipszyc and Schachar 2010). If stop-signal-related slowing is induced by different mechanisms across diagnostic groups, it would raise significant concerns about the interpretation of go responses in the stop signal task, which in turn brings into question the validity of the task’s primary outcome variable, Stop Signal Reaction Time.Footnote 1
Reaction Time Slowing: Dual-task Requirement Hypothesis
There are two primary processes by which RTs to go trials can become slowed when intermittent stop signals are present. As explicated by Verbruggen and Logan (2009), introducing a stop signal to a choice discrimination task requires individuals to maintain two task goals in mind and attend to both auditory and visual information. It is suspected that having to maintain two competing task goals (“go” and “stop”) increases working memory and divided attention demands (Garon et al. 2008); these increased cognitive demands may disrupt efficient bottom-up processing of task stimuli, thereby slowing processing speed and responses to go stimuli – what Verbruggen and Logan (2009) refer to as the dual-task requirement hypothesis. As argued by Wiemers and Redick (2017; cf. Weigard and Huang-Pollock 2017), reduced working memory capacity limits an individual’s ability to maintain goal-relevant information in working memory during task completion, which in turn produces failures in cognitive control and slowed/variable processing of task stimuli.
Relevant to ADHD, the dual-task requirement hypothesis may be particularly appealing given replicated evidence that children with ADHD perform poorly on tasks of working memory (Kasper et al. 2012) and tasks requiring attention to dual tasks (Hutchinson et al. 2012; Hwang et al. 2010), as well as evidence for robust associations between working memory abilities and reaction time/processing speed in ADHD samples (Karalunas and Huang-Pollock 2013; Kofler et al. 2014; Raiker et al. 2018; Weigard and Huang-Pollock 2017). It therefore seems likely that the increased executive control demands evoked by the stop signal would differentially disrupt maintenance of competing task goals, resulting in impaired information processing efficiency for children with ADHD relative to non-ADHD children.
Reaction Time Slowing: Performance Adjustment Hypothesis
Slowed go RTs in the presence of intermittent stop trials may also be produced by intentional slowing to maximize the likelihood of correct inhibition and to maintain high accuracy. Evidence supporting this hypothesis includes demonstrations that participants become more cautious in their response to go trials after inhibition trials (Schachar et al. 2004; Verbruggen et al. 2008) and can proactively adjust their response style when stop signals are introduced (Verbruggen and Logan 2009). Thus, the performance adjustment hypothesis suggests that participants purposefully slow responses to go trials in an attempt to maximize performance on stop trials.Footnote 2 This speed-accuracy trade-off would result in slower go RTs due to a more cautious response style when a stop signal might occur, rather than due to impaired information processing resulting from increased cognitive demands.
Being able to adaptively shift one’s relative emphasis on speed versus accuracy in response to changing task demands is critical for successful self-regulation. In ADHD, apparent deficits across a variety of cognitive domains may be accounted for in part by deficits in basic self-regulatory processes that contribute to poor task performance, regardless of the specific domain assessed (Douglas 1999). Indeed, there is some evidence of ADHD/control group differences in key aspects of self-regulation, including post-error slowing (Balogh and Czobor 2016) and performance monitoring (e.g., Albrecht et al. 2008; Groen et al. 2008), though not all studies observe these differences (e.g., Groom et al. 2010; Van De Voorde et al. 2010). In regard to speed-accuracy tradeoffs specifically, it has been suggested that children with ADHD have difficulty adjusting their behavior in response to changing task instructions relative to their typically-developing peers (Mulder et al. 2010), but other work demonstrates that they can modulate their level of response caution as well as typically-developing children when reinforcement is introduced for speeded accuracy (Fosco et al. 2017).
To summarize, previous research seeking to quantify the nature and extent of ADHD-related self-regulation deficits is mixed. However, searching exclusively for diagnostic group deficits can limit our understanding of ADHD because identifying processes that remain intact in a disorder is also critical for advancing theory and developing targeted interventions (i.e., to ensure remediation is not directed at a process that is unimpaired). To date, work in this area has been limited by the use of null hypothesis testing, for which a lack of a group difference cannot be readily interpreted. The current study advances this area by using Bayesian methods that provide evidence both against and for the null hypothesis to improve our understanding of both impaired and non-impaired processes in children with ADHD.
Dual-Task versus Performance Adjustment Predictions
Both the dual-task and performance adjustment hypotheses predict slower RTs to go trials during tasks with intermittent stop trials. However, they make different predictions regarding the processes driving slower RTs, which can be computationally modeled using a diffusion model framework (Table 1). The drift diffusion model (DDM) is a well-validated model of simple decision making (Ratcliff and McKoon 2008). It integrates RT and accuracy data to decompose task performance into parameters representing processing speed (referred to as “drift rate”), degree of response caution (boundary separation), and processes unrelated to the decision process, such as time for stimulus encoding and response execution (non-decision time; Voss et al. 2013).
Within the DDM framework, the dual-task requirements hypothesis posits that the presence of stop signals increases working memory and/or divided attention demands, which in turn increases the latency of non-decisional processes (e.g., stimulus encoding and response execution) and slows the rate of processing speed. Conversely, the performance adjustment hypothesis predicts that participants will adopt a more cautious response strategy that involves increasing the quantity of information required to choose between response options, reflected by an increase in boundary separation (Verbruggen and Logan 2009).
In a study examining these hypotheses in a small college student sample (Verbruggen and Logan 2009), results were generally consistent with both hypotheses, albeit with stronger support for the hypothesis that slowed go responding during inhibition tasks was driven by participants proactively slowing in an effort to enhance accuracy. To our knowledge, no study to date has investigated these hypotheses in a clinical child sample, or investigated the extent to which intermittent stop trials differentially affect components of information processing in children with ADHD relative to their non-ADHD peers. Given the well-documented developmental findings that children experience weaker controlled attention at lower loads compared to adults (e.g., Cowan et al. 2006), we presumed this would translate to greater susceptibility to dual task interference in our child sample compared to previous adult samples.
Current Study
The current study extends previous work by examining the mechanisms and processes underlying the effects of intermittent stop trials on go RTs in the stop signal task among children with and without ADHD. Although several ADHD studies have assessed information processing within the drift diffusion framework during both stop signal tasks (e.g., Huang-Pollock et al. 2017; Karalunas et al. 2012; Karalunas and Huang-Pollock 2013) and no-tone tasks (Fosco et al. 2017), adequately testing whether children with ADHD show differential patterns of dual-task vs. performance adjustment effects requires that the same children complete both the stop-signal and an otherwise-identical no-tone task to evaluate how information processing parameters change when inhibitory demands are introduced.
Using a counterbalanced experimental design that included tasks with and without intermittent stop signals, we hypothesized that both ADHD and Non-ADHD groups would show slowed response times to go trials during the task with intermittent stop trials. As argued by Verbruggen and Logan (2009), support for the dual-task requirements hypothesis would include significant increases in non-decision time (i.e., slower non-decision time), significant decreases in drift rate (i.e., slower processing speed), and no change in boundary separation during the stop-signal relative to control task (Table 1). In contrast, support for the performance adjustment hypothesis would include significant increases in boundary separation and no changes in drift rate or non-decision time during the stop-signal relative to the control task (i.e., a more cautious response style but stable processing speed).
Evidence for differential effects of intermittent inhibition demands for children with ADHD would include significant group x task interactions for one or more of the drift diffusion parameters (response caution, drift rate, non-decision time), interpreted according to the performance adjustment and dual-task hypotheses outlined above. Given the replicated evidence that children with ADHD exhibit impairments on dual-task working memory tasks (e.g., Alderson et al. 2017; Willcutt et al. 2005), combined with inconsistent evidence regarding the extent to which these children show impaired performance adjustment/monitoring (e.g., Groom et al. 2010; Van De Voorde et al. 2010), we predicted that children with ADHD would exhibit slower processing speed when intermittent stop signals are present, indicating support for the dual-task requirements hypothesis. In contrast, we predicted that children without ADHD would show increased emphasis on accuracy over speed (higher response caution) but no significant change in information processing speed, consistent with previous work that has primarily supported the performance adjustment hypothesis in typically-developing samples (Verbruggen and Logan 2009).
Method
Participants
The sample included 144 children aged 8 to 13 years (M = 9.97, SD = 1.48; 116 boys, 28 girls) from two sites in the Southern United States. Participants were recruited through community resources (e.g., pediatricians, school system personnel, self-referral) to participate in a research study at a university-based research laboratory between 2010 and 2017. All families received no-cost psychoeducational evaluations for study participation. All parents and children gave informed consent/assent, and Institutional Review Board approval from Oklahoma State University and University of Virginia was obtained/maintained. Child race/ethnicity was representative of the recruitment regions, and included Caucasian non-Hispanic (81%), mixed racial/ethnic (8%), Native American (6%), Hispanic English-speaking (3%), and Asian (2%) backgrounds.
Group Assignment
All children and caregivers completed a comprehensive evaluation, regardless of recruitment reason, that included detailed, semi-structured clinical interviewing (K-SADS; Kaufman et al. 1997). The K-SADS (2013 Update) allows differential diagnosis according to symptom onset, course, duration, quantity, severity, and impairment in children and adolescents based on DSM-5 criteria (American Psychiatric Association [APA] 2013). K-SADS interviews were supplemented with parent and teacher broadband (Child Behavior Checklist/Teacher Report Form or Behavior Assessment System for Children-2; Achenbach and Rescorla 2001; Kamphaus and Reynolds 2007) and narrowband ADHD rating scales (Conners-3 or Child Symptom Inventory-IV; Conners 2008; Gadow and Sprafkin 2002). A psychoeducational report was provided to parents.
Eighty-one children met all of the following criteria and were included in the ADHD group (n = 81; 25% girls): (1) DSM-5 diagnosis of ADHD Combined (n = 43), Inattentive (n = 36), or Hyperactive/Impulsive Presentation (n = 1) by the directing clinical psychologist based on K-SADS; and (2) Borderline/clinical elevations on at least one parent and one teacher ADHD rating scale; and (3) current impairment based on parent report. All ADHD subtypes/presentations were eligible given the instability of ADHD subtypes (Lahey et al. 2005; Valo and Tannock 2010). Psychostimulants (Nprescribed = 24) were withheld ≥24 h for testing. To improve generalizability, children with comorbidities were included. Clinical consensus best estimate comorbidities included oppositional defiant (25%), specific learning (21%), anxiety (10%), and depressive (10%) disorders.
The Non-ADHD group (n = 63; 13% girls) included both neurotypical children and children with psychiatric disorders other than ADHD. Neurotypical children (n = 34; 54%) had typical developmental histories and did not meet criteria for any psychiatric disorder. Elevations on parent or teacher ratings were not exclusionary for the neurotypical group if follow-up interviewing suggested these elevations were not due to actual ADHD symptoms (e.g., developmentally-appropriate parent-child relational problems, recency effects such that endorsements did not reflect typical patterns of behavior). Children who met criteria for disorders other than ADHD (n = 29; 46%) were also included in the Non-ADHD group. These Non-ADHD disorders were included to control for comorbidities in the ADHD group, and included best estimate diagnoses of oppositional defiant (11%), specific learning (8%), anxiety (6%), and depressive (6%) disorders. Importantly, the ADHD and Non-ADHD clinical groups did not differ significantly in the proportion of children diagnosed with ODD (BF01 = 0.57) and learning disorders (BF01 = 1.92), and were statistically equivalent with regard to rates of anxiety (BF01 = 6.36) and depression (BF01 = 6.36). The Bayes Factor BF01 is an odds ratio indicating support for the null hypothesis that the groups are equivalent (H0) relative to the alternative hypothesis that the groups differ (H1; see Bayesian Analyses section below).
Children were excluded for gross neurological, sensory, or motor impairment, history of seizure disorder, psychosis, autism spectrum, or intellectual disability, or non-stimulant medications that could not be withheld for testing.
Procedures
The experimental tasks were administered as part of a larger battery that involved several sessions of approximately 3 h each. All tasks were successfully counterbalanced to minimize order effects which resulted in an equal probability of each order across diagnostic groups (χ2 = 0.12, p = .94). Performance was monitored at all times by the examiner, who was stationed just out of the child’s view to provide a structured setting while minimizing performance improvements associated with examiner demand characteristics (Gomez and Sanson 1994). All children received brief (2-3 min) breaks after each task, and preset longer (10-15 min) breaks after every 2-3 tasks to minimize fatigue.
Socioeconomic Status (SES) and Measured Intelligence (IQ)
Hollingshead (1975) SES was estimated based on caregiver(s)’ education and occupation. IQ was estimated using the Wechsler Intelligence Scales for Children, Fourth or Fifth Edition or Wechsler Abbreviated Scales of Intelligence, Second Edition (Wechsler 2014).
Tasks
Stop-signal
Task and administration instructions were identical to Alderson and colleagues (2008). Psychometric evidence includes high internal consistency, 3-week test-retest reliability (both = .72), and convergent validity with other inhibition tests (Soreni et al. 2009). Internal consistency of MRT across the four blocks in the current sample was α = .89.
Go-stimuli were displayed for 1000-ms as uppercase letters X and O positioned in the center of a computer screen (500-ms interstimulus interval; total trial duration = 1500-ms). Xs and Os appeared with equal frequency. A 1000-Hz auditory tone (stop-stimulus) was presented randomly on 25% of trials. Stop-signal delay – the latency between go- and stop-stimuli presentation – was initially set at 250-ms, and dynamically adjusted ±50-ms contingent on performance. The algorithm was designed to approximate successful inhibition on 50% of stop-trials. In the current study, inhibition success was 49.7%, 50.8%, 49.7%, and 50.8% across the four experimental blocks. Children completed two practice and four consecutive experimental blocks of 32 trials/block (8 stop-trials per block). Stop-signal performance data were reported for a subset of the current sample to examine conceptually unrelated hypotheses (Alderson et al. 2017; Kofler et al. 2017)
No-tone choice reaction time task
The choice reaction time task is identical to the stop signal task in every aspect except for the primary independent variable: All trials are go trials, as opposed to the stop-signal task where 25% of trials are stop trials. Administration instructions are identical to the No-Tone condition described by Alderson et al. (2008). All participants completed two practice blocks and four consecutive experimental blocks of 32 trials (total of 128 experimental trials). The experimental blocks required approximately 7.5 min to complete. Participants whose counterbalancing resulted in them completing the no-tone task after the stop-signal task were explicitly told to respond to all trials. Internal consistency for the no-tone MRT across the four blocks was high (α = .91).
Drift Diffusion Modeling
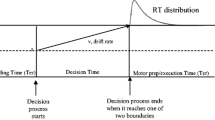
The drift diffusion model is a well-validated stochastic accumulator model of choice decision tasks (Ratcliff and McKoon 2008; Voss et al. 2013). It assumes that information accumulates continuously until there is sufficient evidence to make a decision. According to the diffusion model, a binary decision is represented by an upper and lower boundary reflecting the two response options. The decision process begins between the two response boundaries, and information is accumulated from the stimulus; each sample of information shifts the process towards one boundary or the other. A decision is made once the accumulated information reaches a boundary, at which point the response execution process begins.
Relevant to the current investigation, drift rate (v) refers to the speed of information accumulation; larger drift rate values indicate faster information accumulation. Boundary separation (a) refers to the quantity of information considered before a decision is executed and reflects one’s degree of response caution; higher boundary separation requires more information to be accumulated about the stimulus before a decision is made, and thus results in a higher chance of accuracy, albeit with a slower response (i.e., speed-accuracy trade-off). Lower boundary separation results in a faster response at the cost of reduced accuracy. Non-decision time (t0) captures aspects of reaction time performance unrelated to decision making, including stimulus encoding and skeletomotor response speed; higher non-decision time reflects slower encoding and/or motor speed, which are not separable in the diffusion model. Data were screened for anticipatory responses (RTs < 150 ms). The Kolmogorov-Smirnov (K-S) algorithm was implemented using fast-dm software v. 30.2 (Voss and Voss 2007) given its robustness to outliers, use of individual trial data to derive diffusion parameters, and evidence that it can provide excellent parameter recovery with as few as 20 trials per participant (Voss and Voss 2007). Drift rate, boundary separation, and non-decision time were estimated separately for the No-Tone and Stop-Signal tasks for each child. Model fit was acceptable for all participants for each task, all ps > .05.
Previous work utilizing diffusion modeling to examine go trial performance during inhibition tasks suggests that children with ADHD exhibit slower drift rate in most (Karalunas et al. 2012; Karalunas and Huang-Pollock 2013) but not all studies (Huang-Pollock et al. 2017). Group differences in non-decision time have been inconsistent, with reports of equivalent (Karalunas et al. 2012) or faster non-decision time for children with ADHD (Karalunas and Huang-Pollock 2013). Boundary separation is consistently similar across diagnostic groups (Karalunas et al. 2012; Karalunas and Huang-Pollock 2013). On a no-tone choice discrimination task, children with ADHD demonstrated slower drift rate but equivalent boundary separation and non-decision time (Fosco et al. 2017).
Bayesian Analyses
The benefits of Bayesian methods over null hypothesis significance testing (NHST) are well documented (Rouder and Morey 2012; Wagenmakers et al. 2016a, b) and were selected because they allow stronger conclusions by estimating the magnitude of support for both the alternative and null hypotheses simultaneously (Rouder and Morey 2012). Bayes factor mixed ANOVAs with default prior scales (Rouder and Morey 2012; Wagenmakers et al. 2016a) were conducted using JASP 0.8.3 (JASP Team 2017). Instead of a p value, these analyses provide BF10, which is the Bayes Factor of the alternative hypothesis (H1) against the null hypothesis (H0). BF10 is an odds ratio, where values above 3.0 are considered moderate evidence supporting the alternative hypothesis (i.e., statistically significant evidence for the alternative hypothesis). BF10 values above 10.0 are considered strong (>30 = very strong, >100 = decisive/extreme support; Wagenmakers et al. 2016a).
Conversely, BF01 is the Bayes Factor of the null hypothesis (H0) against the alternative hypothesis (H1). BF01 is the inverse of BF10 (i.e., BF01 = 1/BF10), and is reported when the evidence indicates a lack of an effect (i.e., favors the null hypothesis; Rouder and Morey 2012). BF01 values are interpreted identically to BF10 (>3.0 = moderate, >10.0 = strong, >100 = decisive/extreme support for the null hypothesis that a predictor is not associated with an outcome; Rouder and Morey 2012).
Thus, finding BF10 = 10.0 would indicate that the observed data are 10 times more likely under the alternative hypothesis model (e.g., strong evidence for deficits in the ADHD vs. Non-ADHD group), whereas BF01 = 10 would indicate that the observed data are 10 times more likely under the null hypothesis model (e.g., strong evidence that the ADHD and Non-ADHD groups are equivalent). Comparisons are supplemented with Cohen’s d effect sizes.
Data Analysis Overview
Dependent variables were first examined for outliers, and outliers were winsorized to 3 SDs of the group distribution (ADHD group: 1.5% of data points; Non-ADHD group: 1.2% of data points). The analytic plan was executed in three tiers. Tiers 1 and 2 included 2 Group (ADHD vs. Non-ADHD) × 2 Task (no-tone vs. stop signal) mixed ANOVAs. We first conducted comparisons of MRT to replicate previous findings indicating that go-trial estimates of response speed are slower during tasks with intermittent stop trials, and to determine whether adding these inhibitory demands differentially affects children with vs. without ADHD (Tier 1). In the second Tier, we used the Ratcliff (1978) diffusion model to test the study’s primary hypotheses and examine potential cognitive mechanisms underlying these effects to evaluate support for dual task and performance adjustment predictions. Finally, exploratory analyses probed the effect of our decision to include both neurotypical and clinical control children in the Non-ADHD group by repeating Tier 1 and 2 analyses with the Non-ADHD group separated into Neurotypical and Clinical Control subsamples (3 Group: ADHD vs. non-ADHD clinical vs. neurotypical × 2 Task: no-tone vs. stop signal).
Results
Bayesian Power Analysis
A series of simulation studies were conducted to estimate power for between-group tests using the R BayesFactor package and BayesianPowerTtest script (Lakens 2016) optimized by Zimmerman (2016), with parameters as follows (N = 144; r-scale = 1; k = 100,000 simulated experiments; BF threshold = 3.0). Results indicated power = .89 for supporting the alternative hypothesis of impaired information processing in ADHD based on a true effect of d = 0.63 (meta-analytic estimates for ADHD/Non-ADHD drift rate differences range from 0.63 to 0.75 in Karalunas et al. 2014 and Huang-Pollock et al. 2012, respectively; 89% of simulations correctly supported H1 at BF10 ≥ 3.0, 10% provided equivocal support at BF10 values between 1/3 and 3, and less than 1% incorrectly supported H0). Similarly, results indicate that our Type 1 error probability is 1%. That is, we have a 1% chance of falsely supporting the alternative hypothesis if the null hypothesis is true (i.e., for d = 0.0; 84% of simulations supported H0, 15% provided equivocal support, and only 1% incorrectly supported H1). Taken together, the Bayesian power analyses indicate very low likelihood of drawing false conclusions, with a Type 1 false positive likelihood of 1% and a Type 2 false negative likelihood of 1%.
Of note, these Bayesian power estimates are for single variable comparisons (i.e., independent samples t-tests). To our knowledge, Bayesian power analysis for mixed-model ANOVA is not yet available. Power analysis based on traditional NHST, with α = .05, power = .80, 2 groups (ADHD, Non-ADHD), and 2 measurements (No-Tone, Stop-Signal tasks) indicates that our N = 144 can reliably detect between-group effects of d = 0.40, within-group effects of d = 0.22, and group x condition interaction effects of d = 0.23 or larger. Thus, the study is sufficiently powered to address its primary aims.
Preliminary Analyses
Means and SDs for each outcome variable are shown in Table 2. Parent and teacher ADHD ratings were significantly elevated for the ADHD group relative to the Non-ADHD group as expected (all BF10 > 172.00; Table 2). The groups showed statistically equivalent age (BF01 = 5.48) and IQ (BF01 = 4.15), and did not differ significantly in gender composition (BF01 = 1.25) or SES (BF01 = 2.68).
Examination of the proportion of successful inhibitions on the stop-signal task indicated that the task functioned as expected, and that the ADHD (49.4%) and Non-ADHD (50.8%) groups were equivalent in the proportion of successful inhibitions (between-group comparison: BF01 = 4.69; one-sample test compared to expected 50% successful inhibitions: BF01 = 10.70).Footnote 3
Tier 1: Impact of Inhibition Demands on Overall Response Speed
Response speed (MRT)
Replicating previous research, a main effect of task was observed (BF10 = 8.27 × 1012; d = 0.76), such that children responded more slowly during the stop-signal than the no-tone task, as expected. The ADHD and Non-ADHD groups were equivalent in terms of response speed (BF01 = 3.43; d = 0.17). Relative to the main effects model, there was inconclusive evidence for a group x task interaction (BF10 = 1.94), suggesting no significant evidence that the introduction of the stop signal differentially slowed MRT for children with and without ADHD.
Tier 2: Cognitive Mechanisms Underlying Effects of Inhibition Demands on Response Speed
Boundary separation (a)
As shown in Fig. 1, boundary separation was significantly higher during the stop-signal relative to no-tone task (BF10 = 6221.78; d = 0.38). There was moderate evidence that groups were equivalent in boundary separation (BF01 = 3.26; d = 0.22), and that introducing intermittent stop trials affected the ADHD and Non-ADHD groups equivalently (group x task interaction: BF01 = 5.56). This pattern was consistent with the performance adjustment hypothesis that children adopt a strategy characterized by deliberately slowing their response speeds and considering greater quantities of information before making a decision to respond. It was inconsistent, however, with our expectation that MRT-related slowing would be driven by increases in response caution for the control group but not the ADHD group.

Impact of intermittent stop signals and diagnostic group on drift diffusion parameters. (a) Higher boundary separation reflects greater response caution, (b) higher values of drift rate reflect faster processing speed, and (c) lower values of non-decision time reflect faster stimulus encoding / motor response execution. Error bars are Bayesian 95% credible intervals
Drift rate (v)
Contrary to hypotheses, drift rate was equivalent across the stop-signal and no-tone tasks (BF01 = 3.08; d = 0.12), and the ADHD/Non-ADHD groups showed equivalent changes in drift rate when inhibition demands were added (group x task interaction: BF01 = 4.38). There was also insufficient evidence to support a main effect of group (BF10 = 1.49; d = 0.36). The lack of a main effect of task was consistent with performance adjustment hypothesis predictions, but inconsistent with the dual-task requirement hypothesis that the increased top-down cognitive control associated with the presence of intermittent “stop” trials would significantly affect bottom-up information processing speed. It was also inconsistent with the hypothesis that increased dual-task demands introduced by the stop signal would differentially disrupt information processing speed in ADHD as a function of their top-down impairments in cognitive control.
Non-decision time (t0)
There was moderate evidence that non-decision time was equivalent during the stop-signal and no-tone tasks (BF01 = 5.73; d = 0.07). There was also significant evidence against a main effect of group on non-decision time (BF01 = 5.43; d = 0.01), and against the group x task interaction (BF01 = 4.30). The lack of a main effect of task was consistent with performance adjustment hypothesis predictions, but inconsistent with the dual-task requirement hypothesis that the increased top-down cognitive control associated with the presence of intermittent “stop” trials significantly disrupts efficient stimulus encoding and response execution processes.
Tier 3: Exploratory Analyses
Exploratory results separating the Non-ADHD group into neurotypical and clinical control subgroups were highly consistent with the confirmatory analyses reported above. That is, the 3 Group (ADHD, Clinical Control, Neurotypical) × 2 Task (No-Tone, Stop-Signal) Bayesian mixed-model ANOVAs indicated significant evidence against main effects of group for MRT (BF01 = 4.85), boundary separation (BF01 = 6.25), and non-decision time (BF01 = 7.68), with inconclusive evidence for an effect of group on drift rate (BF10 = 1.70). Importantly, there was also significant evidence against a group x task interaction for boundary separation (BF01 = 7.98), drift rate (BF01 = 8.81), and non-decision time (BF01 = 11.35); there was no significant evidence of a group x task interaction for MRT (BF10 = 1.26). Combined with the evidence for task effects on boundary separation (BF10 = 6221.78), and evidence against task effects on drift rate (BF01 = 3.08) and non-decision time (BF01 = 5.73), these results indicate that the ADHD, clinical control, and neurotypical groups equivalently engaged in a slowing strategy consistent with the performance adjustment hypothesis.
Discussion
Tasks intended to measure inhibitory control are ubiquitously used to understand ADHD-related cognitive functioning. It is well-documented that increasing a task’s inhibitory demands reliably slows reaction time for individuals with (e.g., Alderson et al. 2008) and without ADHD (e.g., Verbruggen and Logan 2009), but little is known about the cognitive processes underlying these slowed responses. More importantly, no study has previously investigated whether the cognitive processes driving these slower responses differ for children with versus children without ADHD, despite the centrality of “go” responding for estimating children’s inhibitory speed. We assessed the extent to which children with ADHD demonstrate slower RTs during tasks with higher inhibition demands due to disruptions in bottom-up information processing efficiency as a function of increased inhibitory, working memory, and divided attention demands (dual-task requirement hypothesis) or due to the adoption of a more deliberate, cautious response strategy (performance adjustment hypothesis).
Effects of Intermittent Inhibition Demands on Response Speed
Replicating previous research (Alderson et al. 2008; Verbruggen and Logan 2009), we found that both children with and without ADHD slowed their overall reaction times (MRT) when intermittent stop signals were introduced. Decomposing reaction times into distinct information processing components revealed that this slowing was driven by an increase in boundary separation, with children adopting a more cautious response strategy and considering greater quantities of information before making a decision to respond. Contrary to expectations, the presence of intermittent stop trials did not significantly change the rate of information accumulation during go trials (drift rate) or the speed of encoding/response execution (non-decision time) for any group. This pattern of findings uniformly supports the performance adjustment hypothesis and is inconsistent with the dual-task requirements hypothesis (see Table 1; Verbruggen and Logan 2009). Furthermore, although we expected a differential impact of increasing inhibitory demands on information processing components across groups, both children with and without ADHD increased their level of response caution to an equivalent degree. This study provides evidence that children with ADHD engage in similar cognitive strategies as children without ADHD when adapting to the increased executive control demands evoked by the stop signal. Moreover, exploratory analyses revealed that this pattern held even when separating the non-ADHD group into clinical control and neurotypical groups. Taken together, results indicate that children’s slowing during inhibition tasks is a deliberate strategy, rather than an outcome of disrupted top-down cognitive control. Future work is needed to determine whether the performance adjustments identified herein are proactive or reactive (Verbruggen and Logan 2009), whether top-down processes are differentially involved in proactive vs. reactive performance adjustments (Wiemers and Redick 2018), and whether children with and without ADHD differ in the form of performance adjustments despite equivalent overall speed-accuracy trade-off changes (Shiels and Hawk 2010).
Information Processing in ADHD: Practical Implications
Reaction time is the primary dependent variable for many cognitive tasks, and it is relatively common for researchers to utilize response times to “go” trials during inhibition tasks as indicators of processing speed (see Kofler et al. 2013). This practice likely leads to inflated response speed estimates for both children with and without ADHD, which is not a significant concern for examining diagnostic group differences. It may, however, create noise when attempting to aggregate or compare MRT data across studies that differ in the presence vs. absence of inhibitory demands.
More problematic is that MRT obscures meaningful information about cognitive performance, and continued reliance on MRT will hinder our ability to refine theory and inform treatment (see Huang-Pollock et al. 2017 for further discussion of this issue). To illustrate, if MRT was the primary outcome variable in the current study, we would likely have concluded that introducing stop signals slows processing speed, as MRT is often described as reflecting speed of processing. Yet, we found evidence against this interpretation when RTs were decomposed into drift diffusion parameters because drift rate was equivalent across the no-tone and stop-tone tasks. We therefore urge researchers to exercise caution when interpreting standard performance metrics, such as RT and error rates, and to utilize metrics that have clearer cognitive interpretations whenever possible.
Information processing in ADHD: Theoretical implications
Self-regulation
Self-regulation is the process by which individuals dynamically modulate their internal states and behavior to adaptively respond to changes in their internal and external environment (Nigg 2017). Although difficulty regulating attention and behavior is a core feature of all behavioral symptoms of ADHD, previous research has not consistently demonstrated that basic self-regulatory processes, including performance monitoring and post-error slowing, are impacted in ADHD (Shiels and Hawk 2010). Other experimental work has been mixed regarding whether response caution adjustments across diagnostic groups are similar (Fosco et al. 2017) or different (Mulder et al. 2010). A complicating factor in synthesizing previous research is that absence of evidence does not provide evidence of absence. That is, the lack of a diagnostic group difference when using a frequentist statistical approach is difficult to interpret. The Bayesian approach utilized in the current study is advantageous in this regard because it estimates the degree of support for the null over the alternative hypothesis, thus providing evidence for the absence of an effect (see e.g., Wagenmakers et al. 2016b). The present study provided significant evidence that children with ADHD were able to adjust their degree of response caution just as well as their non-ADHD peers. This evidence of equivalence across groups, coupled with the inconsistencies of previous findings, suggests relatively intact regulation of speed-accuracy tradeoffs in response to changing task demands in ADHD. When considered along with research in other domains of task-related self-regulation, it is clear that children with ADHD do not exhibit obvious problems with basic components of self-regulation. Rather, self-regulatory difficulties are likely dependent on task demands, such as difficulty level, task type, presence of feedback, etc. (Patros et al. 2017; Shiels and Hawk 2010).
Cognition
Recent evidence suggests that reduced working memory abilities may be a causal pathway to ADHD (Kofler et al. 2018; Nigg et al. 2018) and that reduced working memory capacity results in impaired bottom-up information processing speed due to difficulties maintaining consistent top-down control (Weimers and Redick 2018; cf. Weigard and Huang-Pollock 2017). The current study found no evidence consistent with that pattern, as processing speed (drift rate) was equivalent across the no-tone and stop-signal conditions. Differences in findings could indicate that placing high demands on working memory specifically (as opposed to other cognitive processes such as inhibitory control as manipulated in the current study) drives disruptions in bottom-up processing speed and consistency of reaction times (Kofler et al. 2014; Weimers and Redick 2018). Although intermittent stop signals do increase working memory demands by requiring the maintenance of two competing task goals in mind, it may not produce a degree of difficulty comparable to the working memory manipulations used in previous studies. That is, if bottom-up processing speed is impacted by high working memory demands, then the introduction of the stop signal may have been too weak of a manipulation to produce impairment. Neuroimaging work supports this hypothesis, as working memory tasks tend to activate higher-order circuitry in the prefrontal cortex (Nee et al. 2013) that is not evoked during inhibition paradigms (Cortese et al. 2012; Luijten et al. 2014). Alternatively, the impact of top-down control on bottom-up processing may not be unique to working memory and could be engendered by numerous cognitive processes. It is possible that the stop signal, as typically utilized, is not a strong enough inhibition manipulation to impair top-down control and downstream impairments in information processing speed.
Testing these competing hypotheses in future work will inform the ongoing debate regarding whether children with ADHD exhibit broad deficits across numerous cognitive domains, or whether these deficits are accounted for by a smaller number of cognitive impairments that result in worse performance across tasks intended to measure a wide variety of cognitive functions (Coghill et al. 2014; Kofler et al. 2018). Of course, it would be impossible to design an experimental manipulation that isolates one cognitive process (Friedman and Miyake 2004). As a starting point, one could manipulate the degree of inhibitory demands or manipulate various working memory demands during a standard stop signal task (Alderson et al. 2017). Conducting a series of carefully-controlled experiments that place relatively higher demands on certain processes over others will inform whether impaired performance is primarily driven by demands on specific cognitive processes or by more generalized increases in any cognitive demand (Snyder et al. 2015). It may also be useful to test these hypotheses among children in even younger age groups when some neurocognitive functions show more unitary relations rather than functional specificity (Garon et al. 2008), and may relate to ADHD symptom severity differently (Brocki et al. 2007).
Limitations
The current study was the first to test different hypotheses to explain changes in information processing induced by adding inhibitory control demands in a relatively large sample of children with and without ADHD. Yet, several caveats must be considered when interpreting results. The present study manipulated top-down cognitive control demands and examined effects on bottom-up information processing but was unable to test for effects of bottom-up information processing on top-down cognitive control. Studies investigating reciprocal influences among top-down and bottom-up processes will be critical for establishing a taxomony of neurocognitive impairments in ADHD, particularly given recent evidence that inducing slower information accumulation may result in reduced working memory task performance (Weigard and Huang-Pollock 2017). This study was also unable to tease apart the extent to which findings were driven by increases in inhibitory demands, working memory demands, divided attention demands, or a combination of all three.
Although not the primary focus of the current study, we were somewhat surprised to find that groups did not differ in stop signal reaction time (SSRT), which is often, but not always, observed in the ADHD literature. Though speculative, the groups’ equivalent SSRT is likely due to their equivalent MRT, given evidence that ADHD – control group differences in SSRT appear to be driven primarily by group differences in MRT (Alderson et al. 2007; Lijffijt et al. 2005), and that group differences in MRT are driven primarily by a subset of abnormally slow responses in the tail of the reaction time distribution (Kofler et al. 2013). The stop signal task utilized in the present study had a short response window (1000 ms), which may preclude abnormally slow reaction times that might create diagnostic group differences in MRT (and SSRT subsequently). This interpretation is aligned with simulation work demonstrating that differentially skewed go responses produce ‘fictitious’ inhibitory differences in ADHD (Verbruggen et al. 2013). Similarly, we did not observe diagnostic group differences in drift rate, which may also be due to the response length, as diagnostic group differences in drift rate are greater during slow event rate than fast event rate conditions (Huang-Pollock et al. 2017).
The current findings must be understood within the context of the sample. In any study, decisions regarding whether to recruit a clinical control or healthy control group result in trade-offs between internal validity (and the strength of conclusions that can be drawn about a particular diagnostic group) and generalizability. The current study attempted to balance these considerations by including both a clinical and healthy control group. The ADHD and clinical control groups were matched for the number of non-ADHD disorders because neither cognitive dysfunction nor behavioral symptoms (e.g., difficulty concentrating, restlessness) appear unique to ADHD (e.g., Snyder 2013; Youngstrom et al. 2010), and emerging evidence suggests that some (formally) putative pathways to the ADHD phenotype may be linked with common comorbidities rather than ADHD itself (Tenenbaum et al. 2018). Though inclusion of non-ADHD disorders could potentially have obscured diagnostic group differences, exploratory analyses revealed that the pattern of results is unchanged when the control groups are examined separately.
It is also possible that our sampling methods impacted observed results. Although all children were recruited from the community specifically for research purposes, parental motivation for participation was likely different across participants, which may have introduced sampling bias (Wacholder et al. 1992). For example, some families were likely motivated by the no-cost psychoeducational evaluation provided to all participants, either because they suspected a behavioral/affective/academic disorder or because they wanted data on their child’s intellectual and academic functioning, whereas other families expressed a desire to contribute to research and/or felt that it would be a valuable experience for their child. While the sample more generally represents a community-based rather than hospital/clinical-based sample, replications using explicit community-based recruitment procedures would be helpful to maximize generalizability.
Conclusions
Understanding the nature and severity of ADHD-related cognitive deficits has the potential to refine theoretical models of ADHD etiology (Coghill et al. 2005) and improve diagnosis (Rapport et al. 2000) and treatment (Chacko et al. 2014; Molitor and Langberg 2017). The current study found that children with ADHD slowed their response times during the stop-signal task due to an intentional cognitive control strategy, rather than as a byproduct of disruptions in top-down cognitive control. Moreover, this pattern was equivalent for children with and without ADHD. Despite difficulties in some aspects of performance monitoring and cognitive control (Shiels and Hawk 2010), children with ADHD appear capable of flexibly adjusting their approach to tasks with different demands by modulating levels of response caution. Given increasing interest in targeting basic processes that are implicated in ADHD (e.g., Cortese et al. 2015), identifying processes that are intact in the disorder is critical, as it constrains the scope of potential interventions.
Of course, these results demonstrate group-level patterns, and ADHD is a dimensional and heterogeneous disorder (Fair et al. 2012; Marcus and Barry 2011). Next steps include exploring variation in response to experimental manipulations to understand the extent of this heterogeneity, as well as the processes that may account for this heterogeneity. Replications with a range of clinical and non-clinical groups, more ecologically-valid outcomes, and different types/modalities of information to be processed are also necessary to inform theory and to better understand the contexts under which these acute experimental findings inform real-world functioning.
Notes
SSRT is the primary measure of inhibitory speed in the stop signal task; it is computed as MRT - stop signal delay, which is the average duration of time between stimulus onset and stop signal onset.
Verbruggen and Logan (2009) refer to this as the proactive adjustment hypothesis, but because the current study was not designed to determine whether adjustments are proactive or reactive the more general description is used instead.
Additional analyses were conducted excluding individual participants whose percent inhibition was outside 25%-75% (n = 13). The pattern of results did not differ, so all participants are retained in analyses.
References
Achenbach, T.M., & Rescorla, L.A. (2001). Manual for the Achenbach system of empirically based assessment school-age forms profiles. Burlington, VT.
Albrecht, B., Brandeis, D., Uebel, H., Heinrich, H., Mueller, U. C., Hasselhorn, M., et al. (2008). Action monitoring in boys with attention-deficit/hyperactivity disorder, their nonaffected siblings, and normal control subjects: Evidence for an endophenotype. Biological Psychiatry, 64, 615–625.
Alderson, R. M., Patros, C. H., Tarle, S. J., Hudec, K. L., Kasper, L. J., & Lea, S. E. (2017). Working memory and behavioral inhibition in boys with ADHD: An experimental examination of competing models. Child Neuropsychology, 23, 255–272.
Alderson, R. M., Rapport, M. D., & Kofler, M. J. (2007). ADHD and behavioral inhibition: A meta-analytic review of the stop-signal paradigm. Journal of Abnormal Child Psychology, 35, 745–758.
Alderson, R. M., Rapport, M. D., Sarver, D. E., & Kofler, M. J. (2008). ADHD and behavioral inhibition: A re-examination of the stop-signal task. Journal of Abnormal Child Psychology, 36, 989–998.
American Psychiatric Association (2013). DSM-5. Washington, D.C.: APA.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65–94.
Balogh, L., & Czobor, P. (2016). Post-error slowing in patients with ADHD: A meta-analysis. Journal of Attention Disorders, 20, 1004–1016.
Brocki, K. C., Nyberg, L., Thorell, L. B., & Bohlin, G. (2007). Early concurrent and longitudinal symptoms of ADHD and ODD: Relations to different types of inhibitory control and working memory. Journal of Child Psychology and Psychiatry, 48, 1033–1041.
Bunford, N., Brandt, N. E., Golden, C., Dykstra, J. B., et al. (2015). ADHD symptoms mediate the association between deficits in executive functioning and social impairment in children. Journal of Abnormal Child Psychology, 43, 133–147.
Chacko, A., Kofler, M. J., & Jarrett, M. (2014). Improving outcomes for youth with ADHD: A conceptual framework for combined neurocognitive and skill-based treatment approaches. Clinical Child and Family Psychology Review, 17, 368–384.
Coghill, D., Nigg, J., Rothenberger, A., Sonuga-Barke, E., & Tannock, R. (2005). Whither causal models in the neuroscience of ADHD? Developmental Science, 8, 105–114.
Coghill, D. R., Seth, S., & Matthews, K. (2014). A comprehensive assessment of memory, delay aversion, timing, inhibition, decision making and variability in attention deficit hyperactivity disorder: advancing beyond the three-pathway models. Psychological Medicine, 44, 1989–2001.
Conners, C. K. (2008). Conners 3rd edition: Manual. Toronto, Ontario: Multi-Health Systems.
Cortese, S., Ferrin, M., Brandeis, D., Buitelaar, J., Daley, D., Dittmann, R. W., et al. (2015). Cognitive training for attention-deficit/hyperactivity disorder: Meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials. Journal of the American Academy of Child & Adolescent Psychiatry, 54, 164–174.
Cortese, S., Kelly, C., Chabernaud, C., Proal, E., Di Martino, A., Milham, M. P., & Castellanos, F. X. (2012). Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. American Journal of Psychiatry, 169, 1038–1055.
Cowan, N., Fristoe, N. M., Elliott, E. M., Brunner, R. P., & Saults, J. S. (2006). Scope of attention, control of attention, and intelligence in children and adults. Memory & Cognition, 34, 1754–1768.
Douglas, V. I. (1999). Cognitive control processes in attention-deficit/hyperactivity disorder. In H. C. Quay, & A. E. Hogan (Eds.), Handbook of disruptive behavior disorders (pp. 105−138). New York: Kluwer Academic/Plenum Publishing.
Fair, D. A., Bathula, D., Nikolas, M. A., & Nigg, J. T. (2012). Distinct neuropsychological subgroups in typically developing youth inform heterogeneity in children with ADHD. PNAS, 109, 6769–6774.
Fosco, W. D., White, C. N., & Hawk, L. W. (2017). Acute stimulant treatment and reinforcement increase the speed of information accumulation in children with ADHD. Journal of Abnormal Child Psychology, 45, 911–920.
Friedman, N. P., & Miyake, A. (2004). The relations among inhibition and interference control functions: A latent-variable analysis. Journal of Experimental Psychology: General, 133, 101–135.
Gadow, K. D., & Sprafkin, J. N. (2002). Child Symptom Inventory 4 (CSI-4): Screening and norms manual. Stony Brook, NY: Checkmate Plus.
Garon, N., Bryson, S. E., & Smith, I. M. (2008). Executive function in preschoolers: a review using an integrative framework. Psychological Bulletin, 134, 31–60.
Gomez, R., & Sanson, A. (1994). Effects of experimenter and mother presence on the attentional performance and activity of hyperactive boys. Journal of Abnormal Child Psychology, 22, 517–529.
Groen, Y., Wijers, A. A., Mulder, L. J., Waggeveld, B., Minderaa, R. B., & Althaus, M. (2008). Error and feedback processing in children with ADHD and children with Autistic Spectrum Disorder: an EEG event-related potential study. Clinical Neurophysiology, 119, 2476–2493.
Groom, M. J., Cahill, J. D., Bates, A. T., Jackson, G. M., Calton, T. G., Liddle, P. F., & Hollis, C. (2010). Electrophysiological indices of abnormal error-processing in adolescents with attention deficit hyperactivity disorder (ADHD). Journal of Child Psychology and Psychiatry, 51, 66–76.
Hawk, L.W. Jr., Fosco, W.D., Colder, C.R., Waxmonsky, J.G., Pelham, W.E. Jr., & Rosch, K.S. (in press). How do stimulant treatments for ADHD work? Evidence for mediation by improved cognitive function. Journal of Child Psychology and Psychiatry, online early.
Hollingshead, A. B. (1975). Four factor index of social status. New Haven, CT: Yale.
Huang-Pollock, C. L., Karalunas, S. L., Tam, H., & Moore, A. N. (2012). Evaluating vigilance deficits in ADHD: A meta-analysis of CPT performance. Journal of Abnormal Psychology, 121, 360–371.
Huang-Pollock, C., Ratcliff, R., McKoon, G., Shapiro, Z., Weigard, A., & Galloway-Long, H. (2017). Using the diffusion model to explain cognitive deficits in attention deficit hyperactivity disorder. Journal of Abnormal Child Psychology, 45, 57–68.
Hutchinson, E., Bavin, E., Efron, D., & Sciberras, E. (2012). A comparison of working memory profiles in school-aged children with specific language impairment, ADHD, comorbid SLI and ADHD and their typically developing peers. Child Neuropsychology, 18, 190–207.
Hwang, S. L., Gau, S. S.-F., Hsu, W. Y., & Wu, Y. Y. (2010). Deficits in interval timing measured by the dual-task paradigm among children and adolescents with attention-deficit/hyperactivity disorder. Journal of Child Psychology and Psychiatry, 51, 223–232.
JASP Team (2017). JASP. Version 0.8.5. [Computer Software].
Kamphaus, R. W., & Reynolds, C. R. (2007). BASC-2 behavioral and emotional screening system manual. Circle Pines, MN: Pearson.
Karalunas, S. L., & Huang-Pollock, C. L. (2013). Integrating impairments in reaction time and executive function using a diffusion model framework. Journal of Abnormal Child Psychology, 41, 837–850.
Karalunas, S. L., Huang-Pollock, C. L., & Nigg, J. T. (2012). Decomposing ADHD-related effects in response speed and variability. Neuropsychology, 26, 684–694.
Karalunas, S. L., Geurts, H. M., Konrad, K., Bender, S., & Nigg, J. T. (2014). Annual research review: Reaction time variability in ADHD and autism spectrum disorders: Measurement and mechanisms of a proposed trans-diagnostic phenotype. Journal of Child Psychology and Psychiatry, 55, 685–710.
Kasper, L. J., Alderson, R. M., & Hudec, K. L. (2012). Moderators of working memory deficits in children with ADHD: A meta-analytic review. Clinical Psychology Review, 32, 605–617.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., et al. (1997). K-SADS-PL: Initial reliability and validity data. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 980–988.
Kofler, M. J., Rapport, M. D., Sarver, D. E., Raiker, J. S., Orban, S. A., et al. (2013). Reaction time variability in ADHD: A meta-analytic review of 319 studies. Clinical Psychology Review, 33, 795–811.
Kofler, M. J., Alderson, R. M., Raiker, J. S., Bolden, J., Sarver, D. E., & Rapport, M. D. (2014). Working memory and intraindividual variability as neurocognitive indicators in ADHD: Examining competing model predictions. Neuropsychology, 28, 459–471.
Kofler, M. J., Sarver, D. E., Spiegel, J. A., Day, T. N., Harmon, S. L., & Wells, E. L. (2017). Heterogeneity in ADHD: Neurocognitive predictors of peer, family, and academic functioning. Child Neuropsychology, 23, 733–759.
Kofler, M. J., Irwin, L. N., Soto, E. F., Groves, N. B., Harmon, S.L., & Sarver, D. E. (2018). Executive functioning heterogeneity in pediatric ADHD. Journal of Abnormal Child Psychology, online early.
Lahey, B. B., Pelham, W. E., Loney, J., Lee, S. S., & Willcutt, E. (2005). Instability of the DSM-IV subtypes of ADHD from preschool through elementary school. Archives of General Psychiatry, 62, 896–902.
Lakens (2016). Bayesian Power T test [Computer software]. Retrieved from https://gist.github.com/Lakens/95c97116dfaa1f3a5672.
Lijffijt, M., Kenemans, J. L., Verbaten, M. N., & van Engeland, H. (2005). A meta-analytic review of stopping performance in ADHD. Journal of Abnormal Psychology, 114, 216–222.
Lipszyc, J., & Schachar, R. (2010). Inhibitory control and psychopathology: A meta-analysis of studies using the stop signal task. Journal of the International Neuropsychological Society, 16, 1064–1076.
Logan, G. D., Cowan, W. B., & Davis, K. A. (1984). On the ability to inhibit simple and choice reaction time responses: A model and a method. Journal of Experimental Psychology: Human Perception and Performance, 10, 276–291.
Luijten, M., Machielsen, M. W., Veltman, D. J., Hester, R., de Haan, L., & Franken, I. H. (2014). Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people with substance dependence and behavioural addictions. Journal of Psychiatry & Neuroscience, 39, 149–169.
Marcus, D. K., & Barry, T. D. (2011). Does attention-deficit/hyperactivity disorder have a dimensional latent structure? A taxometric analysis. Journal of Abnormal Psychology, 120, 427–442.
Molitor, S. J., & Langberg, J. M. (2017). Using task performance to inform treatment planning for youth with ADHD: A systematic review. Clinical Psychology Review, 58, 157–173.
Mulder, M. J., Bos, D., Weusten, J. M., van Belle, J., van Dijk, S. C., Simen, P., et al. (2010). Basic impairments in regulating the speed-accuracy tradeoff predict symptoms of attention-deficit/hyperactivity disorder. Biological Psychiatry, 68, 1114–1119.
Nee, D. E., Brown, J. W., Askren, M. K., Berman, M. G., Demiralp, E., et al. (2013). A meta-analysis of executive components of working memory. Cerebral Cortex, 23(2), 264–282.
Nigg, J. T. (2017). Annual Research Review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, 58, 361–383.
Nigg, J. T., Gustafsson, H. C., Karalunas, S. L., Ryabinin, P., McWeeney, S. K., Faraone, S. V., et al. (2018). Working memory and vigilance as multivariate endophenotypes related to common genetic risk for attention-deficit/hyperactivity disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 57, 175–182.
Nigg, J. T., Willcutt, E. G., Doyle, A. E., & Sonuga-Barke, E. J. (2005). Causal heterogeneity in ADHD: Do we need neuropsychologically impaired subtypes? Biological Psychiatry, 57, 1224–1230.
Patros, C. H. G., Alderson, R. M., Lea, S. E., & Tarle, S. J. (2017). Context influences decision-making in boys with attention-deficit/hyperactivity disorder: A comparison of traditional and novel choice-impulsivity paradigms. Child Neuropsychology, 23, 242–254.
Raiker, J. S., Freidman, L. M., Orban, S. A., Kofler, M. J., Sarver, D. E., & Rapport, M. D. (2018). Phonological working memory deficits in ADHD revisited: The role of lower-level information processing deficits in impaired working memory performance. Journal of Attention Disorders, online early.
Rapport, M. D., Chung, K. M., Shore, G., Denney, C. B., & Isaacs, P. (2000). Upgrading the science and technology of assessment and diagnosis: Laboratory and clinic-based assessment of children with ADHD. Journal of Clinical Child Psychology, 29, 555–568.
Ratcliff, R. (1978). A theory of memory retrieval. Psychological Review, 85, 59–108.
Ratcliff, R., & McKoon, G. (2008). The diffusion decision model: Theory and data for two-choice decision tasks. Neural Computation, 20, 873–922.
Rieger, M., & Gauggel, S. (1999). Inhibitory after-effects in the stop signal paradigm. British Journal of Psychology, 90, 509–518.
Rouder, J. N., & Morey, R. D. (2012). Default Bayes factors for model selection in regression. Multivariate Behavioral Research, 47, 877–903.
Schachar, R. J., Chen, S., Logan, G. D., Ornstein, T. J., et al. (2004). Evidence for an error monitoring deficit in ADHD. Journal of Abnormal Child Psychology, 32, 285–293.
Shiels, K., & Hawk, L. W., Jr. (2010). Self-regulation in ADHD: The role of error processing. Clinical Psychology Review, 30, 951–961.
Snyder, H. R. (2013). Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: a meta-analysis. Psychological Bulletin, 139, 81–132.
Sonuga-Barke, E., Bitsakou, P., & Thompson, M. (2010). Beyond the dual pathway model: Evidence for the dissociation of timing, inhibitory, and delay-related impairments in ADHD. Journal of the American Academy of Child & Adolescent Psychiatry, 49, 345–355.
Soreni, N., Crosbie, J., Ickowicz, A., & Schachar, R. (2009). Stop signal and Conners’ CPT: Test-retest reliability of two inhibition measures in ADH. Journal of Attention Disorders, 13, 137–143.
Snyder, H. R., Miyake, A., & Hankin, B. L. (2015). Advancing understanding of executivefunction impairments and psychopathology: Bridging the gap between clinical and cognitive approaches. Frontiers in Psychology, 6. https://doi.org/10.3389/fpsyg.2015.00328.
Tenenbaum, R. B., Musser, E. D., Raiker, J. S., Coles, E. K., Gnagy, E. M., & Pelham, W. E. (2018). Specificity of reward sensitivity and parasympathetic-based regulation among children with attention-deficit/hyperactivity and disruptive behavior disorders. Journal of Abnormal Child Psychology, 46, 965–977.
Tseng, W. L., & Gau, S. S.-F. (2013). Executive function as a mediator in the link between ADHD and social problems. Journal of Child Psychology and Psychiatry, 54, 996–1004.
Valo, S., & Tannock, R. (2010). Diagnostic instability of DSM–IV ADHD subtypes: Effects of informant source, instrumentation, and methods for combining symptom reports. Journal of Clinical Child & Adolescent Psychology, 39, 749–760.
Van De Voorde, S., Roeyers, H., & Wiersema, J. R. (2010). Error monitoring in children with ADHD or reading disorder: An event-related potential study. Biological Psychology, 84, 176–185.
Verbruggen, F., Chambers, C. D., & Logan, G. (2013). Fictitious inhibitory differences: How skewness and slowing distort the estimation of stopping latencies. Psychological Science, 24, 352–362.
Verbruggen, F., & Logan, G. D. (2009). Proactive adjustments of response strategies in the stop-signal paradigm. Journal of Experimental Psychology: Human Perception and Performance, 35, 835–854.
Verbruggen, F., Logan, G. D., Liefooghe, B., & Vandierendonck, A. (2008). Short-term aftereffects of response inhibition: Repetition priming or between-trial control adjustments? Journal of Experimental Psychology: Human Perception and Performance, 34, 413–426.
Voss, A., & Voss, J. (2007). Fast-dm: A free program for efficient diffusion model analysis. Behavior Research Methods, 39, 767–775.
Voss, A., Nagler, M., & Lerche, V. (2013). Diffusion models in experimental psychology: A practical introduction. Experimental Psychology, 60, 385–402.
Wacholder, S., Silverman, D. T., McLaughlin, J. K., & Mandel, J. S. (1992). Selection of controls in case-control studies: II. Types of controls. American Journal of Epidemiology, 135, 1029–1041.
Wagenmakers, E., Morey, R. D., & Lee, M. D. (2016a). Bayesian benefits for the pragmatic researcher. Current Directions in Psychological Science, 25, 169–176.
Wagenmakers, E. J., Verhagen, J., & Ly, A. (2016b). How to quantify the evidence for the absence of a correlation. Behavior Research Methods, 48, 413–426.
Wechsler, D. (2014). Wechsler Intelligence Scale for Children-Fifth Edition. San Antonio: Pearson.
Weigard, A., & Huang-Pollock, C. (2017). The role of speed in ADHD-related working memory deficits: A time-based resource-sharing and diffusion model account. Clinical Psychological Science, 5, 195–211.
Wiemers, E. A., & Redick, T. S. (2018). Working memory capacity and intra-individual variability of proactive control. Acta Psychologica, 182, 21–31.
Willcutt, E., Doyle, A., Nigg, J., Faraone, S., & Pennington, B. (2005). Validity of the executive function theory of ADHD: A meta-analytic review. Biological Psychiatry, 57, 1336–1346.
Wright, L., Lipszyc, J., Dupuis, A., Thayapararajah, S. W., & Schachar, R. (2014). Response inhibition and psychopathology: A meta-analysis of go/no-go task performance. Journal of Abnormal Psychology, 123, 429–439.
Youngstrom, E. A., Arnold, L. E., & Frazier, T. (2010). Bipolar and ADHD comorbidity: Both artifact and outgrowth of shared mechanisms. Clinical Psychology: Science & Practice, 17, 350–359.
Zimmerman (2016). Bayesian Power Analysis T test [Computer software]. Retrieved from https://datashenanigan.wordpress.com/2016/ 01/15/speeding-bayesian-power-analysis-t-test-up-with-snowfall/.
Acknowledgements
This work was supported in part by the UVa Curry School of Education Foundation Galant Family grant (PI: Kofler) and the Oklahoma Center for the Advancement of Science & Technology (HR17-051; PI: Alderson). During the production of this manuscript, Dr. Kofler was supported in part by the National Institutes of Health (R34 MH102499-01); Dr. Raiker was supported in part by the Brain and Behavior Research Foundation (#66791), the Children’s Trust (#7561, #7161), NIMH (MH099030, MH112002), and NSF (CNS-1532061); Dr. Sarver was supported in part by the Mississippi Council on Developmental Disabilities (4680-DD17-HE; PI: Sarver). The sponsors had no role in design and conduct of the study, collection, management, analysis, and interpretation of the data, or preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflicts of interest to report.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent/assent were obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fosco, W.D., Kofler, M.J., Alderson, R.M. et al. Inhibitory Control and Information Processing in ADHD: Comparing the Dual Task and Performance Adjustment Hypotheses. J Abnorm Child Psychol 47, 961–974 (2019). https://doi.org/10.1007/s10802-018-0504-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-018-0504-9