
Abstract
Despite growing evidence that bipolar disorder often emerges in adolescence, there are limited data regarding treatment patterns of youth with bipolar disorder in community samples. Our objective was to present the prevalence and clinical correlates of treatment utilization for a nationally representative sample of US adolescents with bipolar disorder. Analyses are based on data from the National Comorbidity Survey-Adolescent Supplement, a face-to-face survey of 10,123 adolescents (ages 13–18) identified in household and school settings. We found that of adolescents meeting DSM-IV criteria for bipolar I or II disorder (N = 250), 49 % were treated for depression or mania, 13 % were treated for conditions other than depression or mania, and 38 % did not report receiving treatment. Treatment for depression or mania was associated with increased rates of suicide attempts, as well as greater role disability and more comorbid alcohol use relative to those who had not received treatment. Treated adolescents had triple the rate of ADHD and double the rates of behavior disorders than those without treatment. Our findings demonstrate that a substantial proportion of youth with bipolar disorder do not receive treatment, and of those who do, many receive treatment for comorbid conditions rather than for their mood-related symptoms. Treatment was more common among youth with severe manifestations and consequences of bipolar disorder and those with behavior problems. These trends highlight the need to identify barriers to treatment for adolescents with bipolar disorder and demonstrate that those in treatment are not representative of youth with bipolar disorder in the general population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Despite increasing evidence that bipolar disorder often emerges in adolescence (Beesdo et al. 2009; Lewinsohn et al. 2003; Merikangas et al. 2011b; Van Meter et al. 2011), only about half of adolescents with bipolar disorder receive mental health care (Kozloff et al. 2010; Lewinsohn et al. 2003; Merikangas et al. 2011b). Recent studies have documented that bipolar disorder is not rare in the general population (Merikangas et al. 2010) and has serious impact and consequences (Goldstein and Birmaher 2012; Kozloff et al. 2010). These findings highlight the importance of identifying correlates and barriers to service use, particularly in the mental health specialty sector where evidence-based treatment is more widely applied (Youngstrom et al. 2012). Understanding treatment patterns among adolescents with bipolar disorder is especially crucial, as delayed treatment for initial mood episodes in adolescence has been linked to more adverse illness outcomes in adulthood (Post et al. 2010).
Most previous research on treatment utilization among adolescents with bipolar disorder has been derived from studies of clinical samples (Castilla-Puentes 2008; Evans-Lacko et al. 2011; Olfson et al. 2009; Peele et al. 2004). One such study demonstrated that the mental health costs of bipolar spectrum disorders in adolescents are substantially elevated over those associated with either other mood or non-mood disorders (Peele et al. 2004). Treatment use among youth with bipolar disorder in clinical samples has been found to increase with older age (Rizzo et al. 2007), greater symptom severity (Rizzo et al. 2007), the experience of multiple mood episodes per year (Castilla-Puentes 2008), and the number of additional psychiatric diagnoses (Evans-Lacko et al. 2011). Within clinical samples, youths diagnosed with bipolar disorder are often those who have been previously treated for other serious mental health problems (Olfson et al. 2009). These youths continue to be diagnosed with additional psychiatric disorders concurrently with and following their bipolar disorder diagnosis (Evans-Lacko et al. 2011; Olfson et al. 2009).
These findings underscore the difficulty of relying on clinical samples to identify correlates of treatment. In fact, the now well-established concept of Berkson’s bias was identified because of the lack of equivalence of risk factors in cases and controls selected from inpatient samples. In general, adolescents with comorbid disorders are substantially more likely to receive treatment for mental disorders (Merikangas et al. 2011a). For example, more than 70 % of adolescents with three or more classes of disorders compared to only 20 % of those with only one class of disorder have received mental health treatment (Merikangas et al. 2011a). Problematic substance use is particularly likely to facilitate referral to the mental health specialty sector in young adults with bipolar disorder as compared to adolescents with bipolar disorder (Kozloff et al. 2010). The latter study of a large sample of Canadian youth is one of the only studies that has investigated differences between those youth with bipolar disorder in the general community who do and do not receive mental health treatment.
There is a particular lack of information on correlates of treatment for bipolar disorder in youth from nationally representative samples of the U.S., aside from the substantial information that has been derived from regional U.S. community surveys regarding correlates of service use for mental health problems in general (Angold et al. 2000; Farmer et al. 1999; Pumariega et al. 1998; Zwaanswijk et al. 2003b). Identification of characteristics that are associated with treatment has important implications for facilitating treatment for youth in need, as well as for examining the generalizability of clinical samples to the general population of youth with bipolar disorder.
The present study examines treatment patterns of adolescents with bipolar disorder in a nationally representative sample of adolescents in the U.S. The goals of the present report are to: 1) present the rates of treatment in a nationally representative sample of adolescents with bipolar disorder, and 2) examine the differences in clinical correlates and comorbidity of bipolar disorder among those who were treated specifically for symptoms of mania or depression compared to those who were treated for other disorders, and those who did not receive any treatment.
Method
Sample and Procedure
The NCS-A is a nationally representative face-to-face survey of 10,123 adolescents aged 13–18 years in the continental US (Merikangas et al. 2009). The survey was administered by the professional interview staff of the Institute for Social Research at the University of Michigan. The NCS-A was carried out in a dual-frame sample that included a household sub-sample and a school sub-sample (Kessler et al. 2009a, b; Kessler and Merikangas 2004). The overall NCS-A adolescent response rate combining the two sub-samples was 82.9 %. One parent or parent surrogate of each participating adolescent was asked to complete a self-administered questionnaire that contained informant questions about the adolescent’s mental health. All participants provided informed consent prior to their inclusion in the study. These recruitment and consent procedures were approved by the Human Subjects Committees of both Harvard Medical School and the University of Michigan, and have therefore been performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its amendments. Once the survey was completed, cases were weighted for variation in within-household probability of selection (in the household sub-sample) and for residual discrepancies between the sample and the U.S. population on the basis of socio-demographic and geographic variables. These weighting procedures are discussed in more detail elsewhere (Kessler et al. 2009a, b). Socio-demographic variables included in these analyses were age (in years), sex, and race/ethnicity.
The weighted socio-demographic characteristics of the study sample have been presented previously (Merikangas et al. 2010). About half the sample was male (51.3 %) and the mean age was 15.2 years, with a larger proportion of youth aged 13–14 years (36.2 %), and approximately equal distributions of youth aged 15–16 and 17–18 years. The sample was comprised of 65.6 % non-Hispanic Whites, 15.1 % non-Hispanic Blacks, 14.4 % Hispanics, and 5.0 % Other.
Measures
Diagnostic Assessment
Details of the diagnostic and risk factor measures are described by Merikangas and colleagues (Merikangas et al. 2009). Briefly, adolescents were administered a modified version of the World Health Organization (WHO) Composite International Diagnostic Interview Version 3.0 (CIDI), a fully structured interview administered by trained lay interviewers to generate DSM-IV diagnoses (Kessler and Ustun 2004). Lifetime disorders assessed in the CIDI included mood episodes and disorders (major depressive disorder [MDD] or dysthymic disorder, mania, and hypomania), anxiety disorders (agoraphobia, generalized anxiety disorder [GAD], panic disorder, separation anxiety disorder [SAD], social phobia, specific phobia, posttraumatic stress disorder [PTSD]), behavior disorders (oppositional defiant disorder [ODD], conduct disorder [CD]), attention deficit/hyperactivity disorder (ADHD) eating disorders (anorexia nervosa, bulimia nervosa, and binge eating disorder), substance use disorders (alcohol abuse/dependence, drug abuse/dependence). Definitions of all psychiatric disorders adhered to DSM-IV criteria.
Parents provided supplementary diagnostic information for the following subset of disorders: MDD, dysthymic disorder, ODD, CD, and ADHD. Similar to past analyses of the NCS-A, parent and adolescent reports of ODD and CD symptoms were combined if either endorsed the disorder, whereas only parent reports of ADHD symptoms were used to generate diagnoses due to the high frequency of under-reporting and consequent lack of validity of adolescent reports for this disorder (Kessler et al. 2012). Parent reports were incorporated for CD and ODD diagnoses because they have previously been found to be necessary to inform impairment associated with behavior disorders (Johnston and Murray 2003).
Definition of Bipolar Disorder and Treatment Utilization
DSM-IV criteria were applied to define bipolar I and II disorders. Bipolar disorder not otherwise specified and cyclothymia were not included as they were not assessed in the NCS-A. As parents did not report symptoms of mania or hypomania, diagnoses of bipolar disorder are based on adolescent report of mania and depression from the adolescent interview. Details regarding the wording of screening probes and percentage of participants endorsing each probe are described elsewhere (Merikangas et al. 2012). Among adolescents with euphoria or elevated mood, symptomatic criteria for mania/hypomania were fulfilled if at least three of seven mania symptoms were endorsed. For adolescents who endorsed irritability only, four of seven mania symptoms were required for a diagnosis of mania/hypomania. Duration of episodes and impairment ratings were used to distinguish manic from hypomanic episodes. A diagnosis of bipolar I was made if adolescents endorsed mania, with or without a depressive episode. A diagnosis of bipolar II was made if adolescents endorsed hypomania and a major depressive episode. Although bipolar symptoms were not externally validated by parent report, a subsequent clinical reappraisal study found a high degree of concordance between bipolar I and II disorders (κ = 0.70, SE = 0.1) derived from the adolescent CIDI as compared with a clinical diagnostic interview of parents and youth (Kessler et al. 2009c).
Treatment information was collected in the adolescent CIDI mania and depression modules and the service use modules in both the adolescent CIDI and the parent self-administered questionnaire. Each adolescent reported separately whether they had received treatment for mania, and whether they had received treatment for depression. The mania treatment question was: “Did you ever in your life talk to a medical doctor or other professional about your being very (excited and full of energy/irritable or grouchy)?” The depression treatment question was: “Did you ever in your life talk to a medical doctor or other professional about your (sadness/or discouragement/or boredom)?” Adolescents who endorsed either of the above questions were considered as having treatment for depression or mania.
If adolescents did not endorse any treatment in the depression and mania modules but endorsed any mental health specialty treatment in the service use module, they were classified as being a part of the treatment for other disorders group. In addition, if adolescents did not endorse treatment in the depression and mania modules, but their parents endorsed any mental health specialty treatment in the parent service use module, participants were also classified as being part of the treatment for other disorders group. Mental health specialty treatment was defined as a psychiatrist in settings such as a mental health clinic, drug or alcohol clinic, and admission to hospitals and other treatment facilities, or treatment by other mental health professionals like psychologists, social workers, or family counselors. Therefore, only adolescent report of treatment was used to classify the bipolar treatment group, while both adolescent and parent endorsement of mental health specialty treatment outside of the context of treatment for mania or depression was used to classify the treatment for other disorders group. The no treatment group was defined as answering no to all of aforementioned treatment questions.
Data Analysis
We report rates of sociodemographic characteristics, categorical clinical correlates and the means of continuous clinical correlates, and rates of comorbid disorders by the treatment groups. Linear regression was used to study the association between continuous outcomes (age of onset, number of mania episodes, number of mania symptoms, and severity of mania symptoms) and treatment groups. Odds ratios (OR) and their 95 % confidence intervals (C.I.) were derived from logistic regression analyses to assess the associations between dichotomous outcomes and treatment groups. Subgroup comparisons included depression or mania treatment versus treatment for other disorders, depression or mania treatment versus no treatment, and treatment for other disorders versus no treatment. In order to address concern regarding multiple tests, we also report the results after adjustment for the false discovery rate (Benjamini and Hochberg 1995).
Due to the weighting and clustering used in the NCS-A design, all statistical analyses were performed using the Taylor series linearization method, a design-based method implemented in SUDAAN (version 10.0; RTI International, Research Triangle Park, NC). Statistical significance was evaluated using a 2-sided design based test at the 0.05-level.
Results
Prevalence of Treatment Use
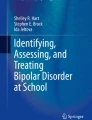
Rates of treatment for adolescents with bipolar disorder are presented in Fig. 1. A total of 250 participants met criteria for bipolar I or II disorder. As is shown, only 49 % of adolescents with bipolar disorder were treated for depression or mania (of those, 35.1 % for mania only, 27.4 % for depression only, and 37.5 % for both depression and mania). Approximately 13 % of adolescents with bipolar disorder were treated for conditions other than depression or mania, and 38 % of adolescents with bipolar disorder received no treatment at all. Subsequent analyses examine demographic and clinical correlates of service use among youth with lifetime bipolar disorder (N = 250) by the three index disorder treatment groups: mania and/or depression (n = 115); other non-affective disorder (n = 38); and no treatment (n = 97).

Lifetime treatment rates among U.S. adolescents with bipolar disorder (N = 250)
The sociodemographic characteristics of each treatment group are displayed in Table 1. There were no significant sex differences among the three groups. There was a direct association of treatment for depression or mania with age, such that approximately 45 % of 13–16 year olds received treatment for bipolar disorder, compared to 61 % of 17–18 year olds, p = 0.011. Non-Hispanic Blacks with bipolar disorder received less treatment for other psychological concerns than did the non-Hispanic White group (2.8 % vs. 15.8 %, p = 0.005).
Clinical Correlates of Treatment Use
Table 2 presents the clinical correlates of bipolar disorder by index disorder treatment subgroups. While no differences in ages of onset, number of mania episodes, or severity of mania symptoms were found, those adolescents who had treatment for depression or mania had significantly more mania symptoms (p = 0.005) and days out of role (OR = 4.7, 95 % CI [1.8, 12.4], p = 0.001) relative to those who did not receive any treatment. Days out of role refers to the number of days in the previous 12 months participants were unable to perform their usual activities as a result of their symptoms. Despite differences in the number of days out of role, it is important to note that all three groups reported a minimum of 27 days out of role in the past calendar year. Adolescents who received treatment for depression or mania were much more likely to have a history of suicide attempts or ideation relative to those who received treatment for other disorders (OR = 11.1, 95 % CI [2.4, 50.8], p = 0.001 and OR = 3.9, 95 % CI [1.8, 8.4], p < 0.001, respectively) and those who received no treatment (OR = 12.8, 95 % CI [2.5, 65.5], p = 0.002 and OR = 3.8, 95 % CI [1.2, 12.0], p = 0.019, respectively). Analyses showed no significant differences with regard to the level of disability experienced by members of all three groups.
Data regarding the service sectors and medications utilized by subgroups are also shown in this table. Adolescents treated for bipolar disorder utilized general medical, human services, and school services more than those who received no treatment (OR = 13.9, 95 % CI [3.1, 63.5], p = 0.001; OR = 2.9, 95 % CI [1.0, 8.8], p = 0.049; and OR = 4.9, 95 % CI [2.0, 12.1], p = 0.001, respectively). These adolescents who were treated for bipolar disorder also used human services and medications more than adolescents treated for other disorders (OR = 7.7, 95 % CI [1.6, 37.6], p = 0.010 and OR = 10.8, 95 % CI [1.3, 91.9], p = 0.005, respectively). Finally, school services were used more frequently by adolescents treated for non-bipolar disorders relative to those who had not received no treatment (OR = 3.0, 95 % CI [1.1, 8.2], p = 0.028).
Patterns of Comorbidity
Patterns of comorbidity by the index disorder treatment subgroups are presented in Table 3. Significant differences concerning lifetime rates of comorbid disorders were found only for the externalizing disorders and alcohol use. Rates of ADHD were approximately triple for the bipolar treatment group (28.6 % [SE = 6.5 %]) and the treatment for other disorders group (34.4% [SE = 6.4 %]) relative to the no treatment group (10.2% [SE = 5.2 %]), (OR = 4.3, 95 % CI [1.1, 16.7], p = 0.030 and OR = 4.1, 95 % CI [1.3, 12.5], p = 0.011, respectively).
Rates of alcohol use were about triple for the bipolar treatment group (35.0 % [SE = 8.0 %]) relative to the no treatment group (9.3 % [SE = 3.8 %]), (OR = 5.4, 95 % CI [1.7, 17.1], p = 0.004). Significant differences were not found when comparing the treatment for other disorders group to the no treatment group. Additionally, approximately double the number of adolescents in both treatment groups met criteria for behavior disorders (CD or ODD) in addition to their mood problems relative to the no-treatment group (57.9 %, [SE = 6.7 %] and 53.8 % [SE = 9.4 %] versus 27.0 % [SE = 6.9 %]). Both of these differences were significant (OR = 3.9, 95 % CI [1.5, 9.9], p = 0.004 and OR = 3.4, 95 % CI [1.3, 8.7], p = 0.009, respectively). A large proportion of adolescents treated for depression or mania and those treated for other disorders used services for attention or behavior problems as well. Among treated adolescents, between 32.2 % and 46.1 % were also treated for ADHD, CD or ODD.
The proportion of adolescents in the bipolar treatment group with comorbid conditions was higher than the proportion of adolescents in the no treatment group who had comorbid disorders. More adolescents treated for bipolar disorder had one or more additional classes of comorbid disorders versus no additional classes of comorbid disorders relative to adolescents with bipolar disorder who were not treated (OR = 5.0, 95 % CI [1.6, 15.9], p = 0.005). Additionally, more adolescents treated for bipolar disorder had more than two additional classes of comorbid disorders versus one or no additional classes of comorbid disorders relative to adolescents with bipolar disorder who were not being treated (OR = 6.5, 95 % CI [2.8, 15.3], p < 0.001).
All of the analyses indicated above were repeated after including parental report of depression treatment (parents did not report on mania treatment), and the findings were nearly identical. The prevalence, clinical correlates, and patterns of comorbidity in this sample thus remained stable regardless of whether adolescents in isolation or both adolescents and their parents provided reports of treatment utilization for depression.
The analyses were also repeated with adjustment for the false discovery rate, after which several results were no longer statistically significant. Please refer to the footnotes in Tables 2 and 3 for additional details.
Treatment for Mania, Depression, or Both
Additional analyses (not shown) were conducted to examine those who had received treatment for bipolar disorder depending on whether they were treated for mania (n = 38), depression (n = 33), or both mood states (n = 44). Results indicated that significantly more males were treated for mania (57.2 % of males in the bipolar treatment group were treated for mania alone, p < 0.001) and significantly more females for depression (41.6 % of females in the bipolar treatment group were treated for depression alone, p = 0.005). No age or race differences among the treatment groups emerged. These findings should be interpreted with caution due to the small sample sizes.
Among adolescents treated for depression and mania, 90.6 % (SE = 9.2 %) experienced severe disability, compared to 84.4 % (SE = 7.6 %) of those treated for depression alone, and 73.4 % (SE = 10.7 %) of those treated for mania alone. Rates of suicidal ideation displayed a similar pattern: 83.0 % (SE = 7.6 %) of those treated for depression and mania had a history of suicidal ideation, compared to 50.5 % (SE = 14.0 %) of those treated for depression alone, and 38.8 % (SE = 11.2 %) of those treated for mania alone.
With regard to the prevalence of comorbid disorders, adolescents treated for both mania and depression and those treated for depression alone manifested more substance-use disorders (45.4 % [SE = 13.2 %] and 58.0 % [SE = 11.7 %] versus 38.4 % [SE = 12.8 %]), and more alcohol use (32.0 % [SE = 12.1 %] and 47.2 % [SE = 14.2 %] versus 28.7 % [SE = 12.8 %]) relative to those being treated solely for mania. Adolescents treated for both mania and depression and those treated for mania alone had been treated more often for problems related to ADHD (38.1 % [SE = 11.2 %] and 45.2 % [SE = 12.0 %] versus 9.6 % [SE = 7.3 %]) than those adolescents being treated for depression alone. Adolescents who received treatment for both mania and depression had been treated more often for problems related to CD/ODD than those treated for mania alone (17.8 % [SE = 6.0 %] versus 14.3 % [SE = 10.9 %]) and depression alone (17.8 % [SE = 6.0 %] versus 4.9 % [SE = 4.8 %]). Finally, between 70.7 % and 81.8 % of adolescents in all three treatment groups had two or more additional classes of comorbid disorders versus one or no additional classes of comorbid disorders.
Discussion
Our findings confirm those of previous community studies that demonstrate that a substantial proportion of youth with bipolar disorder do not receive treatment. Of youth with bipolar disorder, 49.0 % report treatment specifically for mood disorder symptoms, 12.8 % report treatment for other mental health problems, and 38.2 % report no mental health treatment. These rates are similar to those found in previous community studies of the U.S. and Canada that yielded treatment rates of 56 % and 46 %, respectively (Lewinsohn et al. 2003; Kozloff et al. 2010). As our definition of treatment for depression and mania was relatively broad, these low rates are even more striking. Our results also reveal that a sizeable portion (13 %) of those adolescents with bipolar disorder who did utilize mental health services received treatment for comorbid conditions such as ADHD or a behavior disorder rather than for their mood-related symptoms. Finally, we found that as expected, youth with severe manifestations and consequences of bipolar disorder were more likely to receive mental health services.
Adolescents with bipolar disorder who had been treated for depression or mania tended to have significantly more indicators of severity, including more suicide attempts, more mania symptoms, a greater number of days out of role, and more comorbid ADHD, behavior disorders and alcohol use relative to those who had received no treatment. They also had a greater number of different classes of comorbid disorders than those who had not received treatment. These findings confirm those of prior clinical studies, which have demonstrated that the majority of youths treated for bipolar disorder are diagnosed with comorbid conditions (Evans-Lacko et al. 2011; Olfson et al. 2009). In general, treated children and adolescents tend to be more severely disturbed and to have more extensive symptomatology than those who do not receive treatment (Angold et al. 2000; Farmer et al. 1999; Zwaanswijk et al. 2003a). Thus, samples of adolescents with bipolar disorder identified in treatment settings are more likely to have comorbid disorders and show higher levels of severity and symptomatology than adolescents with bipolar disorder in the general population.
Regardless of this pattern, however, a large proportion of adolescents with bipolar disorder do not obtain specialty evaluation and treatment specifically for manic or depressive episodes. It is therefore important to identify the characteristics of these youth in order to develop strategies to facilitate appropriate evaluation and treatment. Similar to Costello et al. (2007) and Farmer et al. (1999), our results demonstrate that bipolar disorder was far more likely to be treated among older than younger adolescents, likely because of greater comorbidity and severity. This finding is of particular importance for prevention in that early recognition and intervention for manic episodes may lead to the prevention of secondary disorders like substance use (Merikangas et al. 2008). Examining the relationship between age and patterns of treatment seeking and response in epidemiological samples is particularly crucial given recent evidence from nationally representative samples of potentially differentiable developmental trajectories of bipolar disorder (Cicero et al. 2009). The finding that more persistent bipolar disorder is associated with seeking treatment for manic symptoms in epidemiological samples (Cicero et al. 2009) underscores the difficulty of assessing bipolar symptomatology and course in clinical samples.
Our finding confirms those of prior studies regarding the increased recognition and treatment of mania in males (Duax et al. 2007) and depression in females (Duax et al. 2007; Olfson et al. 2009). These differences may be attributable to referral bias as well as to sex differences in the prominence of symptoms that lead to referral for bipolar disorder, such as externalizing symptoms exhibited by males and internalizing symptoms exhibited by females (Duax et al. 2007; Merikangas et al. 2010, 2012).
Analyses of other health services used by adolescents with bipolar disorder revealed that those treated for depression or mania utilized general medical, human services, and school services more than those who had not received treatment, and human services and medications more than adolescents treated for other disorders. These patterns confirm past research that has shown that the education sector is a very common and important point of entry and provider of services among youth (Farmer et al. 2003), and lend evidence to the idea that youth with bipolar disorder do not receive the most effective treatment unless the symptoms of their disorder are clearly recognized. Our investigation of the correlates of treatment seeking in adolescents adds to the literature on correlates of service use for bipolar disorder in younger children (Horwitz et al. 2012).
These findings highlight the differences in the demographic and clinical characteristics of youth with bipolar disorder who receive services compared to those who do not. Adolescents with bipolar disorder identified in clinical samples are not representative of those with bipolar disorder in the general population. A recent meta-analysis demonstrating that rates of bipolar disorder in population based studies of youth have remained stable (Van Meter et al. 2011) despite increasing rates in clinical samples of youth (Moreno et al. 2007) provides further evidence of the unrepresentative nature of youth seeking treatment for bipolar disorder. These findings suggest that caution should be exerted when generalizing from such samples to bipolar disorder in general, particularly regarding patterns of comorbidity, impairment, and disability that may lead to referral to specialty settings as well as the recognition of bipolar disorder among youth. This is of particular concern because the vast majority of research on biological pathways, treatment, and phenomenology is derived from non-systematic, clinical samples that may not generalize to the full spectrum of bipolar disorder in youth.
Strengths and Limitations
Some limitations of this study should be considered in interpreting the findings. The cross-sectional nature of the survey limits our ability to document temporal ordering of mental disorders and putative risk and protective factors. In addition, assessment of lifetime disorders was based on retrospective recall that is subject to numerous types of bias. Although we used a number of methods to increase the validity of retrospective reports (Kessler and Merikangas 2004), it is unlikely that we were able to completely correct for retrospective recall bias.
Furthermore, the assessment of mania and depression symptoms was based solely on the report of the adolescent without the external validation provided by parental report. Past studies have found that parent report of bipolar symptoms has greater diagnostic validity than adolescent report, likely due to compromised insight of behavior associated with mania and adolescents’ delayed tendency to perceive manic symptoms as problematic compared to those around them (Youngstrom et al. 2004a, b, 2009). This limitation was partially offset, however, by the agreement between the CIDI and K-SADS interviews for bipolar disorder in our clinical reappraisal study (Kessler et al. 2009c). Additionally, the reported findings appear to be relatively stable, as they were nearly identical when repeated after including parental report of depression treatment.
Finally, we do not have information about the chief complaint that led to treatment seeking, so we could not distinguish whether clinicians made a bipolar disorder diagnosis after referral for services for other disorders, such as ADHD, or specifically for symptoms of mania or depression. Therefore, we cannot draw inferences about the precise pathways through treatment taken by adolescents with bipolar disorder.
Regardless of these limitations, however, this is the first study to examine treatment patterns of adolescents with bipolar I and II disorder in a nationally representative sample of U.S. adolescents. These data demonstrate the biases present in clinical samples that may diminish the generalizability of findings based on such samples. Our data also highlight the importance of comprehensive evaluation of mania as well as the spectrum of mania in adolescents presenting for treatment, irrespective of the chief indication for referral. Future longitudinal analyses of bipolar adolescents in a nationally representative sample can help to further our understanding of treatment patterns in this important group.
References
Angold, A., Costello, E. J., Burns, B. J., Erkanli, A., & Farmer, E. M. (2000). Effectiveness of nonresidential specialty mental health services for children and adolescents in the “real world”. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 154–160. doi:10.1097/00004583-200002000-00013.
Beesdo, K., Hofler, M., Leibenluft, E., Lieb, R., Bauer, M., & Pfennig, A. (2009). Mood episodes and mood disorders: patterns of incidence and conversion in the first three decades of life. Bipolar Disorders, 11, 637–649. doi:10.1111/j.1399-5618.2009.00738.x.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B Methodological, 57, 289–300. doi:10.1016/S0166-4328(01)00297-2.
Castilla-Puentes, R. (2008). Multiple episodes in children and adolescents with bipolar disorder: comorbidity, hospitalization, and treatment (data from a cohort of 8,129 patients of a national managed care database). International Journal of Psychiatry in Medicine, 38, 61–70. doi:10.2190/PM.38.1.f.
Cicero, D. C., Epler, A. J., & Sher, K. J. (2009). Are there developmentally limited forms of bipolar disorder? Journal of Abnormal Psychology, 118, 431. doi:10.1037/a0015919.
Costello, E., Copeland, W., Cowell, A., & Keeler, G. (2007). Service costs of caring for adolescents with mental illness in a rural community, 1993–2000. American Journal of Psychiatry, 164, 36–42. doi:10.1176/appi.ajp.164.1.36.
Duax, J. M., Youngstrom, E. A., Calabrese, J. R., & Findling, R. L. (2007). Sex differences in pediatric bipolar disorder. Journal of Clinical Psychiatry, 68, 1565–1573. doi:10.4088/JCP.v68n1016.
Evans-Lacko, S. E., dosReis, S., Kastelic, E., & Riley, A. W. (2011). Mental health service use before and after diagnosis of early-onset bipolar disorder. Journal of Behavioral Health Services & Research, 38, 398–413. doi:10.1007/s11414-010-9225-8.
Farmer, E. M., Burns, B. J., Phillips, S. D., Angold, A., & Costello, E. J. (2003). Pathways into and through mental health services for children and adolescents. Psychiatric Services, 54, 60–66. doi:10.1176/appi.ps.54.1.60.
Farmer, E. M., Stangl, D. K., Burns, B. J., Costello, E. J., & Angold, A. (1999). Use, persistence, and intensity: patterns of care for children’s mental health across one year. Community Mental Health Journal, 35, 31–46. doi:10.1023/A:1018743908617.
Goldstein, B. I., & Birmaher, B. (2012). Prevalence, clinical presentation and differential diagnosis of pediatric bipolar disorder. The Israel Journal of Psychiatry and Related Sciences, 49, 3–14.
Horwitz, S., Demeter, C., Hayden, M., Storfer-Isser, A., Frazier, T. W., Fristad, M. A., & Findling, R. L. (2012). Parents’ perceptions of benefit of children’s mental health treatment and continued use of services. Psychiatric Services, 63, 793–801. doi:10.1176/appi.ps.201100460a.
Johnston, C., & Murray, C. (2003). Incremental validity in the psychological assessment of children and adolescents. Psychological Assessment, 15, 496. doi:10.1037/1040-3590.15.4.496.
Kessler, R. C., Avenevoli, S., Costello, E. J., Green, J. G., Gruber, M. J., Heeringa, S., & Zaslavsky, A. M. (2009a). Design and field procedures in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). International Journal of Methods in Psychiatric Research, 18, 69–83. doi:10.1002/mpr.279.
Kessler, R. C., Avenevoli, S., Costello, E. J., Green, J. G., Gruber, M. J., Heeringa, S., & Zaslavsky, A. M. (2009b). National comorbidity survey replication adolescent supplement (NCS-A): II. Overview and design. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 380–385. doi:10.1097/CHI.0b013e3181999705.
Kessler, R. C., Avenevoli, S., Green, J., Gruber, M. J., Guyer, M., He, Y., & Zaslavsky, A. M. (2009c). National Comorbidity Survey Replication Adolescent Supplement (NCS-A): III. Concordance of DSM-IV/CIDI diagnoses with clinical reassessments. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 386–399. doi:10.1097/CHI.0b013e31819a1cbc.
Kessler, R. C., Avenevoli, S., McLaughlin, K., Green, J. G., Lakoma, M., Petukhova, M., & Merikangas, K. R. (2012). Lifetime co-morbidity of DSM-IV disorders in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Psychological Medicine, 42, 1997–2010. doi:10.1017/S0033291712000025.
Kessler, R. C., & Merikangas, K. R. (2004). The National Comorbidity Survey Replication (NCS-R): background and aims. International Journal of Methods in Psychiatric Research, 13, 60–68. doi:10.1002/mpr.166.
Kessler, R. C., & Ustun, T. B. (2004). The World Mental Health (WMH) Survey Initiative version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). International Journal of Methods in Psychiatric Research, 13, 93–121.
Kozloff, N., Cheung, A. H., Schaffer, A., Cairney, J., Dewa, C. S., Veldhuizen, S., & Levitt, A. J. (2010). Bipolar disorder among adolescents and young adults: results from an epidemiological sample. Journal of Affective Disorders, 125, 350–354. doi:10.1016/j.jad.2010.02.120.
Lewinsohn, P. M., Seeley, J. R., & Klein, D. N. (2003). Bipolar disorders during adolescence. Acta Psychiatrica Scandinavica. Supplementum, 108, 47–50. doi:10.1034/j.1600-0447.108.s418.10.x.
Merikangas, K. R., Avenevoli, S., Costello, J., Koretz, D., & Kessler, R. C. (2009). National Comorbidity Survey Replication Adolescent Supplement (NCS-A): I. Background and measures. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 367–369. doi:10.1097/CHI.0b013e31819996f1.
Merikangas, K. R., Cui, L. H., Kattan, G., Carlson, G. A., Youngstrom, E. A., & Angst, J. (2012). Mania with and without depression in a community sample of US adolescents. Archives of General Psychiatry, 69, 943–951. doi:10.1001/Archgenpsychiatry.2012.38.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., & Cui, L. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49, 980–989. doi:10.1016/j.jaac.2010.05.017.
Merikangas, K. R., He, J. P., Burstein, M., Swendsen, J., Avenevoli, S., & Case, B. (2011a). Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 50, 32–45. doi:10.1016/j.jaac.2010.10.006.
Merikangas, K. R., Herrell, R., Swendsen, J., Rossler, W., Ajdacic-Gross, V., & Angst, J. (2008). Specificity of bipolar spectrum conditions in the comorbidity of mood and substance use disorders: results from the Zurich cohort study. Archives of General Psychiatry, 65, 47–52. doi:10.1001/archgenpsychiatry.2007.18.
Merikangas, K. R., Jin, R., He, J. P., Kessler, R. C., Lee, S., Sampson, N. A., & Zarkov, Z. (2011b). Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Archives of General Psychiatry, 68, 241–251. doi:10.1001/archgenpsychiatry.2011.12.
Moreno, C., Laje, G., Blanco, C., Jiang, H., Schmidt, A. B., & Olfson, M. (2007). National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Archives of General Psychiatry, 64, 1032–1039. doi:10.1001/archpsyc.64.9.1032.
Olfson, M., Crystal, S., Gerhard, T., Huang, C. S., & Carlson, G. A. (2009). Mental health treatment received by youths in the year before and after a new diagnosis of bipolar disorder. Psychiatric Services, 60, 1098–1106. doi:10.1176/appi.ps.60.8.1098.
Peele, P. B., Axelson, D. A., Xu, Y., & Malley, E. E. (2004). Use of medical and behavioral health services by adolescents with bipolar disorder. Psychiatric Services, 55, 1392–1396. doi:10.1176/appi.ps.55.12.1392.
Post, R. M., Leverich, G. S., Kupka, R. W., Keck, P. E., Jr., McElroy, S. L., Altshuler, L. L., & Nolen, W. A. (2010). Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. The Journal of Clinical Psychiatry, 71, 864–872. doi:10.4088/JCP.08m04994yel.
Pumariega, A. J., Glover, S., Holzer, C. E., 3rd, & Nguyen, H. (1998). II. Utilization of mental health services in a tri-ethnic sample of adolescents. Community Mental Health Journal, 34, 145–156. doi:10.1023/A:1018788901831.
Rizzo, C. J., Esposito-Smythers, C., Swenson, L., Birmaher, B., Ryan, N., Strober, M., & Keller, M. (2007). Factors associated with mental health service utilization among bipolar youth. Bipolar Disorders, 9, 839–850. doi:10.1111/j.1399-5618.2007.00439.x.
Van Meter, A. R., Moreira, A., & Youngstrom, E. A. (2011). Meta-analysis of epidemiologic studies of pediatric bipolar disorder. The Journal of Clinical Psychiatry, 72, 1250–1256. doi:10.4088/JCP.10m06290.
Youngstrom, E. A., Findling, R. L., & Calabrese, J. R. (2004a). Effects of adolescent manic symptoms on agreement between youth, parent, and teacher ratings of behavior problems. Journal of Affective Disorders, 82, S5–S16. doi:10.1016/j.jad.2004.05.016.
Youngstrom, E. A., Findling, R. L., Calabrese, J. R., Gracious, B. L., Demeter, C., Bedoya, D. D., & Price, M. (2004b). Comparing the diagnostic accuracy of six potential screening instruments for bipolar disorder in youths aged 5 to 17 years. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 847–858. doi:10.1097/01.chi.0000125091.35109.1e.
Youngstrom, E. A., Freeman, A. J., & Jenkins, M. M. (2009). The assessment of children and adolescents with bipolar disorder. Child and Adolescent Psychiatric Clinics of North America, 18, 353–390. doi:10.1016/j.chc.2008.12.002. viii-ix.
Youngstrom, E. A., Jenkins, M. M., Doss, A. J., & Youngstrom, J. K. (2012). Evidence-based assessment strategies for pediatric bipolar disorder. The Israel Journal of Psychiatry and Related Sciences, 49, 15–27.
Zwaanswijk, M., Van der Ende, J., Verhaak, P. F. M., Bensing, J. M., & Verhulst, F. C. (2003a). Factors associated with adolescent mental health service need and utilization. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 692–700. doi:10.1097/01.CHI.0000046862.56865.B7.
Zwaanswijk, M., Verhaak, P. F., Bensing, J. M., van der Ende, J., & Verhulst, F. C. (2003b). Help seeking for emotional and behavioural problems in children and adolescents: a review of recent literature. European Child & Adolescent Psychiatry, 12, 153–161. doi:10.1007/s00787-003-0322-6.
Acknowledgments
This work was supported by the Intramural Research Program of the National Institute of Mental Health (Z01 MH002808-08). The National Comorbidity Survey Adolescent Supplement (NCS-A) and the larger program of related NCS surveys are supported by the National Institute of Mental Health (U01-MH60220). The views and opinions expressed in this article are those of the authors and should not be construed to represent the views of any of the sponsoring organizations, agencies, or U.S. Government.
Conflict of Interest
The authors do not have any commercial associations that might present a conflict of interest with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Khazanov, G.K., Cui, L., Merikangas, K.R. et al. Treatment Patterns of Youth with Bipolar Disorder: Results from the National Comorbidity Survey—Adolescent Supplement (NCS-A). J Abnorm Child Psychol 43, 391–400 (2015). https://doi.org/10.1007/s10802-014-9885-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-014-9885-6