
Abstract
The present study examined the role of early fathering in subsequent trajectories of social emotional and academic functioning of preschool children with behavior problems. Participants were 128 preschool-aged children (73 boys, 55 girls) with behavior problems whose biological fathers took part in a longitudinal study. Children were 3 years of age at the beginning of the study and were assessed annually for 3 years. Early paternal depressive symptoms predicted many aspects of children’s outcome 3 years later, including externalizing and internalizing problems, social skills deficits, and lower cognitive and academic functioning, and predicted changes in children’s externalizing, internalizing, and social problems across the preschool years. Paternal socioeconomic status (SES) also consistently predicted children’s later functioning across these domains. Furthermore, self-reported paternal attention-deficit hyperactivity disorder (ADHD) symptoms and laxness, as well as observed frequent commands were associated with later externalizing problems in children. Paternal depressive symptoms and laxness mediated the relation between paternal ADHD symptoms and child functioning. Results suggest that aspects of early father functioning play an important role in the psychosocial, cognitive, and academic development of preschool-aged children with behavior problems.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The last few decades have witnessed a growing interest in the role that fathers play in their children’s lives, but there remains a gross imbalance between research on mothers and research on fathers (Phares et al. 2005). There is a particular need to build on existing longitudinal studies of early fathering among preschool-aged children (Aldous and Mulligan 2002; DeKlyen et al. 1998; Eiden et al. 2009; Eiden et al. 2007; Keown 2012; Loukas et al. 2003; Martin et al. 2007, 2010; National Institute of Child Health and Human Development [NICHD] Early Child Care Research Network [ECCRN] 2004; Paulson et al. 2009; Ramchandani et al. 2005; Tamis-LeMonda et al. 2004; Trautmann-Villalba et al. 2006), given the methodological strengths of longitudinal designs over cross-sectional methods.
The existing body of longitudinal research on early fathering represents an important contribution to our field; however, most studies have focused on community samples. Research on community samples provides insights into variables that distinguish children with and without problems, but there is some evidence that these factors may differ from those that are important for improving preschool children’s subsequent functioning once they develop such problems (DeKlyen et al. 1998). Identifying which aspects of early fathering contribute to the subsequent functioning of preschool children with behavior problems has received scant attention, but is important for advancing theories of the early development of children with behavior problems and for informing early interventions. The present study seeks to address this gap, and focuses on three aspects of fathering that research with community samples suggests may be important: (a) fathers’ parenting practices, (b) fathers’ psychopathology, and (c) father involvement.
Fathers’ Parenting Practices
Longitudinal studies of preschool-aged children have found that fathers’ supportiveness (e.g., NICHD ECCRN 2004; Martin et al. 2007; Tamis-LeMonda et al. 2004), warmth (Eiden et al. 2009), and sensitivity (Keown 2012; Trautmann-Villalba et al. 2006) predict later positive child outcomes, whereas negative paternal parenting practices predict poorer child functioning (e.g., Keown 2012). Although fathers’ laxness has been linked with child functioning in school-aged children (Gryczkowski et al. 2010), cross-sectional studies that have examined the relation between fathers’ permissive parenting and preschoolers’ functioning have yielded conflicting results, with some finding support for a link with externalizing problems (Jewell et al. 2008) and others failing to find such a link (Keown 2011). Longitudinal studies of preschool-aged children have not examined the relation between early paternal laxness and children’s later functioning.
To our knowledge, only one longitudinal study has examined the role of fathers’ early parenting in children’s subsequent functioning among preschoolers with behavior problems. Among clinic-referred preschoolers, fathers’ use of harsh parenting was not predictive of later conduct problems, and fathers’ positive involvement was unexpectedly associated with more conduct problems, even though harsh parenting and positive involvement significantly distinguished clinic-referred from non-referred children in the expected direction (DeKlyen et al. 1998). Thus, although previous research suggests that fathers’ parenting may play an important role in children’s development, more research is needed to examine the role of fathers’ early parenting in the subsequent functioning of preschool children with behavior problems.
Fathers’ Psychopathology
Although paternal psychopathology has been identified as an important correlate of children’s maladjustment in cross-sectional research (see Kane and Garber 2004), few prospective studies have examined the link between fathers’ psychopathology during the preschool years and children’s later functioning. Early paternal depression has been linked to later internalizing and externalizing problems (Eiden et al. 2007; Ramchandani et al. 2005); paternal alcoholism has been associated with preschoolers’ subsequent externalizing problems and poor social competence (Eiden et al. 2007; 2009; Loukas et al. 2003); and fathers’ antisocial personality disorder has been linked with later externalizing problems (Eiden et al. 2007; 2009; Loukas et al. 2003). Although no prospective studies of preschoolers have examined whether paternal attention-deficit hyperactivity disorder (ADHD) symptoms predict children’s later functioning, paternal ADHD has been associated with children’s concurrent ADHD symptom severity among older children with ADHD (Takeda et al. 2010), and retrospective reports of paternal childhood ADHD symptoms have been linked with ADHD diagnoses in their children (Nigg and Hinshaw 1998). To our knowledge, only DeKlyen and colleagues (1998) have examined whether paternal psychopathology predicts subsequent functioning among preschool children with behavior problems. Although paternal psychopathology distinguished clinic-referred preschoolers from comparison children, the relation between a global measure of paternal psychopathology and later conduct problems did not quite reach significance among clinic-referred preschoolers, though the effect was medium-sized. More research is needed to examine distinct types of paternal psychopathology in a larger sample of preschoolers with behavior problems to more fully evaluate the potential role of paternal psychopathology in the development of preschool children with behavior problems.
Father Involvement
Father involvement has been linked with higher functioning in older children and adolescents (e.g., Flouri 2005); however, only a handful of studies have examined the link between father involvement and preschoolers’ development. These studies suggest that father involvement is associated with children’s well-being (e.g., Downer and Mendez 2005). Moreover, interventions to increase father involvement in preschoolers have been associated with improved child academic functioning (Fagan and Iglesias 1999). However, the few longitudinal studies of father involvement and young children’s well-being failed to find a link with children’s behavior problems (e.g., Aldous and Mulligan 2002). More research is needed to longitudinally examine the effects of early father involvement on later development among preschoolers.
Socioeconomic Status
Parental socioeconomic status (SES) has been shown to be a strong predictor of childhood psychopathology, particularly for externalizing behaviors (e.g., Wadsworth and Achenbach 2005). Low parental SES may contribute to child psychopathology by disrupting parenting or through exposure to stressful events (Egeland 1997). Because SES is also highly correlated with fathers’ functioning (Schindler 2010), a full examination of early fathering requires the consideration of the relation between paternal SES and child functioning.
Potential Moderators of the Relation Between Early Fathering and Child Outcome
A number of child characteristics may interact with fathering in predicting subsequent child outcome. For instance, there is some evidence that fathers may have different effects on their daughters than sons, though conflicting findings have been reported (e.g., Aldous and Mulligan 2002; Connell and Goodman 2002; Flouri 2005). In addition, according to differential susceptibility theory (Belsky and Pluess 2009), some children are more sensitive to their environment than others. It may be that children with psychological disorders are one such group of children, and may therefore be influenced more by fathers than are typically developing children.
Potential Mediators of the Relation Between Early Fathering and Child Outcome
Much of the research on early fathering has focused on simple relations between fathers’ characteristics and child outcomes. More research is needed to examine the mechanism underlying these relations. A number of studies suggest that parenting mediates the relation between maternal psychopathology and child outcome (e.g., Dietz et al. 2009), and a few studies suggest that this may be true for fathers as well (e.g., Paulson et al. 2009), though findings have been mixed (Eiden et al. 2007). In addition, evidence that ADHD places adults at risk for depression (Ramsay and Rostain 2008) together with evidence that depression is associated with poor child outcome (e.g., Eiden et al. 2007) suggests that depression may mediate the relation between paternal ADHD symptoms and child outcome. Research is needed to more fully evaluate these potential pathways for fathers of preschoolers.
The Present Study
The past decades have witnessed a growing recognition of the importance of fathers in their children’s development; however, important gaps remain. First, more longitudinal research is needed to examine how early fathering predicts subsequent child functioning. Second, understanding the role that fathers may play in helping preschool children with behavior problems follow positive trajectories is key for developing early interventions for these children. Finally, research is needed to examine meditational pathways by which early fathering contributes to child development, and to examine child characteristics that may moderate the effects of early fathering. The present study sought to examine how fathers’ parenting practices, psychopathology, involvement, and SES are associated with trajectories of child functioning, including internalizing problems, externalizing problems, social skills, academic achievement, and cognitive abilities. The following hypotheses were tested:
-
Question 1: Does early fathering predict trajectories of children’s internalizing problems, externalizing problems, and social skills? It was hypothesized that fathers’ parenting practices, psychopathology, involvement, and SES would predict externalizing and internalizing problem and social skills trajectories among 3-year-old children with behavior problems. It was expected that more effective parenting practices (greater warmth, lower overreactivity and laxness, and fewer commands), lower levels of paternal psychopathology (ADHD and depressive symptoms), and higher involvement and SES would predict fewer internalizing and externalizing problems and higher social competence 3 years later, and would be associated with greater improvement in these areas over time. We also predicted that gender and child ADHD/oppositional defiant disorder (ODD) would moderate the relation between early fathering and later child outcome.
-
Question 2: Does early fathering predict academic achievement and cognitive ability? It was hypothesized that more effective parenting practices, lower levels of paternal psychopathology, and higher involvement and SES would predict better academic achievement and cognitive ability 3 years later. Gender and ADHD/ODD status were also predicted to moderate the relation between early fathering and child outcome.
-
Question 3: What are the underlying mechanisms that mediate the relations between early fathering and later child outcome? It was predicted that (a) fathers’ early parenting practices would mediate the relations between fathers’ early psychopathology and child outcome, and (b) paternal depressive symptoms would mediate the relations between paternal ADHD symptoms and child outcome.
Method
Participants
Participants were drawn from a sample of 199 children who took part in a longitudinal study of preschool-aged children with behavior problems. Children (N = 128; 73 boys) whose biological fathers participated at the first time point were included in this study. Children were 3 years of age at screening and were 36 to 50 months of age (M = 44.36, SD = 3.30) at the first home visit (T1). Data were collected at 1-year (T2), 2-year (T3), and 3-year (T4) follow-up visits. The average age at T4 was 80.31 months (SD = 4.68). The sample included European American (63.30 %), Latino American (14.10 %; mostly Puerto Rican), African American (8.60 %), and multiethnic (14.10 %) children. The median family income at T1 was $50,500. Ten percent of fathers had less than 12 years of education, 48 % had a high school education, 12 % had some college education, and 30 % had at least a bachelor’s degree. Fathers’ average age was 36.31 years (SD = 7.43). Most children (n = 118) were from two-parent families. Ten fathers did not live with their children full-time, but spent time with their children on a regular basis (at least 5 h per week).
Procedure
Children with significant externalizing problems were recruited from a sample of 3-year-old children (N = 1,752) whose parents completed a screening packet that they received through mail (via state birth records), pediatrician offices, child care centers, and community centers. A smaller group of non-problem children were also recruited but are not the focus of this study. Inclusion criteria were (a) no evidence based on parent report of mental retardation, deafness, blindness, language delay, cerebral palsy, epilepsy, autism, or psychosis; (b) parent-reported concern about the child’s activity level, defiance, aggression, or impulse control; and (c) Behavior Assessment System for Children–Parent Report Scale (BASC-PRS; Reynolds and Kamphaus 1992) Hyperactivity and/or Aggression subscale T scores at or above 65. Families were paid for their participation. Fifty-nine percent of behavior problem children whom we sought to recruit participated. Written informed consent was obtained from all parents who participated. The study was conducted in compliance with the authors’ Institutional Review Board.
Measures
Paternal SES
Fathers’ number of years of education and family income at T1 were standardized and averaged to create a single measure of SES.
Paternal Depressive Symptoms
The Center for Epidemiological Studies Depression scale (CES-D; Radloff 1977) is a 20-item measure of adult depressive symptomatology. Fathers rated themselves on a scale from 0 (rarely or none of the time) to 3 (most or all of the time), and responses were averaged across the 20 items. The scale has excellent internal consistency and good validity (Radloff 1977). For this sample, the scale demonstrated good internal consistency (α = 0.88). Fathers’ CES-D scores ranged from 0 to 2.35 and 19 % (n = 24) fell in the clinically significant range (scored 16 or higher using a sum of the 20 items).
Paternal Self-Reported Adult ADHD Symptoms
The Current Symptoms Scale contains 18 items corresponding with the DSM-IV symptoms for ADHD (Barkley and Murphy 1998). Fathers rated each symptom on a scale from 0 (never or rarely) to 3 (very often), and responses were averaged across the 18 items. For this sample, the scale demonstrated good internal consistency (α = 0.84). Five fathers (4 %) showed clinically significant ADHD symptomatology (endorsed a 2 or 3 on at least 6 symptoms of either hyperactivity or inattention). The scores on the scale ranged from 0 to 1.97.
Father Involvement
The Child Care Tasks scale is a 10-item measure that assesses father involvement, adapted from a scale developed by Baruch and Barnett (1986). Fathers indicated the percentage of time they engaged in various daily tasks (e.g., supervising your child’s morning routine, taking your child to and from activities, playing with your child) relative to mothers, and these were averaged across the 10 childcare tasks. The measure has demonstrated good reliability and validity (Baruch and Barnett 1986). For this sample, the scale demonstrated good internal consistency (α = 0.89).
Parenting Practices
The Parenting Scale (Arnold et al. 1993) is a 30-item self-report scale, which yields scores for laxness (e.g., “When I say my child can’t do something, I let my child do it anyway”) and overreactivity (e.g., “When my child misbehaves, I get so frustrated or angry that my child can see I’m upset”). Items are rated on a 7-point Likert scale. Scores were calculated by averaging across items that loaded on each factor according to the Arnold et al. (1993) factor structure, where high scores indicate dysfunctional parenting. The Parenting Scale has demonstrated good internal consistency, good test-retest reliability, and has been found to correlate with observations of parenting and child behavior (Arnold et al. 1993). For this sample, the scale demonstrated good internal consistency for laxness (α = 0.76) and overreactivity (α = 0.75). To explore the validity of this scale, paternal overreactivity and laxness scores in this sample were compared to scores for nonproblem children who were recruited as part of the larger study. Fathers’ overreactivity and laxness were both significantly higher in the present sample than in the nonproblem sample, ps < 0.05.
Audiotaped Assessment of Parenting
Fathers were asked to use a microcassette player to record 2 h of interaction with their children during a time that tended to be challenging. A preliminary review of the tapes suggested that 30 min of tape was sufficient for capturing a wide variety of behavior that was representative of the entire 2 h, and all parents who were willing to take part in this assessment completed at least 30 min. The first 15 min of each side of one tape was coded. Graduate and undergraduate research assistants were trained to code the audiotapes and two raters overlapped for 30 % of fathers’ tapes. In this study, codes for father warmth and commands were used. Warmth referred to using praise, encouragement, and terms of endearment; conveying affection; being supportive, available, open, and positive; and having a cheerful tone. Commands were defined as statements made by the father that directly instruct the child to do or not to do something. Global ratings of father warmth (intraclass correlation [ICC] = 0.73) were made every 5 min and ranged from 1 (not warm) to 7 (extremely warm). Warmth ratings were then averaged across 5 min segments to create a single warmth score for each participant. An event based code was used to count the frequency with which fathers issued commands to their children (ICC = 0.85). To explore the validity of these measures, paternal warmth and command scores in this sample were compared to scores for nonproblem children. Fathers’ warmth was significantly higher in the present sample than in the nonproblem sample, p < 0.05, but fathers’ frequency of commands did not significantly differ, p = 0.44.
Child Internalizing and Externalizing Problems
Because mothers had more complete data on their reports of child behavior, and in order to limit the effects of method variance (since father reports were used for predictors), mothers’ BASC-PRS externalizing and internalizing T scores were used at all time points. Mothers’ and fathers’ reports of behavior were significantly correlated, ranging from 0.55 to 0.62 across time for both internalizing and externalizing problems, ps < 0.001. The BASC-PRS has demonstrated excellent internal consistency for both the internalizing and externalizing scales (α = 0.87 and 0.89, respectively, for the child version and 0.86 and 0.89 for the preschool version) and good convergent validity with the Child Behavior Checklist internalizing and externalizing scales (Reynolds and Kamphaus 1992).
Child Social Skills
The Social Skills scale of the mother-completed BASC-PRS was used to assess social functioning at T1, T2, T3, and T4. This scale has demonstrated strong internal consistency (α = 0.89; Reynolds and Kamphaus 1992). Mothers’ and fathers’ reports of behavior were significantly correlated, ranging from 0.42 to 0.50 across time, all ps < 0.001.
Cognitive Ability
Cognitive ability was measured using the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV; Wechsler 2003) at T4. The Full Scale IQ derived from 10 core subtests was used to measure each child’s cognitive ability. The WISC-IV demonstrates excellent internal consistency (α = 0.97) and test-retest reliability (r = 0.93; Wechsler 2003).
Academic Achievement
Academic achievement was measured using the Wechsler Individual Achievement Test, Second Edition-Abbreviated (WIAT-II-A; The Psychological Corporation 1992) at T4. The WIAT-II-A consists of three subtests—word reading, numerical operations, and spelling—and demonstrates good internal consistency at age 6 (α = 0.97; The Psychological Corporation 1992). The overall composite score was used.
T4 Diagnoses
Clinicians who conducted the T4 home visits assigned diagnoses of ADHD and ODD based on a T4 diagnostic interview and parent and teacher completed rating scales (see Harvey et al. 2011, for more detail). Clinicians were all clinical or school psychology graduate students who had taken graduate courses on child assessment and who were trained by the second author to conduct these clinical assessments. A second clinician reviewed T4 materials and made independent diagnoses. Discrepancies were discussed and a consensus diagnosis was reached. Kappa was 0.78 for ADHD and 0.75 for ODD. Of the 111 behavior problem children in this study who completed T4, 23 met criteria for ADHD only, 13 for ODD only, and 22 for ADHD and ODD.
Data Analyses
MPlus (Muthén and Muthén 1998–2010) was used to examine the relation between fathers’ characteristics and children’s externalizing problems, internalizing problems, social skills, cognitive skills, and academic skills. We provide an overview of the analytic plan here and specific details in the results section. To estimate trajectories for BASC-PRS scores, latent growth curve models were used, which yield estimates of T4 outcome as well as estimates of change over time. These two estimates were regressed on each fathering variable one at a time to address Question 1. Question 2 was addressed by regressing T4 cognitive and academic measures on each fathering variable one at a time. The moderating role of child gender and ADHD/ODD diagnoses was assessed by repeating analyses for Question 1 and 2 using multigroup analyses. Finally, path modeling was used to test meditational hypotheses for Question 3. Although children varied somewhat in age, children’s age in months at T1 did not significantly predict any of the outcome variables, so it was not included in subsequent models. Full Information Maximum Likelihood, which uses all observed information (including from cases with some missing data) was used to estimate parameters.
Results
Descriptive Statistics
Intercorrelations and descriptive statistics for predictor and outcome variables are presented in Tables 1 and 2.
Unconditional Growth Models
Unconditional growth models were first used to estimate the rate of change over time and level at T4 for externalizing problems, internalizing problems, and social skills. For each outcome variable, three latent growth factors (intercept, linear, and quadratic) were estimated based on the four data points for each outcome variable and on four time variables representing the child’s age at each time point. If the quadratic factor was not significant and did not show significant variability, it was dropped from the model. In these models, the intercept is defined as the level of the outcome when time is zero. Therefore, centering time at a given time point allows one to estimate the level of the outcome variable at that time point using the intercept. To predict T4 child functioning levels, T4 Models were constructed in which time was centered at T4 (set to 0 at T4; calculated by subtracting T4 age from child age in years [months/12] at each time point) so that the intercept represented T4 outcome level. The linear growth factor represents the linear rate of change (slope) over time. If the quadratic factor is included in the model, the linear slope changes over time, and the estimate that is provided by the model represents the instantaneous linear rate of change at the time point at which the time variable is centered. If the quadratic factor is not included in the model, the linear growth factor represents the average linear change over time. To predict linear change in child functioning, T1 Models were constructed in which time was centered at T1 (child age minus T1 age). Predicting the linear rate of change estimated from T1 Models allows one to examine predictors of linear change, controlling for initial symptom levels (estimated by the intercept in the T1 Models). This is important because children’s rate of change may vary as a function of their initial symptom level.
The average of the quadratic growth factor (representing curvature in trajectories) was not significantly different from zero for externalizing problems (β = 0.01, SE = 0.31, p = 0.97), internalizing problems (β = −0.01, SE = 0.33, p = 0.98), or social skills (β = −0.15, SE = 0.28, p = 0.60); however, there was significant variability in the quadratic term for internalizing problems, σ 2 = 3.24, SE = 0.92, p < 0.001, and social skills, σ 2 = 4.85, SE = 1.54, p = 0.002, so the quadratic growth factor was retained for internalizing problems and social skills. The average linear growth factor was significantly different from zero for externalizing problems (β = −1.60, SE = 0.33, p < 0.001), indicating that the average externalizing score decreased over time. The average linear growth factor was not significantly different from zero for internalizing problems (β = −1.64, SE = 1.07, p = 0.13) or social skills (β = 1.43, SE = 0.89, p = 0.11). Because quadratic terms were included in social skills and internalizing models, these average slopes represent the instantaneous linear rate of change at T1 (because Time was centered at T1). There was significant variability in the linear rate of change for externalizing problems, σ 2 = 6.04, SE = 2.12, p = 0.004, internalizing problems, σ 2 = 13.51, SE = 2.83, p < 0.001, and social skills, σ 2 = 43.17, SE = 17.97, p = 0.02, suggesting that there was variability in change across children.
Question 1: Does Early Fathering Predict Trajectories of Children’s Externalizing Problems, Internalizing Problems, and Social Skills?
The linear and intercept growth factors were regressed on each predictor one at a time. For T1 Models, the linear growth factor was also regressed on the intercept growth factor to examine the relation between predictors and linear change controlling for initial behavior. Results are presented in Table 3 (only parameters of interest are presented because the focus was on these parameters rather than the model as a whole). Lower levels of paternal depressive symptoms were associated with linear decreases in externalizing problems, initial linear decreases in internalizing problems, and initial linear increases in social skills. Higher paternal SES was significantly associated with initial linear decreases in internalizing problems. Lower levels of T1 paternal depressive symptoms, fewer self-reported ADHD symptoms, lower laxness, fewer commands, and higher SES were associated with fewer T4 externalizing problems. Lower levels of T1 paternal depressive symptoms and paternal self-reported ADHD symptoms, and fewer commands were associated with fewer T4 internalizing problems. Higher SES and lower paternal depressive symptoms were associated with higher T4 social skills (Table 3).
The analyses described above were repeated using multigroup analyses in MPlus. In multigroup analyses, the model is estimated for each group first allowing each parameter to vary across groups and then restricting the parameter in question (the relation between the early fathering variable and the child outcome measure) to be equal across the two groups. If restricting this parameter to be equal across groups provides a significantly worse model fit, this suggests that the parameter is significantly different for the two groups and is presented separately for each group in Tables 3 and 4 under the parameter for the whole sample.
The relation between paternal depressive symptoms and children’s T4 externalizing scores was significantly different for boys than for girls, Χ 2 (1) = 6.76, p = 0.01. Paternal depressive symptomatology was significantly associated with T4 externalizing problems for both boys and girls, but this relation was significantly stronger for girls than for boys (Table 3). Boys and girls also differed in the relation between paternal self-reported ADHD symptoms and children’s T4 externalizing scores, Χ 2 (1) = 5.45, p = 0.02, and children’s cognitive ability, Χ 2 (1) = 4.10, p = 0.04. For girls, paternal self-reported ADHD symptoms were significantly associated with higher T4 externalizing symptoms and marginally significantly associated with lower cognitive ability, but these relations were not significant for boys. The relation between SES and T4 Social Skills was significantly different for boys and girls, Χ 2 (1) = 5.52, p = 0.02. Higher SES was associated with greater social skills for boys, but not for girls.
Children with and without diagnoses differed in the relation between paternal SES and T4 externalizing problems, Χ 2 (1) = 5.04, p = 0.02, internalizing problems, Χ 2 (1) = 7.20, p = 0.01, and social skills, Χ 2 (1) = 7.34, p = 0.01. Higher SES was associated with fewer externalizing and internalizing problems and higher social skills for children with ADHD or ODD diagnoses. Children with and without diagnoses also differed in the relation between father involvement and change in social skills, Χ 2 (1) = 6.16, p = 0.01. Father involvement was associated with initial linear increases in social skills for children with diagnoses, but not for children without diagnoses (Table 3).
Question 2. Does Early Fathering Predict Academic Achievement and Cognitive Ability?
Lower levels of paternal depressive symptoms and higher SES were associated with higher T4 academic achievement and T4 cognitive ability. Fewer paternal commands were associated with higher T4 academic achievement (Table 4). The relation between fathering and academic achievement and cognitive ability was not moderated by child gender. Children with and without diagnoses differed in the relation between paternal SES and T4 academic achievement, Χ 2 (1) = 8.00, p = 0.005, and cognitive ability, Χ 2 (1) = 4.34, p = 0.04. Higher SES was associated with significantly higher cognitive and academic achievement skills for children with ADHD or ODD diagnoses, and only associated with cognitive ability for children without diagnoses (Table 4).
Question 3: What Are the Underlying Mechanisms That Mediate the Relations Between Early Fathering and Later Child Outcome?
Mediational analyses were conducted using T4 child functioning as outcome variables, because few predictors of change in child functioning were identified. Confirmatory factor analyses on the five outcome variables supported two latent factors: externalizing, internalizing, and social skills loaded significantly on a Social Emotional Functioning factor, and cognitive and achievement scores loaded significantly on an Academic factor. This two factor model demonstrated excellent fit, Χ 2 (4) = 3.50, p = 0.48, RMSEA = 0.00, SRMR = 0.03, CFI = 1.00. Path modeling was then used to test mediation hypotheses, with these latent factors as outcomes. Laxness and commands were the only parenting variables that predicted child outcome, so hypotheses involving parenting as a mediator were tested only for laxness and commands.
Does Parenting Mediate the Relation Between Parent Psychopathology and Child Outcome?
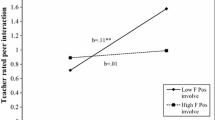
Separate models were estimated for paternal depressive symptoms and self-reported ADHD symptoms. In the path model, each latent outcome variable was regressed on the parenting variable and the paternal psychopathology variable, and then the parenting variable was regressed on the paternal psychopathology variable. There was modest support for paternal laxness as a partial mediator of the relation between paternal self-reported ADHD symptoms and children’s T4 social emotional functioning, but not between paternal self-reported ADHD symptoms and children’s academic functioning (see Fig. 1). There were significant direct paths from paternal self-reported ADHD symptoms to laxness and from paternal laxness to child social emotional functioning. The indirect path from paternal self-reported ADHD symptoms to social emotional functioning through paternal laxness approached significance (B = 1.68, SE B = 0.93, β = 0.06, SE β = 0.03, p = 0.07). However, the direct path from paternal self-reported ADHD symptoms to child social emotional functioning remained significant, suggesting that paternal laxness was only a partial mediator of the relation between paternal self-reported ADHD symptoms and social emotional functioning. Model fit indices for this model suggested good fit, Χ 2 (10) = 11.45, p = 0.32, RMSEA = 0.03, SRMR = 0.04, CFI = 0.99. Paternal laxness did not mediate the relation between paternal depressive symptoms and child outcome. Paternal commands did not mediate any relations between paternal psychopathology and child outcome.

Significant mediation models. Unstandardized path coefficients are on top and standardized coefficients are on the bottom for each path. Ext externalizing problems, Int internalizing problems, Soc social skills, WISC Wechsler intelligence scale for children, fourth edition, WIAT Wechsler individual achievement test, second edition, abbreviated. *p < 0.05, **p < 0.01, ***p < 0.001
Does Paternal Depressive Symptomatology Mediate the Relation Between Paternal Self-Reported ADHD Symptomatology and Child Outcome?
Analyses supported paternal depressive symptomatology as a mediator of the relation between paternal self-reported ADHD symptomatology and child outcome. The direct path from paternal self-reported ADHD symptoms to paternal depressive symptoms was significant as were the direct paths from paternal depressive symptoms to social emotional functioning and academic functioning (Fig. 1). The indirect paths from paternal self-reported ADHD symptoms through paternal depressive symptoms were also significant for social emotional functioning (B = 5.25, SE B = 1.64, β = 0.18, SE β = 0.06, p = 0.001), and for academic functioning (B = −4.84, SE B = 1.97, β = −.16, SE β = 0.06, p = 0.006). The direct paths from paternal self-reported ADHD symptoms to child functioning were no longer significant when paternal depressive symptoms was included as a mediator, suggesting that paternal depressive symptoms fully mediated the relation between paternal self-reported ADHD symptoms and child outcome. Model fit indices for this model suggested good fit, Χ 2 (10) = 10.19, p = 0.42, RMSEA = 0.01, SRMR = 0.04, CFI = 0.99.
Discussion
The present study examined the longitudinal relation between early fathering and subsequent child functioning among preschool children with behavior problems. A number of father characteristics were identified as playing a key role in their children’s development, with low SES and greater depressive symptoms most consistently associated with poorer future functioning across multiple domains. Furthermore, there was evidence that gender and diagnostic status moderated some relations between early fathering and child outcome. Results also provide some insight into the mechanisms by which early fathering predicts child outcome.
The present study suggests that some, but not all dimensions of fathers’ parenting may play a role in the later functioning of preschool children with behavior problems. Extending previous cross-sectional research (Gryczkowski et al. 2010; Tallmadge and Barkley 1983), the present study suggests that fathers’ use of lax parenting and frequent commands may play a role in the prognosis of preschoolers with behavior problems, and may therefore be important targets for early intervention. However, contrary to prediction, paternal overreactivity and warmth did not significantly predict child externalizing and internalizing problems, despite prior evidence that these dimensions are linked to preschool children’s functioning (Keown 2011; Nelson and Coyne 2009). Previous studies of fathers’ parenting have generally examined community samples or have compared clinic to non-clinic samples. It may be that paternal overreactivity and warmth distinguish nonproblem children from children with behavior problems, but do not predict subsequent functioning among children with behavior problems. It is important not only to identify parenting practices that distinguish nonproblem children from those with behavior problems, but also to identify practices that are critical to improving functioning in children with behavior problems. The former has important implications for prevention of behavior problems, whereas the latter may guide intervention efforts for children once they present with behavior problems.
Paternal depressive symptoms may also play a critical role in the prognosis of preschool-aged children with behavior problems. Paternal depressive symptoms not only predicted subsequent levels of child functioning, but also predicted changes in child externalizing and internalizing problems, providing stronger evidence that paternal depressive symptoms may play a causal role in children’s development. However, other causal mechanisms remain plausible. For example, depression may also be a marker of another risk factor that plays a causal role in children’s adjustment, including marital distress, interparental conflict over childrearing, and other aspects of family adversity. The present study also suggests that paternal ADHD symptoms may play a crucial role during the preschool years; however, this role appears to be mediated by paternal depressive symptomatology and lax parenting.
Although there was some evidence that father involvement may play a beneficial role in the development of social skills among children with diagnoses, the present study did not generally find evidence that father involvement among preschool-aged children predicted subsequent child functioning. Thus, it may be the quality rather than quantity of fathering that may be most important. Previous longitudinal research has more consistently linked father involvement with child outcome among older children (Flouri and Buchanan 2003) than among younger children (Aldous and Mulligan 2002), suggesting that children’s age may play a role in the effects of father involvement. Future research is needed to examine whether child age moderates relation between father involvement and child functioning.
This study provides some support for gender differences in the relation between paternal psychopathology and child functioning; however, consistent with previous research, the results were mixed—some relations were stronger for boys, others stronger for girls, and others revealed no gender differences. Our finding that paternal psychopathology predicted externalizing problems more strongly for girls than for boys, suggests that the mechanisms underlying the early development of externalizing problems may be different for boys than for girls. It may be, for example, that girls are more sensitive to their fathers’ moods than are boys. This study also provides support for the notion of differential susceptibility (Belsky and Pluess 2009). Paternal SES was linked to child functioning among children with ADHD and ODD diagnoses, but not among children with transient behavior problems, suggesting that children with psychological disorders may be more sensitive to the stressors that families with fewer resources may experience. Taken together, these findings suggest that child characteristics may play an important role in how early fathering shapes young children’s development.
Limitations
The results of the present study should be interpreted in the context of several limitations. First, only a subsample of fathers completed a measure of father involvement, so power was lower for this variable and may have made it difficult to detect effects. Second, not all children in the larger study had fathers participate; it is possible that fathers who did not participate were lower functioning than fathers who did participate, limiting the generalizability of the findings. Third, it is unclear whether findings regarding paternal psychopathology would generalize to clinically diagnosed fathers, given the low percentage of fathers who fell above clinical thresholds of depression and ADHD in this sample. Fourth, paternal ADHD symptomatology was assessed with a self-report rating scale; other informants’ reports of fathers’ ADHD were not available. Self-report of adult ADHD symptoms may not be as sensitive as others’ reports, and may underestimate ADHD symptomatology (Sibley et al. 2012). Fifth, although the sample was ethnically diverse, these results may not generalize to all ethnic groups. The sample size was not sufficient for examining effects separately for different ethnic groups. Sixth, although audiotaped recordings of father-child interactions provide some benefits for assessing fathers’ parenting in a naturalistic setting, it was not possible to assess nonverbal parenting behavior, which may also be important for child development. Finally, although the longitudinal design of the present study provides stronger support for a causal link between early fathering and child functioning than do cross-sectional studies, the findings of this study do not establish the direction of causality between father and child functioning. For example, early father functioning (particularly parenting) may be affected by early child behavior which in turn is stable over time; observed relations between father functioning and later child outcome may therefore be accounted for by early child functioning.
Clinical Implications
The present study provides a first step toward identifying which aspects of early fathering may be most important in helping preschoolers with behavior problems follow more positive developmental trajectories. Results point to a number of areas of father functioning that may be important; however, paternal depressive symptomatology stood out as a particularly important contributor. Research has begun to examine the effects of treating parent depression on child functioning (Garber et al. 2011), though parents in these studies have primarily been mothers. Research is needed to examine whether specifically treating paternal depressive symptoms may result in better outcomes for young children. Our findings also suggest that parent training efforts that teach fathers effective ways of setting limits may be an important part of early intervention with preschool children with behavior problems. Finally, this study points to SES as an important predictor of child functioning, suggesting that early intervention should particularly reach out to children whose families have fewer resources.
References
Aldous, J., & Mulligan, G. M. (2002). Fathers’ child care and children’s behavior problems: a longitudinal study. Journal of Family Issues, 23, 624–647. doi:10.1177/0192513X02023005003.
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: a measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144. doi:10.1037/1040-3590.5.2.137.
Barkley, R. A., & Murphy, K. R. (1998). Attention deficit hyperactivity disorder: A clinical workbook. New York: Guilford.
Baruch, G. K., & Barnett, R. C. (1986). Role quality, multiple role involvement, and psychological well-being in midlife women. Journal of Personality and Social Psychology, 51, 578–585. doi:10.1037/0022-3514.51.3.578.
Belsky, J., & Pluess, M. (2009). Beyond diathesis stress: differential susceptibility to environmental influences. Psychological Bulletin, 135, 885–908. doi:10.1037/a0017376.
Connell, A. M., & Goodman, S. H. (2002). The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: a meta-analysis. Psychological Bulletin, 128, 746–773. doi:10.1037/0033-2909.128.5.746.
DeKlyen, M., Biernbaum, M. A., Speltz, M. L., & Greenberg, M. T. (1998). Fathers and preschool behavior problems. Developmental Psychology, 34, 264–275. doi:10.1037/0012-1649.34.2.264.
Dietz, L. J., Jennings, K. D., Kelley, S. A., & Marshal, M. (2009). Maternal depression, paternal psychopathology, and toddlers’ behavior problems. Journal of Clinical Child and Adolescent Psychology, 38, 48–61. doi:10.1080/15374410802575362.
Downer, J. T., & Mendez, J. L. (2005). African American father involvement and preschool children’s school readiness. Early Education and Development, 16, 317–340. doi:10.1207/s15566935eed1603_2.
Egeland, B. (1997). Mediators of the effect of child maltreatment on developmental adaptation in adolescence. In D. Cicchetti & S. L. Toth (Eds.), Developmental perspectives on trauma: Theory, research, and intervention (pp. 403–434). Rochester: University of Rochester Press.
Eiden, R. D., Edwards, E. P., & Leonard, K. E. (2007). A conceptual model for the development of externalizing behavior problems among kindergarten children of alcoholic families: role of parenting and children’s self-regulation. Developmental Psychology, 43, 1187–1201. doi:10.1037/0012-1649.43.5.1187.
Eiden, R. D., Colder, C., Edwards, E. P., & Leonard, K. E. (2009). A longitudinal study of social competence among children of alcoholic and nonalcoholic parents: role of parental psychopathology, parental warmth, and self-regulation. Psychology of Addictive Behaviors, 23, 36–46. doi:10.1037/a0014839.
Fagan, J., & Iglesias, A. (1999). Father involvement program effects on fathers, father figures, and their Head Start children: a quasi-experimental study. Early Childhood Research Quarterly, 14, 243–269. doi:10.1016/S0885-2006(99)00008-3.
Flouri, E. (2005). Father’s involvement and psychological adjustment in Indian and White British secondary school age children. Child and Adolescent Mental Health, 10, 32–39. doi:10.1111/j.1475-3588.2005.00114.x.
Flouri, E., & Buchanan, A. (2003). The role of father involvement in children’s later mental health. Journal of Adolescence, 26, 63–78. doi:10.1016/S0140-1971(02)00116-1.
Garber, J., Ciesla, J. A., McCauley, E., Diamond, G., & Schloredt, K. A. (2011). Remission of depression in parents: links to healthy functioning in their children. Child Development, 82, 244–261. doi:10.1111/j.1467-8624.2010.01552.x.
Gryczkowski, M. R., Jordan, S. S., & Mercer, S. H. (2010). Differential relations between mothers’ and fathers’ parenting practices and child externalizing behavior. Journal of Child and Family Studies, 19, 539–546. doi:10.1007/s10826-009-9326-2.
Harvey, E. A., Metcalfe, L. A., Herbert, S. D., & Fanton, J. H. (2011). The role of family experiences and ADHD in the early development of oppositional defiant disorder. Journal of Consulting and Clinical Psychology, 79, 784–795. doi:10.1037/a0025672.
Jewell, J. D., Krohn, E. J., Scott, V. G., Carlton, M., & Meinz, E. (2008). The differential impact of mothers’ and fathers’ discipline on preschool children’s home and classroom behavior. North American Journal of Psychology, 10, 173–188.
Kane, P., & Garber, J. (2004). The relations among depression in fathers, children’s psychopathology, and father–child conflict: a meta-analysis. Clinical Psychology Review, 24, 339–360. doi:10.1016/j.cpr.2004.03.004.
Keown, L. J. (2011). Fathering and mothering of preschool boys with hyperactivity. International Journal of Behavioral Development, 35, 161–198. doi:10.1177/0165025410380982.
Keown, L. J. (2012). Predictors of boys’ ADHD symptoms from early to middle childhood: the role of father–child and mother–child interactions. Journal of Abnormal Child Psychology, 40, 569–581. doi:10.1007/s10802-011-9586-3.
Loukas, A., Zucker, R. A., Fitzgerald, H. E., & Krull, J. L. (2003). Developmental trajectories of disruptive behavior problems among sons of alcoholics: effects of parent psychopathology, family conflict, and child undercontrol. Journal of Abnormal Psychology, 112, 119–131. doi:10.1037/0021-843X.112.1.119.
Martin, A., Ryan, R. M., & Brooks-Gunn, J. (2007). The joint influence of mother and father parenting on child cognitive outcomes at age 5. Early Childhood Research Quarterly, 22, 423–439. doi:10.1016/j.ecresq.2007.07.001.
Martin, A., Ryan, R. M., & Brooks-Gunn, J. (2010). When fathers’ supportiveness matters most: maternal and paternal parenting and children’s school readiness. Journal of Family Psychology, 24, 145–155. doi:10.1037/a0018073.
Muthén, L. K., & Muthén, B. O. (1998–2010). Mplus user’s guide (6th ed.). Los Angeles: Muthén & Muthén.
Nelson, D. A., & Coyne, S. M. (2009). Children’s intent attributions and feelings of distress: associations with maternal and paternal parenting practices. Journal of Abnormal Child Psychology, 37, 223–237. doi:10.1007/s10802-008-9271-3.
National Institute of Child Health and Human Development Early Child Care Research Network. (2004). Fathers’ and mothers’ parenting behavior and beliefs as predictors of children’s social adjustment in the transition to school. Journal of Family Psychology, 18, 628–638. doi:10.1037/0893-3200.18.4.628.
Nigg, J. T., & Hinshaw, S. P. (1998). Parent personality traits and psychopathology associated with antisocial behaviors in childhood attention-deficit hyperactivity disorder. Journal of Child Psychology and Psychiatry, 39, 145–159. doi:10.1111/1469-7610.00309.
Paulson, J. F., Keefe, H. A., & Leiferman, J. A. (2009). Early parental depression and child language development. Journal of Child Psychology and Psychiatry, 50, 254–262. doi:10.1111/j.1469-7610.2008.01973.x.
Phares, V., Fields, S., Kamboukos, D., & Lopez, E. (2005). Still looking for poppa. American Psychologist, 60, 735–736. doi:10.1037/0003-066X.60.7.735.
Radloff, L. S. (1977). The CES-D Scale: a self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. doi:10.1177/014662167700100306.
Ramchandani, P., Stein, A., Evans, J., & O’Connor, T. G. (2005). Paternal depression in the postnatal period and child development: a prospective population study. The Lancet, 365, 2201–2205. doi:10.1016/S0140-6736(05)66778-5.
Ramsay, J. R., & Rostain, A. L. (2008). Adult ADHD research: current status and future directions. Journal of Attention Disorders, 11, 624–627. doi:10.1177/1087054708314590.
Reynolds, C. R., & Kamphaus, R. W. (1992). Behavior assessment system for children. Circle Pines: American Guidance Service.
Schindler, H. S. (2010). The importance of parenting and financial contributions in promoting fathers’ psychological health. Journal of Marriage and Family, 72, 318–332. doi:10.1111/j.1741-3737.2010.00702.x.
Sibley, M. H., Pelham, W. E., Jr., Molina, B. S. G., Gnagy, E. M., Waxmonsky, J. G., Waschbusch, D. A., et al. (2012). When diagnosing ADHD in young adults emphasize informant reports DSM items, and impairment. Journal of Consulting and Clinical Psychology. Advance online publication. doi:10.1037/a0029098
Takeda, T., Stotesbery, K., Power, T., Ambrosini, P. J., Berrettini, W., Hakonarson, H., et al. (2010). Parental ADHD status and its association with proband ADHD subtype and severity. The Journal of Pediatrics, 157, 995–1000. doi:10.1016/j.jpeds.2010.05.053.
Tallmadge, J., & Barkley, R. A. (1983). The interactions of hyperactive and normal boys with their fathers and mothers. Journal of Abnormal Child Psychology, 11, 565–580. doi:10.1007/BF00917085.
Tamis-LeMonda, C. S., Shannon, J. D., Cabrera, N. J., & Lamb, M. E. (2004). Fathers and mothers at play with their 2- and 3-year-olds: contributions to language and cognitive development. Child Development, 75, 1806–1820. doi:10.1111/j.1467-8624.2004.00818.x.
The Psychological Corporation. (1992). The Wechsler individual achievement test. New York: Harcourt, Brace, Jovanovich.
Trautmann-Villalba, P., Gschwendt, M., Schmidt, M. H., & Laucht, M. (2006). Father-infant interaction patterns as precursors of children’s later externalizing behavior problems: a longitudinal study over 11 years. European Archives of Psychiatry and Clinical Neuroscience, 256, 344–349. doi:10.1007/s00406-006-0642-x.
Wadsworth, M. E., & Achenbach, T. M. (2005). Explaining the link between low socioeconomic status and psychopathology: testing two mechanisms of the social causation hypothesis. Journal of Consulting and Clinical Psychology, 73, 1146–1153. doi:10.1037/0022-006X.73.6.1146.
Wechsler, D. (2003). Wechsler intelligence scale for children–fourth edition: Technical and interpretive manual. San Antonio: Psychological Corporation.
Author information
Authors and Affiliations
Corresponding author
Additional information
This research was supported by a grant from the National Institutes of Health (MH60132) awarded to the second author.
Rights and permissions
About this article
Cite this article
Herbert, S.D., Harvey, E.A., Lugo-Candelas, C.I. et al. Early Fathering as a Predictor of Later Psychosocial Functioning Among Preschool Children with Behavior Problems. J Abnorm Child Psychol 41, 691–703 (2013). https://doi.org/10.1007/s10802-012-9706-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-012-9706-8