
Abstract
Purpose
We aimed to investigate the association between subfoveal choroidal thickness (SCT) and the level of aqueous humor (AH) inflammatory cytokines in patients with macular edema (ME) associated with branch retinal vein occlusion (BRVO).
Methods
Twenty-eight eyes of 28 BRVO ME patients who underwent intravitreal injection treatment (ranibizumab, bevacizumab, or dexamethasone implant) were prospectively recruited. The concentrations of vascular endothelial growth factor (VEGF)-A and inflammatory cytokines were measured from AH samples. We analyzed clinical factors associated with visual gain or the degree of central macular thickness (CMT) decrease and the association between SCT and inflammatory cytokine levels.
Results
On multiple linear regression analysis, the AH interleukin (IL)-8 level was significantly associated with visual gain and CMT reduction at 6 months. Age, systemic hypertension, and AH monocyte chemo-attractant protein 1 level showed a significant association with baseline SCT, and VEGF-A showed a significant association with baseline SCT ratio (BRVO eye SCT/fellow eye SCT). Those with thick SCT showed a higher level of AH soluble VEGF receptors 2 and IL-8 and showed better visual gain and greater CMT reduction at 2 and 6 months compared to the thin SCT group.
Conclusions
The level of AH inflammatory cytokines was significantly associated with the ischemic status of the retina, treatment outcomes, and SCT in BRVO ME patients. Thick baseline SCT might be a predictive sign for better treatment outcomes in BRVO ME patients which are thought to be related to a higher level of intraocular inflammatory cytokines in these patients.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Branch retinal vein occlusion (BRVO) is an important cause of visual impairment. Previously reported prevalence rates were ranging from 0.3 to 0.9% [1,2,3], and the incidence rate of the disease is not infrequent, especially in an elderly group. The 15-year cumulative incidence of BRVO was 1.8% [4]. Most vision-threatening complications of BRVO are caused by macular edema (ME). Previously, grid laser photocoagulation was the standard of care for ME associated with BRVO; however, nowadays, anti-vascular endothelial growth factor (VEGF) or sustained-release, biodegradable dexamethasone implant treatment is widely used for the treatment of ME associated with BRVO.
The pathogenesis of ME in BRVO is thought to be complex. It is thought that the release of VEGF and various inflammatory cytokines following the vascular occlusion results in the breakdown of the blood-retinal barrier and an increase in vascular permeability. The intraocular levels of VEGF and inflammatory cytokines, mostly measured on aqueous humor (AH) samples, were higher than those of control [5,6,7,8,9,10,11,12,13,14]. Notably, there was a significant correlation between the aqueous and the vitreous level of VEGF in BRVO ME patients [5]. The levels of the inflammatory cytokines showed a significant correlation with the severity of BRVO, such as the degree of macular edema, aqueous flare, or perfusion status [8, 9, 15]. The VEGF and inflammatory cytokine levels in BRVO ME patients decreased following the treatment and re-elevated when the disease was reactivated [6, 13, 14]. The VEGF and inflammatory cytokine levels were also highly correlated with the recurrence of the disease and the number of intravitreal injection treatment [11]. Taken together, these suggest that the AH level of VEGF and inflammatory cytokines could be a good indicator of the disease activity in ME associated with BRVO. However, it is not practical to measure these values in every patient in the clinic.
Since the enhanced depth imaging mode of optical coherence tomography was introduced to visualize the choroid [16], an increasing number of studies have evaluated choroidal thickness in various chorioretinal disorders and its association with the disease activity. Several studies were performed on evaluating choroidal thickness in retinal vein occlusion (RVO) patients. In general, the RVO eye showed thicker choroidal thickness compared to the non-affected fellow eye or control group [17,18,19,20]. The choroidal thickness or volume decreased following the resolution of ME after treatment [17,18,19,20]. The choroidal thickening in RVO patients showed regional difference, and there was a difference in choroidal thickening according to the type of ME [21, 22]. In central RVO patients, those with thicker baseline choroid tend to show better treatment response [23]. Taken together, these suggest that choroidal thickness could reflect disease activity or treatment outcome in RVO patients with ME. However, studies on the relationship between the AH level of VEGF and inflammatory cytokines and choroidal thickness that are both thought to be related to the disease activity of RVO are lacking. Thus, in this study, we aimed to investigate the association between subfoveal choroidal thickness (SCT) and the level of AH VEGF and inflammatory cytokines in BRVO ME patients to find out whether SCT could be used as a clinical indicator predicting inflammatory status and treatment outcome in BRVO ME patients.
Methods
The study was conducted prospectively in the Department of Ophthalmology at Kangdong Sacred Heart Hospital. The study protocol was approved by the Institutional Review Board (IRB) of Kangdong Sacred Heart Hospital (IRB no. 2017-09-014) and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients before study inclusion.
Inclusion and exclusion criteria
BRVO ME patients who underwent intravitreal anti-VEGF (ranibizumab [Lucentis, Genentech Inc., CA, USA and Novartis AG, Basel, Switzerland] or bevacizumab [Avastin, Genentech and Hoffmann La Roche, Basel, Switzerland]) or dexamethasone implant (Ozurdex, Allergan Inc., Madison, NJ, USA) injections were enrolled according to the following criteria: (1) age > 20 years old, (2) central macular thickness (CMT) > 300 μm. Exclusion criteria were: (1) previous intravitreal injections within 6 months, (2) retinal disorders or inflammation other than BRVO (e.g., central retinal vein occlusion, age-related macular degeneration, diabetic retinopathy, uveitis, etc.), (3) previous intraocular surgery other than uncomplicated cataract surgery.
Aqueous humor sample acquisition and analysis
All aqueous humor specimens were collected using an aseptic technique in an operating room. After applying topical anesthesia eye drops (proparacaine, Alcaine®, Alcon, Fort Worth, TX, USA), the ocular surface, eyelid, and eyebrow were disinfected with 5% povidone iodine, and a sterilized eyelid speculum was inserted. Anterior chamber punctures were performed using a 1-mL syringe with a 30-gauge needle, and 0.1 mL of aqueous humor was collected before intravitreal injection. All undiluted aqueous humor samples were rapidly frozen under liquid nitrogen and stored at − 80 °C deep freezer until they were assayed. The concentrations of VEGF-A, soluble vascular endothelial growth factor receptors 2 (sVEGFR-2), monocyte chemo-attractant protein 1 (MCP-1), interleukin (IL)-6, IL-8, and platelet-derived growth factor AA (PDGF-AA) were measured with a multiplexed sandwich enzyme-linked immunosorbent assay (Human Magnetic Luminex® assay, R&D Systems, USA) according to the manufacturer’s instructions.
Ophthalmologic examinations and central macular thickness and subfoveal choroidal thickness measurements
Patients underwent basic ophthalmologic examinations including measurement of visual acuity and intraocular pressure, slit-lamp examination, and fundus examination using indirect ophthalmoscope on every follow-up visit. Best-corrected visual acuity (BCVA) was assessed using a decimal visual acuity chart and converted into the logarithm of the minimum angle resolution (LogMAR) scale for statistical analysis. Spectral-domain OCT (Spectralis, Heidelberg Engineering, Heidelberg, Germany) was performed on every visit to evaluate the status of the macula. Central macular thickness (CMT) was defined as the mean retinal thickness within the 1-mm-diameter central region of the Early Treatment Diabetic Retinopathy Study grid. Subfoveal choroidal thickness was measured using a horizontal OCT scan centered on the foveal center, which was taken by enhanced depth imaging mode with 100-line scan images averaged. Subfoveal choroidal thickness was measured perpendicularly from the outer border of the hyperreflective retinal pigment epithelium to the inner sclera under the foveal center using the 1:1 micron image with a built-in ruler tool. One experienced observer (Y-KK) measured choroidal thickness masked to the patient information. Fluorescein angiography (FA) was performed (Optos 200TX, Optos PLC, Dunfermline, Scotland) when significant non-perfusion is suspected and patients were able to undergo contrast enhancement. We measured peripheral non-perfusion area by disc area (DA) [24] and categorized it as the following criteria: < 1 DA, ≥ 1 and < 10 DA, ≥ 10 and < 30 DA, and ≥ 30 DA.
Statistical analyses
We explored clinical factors associated with treatment outcomes following intravitreal injection. We analyzed clinical factors associated with visual gain or the degree of CMT reduction 6 months after intravitreal injection using multiple linear regression analysis. Age, sex, the level of AH VEGF-A and inflammatory cytokines, baseline BCVA, baseline CMT, baseline SCT, previous treatment history (treatment naïve case or not), type of the treatment (anti-VEGF vs. dexamethasone implant), number of injections during 6 months were entered into the equation, and stepwise approach was applied. We also investigated the correlation between baseline SCT or baseline SCT ratio (RVO eye SCT/fellow eye SCT) and the level of AH inflammatory cytokines. Pearson’s correlation coefficient was calculated between the SCT or SCT ratio and the level of AH inflammatory cytokines. We compared the level of AH VEGF-A and inflammatory cytokines according to the degree of the non-perfusion area identified by FA using a one-way analysis of variance (ANOVA) and Scheffe test for post hoc analysis. We also performed multiple linear regression analysis for factors associated with baseline SCT and SCT ratio using various clinical factors. Age, sex, underlying diseases (diabetes, hypertension), previous treatment history (treatment naïve case or not), the level of AH VEGF-A and inflammatory cytokines, baseline BCVA, refractive errors, baseline CMT were entered into the equation, and a stepwise approach was applied. We divided patients into two groups according to their baseline SCT. Baseline characteristics, AH VEGF-A and inflammatory cytokines levels, and treatment outcomes were compared between two groups using the Man–Whitney U test for continuous variables and Chi-square or Fisher’s exact test for categorical variables. All statistical analyses were performed using PASW version 18.0 (SPSS, Inc., Chicago, IL). A p value < 0.05 was considered statistically significant.
Results
Twenty-eight eyes of twenty-eight BRVO ME patients (8 men and 20 women) who underwent intravitreal anti-VEGF or dexamethasone implant injection were included in the study. The mean age of patients was 63.2 ± 9.1 years. The proportion of the treatment naïve case was 82%. Sixteen patients were treated with anti-VEGF injection (3 ranibizumab and 13 bevacizumab), and 12 patients underwent dexamethasone implant injection. The average number of injections during 6 months was 1.9 ± 1.1 (range, 1–5). Patients demographics and baseline characteristics are summarized in Table 1.
On multiple linear regression analysis, AH IL-8 level was significantly associated with visual gain at 6 months after intravitreal injections (standardized coefficient β = 0.544; p = 0.003, Table 2) and baseline CMT (standardized coefficient β = 0.572; p < 0.001) and AH IL-8 level (standardized coefficient β = 0.404; p = 0.004) showed a significant association with the degree of CMT reduction at 6 months after intravitreal injections (Table 2).
In 15 patients, FA was performed to evaluate retinal perfusion status. We compared the level of AH VEGF-A and inflammatory cytokines according to the degree of the peripheral non-perfusion area identified by FA. There was a general trend of increasing cytokine levels as the non-perfusion area increase, and there was a significant difference in PDGF-AA level between those with a small area of non-perfusion (< 1 DA or < 10 DA) and those with a large area of non-perfusion (≥ 30 DA; < 1 DA vs. ≥ 30 DA, p = 0.003, < 10 DA versus ≥ 30 DA, p = 0.049, post hoc analysis with Scheffe test, Fig. 1).

Aqueous humor VEGF and inflammatory cytokine levels and the degree of non-perfusion area on fluorescein angiography. The data are driven from the part of the patients (n = 15) in whom fluorescein angiography was taken. * represents p < 0.05. Abbreviation: DA, disc area; IL, interleukin; MCP-1, monocyte chemo-attractant protein 1; PDGF-AA, platelet-derived growth factor AA; sVEGFR2, soluble vascular endothelial growth factor receptors 2; VEGF-A, vascular endothelial growth factor-A
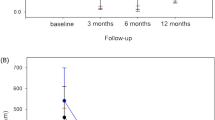
We explored the correlation between SCT or SCT ratio and AH VEGF-A and inflammatory cytokine levels. The level of MCP-1 (r = 0.439, p = 0.019) and IL-8 (r = 0.423, p = 0.025) showed a significant positive correlation with baseline SCT (Fig. 2). The level of VEGF-A showed a significant positive correlation with the baseline SCT ratio (r = 0.537, p = 0.003, Fig. 3). On multiple linear regression analysis, age (standardized coefficient β = − 0.348; p = 0.032), underlying hypertension (standardized coefficient β = − 0.368; p = 0.024), and AH MCP-1 level (standardized coefficient β = 0.380; p = 0.020) showed a significant association with baseline SCT and VEGF-A showed a significant association with baseline SCT ratio (standardized coefficient β = 0.537; p = 0.003, Table 3).

Correlation between subfoveal choroidal thickness and the level of aqueous humor inflammatory cytokines. Pearson correlation coefficient (r) and p-value are represented in each box. Abbreviation: IL, interleukin; MCP-1, monocyte chemo-attractant protein 1; PDGF-AA, platelet-derived growth factor AA; SCT, subfoveal choroidal thickness; sVEGFR2, soluble vascular endothelial growth factor receptors 2; VEGF-A, vascular endothelial growth factor-A

Correlation between subfoveal choroidal thickness ratio and the level of aqueous humor inflammatory cytokines. Pearson correlation coefficient (r) and p-value are represented in each box. Abbreviation: IL, interleukin; MCP-1, monocyte chemo-attractant protein 1; PDGF-AA, platelet-derived growth factor AA; RVO, retinal vein occlusion; SCT_ratio, subfoveal choroidal thickness ratio; sVEGFR2, soluble vascular endothelial growth factor receptors 2; VEGF-A, vascular endothelial growth factor-A
As we found a significant correlation between baseline SCT and AH inflammatory cytokine levels, we investigated whether baseline SCT is related to treatment outcomes in BRVO ME patients. We divided patients into 2 groups according to the median value of the baseline SCT (239 μm). There were no significant differences in terms of age, sex, underlying diseases, the proportion of the treatment naïve cases, type of the treatment (anti-VEGF vs. dexamethasone implant), injection numbers during 6 months, and baseline BCVA. However, the thick choroid group showed thicker baseline CMT (thin group, 473.3 ± 203.4 μm vs. thick group, 540.2 ± 168.2 μm, p = 0.012) and higher level of AH sVEGFR2 (thin group, 606.0 ± 266.2 pg/ml vs. thick group, 892.0 ± 435.4 pg/ml, p = 0.035) and IL-8 (thin group, 22.9 ± 17.3 pg/ml vs. thick group, 49.5 ± 38.4 pg/ml, p = 0.035). The thick choroid group showed better visual gain (2 months: thin group, 0.20 ± 0.24 vs. thick group, 0.44 ± 0.30, p = 0.044; 6 months: thin group, 0.15 ± 0.26 vs. thick group, 0.39 ± 0.28, p = 0.035) and greater CMT reduction (2 months: thin group, 144.0 ± 101.4 μm versus thick group, 242.4 ± 115.3 μm, p = 0.027; 6 months: thin group, 137.0 ± 105.0 μm vs. thick group, 231.0 ± 136.7 μm, p = 0.035) at 2 and 6 months after intravitreal injection (Table 4).
Discussion
In this study, we investigated the relationship between the level of AH inflammatory cytokines and SCT in BRVO ME patients, and whether it is possible to predict inflammatory status and treatment outcomes of the patients through SCT measurement. A higher level of AH IL-8 was associated with greater visual gain and CMT reduction at 6 months. The levels of MCP-1 and IL-8 showed a positive correlation with baseline SCT and that of VEGF-A showed a positive correlation with baseline SCT ratio. On multiple linear regression analysis, age, systemic hypertension, and MCP-1 level were associated with SCT. The AH level of VEGF-A was associated with the SCT ratio between the RVO eye and the unaffected fellow eye. When we divided the patients into two groups according to the baseline SCT, those with thicker SCT showed a higher level of AH sVEGFR2 and IL-8 and better visual gain and greater CMT reduction at 2 and 6 months.
The AH inflammatory cytokine levels showed a good correlation with clinical findings reflecting the disease activity. There were significant differences in the level of PDGF-AA between those with small and large areas of non-perfusion identified by FA. PDGF-A is normally produced by retinal ganglion cells, and it increases retinal astrocytes, which promote the survival of endothelial cells and their expression of barrier characteristics [25, 26]. It is also known to be vital for the maintenance of normal developmental angiogenesis in the retina and prevention of pathological angiogenesis in hypoxic conditions [27]. Our findings are in line with these previous findings that PDGF-AA is highly expressed in patients with a wide area of non-perfusion.
In this study, a high level of AH IL-8 was associated with better visual gain and greater CMT reduction at 6 months. IL-8 is a pro-inflammatory chemokine and induces an accumulation of neutrophils along the vessel wall [28]. Noma et al. reported that IL-8 showed the strongest correlation with the baseline aqueous flare value, suggesting that IL-8 may be the most important inflammatory factor involved in inflammation associated with BRVO ME [15]. In that study, a significant correlation was found between the change of the aqueous flare value and improvement of CMT and visual acuity 6 months after intravitreal ranibizumab injection [15]. Although we did not measure the level of AH inflammatory cytokines following treatment, we assume that those with a higher level of IL-8, thus having a higher degree of inflammation at baseline had a better chance to improve much following treatment.
We also evaluated the correlation between the SCT and the level of the AH inflammatory cytokines. Interestingly, we found a positive correlation between the levels of MCP-1 and IL-8 and the baseline SCT, while VEGF-A level showed a positive correlation with the SCT ratio between RVO and fellow eyes. In the previous studies, researchers hypothesized that RVO associated ischemia will increase the expression of VEGF and VEGF will result in the choroidal thickening through choroidal vascular hyperpermeability [18,19,20]. Assuming that the SCT of both eyes are similar [29, 30], the SCT ratio could be an index reflecting the degree of abnormal choroidal thickening caused by RVO. Our results are in line with the previous hypothesis that an increase in VEGF due to ischemia caused by RVO results in abnormal choroidal thickening. However, VEGF was not correlated with the SCT itself. The baseline SCT showed a positive correlation with inflammatory cytokines such as IL-8 and MCP-1. IL-8 and MCP-1 are known to play major roles in pro-inflammatory human retinal pigment epithelium-derived leukocyte chemotactic activity [28, 31]. Human uveal melanocytes are known to constitutively express a low level of IL-8 and MCP-1 and increase these expressions after pro-inflammatory stimulation [32]. It is reported that even in normal subjects, SCT was correlated with the level of AH CXCL13, suggesting that subclinical level of inflammation existing in the apparently normal subject is associated with SCT [33,34,35]. We hypothesize that some of the intraocular inflammatory cytokine levels are associated with SCT even in disease-free state and the increases in these cytokine levels due to disease activity are associated with a choroidal thickening.
In this study, we simply divided the patients into two groups according to the baseline SCT to compare the clinical outcomes. Those with thicker SCT showed a higher level of sVEGFR2 and IL-8 and better visual gain and greater CMT reduction at 2 and 6 months. These results suggest that those with thicker SCT might show a higher level of inflammatory cytokines and a greater therapeutic effect following BRVO ME treatment. These findings are in line with the previous report that baseline SCT may help predict treatment outcomes following anti-VEGF therapy in central RVO patients [23]. However, considering that the baseline CMT was also thicker in the thick choroid group, which might have affected treatment outcome, further study with a large number of patients is needed.
In this study, the choice of the treatment, either anti-VEGF or dexamethasone implant injection, was at the clinician’s discretion. Both anti-VEGF and dexamethasone implant injections are proven to be effective in the treatment of BRVO ME; however, there are no specific guidelines on which drug should be used on specific cases. In general, in refractory or recurrent cases, a switch of the drug is recommended [36], or even simultaneous treatment of both drugs is considered [37]. The reason for the different responses to anti-VEGF and dexamethasone treatment is thought to be due to different intraocular inflammatory cytokine status. Kaneda et al. reported that IL-8 was the most significant parameter of the disease activity, while IL-12 was the most likely factor associated with unresponsiveness to bevacizumab treatment in BRVO patients [38]. According to our findings, those with thicker SCT but not significantly thicker than that of the non-affected fellow eye, the intraocular profile of inflammatory cytokines will be likely to show a high level of inflammatory cytokines while relatively low level of VEGF. There is a possibility that this kind of patient will benefit from dexamethasone treatment. Unfortunately, due to small sample numbers, we were not able to find differences in treatment outcomes by different treatment methods according to the SCT. Further study with a large number of patients is needed to clarify this issue.
This study was limited by several points. First, we recruited a small number of patients, while the spectrum of the patients was wide. We included both treatment naïve cases and those with previously treated cases. We also included both anti-VEGF and dexamethasone implant injection cases. However, in this study, we did not find any significant effect of previous treatment history or treatment methods on treatment outcomes and SCT measurement. Second, there were no normal controls. Third, we only measured AH inflammatory cytokines once, and we were not able to show the changes in its level following treatment. Future studies with a large number of more uniform patients who were treated with the same treatment will be needed.
In conclusion, the level of AH inflammatory cytokines reflected the ischemic status of the retina and showed a significant association with treatment outcomes in BRVO ME patients. The level of AH inflammatory cytokines such as MCP-1 was also significantly associated with SCT. Thick baseline SCT might be a predictive sign for better treatment outcomes in BRVO ME patients which are thought to be related to a higher level of intraocular inflammatory cytokines in these patients.
Data availability
The datasets generated during the current study are available from the corresponding author upon request.
References
Wong TY, Larsen EK, Klein R, Mitchell P, Couper DJ, Klein BE, Hubbard LD, Siscovick DS, Sharrett AR (2005) Cardiovascular risk factors for retinal vein occlusion and arteriolar emboli: the atherosclerosis risk in communities & cardiovascular health studies. Ophthalmology 112:540–547. https://doi.org/10.1016/j.ophtha.2004.10.039
Cheung N, Klein R, Wang JJ, Cotch MF, Islam AF, Klein BE, Cushman M, Wong TY (2008) Traditional and novel cardiovascular risk factors for retinal vein occlusion: the multiethnic study of atherosclerosis. Invest Ophthalmol Vis Sci 49:4297–4302. https://doi.org/10.1167/iovs.08-1826
Keel S, Xie J, Foreman J, van Wijngaarden P, Taylor HR, Dirani M (2018) Prevalence of retinal vein occlusion in the Australian national eye health survey. Clin Exp Ophthalmol 46:260–265. https://doi.org/10.1111/ceo.13031
Klein R, Moss SE, Meuer SM, Klein BE (2008) The 15-year cumulative incidence of retinal vein occlusion: the beaver dam eye study. Arch Ophthalmol 126:513–518. https://doi.org/10.1001/archopht.126.4.513
Noma H, Funatsu H, Yamasaki M, Tsukamoto H, Mimura T, Sone T, Hirayama T, Tamura H, Yamashita H, Minamoto A, Mishima HK (2008) Aqueous humour levels of cytokines are correlated to vitreous levels and severity of macular oedema in branch retinal vein occlusion. Eye 22:42–48. https://doi.org/10.1038/sj.eye.6702498
Funk M, Kriechbaum K, Prager F, Benesch T, Georgopoulos M, Zlabinger GJ, Schmidt-Erfurth U (2009) Intraocular concentrations of growth factors and cytokines in retinal vein occlusion and the effect of therapy with bevacizumab. Invest Ophthalmol Vis Sci 50:1025–1032. https://doi.org/10.1167/iovs.08-2510
Feng J, Zhao T, Zhang Y, Ma Y, Jiang Y (2013) Differences in aqueous concentrations of cytokines in macular edema secondary to branch and central retinal vein occlusion. PLoS ONE 8:e68149. https://doi.org/10.1371/journal.pone.0068149
Noma H, Mimura T (2013) Aqueous soluble vascular endothelial growth factor receptor-2 in macular edema with branch retinal vein occlusion. Curr Eye Res 38:1288–1290. https://doi.org/10.3109/02713683.2013.821135
Jung SH, Kim KA, Sohn SW, Yang SJ (2014) Association of aqueous humor cytokines with the development of retinal ischemia and recurrent macular edema in retinal vein occlusion. Invest Ophthalmol Vis Sci 55:2290–2296. https://doi.org/10.1167/iovs.13-13587
Sohn HJ, Han DH, Lee DY, Nam DH (2014) Changes in aqueous cytokines after intravitreal triamcinolone versus bevacizumab for macular oedema in branch retinal vein occlusion. Acta Ophthalmol 92:e217-224. https://doi.org/10.1111/aos.12219
Noma H, Mimura T, Yasuda K, Nakagawa H, Motohashi R, Kotake O, Shimura M (2016) Cytokines and recurrence of macular edema after intravitreal ranibizumab in patients with branch retinal vein occlusion. Ophthalmologica 236:228–234. https://doi.org/10.1159/000451062
Noma H, Mimura T, Yasuda K, Nakagawa H, Motohashi R, Kotake O, Shimura M (2016) Intravitreal ranibizumab and aqueous humor factors/cytokines in major and macular branch retinal vein occlusion. Ophthalmologica 235:203–207. https://doi.org/10.1159/000444923
Noma H, Mimura T, Yasuda K, Shimura M (2016) Possible molecular basis of bevacizumab therapy for macular edema in branch retinal vein occlusion. Retina 36:1718–1725. https://doi.org/10.1097/iae.0000000000000983
Kunikata H, Shimura M, Nakazawa T, Sonoda KH, Yoshimura T, Ishibashi T, Nishida K (2012) Chemokines in aqueous humour before and after intravitreal triamcinolone acetonide in eyes with macular oedema associated with branch retinal vein occlusion. Acta Ophthalmol 90:162–167. https://doi.org/10.1111/j.1755-3768.2010.01892.x
Noma H, Mimura T, Yasuda K, Shimura M (2017) Functional-morphological parameters, aqueous flare and cytokines in macular oedema with branch retinal vein occlusion after ranibizumab. Br J Ophthalmol 101:180–185. https://doi.org/10.1136/bjophthalmol-2015-307989
Spaide RF, Koizumi H, Pozzoni MC (2008) Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol 146:496–500. https://doi.org/10.1016/j.ajo.2008.05.032
Tsuiki E, Suzuma K, Ueki R, Maekawa Y, Kitaoka T (2013) Enhanced depth imaging optical coherence tomography of the choroid in central retinal vein occlusion. Am J Ophthalmol 156:543-547.e541. https://doi.org/10.1016/j.ajo.2013.04.008
Chung YK, Shin JA, Park YH (2015) Choroidal volume in branch retinal vein occlusion before and after intravitreal anti-VEGF injection. Retina 35:1234–1239. https://doi.org/10.1097/iae.0000000000000455
Lee EK, Han JM, Hyon JY, Yu HG (2015) Changes in choroidal thickness after intravitreal dexamethasone implant injection in retinal vein occlusion. Br J Ophthalmol 99:1543–1549. https://doi.org/10.1136/bjophthalmol-2014-306417
Esen E, Sizmaz S, Demircan N (2016) Choroidal thickness changes after intravitreal dexamethasone implant injection for the treatment of macular edema due to retinal vein occlusion. Retina 36:2297–2303. https://doi.org/10.1097/iae.0000000000001099
Kim KH, Lee DH, Lee JJ, Park SW, Byon IS, Lee JE (2015) Regional choroidal thickness changes in branch retinal vein occlusion with macular edema. Ophthalmologica 234:109–118. https://doi.org/10.1159/000437276
Shin YU, Lee MJ, Lee BR (2015) Choroidal maps in different types of macular edema in branch retinal vein occlusion using swept-source optical coherence tomography. Am J Ophthalmol 160:328-334.e321. https://doi.org/10.1016/j.ajo.2015.05.003
Rayess N, Rahimy E, Ying GS, Pefkianaki M, Franklin J, Regillo CD, Ho AC, Hsu J (2016) Baseline choroidal thickness as a predictor for treatment outcomes in central retinal vein occlusion. Am J Ophthalmol 171:47–52. https://doi.org/10.1016/j.ajo.2016.08.026
Clarkson JG (1994) Central vein occlusion study: photographic protocol and early natural history. Trans Am Ophthalmol Soc 92:203–213
Yamada H, Yamada E, Ando A, Seo MS, Esumi N, Okamoto N, Vinores M, LaRochelle W, Zack DJ, Campochiaro PA (2000) Platelet-derived growth factor-A-induced retinal gliosis protects against ischemic retinopathy. Am J Pathol 156:477–487. https://doi.org/10.1016/s0002-9440(10)64752-9
Andrae J, Gallini R, Betsholtz C (2008) Role of platelet-derived growth factors in physiology and medicine. Genes Dev 22:1276–1312. https://doi.org/10.1101/gad.1653708
Wilkinson-Berka JL, Babic S, De Gooyer T, Stitt AW, Jaworski K, Ong LG, Kelly DJ, Gilbert RE (2004) Inhibition of platelet-derived growth factor promotes pericyte loss and angiogenesis in ischemic retinopathy. Am J Pathol 164:1263–1273. https://doi.org/10.1016/s0002-9440(10)63214-2
Ghasemi H, Ghazanfari T, Yaraee R, Faghihzadeh S, Hassan ZM (2011) Roles of IL-8 in ocular inflammations: a review. Ocul Immunol Inflamm 19:401–412. https://doi.org/10.3109/09273948.2011.618902
Caramoy A, Heindl LM (2017) Variability of choroidal and retinal thicknesses in healthy eyes using swept-source optical coherence tomography: implications for designing clinical trials. Clin Ophthalmol 11:1835–1839. https://doi.org/10.2147/opth.S145932
Entezari M, Karimi S, Ramezani A, Nikkhah H, Fekri Y, Kheiri B (2018) Choroidal thickness in healthy subjects. J Ophthalmic Vis Res 13:39–43. https://doi.org/10.4103/jovr.jovr_148_16
Elner VM, Strieter RM, Elner SG, Baggiolini M, Lindley I, Kunkel SL (1990) Neutrophil chemotactic factor (IL-8) gene expression by cytokine-treated retinal pigment epithelial cells. Am J Pathol 136:745–750
Hu DN, Bi M, Zhang DY, Ye F, McCormick SA, Chan CC (2014) Constitutive and LPS-induced expression of MCP-1 and IL-8 by human uveal melanocytes in vitro and relevant signal pathways. Invest Ophthalmol Vis Sci 55:5760–5769. https://doi.org/10.1167/iovs.14-14685
Holtkamp GM, Kijlstra A, Peek R, de Vos AF (2001) Retinal pigment epithelium-immune system interactions: cytokine production and cytokine-induced changes. Prog Retin Eye Res 20:29–48. https://doi.org/10.1016/s1350-9462(00)00017-3
Xu H, Chen M, Forrester JV (2009) Para-inflammation in the aging retina. Prog Retin Eye Res 28:348–368. https://doi.org/10.1016/j.preteyeres.2009.06.001
Nomura Y, Takahashi H, Fujino Y, Kawashima H, Yanagi Y (2016) Association between aqueous humor CXC motif chemokine ligand 13 levels and subfoveal choroidal thickness in normal older subjects. Retina 36:192–198. https://doi.org/10.1097/iae.0000000000000668
Pielen A, Bühler AD, Heinzelmann SU, Böhringer D, Ness T, Junker B (2017) Switch of intravitreal therapy for macular edema secondary to retinal vein occlusion from anti-VEGF to DEXAMETHASONE IMPLANT AND VICE VERSA. J Ophthalmol 2017:5831682. https://doi.org/10.1155/2017/5831682
Giuffrè C, Cicinelli MV, Marchese A, Coppola M, Parodi MB, Bandello F (2020) Simultaneous intravitreal dexamethasone and aflibercept for refractory macular edema secondary to retinal vein occlusion. Graefe’s Arch Clin Exp Ophthalmol 258:787–793. https://doi.org/10.1007/s00417-019-04577-8
Kaneda S, Miyazaki D, Sasaki S, Yakura K, Terasaka Y, Miyake K, Ikeda Y, Funakoshi T, Baba T, Yamasaki A, Inoue Y (2011) Multivariate analyses of inflammatory cytokines in eyes with branch retinal vein occlusion: relationships to bevacizumab treatment. Invest Ophthalmol Vis Sci 52:2982–2988. https://doi.org/10.1167/iovs.10-6299
Funding
This research was supported by Hallym University Research Fund 2018 (HURF-2018-33), Korean Association of Retinal Degeneration, and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (2018R1A2B6007809).
Author information
Authors and Affiliations
Contributions
SPP, Y-KK contributed to study design. YA, Y-KK contributed to data acquisition and analysis. YA, Y-KK contributed to manuscript drafting. YA, SPP, Y-KK contributed to review and approval of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
The study protocol was approved by the Institutional Review Board (IRB) of Kangdong Sacred Heart Hospital (IRB no.2017-09-014) and adhered to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from all patients before study inclusion.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
An, Y., Park, S.P. & Kim, YK. Aqueous humor inflammatory cytokine levels and choroidal thickness in patients with macular edema associated with branch retinal vein occlusion. Int Ophthalmol 41, 2433–2444 (2021). https://doi.org/10.1007/s10792-021-01798-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-021-01798-x