
Abstract
Diabetes and blindness are important health issues globally; we determined the prevalence of blindness, diabetic retinopathy, and other eye diseases in Nigerian-type 2 diabetics. A prospective, cross-sectional study was conducted on consenting type 2 diabetic patients who had scheduled comprehensive eye examination including dilated funduscopy with +78DS. Visual status was graded using the WHO criteria. Approval from Institutional Ethics Committee was obtained. Primary outcome measures were the prevalence and causes of blindness as well as prevalence of diabetic retinopathy. Secondary outcome measures were the presence of other eye diseases. Data were analyzed using SPSS version 13. Two hundred and sixty-six eyes of 133 type 2 diabetic patients aged 22–89 years were studied; 69 (51.9 %) were males while 64 (48.1 %) were females. Five (3.8 %) patients were blind while 27 (20.3 %) were visually impaired. Cataract was the leading cause of blindness (60 %) and visual impairment was found in 59.3 %. Diabetic retinopathy was present in 37 (27.8 %) diabetic patients of which 5 (3.8 %) were proliferative. Diabetic macular edema was present in 31 (23.3 %) patients. Severe visual impairment and blindness were commoner in those with diabetic retinopathy. Refractive error 67 (25.2 %), cataract 63 (23.7 %), and chronic glaucoma 44 (16.5 %) were the most prevalent non-diabetic retinopathy eye diseases. High prevalence of blindness, diabetic retinopathy, and other diseases are seen in type 2 diabetics. Health education, early diagnosis as well as treatment of diabetic retinopathy and other diseases will largely alleviate these ocular morbidities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The global prevalence of diabetes mellitus (DM) is expected to increase by 58 % between 2010 and 2030; this increase is tipped to be up to 98 % in sub Saharan Africa [1, 2]. More than half of persons suffering from diabetes are not aware of having the disease and thus are not on treatment [3]. Type 2 diabetes accounts for 90 % of diabetes mellitus in sub Saharan Africa and diabetic retinopathy rates of between 7 and 63 %have been reported in the region [4]. Nigeria has a type 2 diabetes prevalence rate of 4.99 % [5].
Visual impairment (VI) is a major health issue globally with significant socio-economic and psychological consequences [6]. It is believed to be more common in patients with diabetes compared to non-diabetics [7]. Diabetic retinopathy is the most well-known ocular complication of diabetes and a leading cause of blindness [8, 9]. The average risk of blindness from diabetic retinopathy in 2002 was reported as 0.75 % globally; this number is as high as 1.2 % in poorer countries [1]. Persons with diabetes are at an increased risk of other eye diseases apart from diabetic retinopathy; some of which are sight threatening while others increase the morbidity faced by such patients [1, 10, 11].
Type 2 diabetics may present with diabetic retinopathy at the time of diagnosis; this is possible since patients could have the disease and be unaware thus present late with complications as opposed to type 1 diabetes which is more life threatening if untreated [12, 13]. The possibility of late presentation of type 2 diabetes as well inequalities in accessing health care in developing countries of sub Saharan Africa contributes to early presentations of diabetic complications in the region [14]. The economic burden of type 2 diabetes is of immense importance to the patients and the society. The Markov-Model for the specific situation of cost of medical care for 145,000 type 2 diabetes Cambodia in 2008 is 2 million USD; 57 % of this amount would have to be spent for oral hypoglycemic agents and the rest for insulin therapy [15]. This cost, though exclusive of cost of loss of productivity is huge for a developing country in sub Saharan Africa with competing economic burdens of communicable and infectious diseases [14]. The cost of care for type 2 diabetes increases with the onset of diabetic complications. Macular edema remains a leading cause of visual loss in type 2 diabetics with significant public health and socioeconomic impact [16–18]. Duration of DM, level of glycemic control, systemic hypertension, and hyperlipidemia are known risk factors for diabetic retinopathy. Other risk factors identified in the diabetic retinopathy pathogenesis include pregnancy and renal impairment among others [13, 19–21].
The prevalence of cataract is higher in diabetics compared to their age-matched counterparts in the same environments; there is also a higher rate of cataract surgery among diabetics [22, 23]. Ocular motility disorders as well as fluctuating refractive status are some other diabetes-related eye diseases afflicting DM patients [24, 25].
For holistic care of patients with diabetes, management of diabetes-related eye diseases remain an important issue. Lack of resources and infrastructure required for adequately addressing diabetic retinopathy in poor countries have been cited as reasons for increased risk of blindness in poorer countries compared to global Fig. 1 This study is aimed at determining the prevalence of visual impairment, diabetic retinopathy, and other diabetes-related eye diseases as well as determining the causes of visual impairment in a cohort of type 2 diabetics under physician care in a Nigerian University Hospital. It is believed that the data and information obtained will assist in planning and prioritizing health care programme for early detection and treatment of diabetes-related eye diseases in the region.

Prevalence of blindness and visual impairment in type two diabetic patients
Methodology
This was a prospective, cross-sectional study of Type 2 diabetic patients receiving treatment from the endocrinology unit of the Obafemi Awolowo University Teaching Hospital Ile-Ife and its Wesley Guild Hospital Ilesa annex in southwestern Nigeria. These tertiary hospitals provide primary and specialist eye health for host communities (Ife-Ijesa) and beyond. The Ife-Ijesa zone is a senatorial in Osun State, south west Nigeria. It has a population of 1,148,641 according to the 2006 national population census [26]. The host communities are made of largely agrarian communities. The study approval was obtained from the Institutional Ethics Committee of Obafemi Awolowo University Teaching Hospital. Eligible participants for the study were consenting type 2 diabetic patients attending outpatient clinics for diabetic care in the institutions’ endocrinology clinics. Type 2 diabetes was diagnosed based on fasting blood glucose of ≥7.0 mmol/l in the setting of symptoms of diabetes mellitus. [27]. Diabetic patients receiving in-patients care during the study period were excluded due to the mandatory requirement of eye examination in the eye clinics. Eligible patients were counseled about purpose of the study. Consenting patients had anthropometric measures including height, weight as well as blood pressure taken. They were scheduled for eye examination at the eye clinic of the same institution and had additional benefits of individualized counseling, care and referral depending on the ocular findings. At the eye clinic, each patient had visual acuity assessment with illuminated Snellen’s chart for each eye at 6 m; non-literate patients were tested with tumbling E chart. Bright pen light and slit lamp biomicroscopic eye examinations were conducted to detect disorders of the cornea, anterior chamber, pupil, and the crystalline lens. Intraocular pressure measurement with Goldmann’s applanation tonometer was carried out for each eye following the instillation of tetracaine eye drop and fluorescein strips. Pupillary dilations were achieved using tropicamide and phenylephrine eye drops, and dilated retinal examination was conducted at the slit lamp with Volk’s +78DS; binocular indirect ophthalmoscopy was carried with +20D lens and Appasammy’s binocular indirect ophthalmoscope. Ocular findings were recorded into previously predesigned proforma and diagnosis made. Fundus camera became available towards the end of the study affording 12 patients with retinopathy the opportunity to have fundus photography. None of the study patients had optical coherence tomography (OCT) due to non-availability of such in the study centers and its immediate vicinity. Refractive error assessment was based on impaired distance vision which improved with pinhole assessment or distance vision improved with patients spectacles. Lenticular opacity dense enough to obscure detailed fundoscopy following papillary dilation or responsible for vision of 6/18 and worse was diagnosed as cataract. Visual status was graded using the World Health Organization’s criteria; visual impairment was considered as visual acuity of worse than 6/18 in the better eye while blindness was defined as visual acuity of less than 3/60 in the better eye [28]. Diabetic retinopathy was graded as no diabetic retinopathy, non-proliferative diabetic retinopathy (NPDR), or proliferative diabetic retinopathy (PDR) while those with diabetic macular edema were also noted using the modified International clinical diabetic retinopathy disease severity scale [29]. The diagnosis in the worse eye determined if a patient was denoted as NPDR or PDR [19]. Diagnosis of glaucoma was made for patients on treatment for the same or in patients with cup to disk ratio ≥0.7 and intraocular pressure greater than 21 mmHg as well as characteristic optic nerve head damage [3].
Primary outcome measures were the prevalence and causes of blindness as well as prevalence of diabetic retinopathy. Secondary outcome measures were the presence of eye diseases especially of the vitreous and retina.
SPSS version 13 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. Categorical variables were described by frequency distribution and percentages while continuous variables were described with means and standard deviations. The relationship between the presence of retinopathy and severity of visual loss was explored using the Chi-square and statistical significance assumed at p < 0.05.
Results
Two hundred and sixty-six eyes of 133 type 2 diabetes mellitus patients formed the study population with age range 22–89 years; 69 (51.9 %) were males while 64 (48.1 %) were females (Table 1). Most of the patients were aged 50 years and above (90.2 %) while 13 (9.8 %) were younger than 50 years. Three (2.3 %) were under-weight based on their body mass index (BMI), 37 (27.8 %) were obese, 49 (36.8 %) were overweight, and 44 (33.1 %) had normal BMI. Fifty (37.6 %) have had previous dilated eye examination since diagnosis of diabetes. Eighty-five (63.9 %) had one complaint or the other while 48 (36.1 %) had no ocular symptom as at the time of the study. Systemic co-morbidity was present in 103 (77.4 %) diabetics while no other disease was found in 30 (22.6 %); systemic hypertension was the commonest 101 (75.9 %). Others were peptic ulcer disease 2 (1.5 %), and 1 (0.8 %) each of asthma, arthritis, and depressive illness. Oral hypoglycemic agents were the leading mode of treatment for type 2 diabetics (89.3 %) while subcutaneous insulin alone was the mode in 4.1 %.
Five (3.8 %) patients were blind in the better eye while 27 (20.3 %) were visually impaired (Fig. 1). Cataract was the leading cause of blindness (60 %) and visual impairment (59.3 %) in these patients (Table 2). Apart from patients in whom diabetic retinopathy was the main visual impairment, diabetic retinopathy was still present in 4 (14.8 %). Uniocular blindness was present in 20 (15 %) of the type 2 diabetic patients; cataract 12 (60 %), glaucoma 6 (30 %), age-related macular degeneration 1 (5 %), and proliferative diabetic retinopathy 1 (5 %) were the causes of uniocular blindness. Diabetic macular edema was present in 7(35 %) of the patients with uniocular blindness.
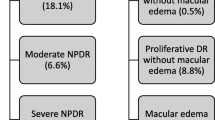
Diabetic retinopathy of varying stages was present in 37 (27.8 %) patients while the remaining 96 (72.2 %) diabetic patients studied had no evidence of diabetic retinopathy on clinical examination. Most of the diabetic retinopathy observed were non-proliferative 32 (24.1 %) while proliferative diabetic retinopathy was seen in five patients (3.8 %). Diabetic macular edema was present in 83.3 % of patients with diabetic retinopathy irrespective of the grade of retinopathy with a slightly higher prevalent in patients with non-proliferative retinopathy (86.4 %) compared with 80 % in those with proliferative retinopathy (Table 3). Diabetics with retinopathy had longer duration of diabetes (6.6 years) compared to 4.8 years in those without retinopathy (Table 4). The percentage of diabetics with severe visual impairment and blindness was higher in those with diabetic retinopathy compared with those without (Fig. 2).

Category of vision against diabetic retinopathy status
Other eye diseases apart from diabetic retinopathy were present with some eyes having more than one disorder on ocular examination. Refractive error 67 (25.2 %), cataract 63 (23.7 %), and chronic glaucoma 44 (16.5 %) were the most prevalent non-diabetic retinopathy eye diseases in the diabetics (Table 5). Vitreous and retinal diseases other than diabetic retinopathy were present in 58 (27.2 %) eyes with hypertensive retinopathy 44 (23.7 %) being the most prevalent (Fig. 3). Vitreoretinal disease including diabetic retinopathy was clinically present in 122 (45.9 %) in the cohort studied.

Non-diabetic retinopathy eye diseases in type 2 diabetic
Discussion
Type 2 diabetes mellitus is the commonest variant of the disease and it affects males as well as females. In this cohort of type 2 diabetic patients receiving care from endocrinologists with near equal distribution of males and females, obesity, and systemic hypertension were common systemic co-morbidities. Globally, hypertension and obesity, separately or together are common co-morbidities in adults with type 2 DM [30].
Blindness and visual impairment prevalence rates of 3.8 and 20.3 %, respectively, in the study population are quite high. Visual impairment is a major health issue with significant socioeconomic consequences; loss of vision is one of the most feared complications of diabetes because it results in major lifestyle modifications [6, 31]. Visual impairment is reported to be more common in patients with diabetes compared with those without diabetes [7]. The 20.3 % rate of VI in this study is much higher than the 4 % reported by Rani et al. [32] in type 2 diabetic subjects in India. Al-Till et al. [33] reported blindness rates of 7.4 % and visual impairment rates of 10.1 % among Jordanian diabetics. Cataract and glaucoma were the leading causes of blindness and visual impairment in this study; higher risk of cataract in type 2 diabetic patients have been well documented and could account for this [21, 34, 35]. Cataract is the cause of visual loss in diabetic patients [7, 32, 34]; it accounted for 61 % of visual impairment in the Sankara Nethralaya study of type 2 diabetics in India [32]. Diabetes mellitus is a risk factor for primary open angle glaucoma; this may be a probable reason for its importance as a major cause of visual impairment in this cohort [36, 37]. It is noteworthy that cataract and glaucoma are the leading causes of blindness and visual impairment in Nigeria as a whole [3]; thus persons living with diabetes mellitus have additional risks of these diseases. Cataract surgery is believed to worsen existing diabetic macular edema hence the need to ensure appropriate treatment of same perioperatively [38, 39].
Diabetic retinopathy was present in 27.8 % and proliferative disease in 3.8 % of type 2 diabetic patients in this study. This is higher than the 18 % reported in an urban population study in India; [40] a diabetic retinopathy rate of 21.9 % was however reported by Tapp et al. [20] in Australia with proliferative disease in 2.1 %. Diabetic retinopathy rate of 21.7 % was reported by Owsley et al. [14] while screening diabetics using telemedicine. Mowatt et al. [21] however reported a much higher diabetic retinopathy rate of a proliferative diabetic retinopathy rate of 78 % and proliferative disease of 50.5 %; this higher rate is likely due to the high turnover rate of patients in that referral retinal clinic. Diabetic retinopathy rate of 20.5 % was reported among diabetics in the Nigerian national blindness survey of persons aged 40 years and above [13]. The high rate of diabetic retinopathy recorded in this current study may not be unconnected to poor glycemic control as evidenced by high fasting glucose levels; suboptimal blood pressure control as well as the absence of regular screening programmes for diabetic retinopathy detection may also be contributory. Duration of diabetes is an important risk factor for development of diabetic retinopathy [13, 19–21]; in our study patients with diabetic retinopathy had diabetes for longer duration (6.6 ± 4.5 years) compared with those without retinopathy (4.8 ± 5.5 years), the difference though not statistically significant. Diabetic retinopathy remains an important cause of visual impairment and blindness in diabetic patients [42, 43]. Diabetic retinopathy accounted for 7.4 % of visual impairment in this study; this is comparable to the 9 % reported by Ranni et al. [32] in India. Severe VI and blindness were present in higher percentages in diabetics with diabetic retinopathy compared with those without retinopathy in this study. This burden of DR in addition to the low rate of dilated retinal examination to screen for DR reported in this study as well as previous study in the region [43] calls attention to focus on development of plans and policies to tackle the disease so as to prevent an escalation in blindness from DR. There is need for early DM detection, DR screening, and treatment in the community. Diabetes mellitus is believed to cause visual impairment mainly through cataract and diabetic retinopathy; hence the listing of both diseases in the nine target diseases of vision 2020 by WHO and IAPB [44]. Although the prevalence in blindness in sub Saharan Africa was reduced as at 2010, Naidoo et al. reported 2.2 % of blindness in sub Saharan Africa to be caused by diabetic retinopathy [ 45]. Large burden of eye diseases other than retinopathy was seen in this study; uncorrected refractive error, cataract, and glaucoma were the leading diseases in this cohort. Refractive error is usually correctable with spectacles; in diabetics however, it is important to ensure adequate glycemic control since both hypo and hyperglycemia have significant effect on refractive state of the eye [25, 46]. Zhang et al. [7] listed uncorrected refractive error as one of the important causes of blindness and visual impairment in diabetes mellitus in their study. Hypertensive retinopathy was the leading vitreo-retinal disease other than diabetic retinopathy; the high rate of systemic hypertension as co-morbidity is probably contributory. In all, there was a high (45.9 %) prevalence of vitreo-retinal diseases in type 2 diabetic patients. Screening for diabetic retinopathy gives additional benefits of detecting other eye diseases including vitreo-retinal diseases in such patients [41]. Holistic care of the diabetics should include diabetic eye care especially ability to detect and care for vitreo-retinal diseases.
This cross-sectional study is limited by it inability to provide data on the progression of diabetic retinopathy over time since follow-up examination was included in the study. Although stereoscopic fundus photography is “the gold standard” for diabetic retinopathy screening, only a minority of the study population underwent this procedure due to non-availability of facility in the region as well as financial limitations.
The possibility that this study could have under-diagnosed diabetic macular edema due to non-availability of facility for optical coherence tomographic examination is a limitation. The cohort of type 2 diabetics studied may represent patients with some degree of awareness about the disease since they are under specialist care and hence an underrepresentation of the eye complication burden of diabetes in the community. Almost half (48 %) of diabetics studied in the national blindness survey were not aware that they had the disease [13].
In conclusion, type 2 diabetic patients have high prevalence of visual impairment, blindness, diabetic retinopathy, and other diseases like cataract, refractive error, and glaucoma. Massive community- and institutional-based health education, early diagnosis as well as treatment of diabetic retinopathy and other diseases will largely alleviate the ocular morbidity in type 2 diabetics in the region. Community-based screening of diabetics for retinopathy and treatment is recommended.
References
Winter I, Yorston D (2011) Diabetic retinopathy: everybody’s business. Community Eye Health J 24:1–2
Van DS, Beulens JWJ, Van der SYT, Grobbee DE, Nealb B (2010) The global burden of diabetes and its complications; an emerging pandemic. Eur J Prev Cardiol 17:s3–s8
Abdull MM, Sivasubramaniam S, Murthy GVS, Gilbert C, Abubakar T, Ezelum C, Rabiu MM, on behalf of Nigeria National Blindness and Visual Impairment Study Group (2009) Causes of blindness and visual impairment in Nigeria: the Nigeria national blindness and visual impairment survey. IVOS 50:4114–4120
Hall V, Thomsein RW, Heriksen O, Lohse N (2011) Diabetes in Sub-Saharan Africa 1999–2011: epidemiology and public health implications a systematic review. BMC Public Health 11:564
International Diabetes Federation (IDF) Diabetes Atlas, 6th edn, IDF, 2014. www.idf.org. Accessed Sept 2015
Pascolini D, Marriotti SP (2011) Global estimates of visual impairment. Br J Ophthalmol 2011
Zhang X, Greff EW, Chang YJ et al (2008) Diabetes mellitus and visual impairment: national health and nutrition examination survey 1999–2004. Arch Ophthalmol 26:1421–1427
Congdon NG, Friedman DS, Lietman T (2003) Important causes of visual impairment in the world today. JAMA 290:2057–2060
Glover SJ, Burgess PI, Cohen DB et al (2012) Prevalence of diabetic retinopathy, cataract and visual impairment in patients with diabetes in sub Saharan Africa. Br J Ophthalmol 96:156–161
Jeganathan VS, Wang JJ, Wong TY (2008) Ocular associations of diabetes other than diabetic retinopathy. Diabetes Care 31:1903–1912
Farrel IC, Muran J (2014) Comparison of comorbidities in patients with prediabetes to those with diabetes mellitus type 2. Ir Med J 107:72–74
Nguyen HT, Luzio SD, Dolben J, West J, Beck L, Coates PA, Owens DR (1996) Dominant risk factors for retinopathy at clinical diagnosis in patients with type II diabetes mellitus. J Diabetes Complicat 10:211–219
Kyari F, Tafida A, Sivasubramaniam S, Murthy GV, Peto T, Gilbert CE, Nigeria National Blindness and Visual Impairment Study Group (2014) Prevalence and risk factors for diabetes and diabetic retinopathy: results from the Nigeria national blindness and visual impairment survey. BMC Public Health 14:1299
Idemyor V (2010) Diabetes in sub-Saharan Africa: health care perspectives, challenges, and the economic burden of disease. J Natl Med Assoc 102:650–653
Flessa S, Zembok A (2014) Costing of diabetes mellitus type II in Cambodia. Health Econ Rev 4:24
Bandello F, Casalino G, Loewenstein A, Goldstein M, Pelayes D, Battaglia Parodi M (2014) Pharmacological approach to diabetic macular edema. Ophthalmic Res 51:88–95
Pershing S, Enns EA, Matesic B, Owens DK, Goldhaber-Fiebert JD (2014) Cost-effectiveness of treatment of diabetic macular edema. Ann Intern Med 160:18–29
Patelli F, Radice P, Giacomotti E (2014) Diabetic macular edema. Dev Ophthalmol 54:164–173
Wang JE, Zhang RY, Chen RP et al (2013) Prevalence and risk factors for diabetic retinopathy in a high-risk Chinese population. BMC Public Health 13:633–639
Tapp RJ, Shaw JE, Harper CA, De Courten MP, Balkau B, McCarty DJ, Taylor HR, Welborn TA, Zimmet PZ, AusDiab Study Group (2003) The prevalence of and factors associated with diabetic retinopathy in Australian population. Diabetes Care 26:1731–1737
Mowatt L (2013) Diabetic retinopathy and its risk factors at the university Hospital in Jamaica. Middle East Afr J Ophthal 20:321–326
Li L, Wan XH, Zhao GH (2014) Metaanalysis of the risk of cataract in type 2 diabetes. BMC Ophthalmol 14:94–107
Murtha T, Cavellerano J (2007) The management of diabetic eye disease in the setting of cataract surgery. Curr Opin Ophthalmol 18:13–18
Patel SV, Holmes JM, Hodge DO, Burke JP (2005) Diabetes and hypertension in isolated sixth nerve palsy; a population based study. Ophthalmology 112:760–763
Lin SF, Lin PK, Chang FL, Tsai RK (2009) Transient hyperopia after intense treatment of hyperglycemia in newly diagnosed diabetes. Ophthalmologica 223:68–71
www.population.gov.ng/index.php/census. Accessed Sept 2015
Kahn Richard (2003) Follow up Report on the diagnosis of diabetes mellitus. The Expert Committee on the diagnosis and classification of diabetes mellitus. Diabetes care 26:3160–3167
World Health Organisation International statistical classification of diseases and related health problems 10th revision Current version. Version 2003 Chapter VII H54 Blindness and low vision. http://ophthaclassification.altervista.org/international-clinical-diabetic-retinopathy-disease-severity-scale/. Accessed Sept 2015
http://ophthaclassification.altervista.org/international-clinical-diabetic-retinopathy-disease-severity-scale/. Accessed Sept 2015
Colosia AD, Palencia R, Khan S (2013) Prevalence of hypertension and obesity in patients with type 2 diabetes mellitus in observational studies: a systematic literature review. Diabetes Metab Syndr Obes 6:327–338
Harris MD (2003) Psychosocial aspects of diabetes with an emphasis on depression. Curr Diabetes Rep 3:49–55
Rani PK, Raman R, Gella L, Kulothingan V, Sharma T (2012) Prevalence of visual impairment and associated risk factor in subjects with type 2 diabetes mellitus: Sankara Nethralaya diabetic retinopathy epidemiology and molecular genetic study(SN-DREAMS; Report 16). Middle East Afr J Ophthalmol 19:129–134
Al-Till MI, Al-Badour MD, Ajlouni KM (2005) Prevalence of blindness and visual impairment among Jordanian diabetics. Eur J Ophthalmol 15:62–68
Pollreisz A, Schmidt-Erfurth U (2010) Diabetic cataract pathogenesis, epidemiology and treatment. J Ophthalmol. doi:10.1155/2010/608751
Hashim Z, Zarina S (2012) Osmotic stress induced oxidative damage: possible mechanism of cataract formation in diabetes. J Diabetes Complicat 26:275–276
Bonovas S, Peponis V, Filioussi K (2004) Diabetes mellitus as a risk factor for primary open angle glaucoma; a metaanalysis. Diabet Med 21:609–614
Zhoun M, Wang W, Huang W, Zhang X (2014) Diabetes mellitus as a risk factor for open angle glaucoma; a systematic review and meta-analysis. PLoS One 9:e102972
Kim SJ, Equi R, Bressler NM (2007) Analysis of macular edema after cataract surgery in patients with diabetes using optical coherence tomography. Ophthalmology 114:881–889
Krepler K, Biowsky R, Schrey S, Jandrasits K, Wedrich A (2002) Cataract surgery in patients with diabetic retinopathy; visual outcome, progression of diabetic retinopathy and incidence of diabetic macular edema. Graefe’s Arch Clin Exp Ophthalmol 240:735–738
Raman R, Rani PK, Rachepalle SR, Uthra S, Kumaramanickavel G, Sharma T (2009) Prevalence of diabetic retinopathy in India. Sankara Nethralaya diabetic retinopathy epidemiology and molecular genetic study report 2. Ophthalmology 116:311–318
Owsley C, McGwin G Jr, Lee DJ, Lam BL, Friedman DS, Gower EW, Haller JA, Hark LA, Saaddine J, for the Innovative Network for Sight (INSIGHT) Research Group (2015) Diabetes eye screening in urban settings serving minority populations detection of diabetic retinopathy and other ocular findings using telemedicine. JAMA Ophthalmol 133:174–181
Patil S, Gogate P, Vora S et al (2014) Prevalence and causes of blindness, visual impairment and cataract surgical services in Sindhuburg district in the western coastal strip, India. Indian J Ophthalmol 62:240–245
Onakpoya OH, Adeoye AO, Kolawole BA (2010) Determinants of dilated eye examination among type 2 diabetics in Southwestern Nigeria. Eur J Int Med 21:176–179
Ellis D, Burges PH, Kayange P (2013) Management of diabetic retinopathy. Malawi Med J 25:116–120
Naidoo K, Gichuhi S, Basáñez M-G, Flaxman SR, Jonas JB, Keeffe J, Leasher JL, Pesudovs K, Price H, Smith JL, Turner HC, White RA, Wong TY, Resnikoff S, Taylor HR, Bourne RR, Vision Loss Expert Group of the Global Burden of Disease Study (2014) Prevalence and causes of vision loss in sub-Saharan Africa: 1990–2010. Br J Ophthalmol 98:612–618
Baris S, Banu B, Aysegul A, Murat I, Mehmet O, Umut S (2005) Effect of glyceamic control on refractive changes in diabetic patients with hyperglycemia. Cornea 24:531–537
Acknowledgments
Grant—Part funding by Benjamin Osuntokun Trust.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Onakpoya, O.H., Kolawole, B.A., Adeoye, A.O. et al. Visual impairment and blindness in type 2 diabetics: Ife-Ijesa diabetic retinopathy study. Int Ophthalmol 36, 477–485 (2016). https://doi.org/10.1007/s10792-015-0145-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-015-0145-8