
Abstract
In acute angle closure crisis (AAC), a laser peripheral iridotomy (LPI) is performed to balance the pressure gradient between anterior and posterior chamber. The hereby induced changes in anterior chamber architecture were analyzed using Scheimpflug photography (SP). SP was performed in eyes with AAC and in fellow eyes (FE) before and after LPI. Intraocular pressure (IOP), anterior chamber volume (ACV), anterior chamber depth (ACD), anterior chamber angle width (ACA), and central corneal thickness (CCT) were analyzed. The group consisted of 18 patients (14♀, 4♂; 69 ± 11 years) with unilateral AAC. Mean IOP in AAC eyes decreased from 49.3 ± 2.8 mmHg at presentation to 13.7 ± 1.6 mmHg after LPI (p = 0.001). Mean ACV increased from 48.2 ± 3.6 to 60.6 ± 2.4 mm3 in AAC eyes (p < 0.001) and from 60.4 ± 4.6 to 74.1 ± 3.7 mm3 in the FE (p < 0.001). Mean ACD increased from 1.27 ± 0.08 to 1.44 ± 0.06 mm (p = 0.01) in AAC eyes and decreased in FE from 1.72 ± 0.08 to 1.59 ± 0.04 mm (p = 0.5). Mean ACA increased from 16.8 ± 1.6 to 20.5 ± 1.5° in AAC eyes (p = 0.01) and from 18.5 ± 1.4 to 22.6 ± 1.5° in the FE (p = 0.01). Mean CCT did not change significantly in both groups after LPI (AAC p = 0.09; FE p = 0.9) but a statistically significant difference between the two groups was detectable before LPI (p = 0.04) which disappeared thereafter (p = 0.14). Using Scheimpflug photography, a significant difference of ACV, ACD, and ACA can be detected after LPI in eyes suffering from acute angle closure crisis which demonstrates the effectiveness of LPI.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute angle closure crisis develops by blockage of the physiological outflow pathway of aqueous from the anterior chamber via the trabecular meshwork by anteriorly displaced peripheral iris tissue. This leads to a pronounced increase of intraocular pressure (IOP) which can cause ophthalmic as well as systemic symptoms like pain, visual impairment, corneal edema, nausea, and bradycardia and can lead to persistent optic nerve damage [1]. Acute angle closure crisis has a low incidence in Caucasian populations over 30 years of age with 4.1 cases in 100,000 per year, but is relatively common worldwide especially in Asian populations [2–5].
Known risk factors for developing acute angle closure crisis are age, female gender, far eastern descent [6], short eye length [7, 8], shallow anterior chamber [9, 10], refractive errors [11] as well as an altered thickness and position of the crystalline lens [12]. The underlying mechanism can either be a pupillary block or a plateau iris syndrome. Acute angle closure crisis occurs unilaterally in most cases, but due to a high risk to develop angle closure in the fellow eye both eyes are normally treated [13].
Acute angle closure crisis is first treated with IOP-lowering drugs to normalize the IOP. To prevent further angle closure crisis, a bypass between posterior and anterior chamber is formed by which aqueous humor can directly flow into the anterior chamber and toward the trabecular meshwork. This can either be achieved by a laser peripheral iridotomy (LPI) using a disruptive laser like the Neodymium: Yttrium–Aluminum-Garnet Laser (Nd:YAG-Laser) or by surgical iridectomy.
For the diagnosis of acute angle closure crisis and angle closure suspects, gonioscopy with a contact lens has for long been the gold standard in anterior chamber angle visualization. Different modes of grading the chamber angle have been designed taking into account angle width, iris curvature, and visibility of angle structures [14–16]. But accurate gonioscopy can be fairly complex and challenging for an untrained ophthalmologist. During the last decades, different (semi-) automatic devices for anterior chamber angle visualization like ultrasound biomicroscopy (UBM), ocular coherence tomography (OCT), and Scheimpflug photography utilizing devices were developed. The Pentacam (Oculus, Wetzlar, Germany) uses Scheimpflug photography technique to completely focus planar objects which are not parallel to the image plane.
Using the Pentacam, a number of anterior segment indices can be measured like anterior chamber depth (ACD), central corneal thickness (CCT), anterior chamber volume (ACV), and anterior chamber angle (ACA) as well as a large number of refractive corneal indices. It has been described before that the Pentacam is a reliable tool for anterior segment examination with high repeatability and good intra-observer reliability [17–20]. It was the main aim of the undertaken investigation to analyze the changes in anterior chamber architecture induced by LPI in patients with one-sided angle closure crisis in the eye suffering from acute crisis and in the fellow eye.
Materials and methods
All cases of unilateral acute angle closure crisis which were referred to our emergency unit between January 2012 and June 2013 were reviewed. Acute angle closure was diagnosed clinically by slit lamp examination and IOP measurement using Goldmann applanation tonometry. Periorbital pain, marked ciliary injection, corneal edema, fixed mid-dilated pupil, visual loss, and an IOP above 30 mmHg were taken as signs supporting the acute angle closure diagnosis. Further evaluation of the anterior chamber angle was performed using van-Herrick’s test and indentation gonioscopy using a Sussman four mirror gonioscope when corneal edema cleared. The anterior chamber angle in both eyes was graded using Shaffer’s classification [14]. Best corrected visual acuity (BCVA) was measured using Snellen charts. Axial length measurements were performed using an IOL Master 5 (Carl Zeiss Meditec, Oberkochen, Germany). Before LPI, the IOP was lowered using appropriate topical and systemic medication. Eye drops containing pilocarpine, beta adrenergic blockers, and carbonic anhydrase inhibitors as well as systemic carbonic anhydrase inhibitors were therefore given.
LPI was performed when IOP was below 30 mmHg to ensure good visibility through a clear cornea. LPI was first performed in the acute angle closure eye and when this was successful in the fellow eye to avoid future development of acute angle closure crisis. Before LPI was performed, pilocarpine 1 % eye drops were administered every 5 min for 20 min and the ocular surface was anesthetized using one drop tetracain 1 %. An Yttrium–Aluminum-Garnet Laser (Nd:YAG-Laser; Alcon Surgical 3000LE) was used. Spot size was fixed at 11-µm diameter and 1 pulse per shot. The applied energy could be selected freely between 0.5 and 12 mJ. An Abraham contact lens was used for magnification and to reduce random eye movements. It was attempted to apply the LPI in the nasal superior quadrant as peripherally as possible. YAG-laser shots were applied until a gap in the iris stroma and a gush of aqueous and pigment became visible.
The Pentacam was used for the topographical analysis of the anterior segment of our acute angle closure cases. The Pentacam utilizes a Scheimpflug camera system which rotates around the eye’s visual axis taking 25 pictures per full 360° rotation. Using the software installed on the Scheimpflug camera controlling computer, the images can be analyzed. A number of anterior segment indices can be calculated such as ACD, CCT, ACV, and ACA. Examination with the Pentacam was carried out on the eye with the angle closure crisis and the fellow eye directly before and one or two days after successful LPI.
In our analysis, we evaluated ACD, CCT, ACV, and ACA from the Pentacam examinations as well as entries from the patient records such as IOP results at first appointment, before LPI and at hospital discharge as well as the powers of the worn glasses and the results from the chamber angle examination using the gonioscope.
The statistical analysis was conducted using the programs Excel© (Microsoft; Redmond, USA) and SPSS (Version 12.0; Chicago, Illinois, USA). All measured values are given as mean ± standard error of mean (SEM). Bonferroni adjusted Student’s t test for repeated measures as well as analysis of variance (ANOVA) were utilized with p < 0.05 being regarded as representing statistical significance.
Results
Between January 2012 and June 2013, 18 patients with a unilateral acute angle closure crisis sought treatment in our emergency unit. Of these 18 patients, 14 were female and 4 were male with a mean age of 69 ± 11 years (range 37–83; median: 69 years). In 10 cases, the right and in 8 cases the left eye was affected by the acute angle closure crisis. All eyes were phakic when affected by acute angle closure crisis. In 15 eyes, the lens was described as having a cataracta provecta. The remaining three eyes were described as having a clear lens. The mean spherical equivalent of the worn glasses was +0.57 ± 0.67 D for the affected eyes and −0.09 ± 0.8 D for the fellow eyes. The difference in refraction of both eyes was not statistically significant (p = 0.37). The mean exact refraction of the affected eyes was +0.29 ± 0.8 D and −0.22 ± 0.6 D in the fellow eyes. Axial length measurements revealed a mean length of 22.17 ± 0.27 mm in the eyes suffering from acute angle closure crisis. BCVA was 0.89 ± 0.12 logMAR at first visit which increased to 0.51 ± 0.11 logMAR at the end of treatment.
No eye was beforehand treated for increased IOP or underwent previous intraocular surgery. After LPI was carried out successfully, the pupil was dilated and the optic disk was examined. No eye showed apparent glaucomatous optic disk changes. During examination of the eyes suffering from acute angle closure crisis using the gonioscope, 40 quadrants were graded as Shaffer 0 with no visible angle structures and the remaining 32 quadrants either as Shaffer grade 1 or grade 2 with visible Schwalbe line or visible trabecular meshwork. In the fellow eyes, we found 16 quadrants of Shaffer grade 1, 48 quadrants Shaffer grade 2, and 8 quadrants Shaffer grade 3.
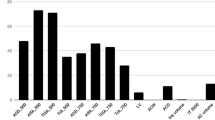
The mean IOP upon first presentation was 49.3 ± 2.8 mmHg in the eyes suffering from acute angle closure crisis. The mean IOP in the fellow eyes was 15.2 ± 0.9 mmHg. The difference in IOP between diseased and healthy eye was statistically significant at this point in time (p = 0.001). After treatment with pressure-lowering medication, the mean IOP was 14.6 ± 1.8 mmHg in the eyes with angle closure crisis and 12.7 ± 0.6 mmHg in the fellow eyes which showed no statistical significant difference (p = 0.32). After successful LPI and reduction of pressure-lowering medication, the mean IOP remained physiological with 13.7 ± 1.6 mmHg in the eyes formerly suffering from acute angle closure crisis and 12.9 ± 0.7 mmHg in the fellow eyes. Again the difference in IOP between angle closure eyes and fellow eyes was not statistically significant (p = 0.71). When comparing the IOP measured in the 18 eyes which suffered from acute angle closure crisis before the beginning of treatment and before LPI, a statistically significant difference can be found (p = 0.001). The difference of IOP in these eyes before the beginning of treatment and after LPI was also statistically significant (p = 0.001) (Fig. 1).

Mean IOP in the 18 angle closure crisis eyes at first contact, before and after LPI. Mean IOP results before and after LPI are significantly different from the IOP measured at first presentation in the eye clinic
The mean CCT in the eyes suffering from acute angle closure crisis was 635 ± 24 µm before and 604 ± 14 µm after successful LPI. The mean CCT measured in the fellow eyes was 573 ± 9 µm before and 575 ± 9 µm after successful LPI. The difference of CCT before and after LPI was not statistically significant (p = 0.09) in the eyes with the acute angle closure crisis, although a trend toward statistical significance can be seen. As in the angle closure eyes, the change of CCT was not statistically significant in the fellow eyes (p = 0.9). However, when comparing the mean CCT of the eyes suffering from acute angle closure crisis with the fellow eyes before LPI, a statistically significant difference can be found (p = 0.04). This statistically significant difference of CCT values between the fellow eyes and the eyes with acute angle closure crisis disappeared after successful LPI (p = 0.14) (Fig. 2).

Mean CCT in the 18 eyes suffering from angle closure crisis and in the 18 fellow eyes. The difference between mean baseline CCT of eyes suffering from acute angle closure crisis compared to the fellow eyes is statistically significant
The mean ACV in the 18 eyes with angle closure crisis was 48.2 ± 3.6 mm3 directly before LPI which increased to 60.6 ± 2.4 mm3 thereafter. This change of ACV was statistically significant (p < 0.001). In the 18 fellow eyes, the mean ACV also increased from pre- to post-LPI from 60.4 ± 4.6 to 74.1 ± 3.7 mm3. The change of ACV from pre- to post-LPI was also statistically significant in the fellow eyes (p < 0.001). However, when comparing the mean ACV of both groups—angle closure eyes and fellow eyes—the difference between groups was also statistically significant at the point in time directly before and after successful LPI (pre: p = 0.04; post: p = 0.03) (Fig. 3).

Mean ACV for the 18 eyes suffering from angle closure crisis and the 18 fellow eyes before and after LPI. Mean ACV values found in both groups after LPI are significantly different from baseline values
The mean ACD in the eyes suffering from angle closure crisis was 1.27 ± 0.08 mm before LPI, which increased to 1.44 ± 0.06 mm after LPI. This difference was statistically significant (p = 0.01). However, in the 18 fellow eyes, the mean ACD decreased from 1.72 ± 0.08 mm before to 1.59 ± 0.04 mm after LPI. This change showed no statistical significance (p = 0.49). When comparing the mean ACD in the eyes suffering from acute angle closure crisis with the mean ACD in the fellow eyes before and after LPI, the difference between both groups was statistically significant before LPI (p = 0.02) and lost statistical significance thereafter (p = 0.08) (Fig. 4).

Mean ACD in eyes with acute angle closure crisis and fellow eyes before and after LPI. The difference of mean ACD before and after LPI in the 18 eyes suffering from acute angle closure crisis was statistically significant
The mean ACA increased through LPI in the 18 eyes affected by acute angle closure crisis from 16.8 ± 1.6 to 20.5 ± 1.5°. In the fellow eyes, LPI induced an increase of chamber angle width from 18.5 ± 1.4 to 22.6 ± 1.5°. The difference of chamber angle width in the 18 eyes after acute angle closure crisis before and after LPI was statistically significant (p = 0.03). This corresponding difference in the fellow eyes was also statistically significant (p = 0.01). When comparing the chamber angle width in between eyes before and after LPI, we found no statistically significant difference at the point in time before (p = 0.1) and after carrying out the peripheral LPI (p = 0.2) (Fig. 5).

Mean ACA in eyes with acute angle closure crisis and fellow eyes before and after LPI. The difference between mean ACA before and after LPI was statistically significant in the 18 eyes suffering from acute angle closure crisis and in the 18 fellow eyes
Conclusions
We used Scheimpflug photography to analyze the changes induced by LPI in the anterior segments of patients suffering from unilateral angle closure crisis. Therefore, we performed Pentacam examinations directly before and 1 day after LPI in eyes suffering from acute angle closure and in fellow eyes to analyze the changes induced in either eye and to compare both eyes. We found a statistically significant decrease of IOP from the time point before the beginning of IOP-lowering treatment to measurements performed before and after LPI. Initially, we also found a statistically significant difference in CCT between the eye suffering from acute angle closure and the fellow eye which disappeared after successful LPI. We ascribed this finding to the corneal edema usually found in eyes with elevated IOP. In the 18 eyes with acute angle closure crisis as in the fellow eyes, we found a significant increase of ACV and ACA after LPI. Lastly, we also found a significant increase of ACD in the angle closure eyes which we could not demonstrate in the 18 fellow eyes. The decrease of ACD in the fellow eyes was small and not significant but might be regarded as a side effect of pilocarpine treatment which was given to place the LPI as peripherally as possible. We explained the discrepancy between the refractive power of the worn glasses, the exact refraction, and the axial length measurements of our patients with the increasing myopisation of the senile cataractic lenses. The cataractic lenses and the hereby caused myopisation seem to masquerade the decreased mean axial length of the eyes suffering from acute angle closure crisis. Altogether, we could demonstrate pronounced changes of anterior segment architecture in eyes suffering from acute angle closure and in fellow eyes which were induced by LPI.
We are the first to describe the changes of anterior segment architecture induced by LPI in such a large group consisting entirely of patients suffering from unilateral acute angle closure crisis in a group of Caucasian patients. It has been shown before in other patient populations of angle closure suspects from various cultural backgrounds that performing a LPI can lead to increasing ACV and ACA. Using Scheimpflug photography in a group of 37 Canadian primary angle closure suspects, LPI leads to a significant increase of ACV and ACA but left ACD unchanged [21]. The same was previously described in a group of 20 Italian patients who underwent LPI due to a high risk of developing acute angle closure [22]. Jain et al. [23] found in 68 patients of Indian descent which were treated with LPI for primary angle closure that LPI leads to a significant increase of ACV and peripheral anterior chamber depth but not central anterior chamber depth using Scheimpflug photography. Li et al. [24] found a significant increase of ACD after LPI in 37 eyes of 25 Chinese patients using Scheimpflug photography, whereas only three eyes had acute angle closure crisis and the remaining eyes where suspected to have angle closure.
Anterior segment optical coherence tomography (AS-OCT) is an alternative for non-contact examination of the anterior segment architecture with high reproducibility [25, 26]. The main advantage of AS-OCT over Scheimpflug photography is its ability to image anterior segment structures directly because a laser beam is utilized that penetrates tissues to a certain degree. With Scheimpflug photography techniques, this is not possible due to the utilized optical methods and the total internal reflectivity of the cornea that makes direct visualization of the chamber angle impossible.
Karandish et al. [27] showed that LPI increases chamber angle width and flattens the peripheral iris in three eyes with acute angle closure and 10 eyes with narrow chamber angle using AS-OCT. The same could be demonstrated in 71 eyes of 71 Caucasian patients with primary angle closure, primary angle closure glaucoma, and primary angle closure suspects by Ang and Wells using an AS-OCT system [28]. See et al. [29] found an increase of ACA width but no change of ACD in 17 eyes of 17 patients with suspected primary angle closure, primary angle closure, or primary angle closure glaucoma using AS-OCT. Using the AS-OCT in a group of 84 eyes of 52 angle closure suspects, it could be found that prophylactic LPI causes ACA to increase significantly and that narrower angles at baseline before LPI are associated with a more pronounced increase of ACA than wider angles [30]. Lee et al. [31] could show that anterior chamber area and ACA increase after LPI in 32 eyes of 32 primary angle closure suspects but decreases again thereafter so that 18 months after LPI, a group of ACA indices are not statistically different from their pre-LPI values anymore.
The main disadvantage of the above mentioned studies concerning anterior chamber architecture evaluation using AS-OCT methods was that measurements were only carried out using a single horizontal scan through the nasal and temporal quadrants. Extrapolating from two locations over the complete anterior chamber angle seems hardly sufficient. Apart from this, it seems hardly feasible to compare ACA width before and after LPI at the exact same locations on single AS-OCT scans and was therefore criticized before.
With the presented data from examinations using Scheimpflug photography, we could show that anterior segment architecture changes drastically after LPI in patients suffering from acute angle closure crisis. In our group of patients, which is to our knowledge the biggest group of patients of Caucasian heritage and acute unilateral angle closure crisis published so far, we could show that LPI leads to a significant increase of ACV, ACA, and ACD. Future investigations should be undertaken to analyze the long-term development of anterior chamber architecture after LPI in former angle closure crisis patients and to establish threshold values for when to recommend prophylactic LPI for patients with narrow anterior chamber angles.
References
Aung T, Husain R, Gazzard G, Chan YH, Devereux JG, Hoh ST, Seah SK (2004) Changes in retinal nerve fiber layer thickness after acute primary angle closure. Ophthalmology 111:1475–1479
Bonomi L, Marchini G, Marraffa M, Bernardi P, De Franco I, Perfetti S, Varotto A (2000) Epidemiology of angle-closure glaucoma: prevalence, clinical types, and association with peripheral anterior chamber depth in the Egna-Neumarket Glaucoma Study. Ophthalmology 107:998–1003
Klein BE, Klein R, Sponsel WE, Franke T, Cantor LB, Martone J, Menage MJ (1992) Prevalence of glaucoma. The beaver dam eye study. Ophthalmology 99:1499–1504
Quigley HA (1996) Number of people with glaucoma worldwide. Br J Ophthalmol 80:389–393
Ramesh S, Maw C, Sutton CJ, Gandhewar JR, Kelly SP (2005) Ethnic aspects of acute primary angle closure in a UK mulicultural conurbation. Eye 19:1271–1275
Seah SK, Foster PJ, Chew PT, Jap A, Oen F, Fam HB, Lim AS (1997) Incidence of acute primary angle-closure glaucoma in Singapore. An island-wide survey. Arch Ophthalmol 115:1436–1440
Sihota R, Lakshmaiah NC, Agarwal HC, Pandey RM, Titiyal JS (2000) Ocular parameters in the subgroups of angle closure glaucoma. Clin Exp Ophthalmol 28:253–258
Sun X, Ji X, Zheng Y, Guo B (1994) Primary chronic angle-closure glaucoma in Chinese—a clinical exploration of its pathogenesis and natural course. Yan Ke Xue Bao 10:176–185
Alsbirk PH (1974) Anterior chamber depth in Greenland Eskimos. I. A population study of variation with age and sex. Acta Ophthalmol (Copenh) 52:551–564
Foster PJ, Alsbirk PH, Baasanhu J, Munkhbayar D, Uranchimeg D, Johnson GJ (1997) Anterior chamber depth in Mongolians: variation with age, sex, and method of measurement. Am J Ophthalmol 124:53–60
Lowe RF (1970) Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angle-closure glaucoma. Br J Ophthalmol 54:161–169
Lowe RF, Clark BA (1973) Radius of curvature of the anterior lens surface. Correlations in normal eyes and in eyes involved with primary angle-closure glaucoma. Br J Ophthalmol 57:471–474
Snow JT (1977) Value of prophylactic peripheral iridectomy on the second eye in angle-closure glaucoma. Trans Ophthalmol Soc UK 97:189–191
Shaffer RN (1960) Primary glaucomas. Gonioscopy, ophthalmoscopy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 64:112–127
Scheie HG (1957) Width and pigmentation of the angle of the anterior chamber; a system of grading by gonioscopy. AMA Arch Ophthalmol 58:510–512
Spaeth GL (1971) The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Soc UK 91:709–739
Shankar H, Taranath D, Santhirathelagan CT, Pesudovs K (2008) Anterior segment biometry with the Pentacam: comprehensive assessment of repeatability of automated measurements. J Cataract Refract Surg 34:103–113
Chen D, Lam AK (2009) Reliability and repeatability of the Pentacam on corneal curvatures. Clin Exp Optom 92:110–118
Miranda MA, Radhakrishnan H, O’Donnell C (2009) Repeatability of oculus pentacam metrics derived from corneal topography. Cornea 28:657–666
Kawamorita T, Uozato H, Kamiya K, Bax L, Tsutsui K, Aizawa D, Shimizu K (2009) Repeatability, reproducibility, and agreement characteristics of rotating Scheimpflug photography and scanning-slit corneal topography for corneal power measurement. J Cataract Refract Surg 35:127–133
Talajic JC, Lesk MR, Nantel-Battista M, Harasymowycz PJ (2013) Anterior segment changes after pilocarpine and laser iridotomy for primary angle-closure suspects with scheimpflug photography. J Glaucoma 22(9):776–779
Antoniazzi E, Pezzotta S, Delfino A, Bianchi PE (2010) Anterior chamber measurements taken with Pentacam: an objective tool in laser iridotomy. Eur J Ophthalmol 20:517–522
Jain R, Grewal D, Grewal SP (2013) Quantitative analysis of anterior chamber following peripheral laser iridotomy using Pentacam in eyes with primary angle closure. Eur J Ophthalmol 23(1):55–60
Li S, Wang H, Mu D, Fu J, Wang X, Wang J, Wang N (2010) Prospective evaluation of changes in anterior segment morphology after laser iridotomy in Chinese eyes by rotating Scheimpflug camera imaging. Clin Exp Ophthalmol 38:10–14
Muller M, Dahmen G, Porksen E, Geerling G, Laqua H, Ziegler A, Hoerauf H (2006) Anterior chamber angle measurement with optical coherence tomography: intraobserver and interobserver variability. J Cataract Refract Surg 32:1803–1808
Muller M, Geerling G (2008) Anterior segment optical coherence tomography in glaucoma. Klin Monatsbl Augenheilkd 225:194–199
Karandish A, Wirbelauer C, Haberle H, Pham DT (2006) OCT-goniometry before and after iridotomy in angle-closure glaucoma. Ophthalmologe 103:35–39
Ang GS, Wells AP (2010) Changes in Caucasian eyes after laser peripheral iridotomy: an anterior segment optical coherence tomography study. Clin Exp Ophthalmol 38:778–785
See JL, Chew PT, Smith SD, Nolan WP, Chan YH, Huang D, Zheng C, Foster PJ, Aung T, Friedman DS (2007) Changes in anterior segment morphology in response to illumination and after laser iridotomy in Asian eyes: an anterior segment OCT study. Br J Ophthalmol 91:1485–1489
Lee RY, Kasuga T, Cui QN, Huang G, He M, Lin SC (2013) Association between baseline angle width and induced angle opening following prophylactic laser peripheral iridotomy. Invest Ophthalmol Vis Sci 54:3763–3770
Lee KS, Sung KR, Shon K, Sun JH, Lee JR (2013) Longitudinal changes in anterior segment parameters after laser peripheral iridotomy assessed by anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci 54:3166–3170
Conflict of interest
No conflicting relationship exists for any author.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Unterlauft, J.D., Yafai, Y. & Wiedemann, P. Changes of anterior chamber architecture induced by laser peripheral iridotomy in acute angle closure crisis. Int Ophthalmol 35, 549–556 (2015). https://doi.org/10.1007/s10792-014-9982-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-014-9982-0