
Abstract
The purpose of this study was to evaluate optic nerve head (ONH) differences of the patients with Alzheimer’s disease (AD) measured by confocal scanning laser tomography [Heidelberg Retina Tomograph (HRT) III] and compare with glaucoma and control subjects. Eighty-four patients were enrolled into the study: 44 eyes of 24 patients with mild to moderate AD (Group 1), 68 eyes of 35 patients with glaucoma (Group 2), and 49 eyes of 25 heathy volunteers as a control (Group 3). A complete ophthalmologic examination as well as a confocal scanning laser ophthalmoscopic assessment with HRT III were performed on all patients. Mean values of the ONH topographic parameters such as rim area (RA), rim volume (RV), height variation contour, linear cup/disc ratio, cup shape measure, and retinal nerve fiber layer (RNFL) were recorded. Mean values of RNFL thickness was 0.23 ± 0.07 in AD, 0.22 ± 0.09 in glaucoma and 0.24 ± 0.07 in the control group (p = 0.323). RA and RV were significantly lower, and linear C/D ratio was significantly higher in the glaucoma group when compared to AD and control (p < 0.05). There was no statistically significant difference between AD and control for the optic disc parameters tested (p > 0.05). We observed a negative correlation of the age with RNFL in all of the groups (p < 0.005). Age was the most important parameter affecting RNFL. Our results suggest that HRT does not demonstrate ONH differences between AD and control group, while it successfully differentiates glaucoma from AD and control cases of older age.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Alzheimer’s disease (AD) is the major cause of dementia in the world [1]. Patients with AD demonstrate severe deficits in memory with cortical features of language difficulty and visuomotor spatial deficits. Visual abnormalities have been described in AD, which include deficits in stereopsis, color vision, contrast sensitivity, and motion detection [1, 2].
Glaucoma is characterized by a chronic, slowly progressive loss of retinal ganglion cells and their neurons. The disease is associated with remodeling of the optic nerve head (ONH) and the retina leading to the major clinical signs: characteristic ONH cupping and visual field defects [3]. A possible relationship between glaucoma and AD has been suggested, because there are similarities in the process leading to retinal ganglion cell death in both diseases [4–9].
As the retina shares many features with the brain, it may provide an easily accessible and non-invasive way of examining pathology in the brain. The application of imaging technologies such as optical coherence tomography has gained popularity recently in neuro-ophthalmology. Thinning of the peripapillary retinal nerve fiber layer (RNFL) has been detected in patients with optic neuritis, multiple sclerosis, neuromyelitis optica, AD, and Parkinson’s disease [10–12]. Findings that indicate loss of retinal ganglion cells may reflect neurodegenerative change in the brain in these conditions. That is why it is considered that RNFL thickness may be used as a biological marker [13–15].
Heidelberg Retina Tomograph (HRT, Heidelberg Engineering GmBH, Heidelberg, Germany) is a confocal scanning laser ophthalmoscope that provides quantitative, objective, and highly reproducible 3-dimensional images of the ONH, and the combination of disc parameters can discriminate between the glaucomatous and the healthy optic discs with reasonable sensitivity and specificity [16, 17]. As glaucoma is a frequently established cause of peripapillary nerve fiber loss in the older age group, it may be useful to discriminate the optic nerve findings between glaucoma and AD. In this study, our aim was to evaluate ONH differences of the patients with AD-type dementia measured with HRT and compare with glaucoma, and control subjects.
Materials and methods
Eighty-four patients were enrolled into this cross-sectional study: 44 eyes of 24 patients with mild to moderate AD (Group 1), 68 eyes of 35 patients with glaucoma (Group 2), and 49 eyes of 25 heathy volunteers as a control (Group 3). Group 1 was constituted from the patients who met the criteria for the diagnosis of AD according to diagnostic and statistical manual of mental disorders, 4th edition [18]. Cognitive decline and severity of dementia was defined by a range of scores on the mini-mental state examination (MMSE) as mild (MMSE scores between 20 and 24) and moderate (MMSE scores between 11 and 19) [18]. Group 2 was constituted from the patients attending to the glaucoma section in our clinic. All patients in Group 2 were using antiglaucomatous medication during the study. Each patient provided written informed consent; the study followed principles in the Declaration of Helsinki and was approved by the ethics committee.
Detailed neurological tests were made for the patients in Group 1. Patients with ocular diseases and systemic disorders affecting vision, previous history of diabetes, optic neuritis, or cranial disease effecting visual pathways were excluded. During the ophthalmic examination, all subjects had measurement of best-corrected visual acuity (BCVA) performed by Snellen charts, slit-lamp examination, applanation tonometry, gonioscopy, and fundus examination before HRT testing.
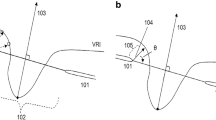
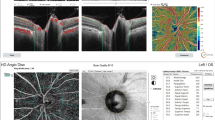
ONH was imaged with HRT III. The screenings were made with 15 × 15° angle and 50-μm reference plane. The device acquired a series of 64 consecutive, 384 × 384 pixel resolution images and produced a single topographic image. Before image acquisition, refractive error and keratometry readings were obtained and entered into the HRT III software to help correction of magnification errors. After the screening, optic disc contour line was marked and drawn at mean 5–6 points, and optic disc topographic assays were done with the image analysis program. All study participants underwent HRT III tests obtained through undilated eyes by two ophthalmologists and only recordings that had topographic standard deviation (SD) of less than 30 µm were included. All recordings were analyzed using HRT III software version 2.0.1. Rim area (RA), rim volume (RV), linear cup/disc (linear C/D) ratio, mean RNFL thickness, cup shape measure (CSM), and height variation contour (HVC) values were recorded for each case. Software analysis programs of Moorfields regression analysis and glaucoma probability scores (GPS) were used for classification of eyes as normal, borderline, or abnormal.
Statistical analyses were made with number cruncher statistical system (NCSS) 2007 and power analysis and sample size (PASS) 2008 Statistical Software (Utah, USA) program on the computer. When evaluating the parameters other than definitive statistical methods (mean, median, SD, ratio) One-way ANOVA test and Tukey HSD, Kruskal–Wallis and Mann–Whiney U tests, Pearson χ 2 test, and Yates continuity correction were used for the comparison of the groups. Spearman rank and linear regression analysis (Pearson’s test) were used to evaluate the correlations. Data were expressed as mean ± SD. Results were evaluated at p < 0.05 significance level.
Results
Characteristics of the patients [age, mean values for BCVA, intraocular pressure (IOP), and gender] according to the groups are shown in Table 1. There was a statistically significant difference for age between the groups. The mean age of the glaucoma group was significantly younger than AD group (p = 0.001) but no difference was observed between AD and control (p = 0.153) or glaucoma and control groups (p = 0.052). There was no significant difference between the groups for the gender (p = 0.395). The mean BCVA in AD group was significantly lower compared to glaucoma group (p = 0.044). IOP was significantly higher in the glaucoma compared to AD and control groups (p = 0.001).
Glaucoma subjects mean automatic full threshold perimetry (30/2 Humphrey) mean deviation (MD) was 7.76 ± 8.8, and pattern standard deviation (PSD) was 4.84 ± 2.9. Glaucoma stage was defined as 66.2 % mild, 12.1 % moderate, and 21.6 % severe according to the visual field defects with the Hodapp-Parrish-Anderson method in the glaucoma patients [19].
HRT III parameters according to the groups are shown in Table 2. Mean values of RA were 1.53 ± 0.33 mm2 in AD group, 1.32 ± 0.44 mm2 in glaucoma group, and 1.62 ± 0.34 mm2 in control group (p = 0.001). RV values were 0.42 ± 0.15 mm3 in AD group, 0.34 ± 0.17 mm3 in glaucoma group, and 0.45 ± 0.19 mm3 in control group (p = 0.004). RA and RV were significantly lower in glaucoma group when compared with AD (p = 0.017, p = 0.036) and control groups (p = 0.001, p = 0.013). And there was no statistically significant difference for RA and RV between AD and glaucoma groups (p = 0.514, p = 0.654). Mean values of HVC were 0.34 ± 0.09 in AD, 0.40 ± 0.15 in glaucoma, and 0.39 ± 0.11 in control group. There was no statistically significant difference in the mean values of HVC between the groups (p = 0.585). Mean values of RNFL thickness were 0.23 ± 0.07 mm in AD, 0.22 ± 0.09 mm in glaucoma, and 0.24 ± 0.07 in control group (p = 0.323). There was no statistically significant difference in mean values of RNFL thickness between the groups (p > 0.05). Mean values of linear C/D ratio were 0.42 ± 0.14 in AD, 0.52 ± 0.22 in glaucoma, and 0.36 ± 0.18 in control groups (p = 0.002). Linear C/D ratio was significantly higher in glaucoma group when compared with AD (p = 0.022) and control groups (p = 0.001). There was no statistically significant difference in the mean values of linear C/D ratio between AD and control groups (p = 0.194). Mean values of CSM were −0.16 ± 0.06 in AD, −0.14 ± 0.09 in glaucoma, and −0.18 ± 0.07 in control groups (p = 0.021). Mean values of CSM were significantly higher in the glaucoma when compared with control group (p = 0.007). There was no statistically significant difference in mean values of CSM between AD and glaucoma (p = 0.227) or AD and control groups (p = 0.130).
During the Moorfields analysis, abnormal result ratios (outside normal) were 4.1 % for AD, 37.8 % for glaucoma, and 0 % for control group (p = 0.001). When borderline results were included to outside normal results, they were 14.5 % for AD, 51.3 % for glaucoma, and 6.6 % for control groups (p = 0.001).
GPS analysis abnormal result ratios (outside normal) was 16.6 % for AD, 39.1 % for glaucoma, and 6.6 % for control groups (p = 0.001). When borderline GPS results were included to outside normal results, they were 41.6 % for AD, 71.4 % for glaucoma, and 33.3 % for control groups (p = 0.001).
When we evaluated the correlation of the age with the HRT parameters we tested, we observed a negative correlation of the age with RNLF in the AD group (r = −0.351, p = 0.026), glaucoma group (r = −0.357, p = 0.003), and control group (r = −0.448, p = 0.002). We observed no significant correlation of age with RA, HVC, linear C/D, or CSM (p > 0.05) (Table 3).
MMSE value of the patients in AD group was 21.91 ± 3.27. Sixteen patients were defined as mild AD, and eight patients were defined as moderate AD. We examined the correlation between MMSE and HRT III parameters (RA, RV, linear C/D, CSM, HVC, RNFL) in the AD patients. We did not observe a significant correlation between the HRT III parameters and MMSE (p > 0.05). When we compared mild and moderate AD patients, no significant difference was observed for the HRT parameters tested (p > 0.05).
Discussion
AD is a chronic disorder characterized by a progressive decline in cognitive functions [20].
Histological examinations of postmortem retinas and optic nerves have suggested that retinal ganglion cells and their axons atrophy and die in AD [21–23]. Similar to idiopathic glaucoma, large axons were generally reported to be lost preferentially in AD [21–24]. The presence of optic neuropathy was recently confirmed in the optic nerves of the patients with AD by demonstrating greatly reduced immunostaining for neurofilament protein as compared to controls, which is interpreted as a large loss of axons [25]. Some authors suggest that optic nerve degeneration is not a feature of AD and the visual deficits in the disease result from cortical dysfunction [26].
Optic nerve degeneration presents clinically in patients with mild to moderate AD as impaired visual acuity [8], poor contrast sensitivity [27], and color vision deficiencies [28]. In patients with the early stages of AD and normal routine ophthalmological examination results, dysfunction of the pattern electroretinogram, and pattern visual evoked potential tests has been observed, indicating the presence of dysfunctions of retinal ganglion cells and optic nerve [10, 29]. In our study, the mean BCVA was significantly lower in Group 1 (AD group) when compared to Group 2 (Glaucoma group) (p = 0.044), while we observed no significant difference between Group 1 and Group 3 (Control group). As Group 2 (63.9 ± 9 years) are younger than Group 1 (71.51 ± 8. 83 years) in the present study, trace cataracts which is common in the aged population may be responsible for this difference.
It has been hypothesized that there might be a causal relationship between AD and glaucoma that may be explained by decreased cerebrospinal fluid pressure (CSFP). An abnormal high trans-lamina cribrosa pressure difference, whether the result of elevated IOP, reduced CSFP, or both, is considered to play an important role in glaucomatous optic nerve damage. It was also reported that a substantial proportion of AD patients has very low CSFP which may explain how the nerves of AD in general might have differed from controls [30].
Recent technical advancements prompted a still ongoing systematic re-investigation of retinal and optic nerve involvement in neurodegenerative disorders. Three technologies for imaging the optic disc and RNFL used in the literature are (1) confocal scanning laser tomography with the HRT; (2) confocal scanning laser polarimetry with the GDx VCC; and (3) optical coherence tomography with time domain OCT or spectral domain OCT. Each uses different principles of physics for the analysis of optic nerve, RNFL, and macula [31]. We used the HRT III to measure ONH parameters because it is specific for glaucoma. Optic nerve topographic changes and structural damage from glaucoma detected with confocal laser image analysis were evaluated in many previous studies, and optic disc HRT parameter values of cup area, RA, and C/D ratio were found to change in patients converting to early glaucoma [32, 33]. HRT has also been demonstrated to be successful in detecting functionally relevant changes in RNFL thickness and neuroretinal RV in neuro-ophthalmologic diseases such as optic neuritis and multiple sclerosis [34, 35].
Conflicting reports have emerged about the ONH parameters in AD patients with different instruments. Danesh-Meyer et al. demonstrated a reduction in the number of optic nerve fibers in patients with AD, with a threefold greater odds ratio for a larger optic C/D ratio in patients with AD [36]. They compared the ONH of 40 patients with AD and of 50 age- and sex-matched controls both by scanning laser ophthalmoscopy (SLO) and by clinical funduscopy. Patients and controls differed in mean vertical C/D ratio, RV, RA, and RNFL thickness. On the other hand, Kergoat and colleagues [37] failed to find differences in the ONH parameters between early stages of AD and age-matched subjects measured with HRT.
Berisha et al. have reported the only study evaluating the localized RNFL changes and ONH parameters using Stratus OCT in patients with early glaucoma (mean age: 71), AD (mean age: 76), and age-matched control participants (mean age: 72) [38]. Their glaucoma patients showed significantly increased vertical and horizontal C/D ratios compared with both AD patients and controls (p < 0.01). No significant differences in the ONH parameters were found between AD patients and healthy controls. The average RNFL thickness values were 80.7 ± 7.0 µm in glaucoma, 83.2 ± 13.6 µm in AD, and 93.8 ± 9.3 µm in controls. The differences did not reach the level of statistical significance. However, when RNFL thickness was evaluated in the separate quadrants, a significant thinning was found at the superior quadrant in AD patients compared with glaucoma and control subjects. RNFL thickness at the inferior quadrant in glaucoma patients was significantly reduced compared with both AD patients and controls. In our study, there was no statistically significant difference between Group 1 (AD group) and Group 3 (Control group) for the optic-to-disc parameters: mean vertical CDR (0.42 for AD to 0.36 for control), RV (0.42 for AD to 0.45 for control), RA (1.53 for AD to 1.62 for control), and RNFL thickness (0.23 for AD to 0.24 for control) (p > 0.05). RA and RV were significantly lower, and linear C/D ratio was significantly higher in Group 2 (Glaucoma group) when compared with Group 1 and Group 3 (p < 0.05). Our ONH parameters other than segmental RNFL differences were similar to the findings of Berisha et al.
There are a few reports measuring RNFL with OCT in AD patients which may have advantages in their ability to measure RNFL directly. Parisi et al. found a significant reduction in RNFL thickness in mild AD (with the age range of 63–77) using a Stratus OCT [39]. In another study, Parisi reported that the patients affected by ocular hypertension, glaucoma, demyelinating optic neuritis, and AD have a reduction of RNFL thickness evaluated by OCT, and this morphological involvement is correlated with electrophysiological responses assumed to be originating from the innermost retinal layers [10]. Iseri et al. measured RNFL thickness, macular thickness, and macular volume with OCT and cognitive impairment through the MMSE [40]. They observed a reduction of parapapillary and macular RNFL thickness and macular volume in the patients with AD which was related to the severity of cognitive impairment. He et al. investigated the RNFL thickness measured with Stratus OCT between AD patients and age–sex-matched control groups in a meta-analysis including seven studies [41]. Their meta-analysis showed that in AD patients, there was a significant RNFL thickness reduction in all quadrants compared with the healthy control group. Kirbas et al. [42] Investigated RNFL thickness in patients with early untreated AD (mean age was 69.3 ± 4.9 years) and healthy controls (mean age was 68.9 ± 5.1 years) using spectral domain OCT. The average RNFL thickness was significantly less in the AD patients than in controls with a selective thinning in the superior quadrant on the AD patients. On the other hand, Kergoat et al. has found no differences in RNFL thickness between AD and healthy subjects using scanning laser polarimetry. The regional distribution of RNFL thickness was similar between the two test groups in their study [43].
In our study, global RNFL thicknesses were 0.23 ± 0.07 in Group 1, 0.22 ± 0.09 in Group 2, and 0.24 ± 0.07 in Group 3 (p = 0.323). There was no statistically significant difference in mean values of RNFL thickness between groups (p ≥ 0.05). We analyzed global RNFL and not segments during this study while the papers with OCT mostly broke down the retina into periphery, central, superior, inferior, temporal, and nasal, and some authors observed mostly superior quadrant differences [37, 38].
Our results in the Group 1 were different from the previous studies with OCT but similar to Kergoat’s studies with HRT and scanning laser polarimetry [37, 43]. The HRT differs significantly from OCT used in other publications finding decreases in RNFL. It has differences both in technical aspects and analysis/algorithms. HRT employs confocal scanning diode technology to provide topographical measures of the optic disc and peripapillary retina. The technology provides information such as cup surface area and volume, RV, and C/D ratio. The RNFL thickness measurement is calculated indirectly using the mean HVC measurements relative to an individual-based reference plane. However, OCT can both image the ONH and determine directly the RNFL thickness. In ONH scans, the OCT machine automatically defines the disc margin as the place where the retinal pigment epithelium ends. RNFL thickness is measured by the difference in temporal delay of back-scattered light from the RNFL and a reference beam [44]. Studies also differ in the region observed and retina may tend to show more differences than disc itself. The number of the subjects and the severity of the dementia also vary. We think that these technical and regional differences may be responsible for the different results for RNFL in AD.
The RNFL seemed to be involved early during the course of mild cognitive impairment (MCI) which may represent a transition to early AD [45]. Paquet et al. have demonstrated that RNFL thickness was reduced in patients with MCI, mild AD, or moderate to severe AD compared to controls with no statistical difference between the results in MCI patients and mild AD patients [46]. In our study, we did not observe a significant correlation between the HRT III parameters and MMSE (p > 0.05);
HRT is a structural test, which requires less cooperation from the subjects than do functional examinations [47]. The use of HRT offers an advantage of using its automated software scoring systems, GPS, and Moorfields regression analysis. In our study, Moorfields analysis abnormal result ratios (outside normal) wereas 4.1 % for Group 1, 37.8 % for Group 2, and 0 % for Group 3 (p = 0.001), while they were 16.6 % for Group 1, 39.1 % for Group 2, and 6.6 % for Group 3 during GPS analysis (p = 0.001). According to this, software scoring systems seem to be sensitive to discriminate Group 1 and Group 3 from Group 2.
Duration and severity of AD and most importantly age probably affect optic nerve findings. Studies reported a decline in peripapillary RNFL thickness with age [48]. Older age has been found to be independently associated with a greater cup, smaller rim, and thinner RNFL when measured by HRT [49]. Supportingly in our study, we observed a negative correlation of the age with RV (only in controls) and RNFL in all of the groups (p < 0.05).
In conclusion, we examined optic disc parameters of the subjects with AD measured with the HRT III and compared the findings with glaucoma and control eyes. We found that subjects with AD presented with no difference for RNFL thickness compared to glaucoma and age-matched control cases. Age was the most important parameter affecting RNFL. Although research in the retina and optic nerve offers many advantages over the brain in terms of cost, time, and analytical methods, our results suggest that HRT does not demonstrate ONH differences between age-related neurodegenerative diseases like AD and control groups, while it is successful in the differentiation of glaucoma from AD and control cases of older age.
References
Guo L, Duggan J, Cordeiro MF (2010) Alzheimer’s disease and retinal neurodegeneration. Curr Alzheimer Res 7(1):3–14
Holroyd S, Shepherd ML (2001) Alzheimer’s disease: a review for the ophthalmologist. Surv Ophthalmol 45:516–524
Pache M, Flammer J (2006) A sick eye in a sick body? Systemic findings in patients with primary open-angle glaucoma. Surv Ophthalmol 51:179–212
Gupta N, Yucel YH (2007) What changes can we expect in the brain of glaucoma patients? Surv Ophthalmol 52:122–126
Wostyn P, Audenaert K, De Deyn PP (2008) Alzheimer’s disease-related changes in diseases characterized by elevation of intracranial or intraocular pressure. Clin Neurol Neurosurg 110(2):101–109
Quigley HA (1999) Neuronal death in glaucoma. Prog Retin Eye Res 18:39–57
Tezel G (2006) Oxidative stress in glaucomatous neurodegeneration: mechanisms and consequences. Prog Retin Eye Res 25:490–513
Kirby E, Bandelow S, Hogervorst E (2010) Visual impairment in Alzheimer’s disease: a critical review. J Alzheimers Dis 21(1):15–34
McKinnon SJ (2012) The cell and molecular biology of glaucoma: common neurodegenerative pathways and relevance to glaucoma. Invest Ophthalmol Vis Sci 53(5):2485–2487
Parisi V (2003) Correlation between morphological and functional retinal impairment in patients affected by ocular hypertension, glaucoma, demyelinating optic neuritis and Alzheimer’s disease. Semin Ophthalmol 18:50–57
Kallenbach K, Frederiksen J (2007) Optical coherence tomography in optic neuritis and multiple sclerosis: a review. Eur J Neurol 14(8):841–849
Kirbas S, Turkyilmaz K, Anlar O, Tufekci A, Durmus M (2013) Retinal nerve fiber layer thickness in Parkinson disease. J Neuroophthalmol 33(1):62–65
Jindahra P, Hedges TR, Mendoza-Santiesteban CE, Plant GT (2010) Optical coherence tomography of the retina: applications in neurology. Curr Opin Neurol 23(1):16–23
Ikram MK, Cheung CY, Wong TY, Chen CP (2012) Retinal pathology as biomarker for cognitive impairment and Alzheimer’s disease. J Neurol Neurosurg Psychiatry 83(9):917–922
Frost S, Martins RN, Kanagasingam Y (2010) Ocular biomarkers for early detection of Alzheimer’s disease. J Alzheimers Dis 22(1):1–16
Badalà F, Nouri-Mahdavi K, Raoof DA, Leeprechanon N, Law SK, Caprioli J (2007) Optic disk and nerve fiber layer imaging to detect glaucoma. Am J Ophthalmol 144(5):724–732
Klamann MK, Grünert A, Maier AK, Gonnermann J, Joussen AM, Huber KK (2013) Comparison of functional and morphological diagnostics in glaucoma patients and healthy subjects. Ophthalmic Res 49(4):192–198
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Hodapp E, Parrish RK II, Anderson DR (1993) Clinical decisions in glaucoma. The C.V. Mosby Co., St. Louis
Pei JJ, Sjogren M, Winblad B (2008) Neurofibrillary degeneration in Alzheimer’s disease: from molecular mechanisms to identification of drug targets. Curr Opin Psychiatry 21:555–561
Blanks JC, Hinton DR, Sadun AA, Miller CA (1989) Retinal ganglion cell degeneration in Alzheimer’s disease. Brain Res 501:364–372
Sadun A, Bassi C (1990) Optic nerve damage in Alzheimer’s disease. Ophthalmology 97:9–17
Hinton DR, Sadun AA, Blanks JC, Miller CA (1986) Optic-nerve degeneration in Alzheimer’s disease. N Engl J Med 315:485–487
Syed AB, Armstrong RA, Smith CU (2005) A quantitative analysis of optic nerve axons in elderly control subjects and patients with Alzheimer’s disease. Folia Neuropathol 43(1):1–6
Cuzzo LM, Ross-Cisneros FN, Yee KM, Wang MY, Sadun AA (2011) Low density lipoprotein receptor-related protein (LRP) is decreased in optic neuropathy of Alzheimer’s disease. J Neuroophthalmol 31(2):139–146
Davies DC, McCoubrie P, McDonald B, Jobst KA (1995) Myelinated axon number in the optic nerve is unaffected by Alzheimer’s disease. Br J Ophthalmol 79:596–600
Risacher SL, Wudunn D, Pepin SM, MaGee TR, McDonald BC, Flashman LA, Wishart HA, Pixley HS, Rabin LA, Paré N, Englert JJ, Schwartz E, Curtain JR, West JD, O’Neill DP, Santulli RB, Newman RW, Saykin AJ (2013) Visual contrast sensitivity in Alzheimer’s disease, mild cognitive impairment, and older adults with cognitive complaints. Neurobiol Aging 34(4):1133–1144
Pache M, Smeets CH, Gasio PF, Savaskan E, Flammer J, Wirz-Justice A, Kaiser HJ (2003) Colour vision deficiencies in Alzheimer’s disease. Age Ageing 32:422–426
Krasodomska K, Lubiński W, Potemkowski A, Jobst KA (2010) Pattern electroretinogram (PERG) and pattern visual evoked potential (PVEP) in the early stages of Alzheimer’s disease. Doc Ophthalmol 121(2):111–121
Wostyn P, Audenaert K, De Deyn PP (2009) Alzheimer’s disease and glaucoma is there a causal relationship? Br J Ophthalmol 93(12):1557–1559
Trick GL, Calotti FY, Skarf B (2006) Advances in imaging of the optic disc and retinal nerve fiber layer. J Neuroophthalmol 26(4):284–295
Hoffmann EM, Miglior S, Zeyen T, Torri V, Rulli E, Aliyeva S, Floriani I, Cunha-Vaz J, Pfeiffer N (2013) The Heidelberg retina tomograph ancillary study to the European Glaucoma Prevention Study: study design and baseline factors. Acta Ophthalmol 91(8):e612–e619
Kamal DS, Viswanathan AC, Garway-Heath DF et al (1999) Detection of optic disc change with the Heidelberg retina tomograph before confirmed visual field change in ocular hypertensives converting to early glaucoma. Br J Ophthalmol 83:290–294
Toledo J, Sepulcre J, Salinas-Alaman A, García-Layana A, Murie-Fernandez M, Bejarano B, Villoslada P (2008) Retinal nerve fiber layer atrophy is associated with physical and cognitive disability in multiple sclerosis. Mult Scler 14(7):906–912
Trip SA, Schlottmann PG, Jones SJ, Garway-Heath DF, Thompson AJ, Plant GT, Miller DH (2006) Quantification of optic nerve head topography in optic neuritis: a pilot study. Br J Ophthalmol 90(9):1128–1131
Danesh-Meyer HV, Birch H, Ku JY, Carroll S, Gamble G (2006) Reduction of optic nerve fibers in patients with Alzheimer disease identified by laser imaging. Neurology 67(10):1852–1854
Kergoat H, Kergoat MJ, Justino L, Chertkow H, Robillard A, Bergman H (2001) An evaluation of the retinal nerve fiber layer thickness by scanning laser polarimetry in individuals with dementia of the Alzheimer type. Acta Ophthalmol Scand 79(2):187–191
Berisha F, Feke GT, Trempe CL, McMeel JW, Schepens CL (2006) Localized retinal nerve fiber layer thinning in patients with early glaucoma or Alzheimer’s disease. Investig Ophthalmol Vis Sci 47:18–24
Parisi V (2001) Morphological and functional retinal impairment in Alzheimer’s disease patients. Clin Neurophysiol 112:1860–1867
Iseri PK, Altinas O, Tokay T, Yuksel N (2006) Relationship between cognitive impairment and retinal morphological and visual functional abnormalities in Alzheimer’s disease. J Neuro-ophthalmol 26:18–24
He XF, Liu YT, Peng C, Zhang F, Zhuang S, Zhang JS (2012) Optical coherence tomography assessed retinal nerve fiber layer thickness in patients with Alzheimer’s disease: a meta-analysis. Int J Ophthalmol 5(3):401–405
Kirbas S, Turkyilmaz K, Anlar O et al (2013) Retinal nerve fiber layer thickness in patients with Alzheimer disease. Neuroophthalmology 33(1):58–61
Kergoat H, Kergoat MJ, Justino L, Robillard A, Bergman H, Chertkow H (2001) Normal optic nerve head topography in the early stages of dementia of the Alzheimer type. Dement Geriatr Cogn Disord 12(6):359–363
Zangwill LM, Bowd C (2006) Retinal nerve fiber layer analysis in the diagnosis of glaucoma. Curr Opin Ophthalmol 17:120–131
Kesler A, Vakhapova V, Korczyn AD, Naftaliev E, Neudorfer M (2011) Retinal thickness in patients with mild cognitive impairment and Alzheimer’s disease. Clin Neurol Neurosurg 113(7):523–526
Paquet C, Boissonnot M, Roger F, Dighiero P, Gil R, Hugon J (2007) Abnormal retinal thickness in patients with mild cognitive impairment and Alzheimer’s disease. Neurosci Lett 420(2):97–99
Coops A, Henson DB, Kwartz AJ, Artes PH (2006) Automated analysis of heidelberg retina tomograph optic disc images by glaucoma probability score. Invest Ophthalmol Vis Sci 47:5348–5355
Alasil T, Wang K, Keane PA, Lee H, Baniasadi N, de Boer JF, Chen TC (2013) Analysis of normal retinal nerve fiber layer thickness by age, sex, and race using spectral domain optical coherence tomography. J Glaucoma 22(7):532–541
Khawaja AP, Chan MP, Broadway DC, Garway-Heath DF, Luben R, Yip JL, Hayat S, Khaw KT, Foster PJ (2013) Laser scanning tomography in the EPIC-Norfolk eye study: principal components and associations. Invest Ophthalmol Vis Sci 54(10):6638–6645
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kurna, S.A., Akar, G., Altun, A. et al. Confocal scanning laser tomography of the optic nerve head on the patients with Alzheimer’s disease compared to glaucoma and control. Int Ophthalmol 34, 1203–1211 (2014). https://doi.org/10.1007/s10792-014-0004-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-014-0004-z