
Abstract
Boosting myocardial resistance to acute as well as chronic ischemic damage would ameliorate the detrimental effects of numerous cardiac pathologies and reduce the probability of transition to heart failure. Experimental cardiology has pointed to ischemic and pharmacological pre- as well as post-conditioning as potent acute cardioprotective manipulations. Additional exciting experimental strategies include the induction of true regenerative and/or angiogenic responses to the damaged heart, resulting in sustained structural and functional beneficial effects. Fibroblast growth factor-2 (FGF-2), an endogenous multifunctional protein with strong affinity for the extracellular matrix and basal lamina and well-documented paracrine, autocrine and intacellular modes of action, has been shown over the years to exert acute and direct pro-survival effects, irrespectively of whether it is administered before, during or after an ischemic insult to the heart. FGF-2 is also a potent angiogenic protein and a crucial agent for the proliferation, expansion, and survival of several cell types including those with stem cell properties. Human clinical trials have pointed to a good safety record for this protein. In this review, we will present a case for the low molecular weight isoform of fibroblast growth factor-2 (lo-FGF-2) as a very promising therapeutic agent to achieve powerful acute as well as sustained benefits for the heart, due to its cytoprotective and regenerative properties.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
General Introduction
Fibroblast growth factor-2 (FGF-2), previously termed basic FGF, is a prototypic and extensively studied member of a large family (FGF-1 to FGF-23) of highly conserved, structurally related heparin binding growth factors [1]. FGFs show developmental, tissue, and cell-specific regulation, and there seems to exist a need for certain members of this family during distinct early developmental stages [1, 2]. FGFs act by binding to plasma membrane tyrosine kinase receptors (FGFR1–4), albeit with different affinities, thus substantial redundancy between the various FGF ligands is to be expected. This redundancy can account for the fact that transgenic mouse models lacking FGF-1 and/or FGF-2 are viable, presenting nevertheless specific abnormalities and defects [3]. Preferential interactions between specific FGF ligands and specific FGFRs have also been noted, and are believed to contribute to cell, stage and tissue specificity as well as fine tuning of the action of FGFs [1, 2].
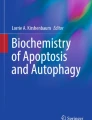
FGF-2 is ubiquitously expressed, and exists as 18 kDa low molecular weight (lo-FGF-2) and 20–34 kDa, high molecular weight (hi-FGF-2) isoforms. The vast majority of studies to-date, especially in the heart, and all of the FGF-2 clinical trials, have tested the effects of lo-FGF-2, acting ‘from the outside in’. Relatively little information exists about the activities of hi-FGF-2 isoforms, especially in the context of paracrine or autocrine signaling. Nevertheless, hi-FGF-2 isoforms have been found to possess certain distinct activities, as we reviewed recently [4]. Briefly, only hi-FGF-2 can stimulate cardiac and cardiomyocyte hypertrophy when acting on plasma membrane receptors; and only hi-FGF-2 can cause apoptotic cell death when acting in an intracrine fashion. Properties of hi- and lo-FGF-2, and also of specific mutant versions of lo-FGF-2, are summarized in Table 1. Figure 1 provides an overview of how subcellular location of hi- and lo-FGF-2 interrelates with their biological effects.

The various sites of endogenous FGF-2 location and action in the myocardium. Cardiac myocytes express both hi- and lo-FGF-2, localizing to nuclear, cytosolic and extracellular sites. Cardiac fibroblasts accumulate and release predominantly the hi-FGF-2 isoforms [46]. Released FGF-2 is bound by HSPGs at the plasma membrane, basal lamina and extracellular matrix; matrix and basal lamina-bound FGF-2 can be ‘liberated’ by heparinases and can then act on cell surface FGFR. Extracellular, HSPG-bound hi-FGF-2 can be converted to lo-FGF-2 through limited proteolysis by proteases that are also associated with HSPGs [41]. Released FGF-2 can find its way into the circulation. Extracellular FGF-2 (either type of isoform) affects cells by binding to plasma membrane FGFR and thus activating a multitude of downstream cascades inducing phosphorylation of many targets; at the same time it also becomes internalized, translocates into the nucleus and influences gene expression. The pattern of FGF-2-induced gene expression is isoform-specific [47]. Endogenous FGF-2 may also find its way into the nucleus without exiting the cell, and thus exert isoform-specific intracrine effects: intracrine action of hi-FGF-2 in myocytes includes induction of apoptosis [48]
The low molecular weight (Lo) isoform
Function
Lo-FGF-2 is a potent mitogen for cells of mesodermal and neuroectodermal origin and a powerful angiogenic agent. It can also promote survival and prevent apoptosis in many cell types in addition to regulating differentiation and gene expression [1]. In the myocardium, FGF-2 is upregulated in response to injury and/or chronic stress at both the transcriptional and translational level [10], and this factor is implicated in most aspects and cell types associated with the injury-repair-regeneration response [11]. Cardiomyocytes express functional FGF-2 receptors at all developmental stages including the adult [12]; they respond to FGF-2 addition by activating numerous down-stream signals, leading to a number of end-points such as cytoprotection, activation of DNA synthesis, and also a negative inotropic effect [5, 13]. Lo-FGF-2 is a potent mitogen and survival agent for responsive, committed cells of various lineages, as well as bone marrow-derived, and tissue-derived (resident) human and rodent cells with stem-cell properties [14–20]. Lo-FGF-2 has been traditionally considered as an inducer of pathological myocardial hypertrophy [4]; our recent research however demonstrated that this is not true, and that only the hi-FGF-2 isoform is pro-hypertrophic [21]. Some of the effects of administered FGF-2 are summarized in Table 1.
Distribution, expression, release
Lo-FGF is present in most cells and tissues and is relatively elevated in highly vascularized organs such as the adult heart or slow skeletal muscles [22–24]. It is generally believed that lo-FGF-2 is localized in the extracellular space and the cytosol, translocating to the nucleus only during the G1-S transition of the cell cycle [25–27]. Nevertheless ectopic expression studies using tagged or untagged, human, rodent or avian lo-FGF-2 in a variety of cell types from a variety of species have consistently detected lo-FGF-2 in cell nuclei, in a manner not necessarily relating to cell cycle stimulation [22, 28–31].
FGF-2 gene expression is upregulated by many stress stimuli, including hypoxia and ischemia [32], and also in response to angiotensin-II [33] and adrenergic stimulation [34]. In addition, there is some evidence to suggest that FGF-2 stimulates its own gene expression in a positive feed-back loop [35, 36]. Further to transcriptional regulation, FGF-2 accumulation is regulated at the translational level: cells need to be directed to employ either a cap-dependent mechanism of translation, or the less conventional internal ribosome entry site (IRES) mode; and they also need to decide whether to initiate translation from AUG or CUG start sites [27]. These decisions will determine which FGF-2 isoforms will accumulate within the cell. It is theorized that factors/complexes binding to the 5′ untranslated, as well as the usually extremely long 3′ untranslated regions of the FGF-2 mRNA are ultimately responsible for determining relative levels of translation of the various FGF-2 isoforms. In human cells, standard cap-dependent translation produces the 34 kDa (hi; CUG initiated) FGF-2, while IRES-dependent translation produces lo-FGF-2 (AUG-initiated) as well as 21–25 kDa (hi; CUG initiated) isoforms [37–39]. A potential third level of regulation, converting hi-FGF-2 to lo-FGF-2, by limited degradation of the N-terminal extension, has also been considered but has not been addressed in any detail to-date [40, 41].
The FGF-2 protein lacks a classic export signal sequence but is nevertheless released from viable cells in an ongoing manner; it is also released by dying cells during tissue injury. Thus, FGF-2 is found in association with heparin sulphate proteoglycans (HSPGs) at the basal lamina and the extracellular matrix; it can also be detected in the serum and other body fluids [42]. In fact a number of acute or chronic pathologies are associated with increased FGF-2 levels in the blood or urine [43–45]. It is important to note, however, that because these studies rely almost exclusively on ELISA-based FGF-2 detection with antibodies that are not isoform-specific, it is not known if they actually report on lo-FGF-2, hi-FGF-2, or both types of isoforms [4]. Figure 1 illustrates the various cellular, extracellular and subcellular sites of localization and action of FGF-2.

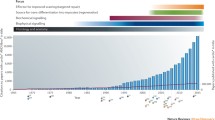
Localization of presumptive mesenchymal stem cells and stem-cell factor (SCF) in FGF-2-treated myocardial infarcts. Myocardial infarction was induced by permanent coronary occlusion in a rat model; lo-FGF-2 was injected directly into the ischemic left ventricle within 15 min from occlusion, exactly as we described previously [7, 8]. Animals were euthanized at 3 days post MI, and hearts were processed for cryosectioning and immunofluorescence. Sections were stained for c-kit (green; fluorescein-labeled anti c-kit antibodies), SCF (red; Texas-red-labeled anti-SCF primary antibodies) and nuclei (blue; Hoechst stain). Staining with the secondary fluorescent antibodies, without pre-incubation with primary antibodies, displayed only very low background staining, indicating that the patterns observed with the primary antibodies were specific. Clusters of round c-kit-positive cells can be observed within the infarct, in association with pools of SCF at the pericellular space
The mechanism of FGF-2 release from viable cells is not well understood. It is ATP-dependent and does not involve the endoplasmic reticulum/Golgi transportation pathway; pharmacological inhibitors of the Na+/K+ ATPase pump can prevent FGF-2 export from a number of cell lines, implicating the Na+/K+ ATPase in this process [49, 50]. FGF-2 can also be released through plasma membrane vesicle shedding [51], and non-lethal transient membrane disruptions [52]. Contractile cells such as cardiomyocytes release FGF-2 on a beat-to-beat basis, under normal conditions. Cardiac fibroblasts, a rich source of released FGF-2 and a major cardiac population existing in close association with myocytes, would be stretched passively by myocyte contraction, and thus also release FGF-2 to the extracellular matrix. This is quite significant since (myo)fibroblasts accumulate and release predominantly the pro-hypertrophic hi-FGF-2 isoforms [46]. Increased contractility, and increased endogenous FGF-2 expression result in increased levels of heart-released FGF-2 [53, 54], increasing the opportunity for exerting effects in an autocrine–paracrine manner. As summarized in Fig. 1, extracellular FGF-2 becomes free to interact with cell surface receptors subsequent to the action of heparinase(s) and/or plasminogen activator-mediated proteolysis, events that are upregulated during injury, repair, and pathological situations associated with cell invasion [55, 56].
Signal transduction
The biological effects of extracellular FGF-2 are mediated by binding to high-affinity FGF receptors (FGFR1-4) of the tyrosine kinase family [57]. FGFR1 is the best-studied FGFR in embryonic, neonatal, and adult cardiomyocytes [12, 58]. Heparan sulphate proteoglycans (HSPGs), which function partly to sequester FGF-2 in the extracellular matrix until signaling is triggered, are also present at the plasma membrane and act as lower affinity ‘receptors’ to facilitate interaction of the ligand with FGFR [57, 59]; see also Fig. 1. Plasma membrane HSPGs may in fact carry their own signaling capacity in response to FGF-2 binding [60]. Activated FGFRs recruit and phosphorylate other signaling molecules culminating in the activation of major signal transduction pathways such as all three branches of the mitogen activated protein kinase (MAPK pathway), the phospholipase C-protein kinase C (PKC)- and Src-associated pathways [10].
An additional, concurrent pathway for extracellular FGF-2-triggered signalling is initiated by binding and activating FGFR1 at the plasma membrane, followed by FGF-2-FGFR1 internalization and nuclear translocation. Activated nuclear FGFR1 may then activate a number of genes directly [61, 62]. Thus the end-effects of extracellular FGF-2 are brought about by signals activated downstream of the plasma membrane FGFR as well as by those triggered by internalized FGF-2 and FGF-2/FGFR complexes that translocate to the nucleus and affect gene expression directly [4].
Internalization followed by nuclear translocation is reported to be essential for the mitogenic response to lo-FGF-2. It occurs during the G1 stage of the cell cycle and is mediated by lo-FGF-2 binding to translokin, an ubiquitous cytosolic protein [25]. Activation of casein kinase 2 (CK2) through the interaction of its beta-subunit with lo-FGF-2 in the nucleus is also essential for the induction of the mitogenic response [25, 63, 64].
Pre-conditioning-like cardioprotection
Exposure to short periods of ischemia protects the heart from a subsequent severe insult, a phenomenon termed ischemic preconditioning [65]. Protection manifests as preservation of tissue viability and overall function, and can be observed in two stages: an early phase developing within minutes of the brief ischemic episode(s) and lasting several hours, and a late phase, the “second window”, emerging 12–24 h later and lasting several days [66]. Early preconditioning does not require novel gene expression but is dependent on the activation of particular signal transduction cascades, eliciting post-translational modifications (phosphorylation) and changing the behavior of a multitude of target proteins [66]. These cascades eventually promote changes in gene expression resulting in upregulation and/or downregulation of molecules mediating the second window of protection. Considerable research effort has been applied to the identification of triggers and mediators of cardioprotection with the intent to realize therapeutic potential through activation of the pre-conditioning response (pharmacological pre-conditioning) [67–70].
Several models have been used by us and other laboratories to examine the ability of exogenously administered lo-FGF-2 to confer protection from cardiac injury (reviewed in more detail in [10, 11]). Addition of FGF-2 protected neonatal cultured cardiomyocytes from H2O2-induced cell injury and death [71]. In the isolated adult rat or mouse heart model, lo-FGF-2 given by retrograde perfusion, entered the myocardium and distributed in a basement-membrane fashion, increasing the overall heart-associated FGF-2 levels nearly 4-fold [6]; it also protected the heart from subsequent ischemia-reperfusion induced contractile dysfunction and myocardial tissue loss, and preserved cardiac energy metabolites [6]. Perfusion-administered lo-FGF-2 prevented the ischemia-induced dephosphorylation of the gap junction protein connexin-43 suggesting an ability to preserve pre-ischemic patterns of intercellular communication and rhythm [72], in agreement with reports addressing this issue directly [73]. We have also shown that chronic overexpression of lo-FGF-2 in transgenic mouse myocardium resulted in increased resistance to myocardial ischemic injury, and increased levels of peri-cellular FGF-2 [53]. Our data have since been confirmed by other investigators [74].
In terms of mechanism we found that acute cardioprotection by extracellular lo-FGF-2 required interaction with and activation of FGFR1, and activation of the PLC-PKC signal cascade [5, 7]. PKC activation, in particular the ε isoform, is a central mediator of the injury-resistant phenotype, modifying targets at the plasma membrane, mitochondria, and other subcellular sites [75–80]. Chronic overexpression of lo-FGF-2 in transgenic mouse hearts also resulted in increased levels of membrane associated α-PKC and total ε-PKC [53]; upregulation of these signals would be expected to elicit protection.
Activation of extracellular signal regulated kinase (ERK) has been reported to mediate a pro-survival phenotype [81] and thus could be expected to contribute to lo-FGF-2-induced protection. In agreement, cardioprotection induced by overexpressed FGF-2 in a transgenic mouse model was reported to be dependent on the ERK activating pathway [82]. We have found that, by inhibiting PKC, it was possible to completely block FGF-2-induced cardioprotection without affecting activation of ERK. Our data suggested that ERK activation may occur upstream of the PKC pathway and/or that ERK activation is not sufficient, in and of itself, to substitute for lo-FGF-2-induced resistance to injury. In addition to activation [5] lo-FGF-2 increased the interaction of ε-PKC with the gap junction protein connexin-43 (Cx43) at the intercalated discs [83], and caused hyper-phosphorylation of Cx43 at PKC target amino-acid sites including serine 262 in vitro [84] and in the adult perfused heart [85]. In view of recent reports that Cx43 is required for the development of a pre-conditioning response our data imply that the lo-FGF-2-induced Cx43 phosphorylation is an important component of an injury-resistant phenotype. Additional signals that upregulate and are upregulated by lo-FGF-2 and that are involved in pre-conditioning type cardioprotection include nitric oxide and the nitric oxide synthases as reviewed in more detail previously [4, 10].
The potent protective actions of administered or overexpressed lo-FGF-2 have indicated that its endogenous counterpart may play a similar role. FGF-2, released on a beat-to-beat basis is likely contributing to the maintenance of a healthy myocardium, and would be expected to confer increased capacity to resist injury and function under stress. A component of its protective action likely includes effects on contractility and thus energy consumption and requirement: positive inotropism induced by a variety of agents, catecholamine stimulation for example, results in increased release of FGF-2 [34] which, by exerting a negative inotropic effect [5, 13], would be expected to normalize force of contraction, and thus bring FGF-2 release back to baseline levels. Studies using FGF-2-deficient mice, lacking both hi- and lo-FGF-2 isoforms, have offered strong support to the notion that endogenous FGF-2 is mediating resistance to injury: House and colleagues showed that, compared to wild type, FGF-2-deficient hearts are more vulnerable to ischemic injury, while overexpression of human FGF-2 in the FGF-2-defficient mouse conferred significant protection [74].
Secondary injury prevention
Pre-conditioning-type protection, be it ischemic or pharmacological, is impractical as a general approach since it requires to predict when the need for protection will arise [86]. This issue is no longer a concern in situations where ischemic injury is developing or on-going, and also in the context of ischemia-reperfusion induced pathologies [87]. Acute myocardial infarction (MI), resulting from an interruption of blood flow to the heart, is a major cause of mortality and morbidity worldwide; its management requires re-establishment of blood flow by surgical and/or pharmacologically means [88]. Reperfusion of the ischemic myocardium carries added risks since it is associated with exacerbation of cell injury and death in the acute stage [87]. Interventions and factors that can reduce damage during development of MI and during reperfusion have thus attracted much attention over several years [67, 89–91].
Using a rat model we demonstrated that lo-FGF-2, administered by intra-cardiac injection to the ischemic left ventricle during the development of MI caused by permanent coronary ligation remained near the injection sites for several hours in association with both viable and necrotic tissue, and exerted significant protection from acute (4–24 h from occlusion) muscle loss and contractile dysfunction [7]. Using a variety of animal models other laboratories have reported similar findings, as reviewed in detail previously [92]. It is evident that acute FGF-2 protection reflects a direct effect on myocardial tissue and is not dependent on angiogenesis [93, 94]. In fact, a mutant, non-angiogenic and non-mitogenic lo-FGF-2 (S117A-FGF-2) remained capable of eliciting acute cardioprotection [8]; see also Table 1.
It is noteworthy that exogenous lo-FGF-2, whether injected directly into the tissue, or administered by perfusion, shows similar distribution to the basal lamina and extracellular matrix as the endogenously expressed molecule [6, 7, 53, 95]. This is likely due to its very high affinity for HSPGs present at the cell surface, basal lamina and matrix; illustrated in Fig. 1. Locations enriched in HSPGs would thus be expected to absorb FGF-2 from both intracellular and extracellular origins. Muscle-linked repair-regeneration studies conducted over many years have shown that basement membranes may remain relatively intact after cellular demise, thus serving as a scaffold and a blueprint informing tissue rebuilding [96–98]. Basal laminae can provide local ‘cues’ and spatial guidance for cells homing in from the circulation and/or neighboring tissue. Strong retention of the FGF-2 protein by basement membranes and extracellular matrix would be expected to serve as a natural reservoir for prolonged stimulation of reparative processes [96]. Binding to HSPGs not only sequesters FGF-2 to sites of actual and ‘pending’ action, it can also protect it from degradation. This is not quite the case for hi-FGF-2: binding to heparin protects its core 18 kDa sequence from degradation by proteases that are also heparin-bound, while allowing limited proteolysis of its N-terminal extension. This process effectively converts hi-FGF-2 to lo-FGF-2, can be regulated by second messengers such as calcium [99], and may reduce hi-FGF-2 detectable at the extracellular matrix.
To examine the potential of FGF-2 for specifically protecting during the reperfusion phase, we subjected ex vivo perfused hearts to 30 min of global ischemia, followed by 10 min of reperfusion in the presence or absence of lo-FGF-2 and 50–110 min of reperfusion with standard perfusion medium. Administration of lo-FGF-2 during reperfusion resulted in significantly improved contractile recovery and reduced apoptotic cell death [7, 8]. It also resulted in re-establishment of pre-ischemic levels of phosphorylated Cx43, even though this protein becomes dephosphorylated after 30 min of global ischemia [100, 101]; without added FGF-2, reperfusion achieved low level of recovery in phosphorylated Cx43 [72]. FGF-2 given during reperfusion re-established localization of Cx43 mostly to intercalated disks [72], supporting the notion that it can prevent reperfusion-linked conduction abnormalities and arrhythmias. Exogenously administered hi-FGF-2, or non-mitogenic lo-FGF-2, were equally effective as lo-FGF-2 as survival and protection agents during reperfusion, again demonstrating a dissociation between the mitotic and cytoprotective pathways induced by FGF-2 [8].
Lo-FGF-2 administered during reperfusion stimulated a number of intracellular signals (PKC; ERK; Akt) which are expected to mediate its beneficial effects ([74, 94] and unpublished observations). Apoptotic cell death is a feature of reperfusion-induced injury since stimulation of signaling pathways capable of preventing apoptosis elicits cardioprotection during reperfusion [90, 102]. Such protective signaling pathways include PKC-dependent cascades [7, 103]; and the ERK as well as the phosphatidylinositol-3-OH kinase (PI3K)—Akt axis [89].
We propose that the ability of FGF-2 to exert cytoprotection when administered during reperfusion, in combination with its particular ‘spatial-retention’ properties (Table 1, Fig. 1), represents a very attractive features for any reperfusion regime in the clinic. A relatively low dose of the FGF-2 protein (we would hypothesize this to be at about 10–100 μg/human heart), could be introduced once during, for example, balloon angioplasty, and would be expected to prevent ischemic and reperfusion-induced myocardial damage. Selecting the non-mitogenic (S117A) FGF-2 mutant (see Table 1) would be equally effective as a cytoprotective agent with the added bonus of being devoid of any possible side effects linked to mitogenic stimulation, such a stimulating vascular proliferative events (restenosis), or when treating cancer patients. FGF-2, a ubiquitous protein acknowledged by our immune system as ‘one of our own’, would not be expected to elicit adverse immune responses, especially when used as a brief treatment. Finally, the non-mitogenic lo-FGF-2 mutant could also be considered for systemic and/or prolonged usage, when a generalized cytoprotection is required, for example as a supplement to cardioplegic solutions in surgery and organ transplantation; in muscle degenerative diseases; and in various types of heart failure.
Long-term benefits
In addition to its ability to elicit acute, direct cardioprotection, lo-FGF-2 is also capable of exerting sustained benefits to the heart. Once-only intramyocardial delivery of the lo-FGF-2 protein into the ischemic, akinetic left ventricle during the development of MI exerted substantial beneficial effects detectable 8–16 weeks post-MI: these included smaller scars and improved contractile function compared to a vehicle-treated, infarcted group ([21, 74] and unpublished data); see also Table 1. These long-term effects were dependent on the ability of lo-FGF-2 to increase infarct and peri-infarct vascularity by promoting angiogenesis [8, 21], an activity requiring that FGF-2 possesses both mitotic and chemo-attractant properties. Thus the non-mitotic and non-angiogenic S117A-lo-FGF-2 mutant, used in an identical fashion, was incapable of conferring sustained benefits beyond 1 week post-administration [8], while the hi-FGF-2 isoform, which cannot stimulate cell migration but is still capable of stimulating mitosis did not promote neovascularization and its beneficial effects were not sustainable in the long-term [21]. The magnitude of sustained beneficial effects exerted by a once-only administration of the lo-FGF-2 protein (at 2 μg/rat heart; in 50 μl of saline) is broadly similar to that reported in several experimental models dependent on: stem-cell transplantation and/or recruitment [104] and/or the strong paracrine component of stem-cell based therapy [105, 106]. Thus it is worth examining the notion that lo-FGF-2 can induce a truly regenerative response (see section below). If proven to be true, administration of the lo-FGF-2 protein could represent an effective, quick as well as inexpensive strategy to promote better heart repair. This approach would not require any cell isolations, purification, expansion or transfection, gene therapy, transplantation, or immunosuppression, although it could complement all of these procedures. We propose that the delivery of a few microgram of lo-FGF-2 protein into the infarcted myocardium would simply boost and guide what is already there.
Potential to induce regeneration
Lo-FGF-2 possesses properties considered desirable in the context of stimulating and sustaining the repair/regeneration process [15, 18, 20, 107–111]. Thus it can promote cell migration, homing, proliferation, and survival; it also allows differentiation into cardiogenic and other lineages; prevents senescence; its strong binding to HSPGs retains it within the area of administration (or injury, for the endogenous molecule) and protects it from degradation, while allowing slow diffusion to adjacent areas; it stimulates its own expression, effectively prolonging its influence. Importantly the safety of lo-FGF-2 for clinical use has been studied in several clinical trials (reviewed by us previously [10, 11, 92]) that pointed to lack of side effects such as hypotension, hypertrophy, tumorigenesis when this protein was administered by intracoronary bolus injection and used within an effective concentration range. We would like to also bring particular attention to reports showing that lo-FGF-2 can upregulate expression of stem cell factor (SCF), the ligand for the c-kit plasma membrane receptor in mesenchymal stem cells and a potent homing signal for these cells to areas of injury [16, 112, 113].
While the angiogenic properties of lo-FGF-2 have been documented extensively, and there is little doubt that its long-term beneficial effects include an angiogenic response (please see detailed review in [10, 11, 92]) it is somewhat surprising how relatively little attention has been paid to lo-FGF-2 by the scientific and clinical communities in regards to its potential to act as a safe, relatively easy to administer, and relatively inexpensive agent of a true regenerative response. We have already shown that a once only administration of lo-FGF-2 to a developing infarct elicited sustained benefits including smaller scars and improved function [7, 8, 21]. Using the same rat model and experimental design, our recent pilot studies (n = 4/group), indicated that infarcts injected with lo-FGF-2 also contained a statistically significant, 3-fold increase in the fraction of presumptive stem cells (positive for the c-kit antigen), as well as cells undergoing cell division (cells positive for phosphorylated histone H3), compared to saline-injected infarcts, at 3 days post-MI (unpublished observations). We also detected ample presence of the ‘homing signal’, SCF, in the lo-FGF-2-injected infarcts (Fig. 2). Thus we suggest that the pronounced and prolonged benefits elicited by lo-FGF-2 are very likely to include a regenerative component.
Concluding remarks
In the preceding sections, we have built a case for lo-FGF-2 as a very promising therapeutic agent for both acute (pre- and post-conditioning) as well as long-term interventions (tissue repair-regeneration). What makes lo-FGF-2 stand out, in our opinion, amongst several mitogenic and angiogenic factors and cytokines that have been reported as having a variety of beneficial effects, is: (A): its very strong affinity for heparin and HSPGs that allows it to be retained where it is needed, even if given during reperfusion and subjected to continuous ‘wash-out’ [6] and (B): its proven ability not to cause detrimental effects in the long run (see also Table 1). This point was brought home by our recent studies on the long-term effect of a once-only administration of hi-FGF-2: our initial studies had suggested that this isoform was as beneficial as lo-FGF-2, because it exerted acutely cytoprotective effects, reduced infarct size, and elicited overall functional improvement for up to 6 weeks post-MI. More long-term studies told another story: unlike lo-FGF-2, hi-FGF-2-treated groups developed significant cardiac and cardiomyocyte hypertrophy, and any functional improvement was lost after the 6th week post-MI. The effects of hi-FGF-2 (but not lo-FGF-2) were accompanied by significant upregulation of cardiotrophin-1, a cytokine that, while cytoprotective as an acute agent, is also linked to the development of pathological hypertrophy and heart failure [114, 115]. Other members of the FGF family (FGF-1, FGF-5) have been investigated in the context of inducing beneficial effects to the heart [116–118], highlighting the potential for these factors to be used therapeutically.
In considering lo-FGF-2 for therapeutic usage, a number of specific issues should be resolved. Most importantly, the optimal strategy for administering this protein should be established in preclinical models for specific diseases. Dosage, timing, and the particular lo-FGF-2 mutant to be used in relation to a particular pathology should also be investigated. Study of potential side effects, acute as well as chronic and even when the protein is administered for only a brief period, should not be neglected: a good reminder for remaining vigilant is provided by the hi-FGF-2 example mentioned in the preceding paragraph. Finally, the potential of lo-FGF-2 and/or its mutant versions to be of benefit in early and even late stages of heart failure, caused by a variety of conditions, demands attention.
References
Ornitz DM (2000) FGFs, heparan sulfate and FGFRs. Bioassays 22:108–112
Itoh N, Ornitz DM (2004) Evolution of the FGF and FGFR gene families. Trends Genet 20:563–569
Detillieux KA, Jimenez SK, Sontag DP, Nickerson PW, Kardami E, Cattini PA (2004) The application of genetic mouse models to elucidate a role for FGF-2 in the mammalian cardiovascular system. Kluwer Academic Publishers, Boston, pp 373–391
Kardami E, Jiang ZS, Jimenez SK, Hirst CJ, Sheikh F, Zahradka P, Cattini PA (2004) Fibroblast growth factor 2 isoforms and cardiac hypertrophy. Cardiovasc Res 63:458–466
Padua RR, Merle PL, Doble BW, Yu CH, Zahradka P, Pierce GN, Panagia V, Kardami E (1998) FGF-2-induced negative inotropism and cardioprotection are inhibited by chelerythrine: involvement of sarcolemmal calcium-independent protein kinase C. J Mol Cell Cardiol 30:2695–2709
Padua RR, Sethi R, Dhalla NS, Kardami E (1995) Basic fibroblast growth factor is cardioprotective in ischemia-reperfusion injury. Mol Cell Biochem 143:129–135
Jiang ZS, Padua RR, Ju H, Doble BW, Jin Y, Hao J, Cattini PA, Dixon IM, Kardami E (2002) Acute protection of ischemic heart by FGF-2: involvement of FGF-2 receptors and protein kinase C. Am J Physiol Heart Circ Physiol 282:H1071–1080
Jiang ZS, Srisakuldee W, Soulet F, Bouche G, Kardami E (2004) Non-angiogenic FGF-2 protects the ischemic heart from injury, in the presence or absence of reperfusion. Cardiovasc Res 62:154–166
Tappia PS, Padua RR, Panagia V, Kardami E (1999) Fibroblast growth factor-2 stimulates phospholipase Cbeta in adult cardiomyocytes. Biochem Cell Biol 77:569–575
Detillieux KA, Sheikh F, Kardami E, Cattini PA (2003) Biological activities of fibroblast growth factor-2 in the adult myocardium. Cardiovasc Res 57:8–19
Detillieux KA, Cattini PA, Kardami E (2004) Beyond angiogenesis: the cardioprotective potential of fibroblast growth factor-2. Can J Physiol Pharmacol 82:1044–1052
Liu L, Pasumarthi KB, Padua RR, Massaeli H, Fandrich RR, Pierce GN, Cattini PA, Kardami E (1995) Adult cardiomyocytes express functional high-affinity receptors for basic fibroblast growth factor. Am J Physiol 268:H1927–1938
Ishibashi Y, Urabe Y, Tsutsui H, Kinugawa S, Sugimachi M, Takahashi M, Yamamoto S, Tagawa H, Sunagawa K, Takeshita A. (1997) Negative inotropic effect of basic fibroblast growth factor on adult rat cardiac myocyte. Circulation 96:2501–2504
Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K et al. (2003) Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell 114:763–776
van den Bos C, Mosca JD, Winkles J, Kerrigan L, Burgess WH, Marshak DR (1997) Human mesenchymal stem cells respond to fibroblast growth factors. Hum Cell 10:45–50
Sugimoto Y, Koji T, Miyoshi S (1999) Modification of expression of stem cell factor by various cytokines. J Cell Physiol 181:285–294
Burger PE, Coetzee S, McKeehan WL, Kan M, Cook P, Fan Y, Suda T, Hebbel RP, Novitzky N, Muller WA et al (2002) Fibroblast growth factor receptor-1 is expressed by endothelial progenitor cells. Blood 100:3527–3535
Levenstein ME, Ludwig TE, Xu RH, Llanas RA, VanDenHeuvel-Kramer K, Manning D, Thomson JA (2006) Basic fibroblast growth factor support of human embryonic stem cell self-renewal. Stem Cells 24:568–574
Xu C, Rosler E, Jiang J, Lebkowski JS, Gold JD, O’Sullivan C, Delavan-Boorsma K, Mok M, Bronstein A, Carpenter MK (2005) Basic fibroblast growth factor supports undifferentiated human embryonic stem cell growth without conditioned medium. Stem Cells 23:315–323
Kawai T, Takahashi T, Esaki M, Ushikoshi H, Nagano S, Fujiwara H, Kosai K (2004) Efficient cardiomyogenic differentiation of embryonic stem cell by fibroblast growth factor 2 and bone morphogenetic protein 2. Circ J 68:691–702
Jiang ZS, Jeyaraman M, Wen GB, Fandrich RR, Dixon IM, Cattini PA, Kardami E (2007) High- but not low-molecular weight FGF-2 causes cardiac hypertrophy in vivo; possible involvement of cardiotrophin-1. J Mol Cell Cardiol 42:222–233
Kardami E, Fandrich RR (1989) Basic fibroblast growth-factor in atria and ventricles of the vertebrate heart. J Cell Biol 109:1865–1875
Strohman RC, Kardami E (1986) Muscle regeneration revisited: growth factor regulation of myogenic cell replication. Prog Clin Biol Res 226:287–296
Kardami E, Spector D, Strohman RC (1985) Myogenic growth factor present in skeletal muscle is purified by heparin-affinity chromatography. Proc Natl Acad Sci USA 82:8044–8047
Bossard C, Laurell H, Van den Berghe L, Meunier S, Zanibellato C, Prats H. (2003) Translokin is an intracellular mediator of FGF-2 trafficking. Nat Cell Biol 5:433–439
Bikfalvi A, Savona C, Perollet C, Javerzat S (1998) New insights in the biology of fibroblast growth factor-2. Angiogenesis 1:155–173
Touriol C, Bornes S, Bonnal S, Audigier S, Prats H, Prats AC, Vagner S (2003) Generation of protein isoform diversity by alternative initiation of translation at non-AUG codons. Biol Cell 95:169–178
Powell PP, Klagsbrun M (1991) Three forms of rat basic fibroblast growth factor are made from a single mRNA and localize to the nucleus. J Cell Physiol 148:202–210
Riese J, Zeller R, Dono R (1995) Nucleo-cytoplasmic translocation and secretion of fibroblast growth factor-2 during avian gastrulation. Mech Dev 49:13–22
Kardami E, Murphy LJ, Liu L, Padua RR, Fandrich RR (1990) Characterization of two preparations of antibodies to basic fibroblast growth factor which exhibit distinct patterns of immunolocalization. Growth Factors 4:69–80
Claus P, Doring F, Gringel S, Muller-Ostermeyer F, Fuhlrott J, Kraft T, Grothe C (2003) Differential intranuclear localization of fibroblast growth factor-2 isoforms and specific interaction with the survival of motoneuron protein. J Biol Chem 278:479–485
Endoh M, Pulsinelli WA, Wagner JA (1994) Transient global ischemia induces dynamic changes in the expression of bFGF and the FGF receptor. Brain Res Mol Brain Res 22:76–88
Peifley KA, Winkles JA (1998) Angiotensin II and endothelin-1 increase fibroblast growth factor-2 mRNA expression in vascular smooth muscle cells. Biochem Biophys Res Commun 242:202–208
Detillieux KA, Meij JTA, Kardami E, Cattini PA (1999) alpha(l)-Adrenergic stimulation of FGF-2 promoter in cardiac myocytes and in adult transgenic mouse hearts. Am J Physiol Heart Circ Physiol 276:H826–H833
Jimenez SK, Sheikh F, Jin Y, Detillieux KA, Dhaliwal J, Kardami E, Cattini PA (2004) Transcriptional regulation of FGF-2 gene expression in cardiac myocytes. Cardiovasc Res 62:548–557
Jimenez SK, Kardami E, Cattini PA (2004) FGF-2 autoregulation in cardiac myocytes. J Mol Cellular Cardiol 36:625–625
Arnaud E, Touriol C, Boutonnet C, Gensac MC, Vagner S, Prats H, Prats AC (1999) A new 34-kilodalton isoform of human fibroblast growth factor 2 is cap dependently synthesized by using a non-AUG start codon and behaves as a survival factor. Mol Cell Biol 19:505–514
Bonnal S, Schaeffer C, Creancier L, Clamens S, Moine H, Prats AC, Vagner S. (2003) A single internal ribosome entry site containing a G quartet RNA structure drives fibroblast growth factor 2 gene expression at four alternative translation initiation codons. J Biol Chem 278:39330–39336
Gonzalez-Herrera IG, Prado-Lourenco L, Teshima-Kondo S, Kondo K, Cabon F, Arnal JF, Bayard F, Prats AC (2006) IRES-dependent regulation of FGF-2 mRNA translation in pathophysiological conditions in the mouse. Biochem Soc Trans 34:17–21
Klagsbrun M, Smith S, Sullivan R, Shing Y, Davidson S, Smith JA, Sasse J (1987) Multiple forms of basic fibroblast growth factor: amino-terminal cleavages by tumor cell- and brain cell-derived acid proteinases. Proc Natl Acad Sci USA 84:1839–1843
Doble BW, Fandrich RR, Liu L, Padua RR, Kardami E (1990) Calcium protects pituitary basic fibroblast growth factors from limited proteolysis by co-purifying proteases. Biochem Biophys Res Commun 173:1116–1122
Kawamoto A, Kawata H, Akai Y, Katsuyama Y, Takase E, Sasaki Y, Tsujimura S, Sakaguchi Y, Iwano M, Fujimoto S et al (1998) Serum levels of VEGF and basic FGF in the subacute phase of myocardial infarction. Int J Cardiol 67:47–54
O’Brien TS, Smith K, Cranston D, Fuggle S, Bicknell R, Harris AL (1995) Urinary basic fibroblast growth factor in patients with bladder cancer and benign prostatic hypertrophy. Br J Urol 76:311–314
Soutter AD, Nguyen M, Watanabe H, Folkman J (1993) Basic fibroblast growth factor secreted by an animal tumor is detectable in urine. Cancer Res 53:5297–5299
Fujimoto K, Ichimori Y, Kakizoe T, Okajima E, Sakamoto H, Sugimura T, Terada M (1991) Increased serum levels of basic fibroblast growth factor in patients with renal cell carcinoma. Biochem Biophys Res Commun 180:386–392
Santiago JJR, Fandrich R, Kardami E. (2005) Angiotensin-II stimulates expression and release of prohypertrophic hi-FGF-2 molecule by cardiac fibroblasts. J Mol Cellular Cardiol 38:834–834
Quarto N, Fong KD, Longaker MT (2005) Gene profiling of cells expressing different FGF-2 forms. Gene 356:49–68
Ma X, Hirst C, Cattini PA, Kirshenbaum L, Kardami E (2006) Nuclear FGF-2 triggers reciprocal communication between nucleus and mitochondria resulting in ERK1/2 pathway-dependent chromatin compaction and cell death. Circulation 114:48–48
Smith JA, Madden T, Vijjeswarapu M, Newman RA (2001) Inhibition of export of fibroblast growth factor-2 (FGF-2) from the prostate cancer cell lines PC3 and DU145 by Anvirzel and its cardiac glycoside component, oleandrin. Biochem Pharmacol 62:469–472
Florkiewicz RZ, Anchin J, Baird A. (1998) The inhibition of fibroblast growth factor-2 export by cardenolides implies a novel function for the catalytic subunit of Na+, K+-ATPase. J Biol Chem 273:544–551
Taverna S, Ghersi G, Ginestra A, Rigogliuso S, Pecorella S, Alaimo G, Saladino F, Dolo V, Dell’Era P, Pavan A et al (2003) Shedding of membrane vesicles mediates fibroblast growth factor-2 release from cells. J Biol Chem 278:51911–51919
Clarke MS, Caldwell RW, Chiao H, Miyake K, McNeil PL (1995) Contraction-induced cell wounding and release of fibroblast growth factor in heart. Circ Res 76:927–934
Sheikh F, Sontag DP, Fandrich RR, Kardami E, Cattini PA (2001) Overexpression of FGF-2 increases cardiac myocyte viability after injury in isolated mouse hearts. Am J Physiol Heart Circ Physiol 280:H1039–1050
Kaye D, Pimental D, Prasad S, Maki T, Berger HJ, McNeil PL, Smith TW, Kelly RA (1996) Role of transiently altered sarcolemmal membrane permeability and basic fibroblast growth factor release in the hypertrophic response of adult rat ventricular myocytes to increased mechanical activity in vitro. J Clin Invest 97:281–291
Bashkin P, Doctrow S, Klagsbrun M, Svahn CM, Folkman J, Vlodavsky I. (1989) Basic fibroblast growth factor binds to subendothelial extracellular matrix and is released by heparitinase and heparin-like molecules. Biochemistry 28:1737–1743
Vlodavsky I, Miao HQ, Medalion B, Danagher P, Ron D. (1996) Involvement of heparan sulfate and related molecules in sequestration and growth promoting activity of fibroblast growth factor. Cancer Metastasis Rev 15:177–186
Szebenyi G, Fallon JF (1999) Fibroblast growth factors as multifunctional signaling factors. Int Rev Cytol 185:45–106
Jin Y, Pasumarthi KB, Bock ME, Lytras A, Kardami E, Cattini PA (1994) Cloning and expression of fibroblast growth factor receptor-1 isoforms in the mouse heart: evidence for isoform switching during heart development. J Mol Cell Cardiol 26:1449–1459
Rapraeger AC, Krufka A, Olwin BB (1991) Requirement of heparan sulfate for bFGF-mediated fibroblast growth and myoblast differentiation. Science 252:1705–1708
Chua CC, Rahimi N, Forsten-Williams K, Nugent MA (2004) Heparan sulfate proteoglycans function as receptors for fibroblast growth factor-2 activation of extracellular signal-regulated kinases 1 and 2. Circ Res 94:316–323
Maher PA (1996) Nuclear translocation of fibroblast growth factor (FGF) receptors in response to FGF-2. J Cell Biol 134:529–536
Reilly JF, Maher PA (2001) Importin beta-mediated nuclear import of fibroblast growth factor receptor: role in cell proliferation. J Cell Biol 152:1307–1312
Bonnet H, Filhol O, Truchet I, Brethenou P, Cochet C, Amalric F, Bouche G (1996) Fibroblast growth factor-2 binds to the regulatory beta subunit of CK2 and directly stimulates CK2 activity toward nucleolin. J Biol Chem 271:24781–24787
Bouche G, Baldin V, Belenguer P, Prats H, Amalric F (1994) Activation of rDNA transcription by FGF-2: key role of protein kinase CKII. Cell Mol Biol Res 40:547–554
Walker DM, Yellon DM (1992) Ischaemic preconditioning: from mechanisms to exploitation. Cardiovasc Res 26:734–739
Bolli R. (2000) The late phase of preconditioning. Circ Res 87:972–983
Hausenloy DJ, Yellon DM (2006) Survival kinases in ischemic preconditioning and postconditioning. Cardiovasc Res 70:240
Yellon DM, Hausenloy DJ (2005) Realizing the clinical potential of ischemic preconditioning and postconditioning. Nat Clin Pract Cardiovasc Med 2:568–575
Yellon DM, Downey JM (2003) Preconditioning the myocardium: from cellular physiology to clinical cardiology. Physiol Rev 83:1113–1151
Gross ER, Gross GJ (2006) Ligand triggers of classical preconditioning and postconditioning. Cardiovasc Res 70:212–221
Padua RR, Sethi R, Davey-Forgie SE, Liu L, Dhalla NS, Kardami E (1996) Cardioprotection and basic fibroblast growth factor. Boston, Kluwer Academic Publishers, pp 501–518
Srisakuldee W, Jeyaraman M, Nickel BE, Jiang ZS, Fandrich RR, Kardami E (2005) Pre- as well as post-conditioning cardioprotection by fibroblast growth factor-2 is linked to the phosphorylation of connexin-43 at specific protein kinase C target sites. Circulation 112:U364–U364
Nishida S, Nagamine H, Tanaka Y, Watanabe G (2003) Protective effect of basic fibroblast growth factor against myocyte death and arrhythmias in acute myocardial infarction in rats. Circ J 67:334–339
House SL, Bolte C, Zhou M, Doetschman T, Klevitsky R, Newman G, Schultz Jel J (2003) Cardiac-specific overexpression of fibroblast growth factor-2 protects against myocardial dysfunction and infarction in a murine model of low-flow ischemia. Circulation 108:3140–3148
Ping P, Song C, Zhang J, Guo Y, Cao X, Li RC, Wu W, Vondriska TM, Pass JM, Tang XL et al (2002) Formation of protein kinase C(epsilon)-Lck signaling modules confers cardioprotection. J Clin Invest 109:499–507
Vondriska TM, Zhang J, Song C, Tang XL, Cao X, Baines CP, Pass JM, Wang S, Bolli R, Ping P (2001) Protein kinase C epsilon-Src modules direct signal transduction in nitric oxide-induced cardioprotection: complex formation as a means for cardioprotective signaling. Circ Res 88:1306–1313
Vondriska TM, Klein JB, Ping P (2001) Use of functional proteomics to investigate PKC epsilon-mediated cardioprotection: the signaling module hypothesis. Am J Physiol Heart Circ Physiol 280:H1434–1441
Inagaki K, Begley R, Ikeno F, Mochly-Rosen D (2005) Cardioprotection by epsilon-protein kinase C activation from ischemia: continuous delivery and antiarrhythmic effect of an epsilon-protein kinase C-activating peptide. Circulation 111:44–50
Liu GS, Cohen MV, Mochly-Rosen D, Downey JM (1999) Protein kinase C-epsilon is responsible for the protection of preconditioning in rabbit cardiomyocytes. J Mol Cell Cardiol 31:1937–1948
Baines CP, Zhang J, Wang GW, Zheng YT, Xiu JX, Cardwell EM, Bolli R, Ping P (2002) Mitochondrial PKCepsilon and MAPK form signaling modules in the murine heart: enhanced mitochondrial PKCepsilon-MAPK interactions and differential MAPK activation in PKCepsilon-induced cardioprotection. Circ Res 90:390–397
Hausenloy DJ, Tsang A, Mocanu MM, Yellon DM (2005) Ischemic preconditioning protects by activating prosurvival kinases at reperfusion. Am J Physiol Heart Circ Physiol 288:H971–976
House SL, Branch K, Newman G, Doetschman T, Schultz Jel J (2005) Cardioprotection induced by cardiac-specific overexpression of fibroblast growth factor-2 is mediated by the MAPK cascade. Am J Physiol Heart Circ Physiol 289:H2167–2175
Doble BW, Ping PP, Kardami E (2000) The epsilon subtype of protein kinase C is required for cardiomyocyte connexin-43 phosphorylation. Circ Res 86:293–301
Doble BW, Dang X, Ping P, Fandrich RR, Nickel BE, Jin Y, Cattini PA, Kardami E (2004) Phosphorylation of serine 262 in the gap junction protein connexin-43 regulates DNA synthesis in cell-cell contact forming cardiomyocytes. J Cell Sci 117:507–514
Srisakuldee W, Nickel BE, Fandrich RR, Jiang ZS, Kardami E (2006) Administration of FGF-2 to the heart stimulates connexin-43 phosphorylation at protein kinase C target sites. Cell Commun Adhesion 13:13–19
Yellon DM, Baxter GF (2000) Protecting the ischaemic and reperfused myocardium in acute myocardial infarction: distant dream or near reality? Heart 83:381–387
Gross GJ, Auchampach JA (2007) Reperfusion injury: does it exist? J Mol Cell Cardiol 42:12–18
Opie LH (1989) Reperfusion injury and its pharmacologic modification. Circulation 80:1049–1062
Hausenloy DJ, Yellon DM (2004) New directions for protecting the heart against ischaemia-reperfusion injury: targeting the Reperfusion Injury Salvage Kinase (RISK)-pathway. Cardiovasc Res 61:448–460
Garcia-Dorado D, Rodriguez-Sinovas A, Ruiz-Meana M, Inserte J, Agullo L, Cabestrero A (2006) The end-effectors of preconditioning protection against myocardial cell death secondary to ischemia-reperfusion. Cardiovasc Res 70:274–285
Zweier JL, Talukder MA (2006) The role of oxidants and free radicals in reperfusion injury. Cardiovasc Res 70:181–190
Kardami E, Detillieux KA, Jimenez SK, Cattini, PA (2006) Fibroblast growth factor-2 as a therapeutic agent against heart disease. Springer, pp 145–166
Horrigan MC, Malycky JL, Ellis SG, Topol EJ, Nicolini FA (1999) Reduction in myocardial infarct size by basic fibroblast growth factor following coronary occlusion in a canine model. Int J Cardiol 68(Suppl 1):S85–91
Horrigan MC, MacIsaac AI, Nicolini FA, Vince DG, Lee P, Ellis SG, Topol EJ (1996) Reduction in myocardial infarct size by basic fibroblast growth factor after temporary coronary occlusion in a canine model. Circulation 94:1927–1933
Padua RR, Kardami E (1993) Increased basic fibroblast growth factor (bFGF) accumulation and distinct patterns of localization in isoproterenol-induced cardiomyocyte injury. Growth Factors 8:291–306
Engvall E (1995) Structure and function of basement membranes. Int J Dev Biol 39:781–787
Vracko R. (1974) Basal lamina scaffold-anatomy and significance for maintenance of orderly tissue structure. Am J Pathol 77:314–346
D’Amore PA (1990) Modes of FGF release in vivo and in vitro. Cancer Metastasis Rev 9:227–238
Doble BW, Fandrich RR, Liu L, Padua RR, Kardami E (1990) Calcium protects pituitary basic fibroblast growth-factors from limited proteolysis by copurifying proteases. Biochem Biophys Res Commun 173:1116–1122
Beardslee MA, Lerner DL, Tadros PN, Laing JG, Beyer EC, Yamada KA, Kleber AG, Schuessler RB, Saffitz JE (2000) Dephosphorylation and intracellular redistribution of ventricular connexin43 during electrical uncoupling induced by ischemia. Circ Res 87:656–662
Schulz R, Gres P, Skyschally A, Duschin A, Belosjorow S, Konietzka I, Heusch G (2003) Ischemic preconditioning preserves connexin 43 phosphorylation during sustained ischemia in pig hearts in vivo. Faseb J 17:1355–1357
Piper HM, Garcia-Dorado D (1999) Prime causes of rapid cardiomyocyte death during reperfusion. Ann Thorac Surg 68:1913–1919
Inagaki K, Churchill E, Mochly-Rosen D (2006) Epsilon protein kinase C as a potential therapeutic target for the ischemic heart. Cardiovasc Res 70:222
Anversa P, Leri A, Kajstura J (2006) Cardiac regeneration. J Am Coll Cardiol 47:1769–1776
Gude N, Muraski J, Rubio M, Kajstura J, Schaefer E, Anversa P, Sussman MA (2006) Akt promotes increased cardiomyocyte cycling and expansion of the cardiac progenitor cell population. Circ Res 99:381–388
Uemura R, Xu M, Ahmad N, Ashraf M (2006) Bone marrow stem cells prevent left ventricular remodeling of ischemic heart through paracrine signaling. Circ Res 98:1414–1421
Bianchi G, Banfi A, Mastrogiacomo M, Notaro R, Luzzatto L, Cancedda R, Quarto R (2003) Ex vivo enrichment of mesenchymal cell progenitors by fibroblast growth factor 2. Exp Cell Res 287:98–105
Kofidis T, de Bruin JL, Yamane T, Tanaka M, Lebl DR, Swijnenburg RJ, Weissman IL, Robbins RC (2005) Stimulation of paracrine pathways with growth factors enhances embryonic stem cell engraftment and host-specific differentiation in the heart after ischemic myocardial injury. Circulation 111:2486–2493
Song H, Kwon K, Lim S, Kang SM, Ko YG, Xu Z, Chung JH, Kim BS, Lee H, Joung B et al (2005) Transfection of mesenchymal stem cells with the FGF-2 gene improves their survival under hypoxic conditions. Mol Cells 19:402–407
Dvorak P, Dvorakova D, Hampl A (2006) Fibroblast growth factor signaling in embryonic and cancer stem cells. FEBS Lett 580:2869–2874
Han W, Yu Y, Liu XY (2006) Local signals in stem cell-based bone marrow regeneration. Cell Res 16:189–195
Wang Y, Johnsen HE, Mortensen S, Bindslev L, Ripa RS, Haack-Sorensen M, Jorgensen E, Fang W, Kastrup J (2006) Changes in circulating mesenchymal stem cells, stem cell homing factor, and vascular growth factors in patients with acute ST elevation myocardial infarction treated with primary percutaneous coronary intervention. Heart 92:768–774
Ayach BB, Yoshimitsu M, Dawood F, Sun M, Arab S, Chen M, Higuchi K, Siatskas C, Lee P, Lim H et al (2006) Stem cell factor receptor induces progenitor and natural killer cell-mediated cardiac survival and repair after myocardial infarction. Proc Natl Acad Sci USA 103:2304–2309
Freed DH, Cunnington RH, Dangerfield AL, Sutton JS, Dixon IM (2005) Emerging evidence for the role of cardiotrophin-1 in cardiac repair in the infarcted heart. Cardiovasc Res 65:782–792
Chien KR (2000) Myocyte survival pathways and cardiomyopathy: implications for trastuzumab cardiotoxicity. Semin Oncol 27:9–14; discussion 92–100
Palmen M, Daemen MJ, De Windt LJ, Willems J, Dassen WR, Heeneman S, Zimmermann R, Van Bilsen M, Doevendans PA (2004) Fibroblast growth factor-1 improves cardiac functional recovery and enhances cell survival after ischemia and reperfusion: a fibroblast growth factor receptor, protein kinase C, and tyrosine kinase-dependent mechanism. J Am Coll Cardiol 44:1113–1123
Buehler A, Martire A, Strohm C, Wolfram S, Fernandez B, Palmen M, Wehrens XH, Doevendans PA, Franz WM, Schaper W et al (2002) Angiogenesis-independent cardioprotection in FGF-1 transgenic mice. Cardiovasc Res 55:768–777
Cuevas P, Carceller F, Martinez-Coso V, Asin-Cardiel E, Gimenez-Gallego G (2000) Fibroblast growth factor cardioprotection against ischemia-reperfusion injury may involve K+ ATP channels. Eur J Med Res 5:145–149
Acknowledgments
This work was supported (EK, PAC) by the Canadian Institutes for Health Research. ZS-J was supported by a postdoctoral award from the IMPACT-CIHR program. JJ-S and SKJ had studentship awards from the Manitoba Health Research Council and the Heart and Stroke Foundation of Canada, respectively.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kardami, E., Detillieux, K., Ma, X. et al. Fibroblast growth factor-2 and cardioprotection. Heart Fail Rev 12, 267–277 (2007). https://doi.org/10.1007/s10741-007-9027-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-007-9027-0