
Abstract
With an increasing ageing population, there is a growing concern about how the elderly would be looked after. The primary purpose of this paper is to develop scenario analysis using simulated data where various criteria are incorporated into modeling policy targets, and apply an intertemporal productivity analysis to observe inefficiencies as reform unfolds. The study demonstrates how dynamic network data envelopment analysis (DN-DEA) can be used to evaluate the changing productivity of residential aged care (RAC) networks over time. Results indicate that it takes 9 years for 90 % of the RAC networks to have 85 % or more of the total beds in high-level care, and an optimal bed capacity is reached by the end of year 7. Number of beds and registered nurses employed are the main sources of inefficiency. The common core inefficient cohort identified with the paper’s method represents a sub-group of RAC networks more deserving of closer managerial attention because of their constantly inefficient operations over time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
With a rapid rise in the ageing population in developed countries, there is an increasing concern regarding how this demographic with ever longer life spans will be cared for with the assistance of a shrinking taxpaying workforce. Another factor that compounds the stress on aged care facilities is the critical role played by registered nurses in delivering resident care outcomes, who happen to be in short supply (Productivity Commission, [1]).
Normally, governments, care providers and communities prefer to see retirees remain at home for as long as possible. Nevertheless, due to a variety of circumstances, individuals leave their homes to take up residence in permanent care where they are more closely monitored. Historically, such institutional care in Australia has been funded at two levels, namely, low-level care and high-level care. In April 2012, the Australian Federal Government announced its latest aged care reform package worth $3.7 billion over 5 years, where $660.3 million have been earmarked for residential aged care (RAC) facilities. This reform package entitled ‘Living Longer. Living Better.’ is designed to encourage retirees to remain in their homes for low-level care—supported by a range of hotel-type services and amenities beyond basic services. Thus, as the proposed reform unfolds over the next few years, a substantial reduction is expected in low-level care places offered in residential aged care networks, as well as a rise in high-level care.
The main purpose of the current study is to develop scenario analyses based on data generation that follows carefully selected criteria on variables designated as comprising key organizational inputs and outputs, while monitoring inefficiencies revealed by intertemporal productivity or efficiency analysis. The conceptual contribution to literature can be summarized as developing a network perspective on residential aged care that includes linked multiple divisions, and introducing a dynamic dimension to productivity analysis by including undesirable outputs or carry-overs from one period to the next.
The study demonstrates, for the first time, how dynamic network data envelopment analysis (DN-DEA) can be used to evaluate the productivity of residential aged care. An introduction to traditional DEA, as well as its applications in the context of various health care settings, can be perused in Ozcan [2] (also see Appendix A). Briefly, data envelopment analysis is a popular efficient frontier technique used for benchmarking the relative performance of various organizational units of similar operational structure. In a review of literature on frontier efficiency measurement in health care delivery, Hollingsworth [3] acknowledges the prevalence of DEA. The current study’s motivation is to help management better map the interactions across time among various resources (inputs) utilized in providing different levels of care and resident outcomes (outputs), thus identifying where the main potential improvements (inefficiencies) lie. The intertemporal nature of DN-DEA also allows governments to monitor the impact of policy changes that may concern RAC, as well as devise what-if or scenario analyses prior to implementation.
In view of the Federal government’s reform package, the paper later demonstrates how the method developed can be used with the policymakers and management in mind. For example, we undertake scenario analyses that model how long it would take for a pre-determined proportion of RAC facilities to reach a targeted minimum proportion of high-level care beds. Parameters selected are those that one is likely to encounter on the ground. The observed inefficiencies that may develop as a result of growing bed capacities are interpreted. We also identify a common core inefficient cohort of RAC networks that are likely to benefit the most from management’s efforts designed to bring about improvement to operations.
2 Framework for measuring the relative organizational productivity of RAC networks
2.1 Literature review
Literature on measuring the relative efficiency of nursing homes (which are part of the RAC facilities discussed in the current study) is dominated by traditional DEA applications (TDEA) focusing on technical efficiency (this observation is also made by Zhang, Unruh and Wan [4]). Technical efficiency is defined as the efficiency of a production process in converting inputs to outputs that is calculated independent of prices and costs. DEA, a non-parametric efficient frontier technique based on linear programming, measures the relative efficiencies of a group of operationally similar entities or peers in transforming inputs to outputs. TDEA would normally treat an organization as a black box, where a set of exogenous input(s) (resources) enter an organization and emerge as a set of final output(s), with no insight as to what happens in between.
We continue with a brief chronological review of the relevant literature on technical efficiency studies of nursing homes. One of the earlier publications to apply TDEA to nursing homes is Kleinsorge and Karney [5], where the authors compare results from a productivity model designed around economic variables versus a model that incorporates measures of quality. Others include Fizel and Nunnikhoven [6] investigating the impact of chain ownership on nursing home efficiency; Kooreman [7] analyzing the efficiency of nursing homes in utilizing labor and testing for associations between efficiency estimates and a number of quality indicators; Chattopadhyay and Ray [8] undertaking a study with a broader scope where the authors investigate technical, as well as size efficiencies of nursing homes; Ozcan, Wogen and Mau [9] examining a sample of nursing homes stratified by ownership and size; Björkgren, Häkkinen and Linna [10] calculating an extensive range of efficiency estimates that include cost, technical, allocative and scale efficiencies with a view to identifying inefficiencies at the ward level; Laine, Finne-Soveri, Bjorkgren, Linna, Noro and Hakkinen [11] exploring the association between quality of care and technical efficiency; Zhang et al. [4] assessing the impact of changes to the Medicare prospective payment system on the efficiency of nursing homes; Lee, Bott, Gajewski and Taunton [12] examining the efficiency of care planning processes; Lenard and Shimshak [13] reporting on quality and operating efficiencies at the state level; Shimshak, Lenard, and Klimberg [14] incorporating quality of care into DEA of nursing homes; and, Garavaglia, Lettieri, Agasisti and Lopez [15] also investigating technical efficiency with a focus on quality of care.
There are a number of common threads and trends in literature. For example, data used are mostly cross-sectional and inputs commonly consist of various types of labor measured in full-time equivalent (FTE) and number of beds; there appears to be a greater variation on the choice of outputs. In the same studies, DEA modeling is often input-oriented. Furthermore, radial DEA formulations are used that inherently assume proportional contractions in inputs or expansion of outputs that may be unrealistic at the point of implementing potential improvements suggested by DEA. Regarding the foci of research questions, there is also a shift towards including measures of quality of care—particularly noticeable in studies published in the 21st century. On the other hand, the association between efficiency estimates and size appears to be inconclusive.
2.2 Residential aged care as a dynamic network
As the starting point, we bring some of the insight gained from the literature review to bear on the task of designing a performance framework for residential aged care. Specifically, the current study also deems important the role of labor and number of beds on the input side of the efficiency evaluation, and the need to include measures of quality of care. Figure 1 depicts how an RAC facility with two main levels of care is modeled for the purpose of illustrating dynamic network productivity analysis. The model assumes a natural progression from one level of care to the next as people age and their circumstances and/or health care needs change. For example, as a person ages and health deteriorates, the person would be admitted into low-level care (LLC) (i.e., historically known as a hostel). If a person’s needs are more acute, the person would be looked after by a high-level care (HLC) team (i.e., in a nursing home). Therefore, the key resources at each level of care consist of a different mix of inputs such as registered nurses measured in full-time equivalent (RN-FTE), average length of service of registered nurses (RN-ALS) (i.e., experience in years as a measure of quality of care), and other caregivers (OC-FTE). The number of residents receiving a particular level of care is captured by the input variable number of beds (NB). We include the average resident classification score (ARCS, a score on a ten-point scale) designed to capture the level of care needed by residents, where a greater score implies more intensive care. Chesteen, Helgheim, Randall and Wardell [16] refer to a measure of resident disability as input quality and argue that it is linked to outcome quality. Under inputs, staffing (and experience) is emphasized because it is positively associated with better quality of care (Laine et al. [11]).

Modeling intertemporal organizational productivity for residential aged care networks with two levels of care. Note: For brevity, undesirable outputs or carry-overs are detailed only once, although the same items are assumed entering and exiting a given period. The intermediate product of ‘number of residents transferred’ is an output from the LLC division that becomes an input to the HLC division. Legend: RN-FTE registered nurses full-time equivalent; RN-ALS registered nurses average length of service; OC-FTE other caregivers full-time equivalent; NB number of beds; ARCS average resident classification score; ALOS average length of stay; HLC high-level care; LLC low-level care
In terms of resident care outcomes, we make an important distinction between desirable outputs and undesirable outputs. For example, the average length of stay (ALOS) measured in years is listed as a desirable output from a resident care perspective because the longer a resident stays in lower level care, the more independent and healthy that person is likely to be (this is essentially a proxy measure of quality of care). Even in high-level care, a longer stay is desirable because anyone who cannot be cared for in an HLC division is most likely to be moved to palliative care—increasingly also maintained at home.
Other resident care outcomes such as the annual number of hospitalizations (ANH), the average severity of hospitalizations (severity is measured on a ten-point rising scale), and mortality rate (MR represents residential deaths) are undesirable. That is, such variables would have a negative impact on the productivity or efficiency of a given level of care. Therefore, such negative outcomes are designated as undesirable outputs or carry-overs from one period to the next. This approach acknowledges that some LLC and/or HLC divisions may enter a period at a relative disadvantage if they have higher undesirable carry-overs than others (i.e., the dynamic dimension of the model). The three carry-overs can be viewed as measures of quality of care, and because only lower levels would be desirable, such variables are treated as inputs in the formulation of efficiency estimates (see Tone and Tsutsui [17] for a further discussion of carry-overs).
Finally, the number of residents being transferred from one level of care to the next represents divisional links (or intermediate products in DEA jargon). For example, people being transferred from an LLC to an HLC division become an undesirable output for an LLC division and an input for an HLC division. In this instance of vertical links seen in Fig. 1, the linkage is between different levels of care, rather than between the same divisions across time. The core structure of Fig. 1 is similar to Fig. 4 in Tone and Tsutsui [17].
We emphasize that the choice of input and output variables is a complex process at best, and in real life, it should reflect the interests of the policymakers and managers. That is, there is no universally accepted set of measures, and the models developed and the variables used therein should be those that are salient to people who will be making the key managerial decisions. This approach inherently assumes that management is capable of making decisions that take into account the interests of other key stakeholders in RAC such as the retirees and the people employed in such facilities.
2.3 Measuring technical efficiency with dynamic network DEA
According to Kooreman ([7], p.304), “… it is extremely difficult to define an external standard of an efficient nursing home sector. This makes a comparison of the relative performance of nursing homes as in DEA perhaps even more useful a tool of efficiency analysis”. Kooreman also points out the importance of technical efficiency analysis proposed in the current study because it is a prerequisite to cost efficiency analysis (i.e., a technically inefficient unit cannot be cost efficient).
In the RAC network setting depicted in Fig. 1, the black box would be the situation where the inputs and outputs of the two care levels or divisions are collapsed into one set of measures and vertical links and carry-overs are removed. Thus, traditional DEA does not explicitly identify the key sub-processes engaged by divisions of care level found within an organization, nor does it attempt to simultaneously capture the impact on productivity measurement of intertemporal linkages dubbed carry-overs. This shortcoming in efficiency literature is acknowledged by Hollingsworth and Peacock [18] as being of particular relevance to healthcare, and the authors mention the need to explore new ways to identify where technical improvements could be made. Traditional DEA also does not enable expert or managerial opinion to be brought to bear on weights representing divisional contributions. In essence, under DN-DEA (rather than traditional DEA) there is the opportunity to arrive at a more comprehensive measure of efficiency that incorporates divisional as well as intertemporal links (we re-visit DN-DEA in the method section).
As far as we can tell, the current study presents the first in-depth application of dynamic network DEA in a health care setting where a homogeneous organizational network structure is identified and various scenarios are tested. The only other application of network DEA (but without the dynamic dimension) in health care literature at the time of writing the current paper is the study of university hospitals in Brazil by Lobo, Lins, da Silva and Fiszman [19] using radial formulations. In their concluding paragraph, Lobo et al. [19] highlight the need for future studies to use non-radial formulations with weights, and dynamic evaluation of efficiency estimates over time. All these modeling improvements on network DEA are included in the current study, and the paper follows the intuitive framework in Fig. 1 that describes the main services in residential aged care. The emerging efficiency estimates may be used for ranking RAC networks, and more importantly, for identifying potential improvements. Nevertheless, a low estimate should not be used as an excuse to close down an RAC network or care level. Instead, DEA results can provide direction for those who oversee the sector to devise and navigate further investigations by other means in order to follow up initial findings.
3 Method
3.1 Main scenario for what-if analysis
Following consultations with executive of RSL Care (a not-for-profit care provider) and government publications, we construct a scenario analysis that may be of use to policy makers and other key decision makers (see http://www.rslcare.com.au/About_RSL_Care.cfm). Starting from the premise that implementation of sector reforms is best undertaken following what-if analyses, the main scenario put forward in this study demonstrates how the decision makers can first set various targets and then observe the results. Specifically, the government could target for, say, 90 % of the RAC networks to have 85 % or more of the total beds in high-level care. In an effort to make realistic assumptions about data generation parameters, the model allows for about 10 % of the networks failing to reach a targeted minimum proportion of high-level care beds.
In this modeling, the initial number of 526 RAC networks is maintained over time in the simulated sample, but growth in the number of high-level care beds and a simultaneous limited reduction in the number of low-level care beds are allowed. That is, the existing low-level care beds in RAC networks are not entirely removed because it is not realistic to assume all low-level care will be provided at home to everyone in the society. Full details of data simulation are reported in Appendix B.
In recognition of Federal government plans to re-configure RAC beds, a scenario is built into the data simulation where RAC networks undertake growth in their number of high-care beds; this growth is partly funded by closing down low-care beds while observing a minimum number of 50. The trade-off between high- and low-level care beds recognizes the limited resources and the government’s push to reduce institutional low-level care. The growth in high-care beds in the range of 5–10 % per annum continues across a number of years until the pre-determined targets mentioned earlier are reached. The modeling then proceeds to monitor how inefficiencies are introduced into the residential aged care sector under such a growth scenario. Findings based on the main scenario assumptions constitute the baseline results.
3.2 Dynamic network data envelopment analysis (DN-DEA)
The current section outlines the type of DN-DEA used in this study, namely, weighted, variable returns-to-scale, dynamic network range adjusted measure (DN-RAM). Under the network approach to DEA, the capability to determine each division’s contribution to organizational performance brings agility to managerial decision making in targeting desired outcomes and allocating resources. Similarly, introducing an intertemporal dimension captured by the word ‘dynamic’ accounts for the impact of a period’s managerial decisions on the following period. When network and dynamic dimensions are brought together under the same roof, a more comprehensive analysis is enabled where divisional and between-period interactions are reflected in efficiency estimates and more accurate potential improvements thus identified.
We model input-orientation in recognition of the discretionary input variables, and output variables that are outside direct managerial control—a choice that is also in line with what is reported in the literature. This means, the efficiency estimate for a given RAC network is based on economical use of inputs relative to other networks in the sample with similar output levels. Ozcan’s [20] reasoning, where he states that managers of health care facilities are more likely to have discretion in using lower levels of inputs in generating patient outputs, lends further support to input-orientation. Similarly, using variable returns-to-scale acknowledges the range of different size RAC networks simulated. A brief justification of the DN-RAM choice follows.
In recent research, Avkiran and McCrystal [21] systematically compare two non-radial DN-DEA models. The authors show that DN-RAM is more robust to data perturbations, more discriminating as evidenced by a greater range of efficiency estimates, and has additional desirable technical efficiency properties such as translation invariance when compared to a dynamic network model based on the slacks-based measure. According to Cooper, Park and Pastor [22], range adjusted measure (RAM) is a measure that permits easy interpretation in a variety of contexts because it captures the average proportion of inefficiencies that input/output ranges indicate as feasible.
Use of RAM as the core formulation in equations, instead of the more traditional CCR (Charnes, Cooper and Rhodes [23]) or BCC (Banker, Charnes and Cooper [24]) radial models, enables the analysis to capture the potential non-radial changes in inputs and outputs normally found in practice. Thus, in a similar manner to Avkiran and Morita [25] and Tone and Tsutsui [26], the current study also maintains that the radial input contractions or output expansions assumed in the CCR and BCC models are inappropriate unless proportionality in production is clearly established. In short, estimating non-proportional projections in RAC networks through RAM is a more realistic perception of an otherwise complex interaction among organizational variables. Formulations behind the dynamic network RAM are detailed in Appendix C.
4 Results
4.1 Time taken to reach key target ratios
Results indicate that it would take 9 years for 90 % of the RAC networks to have 85 % or more of the total beds in high-level care. An initial steady rise in the growth rate in total bed capacity in the sample of 526 RAC networks turns into a slowing growth after year 3 as more networks reach the targeted minimum proportion of high-level care beds. The average annual growth and the geometric mean growth rates are close to each other at 1.85 % and 1.66 %, respectively; the overall growth in bed capacity from year 1 to 9 is 15.75 %. Figure 2 charts the growth in bed numbers.

Charting growth in bed numbers across 9 years
An extended analysis reveals how long it would take RAC networks to reach the target proportion of 85 % in high-level care beds if policy makers were to aim for a number other than 90 % of the networks. For example, if we were to assume that all the RAC networks ought to reach the target ratio, the growth process will take 14 years—an additional 5 years on top of the original 9 years. Similarly, if the 90 % cut-off were assumed to be either 80 % or 70 %, the respective times would be 8 and 7 years.
Of course, other key variables in the model and research design can be changed to deliver results in different timeframes and with varying resourcing levels. For example, if the proportion of 90 % of the networks in the sample reaching the targeted minimum proportion of high-level care beds is kept constant, but the minimum proportion is raised to 95 % or lowered to 75 % instead, the number of years needed to attain such alternative targets would now be 29 and three, respectively. This bodes well for the original choice of 85 % proportion which is reached in a more realistic timeframe of 9 years by 90 % of the RAC networks (see Table 1 for a summary of these scenarios).
4.2 Efficiency estimates based on the 9-year time span, optimal bed capacity, and inefficiencies at the variable level
Figure 3 plots the total number of beds across 9 years against mean efficiency estimates at the RAC network and divisional levels based on baseline results. We start with DN-RAM estimates based on a 9-year span, and to arrive at the yearly estimates used in Fig. 3, we take into account inefficiencies for each year and re-compute efficiency estimates as per Eq. (C.2) in Appendix C. The mean network efficiency appears to closely follow the efficiency of HLC divisions where the number of networks is kept constant across the study period. On the other hand, the mean LLC estimates, while following a similar pattern, are substantially higher. Up-to year 4, all efficiency estimates are rising. In years 4 and 5, LLC mean efficiency estimates start dropping, while HLC is stable, thus leading to the leveling off of network estimates. An optimal bed capacity is reached by the end of year 7, based on organizational technical efficiency modeled in Fig. 1.

Charting annual mean RAC network and divisional efficiency estimates against number of beds across 9 years
Scrutinizing inefficiencies at the variable level represented by the slacks in Eq. (C.1) (Appendix C) helps better understand the efficiency estimate patterns observed in Fig. 3. Overall, growth in inefficiencies does not start in earnest until year 7. By year 8, the highest inefficiency growth rates are with the undesirable outputs, followed by discretionary inputs (details are available upon request). Focusing on the four discretionary inputs in Fig. 1 shows that, on average, the number of beds (29.92 %), followed by registered nurses employed (26.55 %), contribute the largest proportion of the inefficiencies in variables under managerial control. Other caregivers employed make the lowest contribution to inefficiencies embedded in discretionary input variables. This insight suggests that management ought to give more attention to bed numbers and registered nurses employed, whereas the number of other caregivers employed is relatively less critical in running efficient operations. The reader is reminded that in the context of the current study, the phrase ‘efficient operations’ refers to minimizing the use of various inputs identified in Fig. 1 for given levels of outputs.
4.3 Cumulative managerial decisions evaluated by progressive DN-RAM estimates and the common core inefficient cohort
The yearly estimates plotted in Fig. 3 are based on the initial 9-year period DN-RAM estimates. In order to compare dynamic estimates across different time periods separated by equal increments, eight separate DN-RAM tests are constructed, namely, for periods 1–2, 1–3, 1–4, 1–5, 1–6, 1–7, 1–8, and 1–9. We call this approach progressive DN-RAM which enables a comparison across two or more years and reveals the impact of cumulative managerial decisions made as the period under analysis is expanded and DN-RAM estimates from two consecutive periods are compared. Figure 4 shows a gradual rise in efficiency estimates as bed capacity rises, although the optimal point seen in Fig. 3 is not as clearly defined in Fig. 4. Nevertheless, a slow-down in efficiency improvement is noticeable as of period 1–7, which does coincide with the observation made in Fig. 3 regarding optimal bed capacity.

Charting periodic mean RAC network and divisional progressive DN-RAM efficiency estimates across eight periods
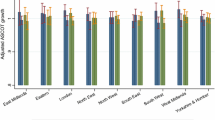
Next, we extend the inefficiency analysis to what Avkiran and McCrystal [27] call the core inefficient cohort (CIC) by taking advantage of the progressive DN-RAM analysis. That is, using an approach called layering or peeling the DEA onion first demonstrated in Barr, Durchholz, and Seiford [28], those RAC networks on the efficient frontier are removed until a core inefficient cohort emerges for each of eight periods. Next, those networks that are found in all the CICs are isolated. This common core inefficient cohort (C-CIC) can then be scrutinized for changes in rankings over time, as well as in which variables their main inefficiencies lie. Essentially, C-CIC forms the group of RAC networks management needs to monitor more closely. Here, the study adheres to the technical definition of ‘inefficient’, which implies a network with an efficiency estimate below 1. In practice, this definition may be altered by policy makers as, say, below 0.9.
Results indicate a C-CIC comprised of 424 RAC networks inefficient across eight dynamic efficiency evaluation periods. There is no clear pattern in the changes in inefficiencies from one dynamic efficiency evaluation period to the next (details available upon request). However, a closer scrutiny of the four discretionary inputs indicates that, on average, once again, the number of beds (30.02 %) is the source of the largest contribution to inefficiencies, followed by registered nurses employed (26.88 %). A further analysis could include ranking the C-CIC in descending order by efficiency estimates and focusing managerial scrutiny on, say, the bottom 10 % of this sub-group inefficient throughout eight periods. In order to highlight the differences in potential improvements among the C-CIC members, we compute the mean network efficiency for the units above the 90th and below the 10th percentiles, where the respective means are 0.9802 and 0.7254. Clearly, management stands to show potentially more for their efforts if the initial focus were to remain on those networks below the 10th percentile of the C-CIC sub-group.
4.3.1 Briefly following the productivity of two RAC networks over time
As described in Section 3.1, the main scenario includes a rise in the number of high-care beds in recognition of the Australian Federal government plans to re-configure RAC beds. Thus, for illustrative purposes, we monitor the progress of two RAC networks and their corresponding high-level care divisions across the study period. In our sample of 526 RAC networks, network #206 was relatively inefficient using DN-RAM for year 1 with an efficiency estimate of 0.5876. However, it was relatively efficient over the full study period of 1 to 9 years with a mean efficiency estimate of 0.8957. For example, for the HLC division within network #206, the number of beds increased by 19.6 % from years 1 to 9. This may indicate underutilization of potential capacity in the earlier years. Also in the HLC division the average length of stay increased by 0.85 year from year 1 to 9, which is a desirable outcome from a resident care perspective as argued in Section 2.2. Figure 5 charts annual efficiency estimates across 9 years.

Charting annual efficiency estimates for RAC networks #206 and #349 across 9 years
Network #349 was efficient using DN-RAM for year 1 with an efficiency estimate of 1. It was less efficient over the full study period of years 1 to 9 with a mean efficiency estimate of 0.8315. Once again focusing on the HLC division for comparison purposes, the number of beds increased by 46 % from year 1 to 9. This increase may have exceeded the network’s efficient expansion capacity. Also in HLC, the average length of stay declined by 0.58 year from years 1 to 9, which is an undesirable outcome.
5 Concluding remarks
We set out to illustrate how management can better pinpoint the interactions across time among various resources (inputs) used in providing different levels of care and resident outcomes (outputs), while identifying where main potential improvements (inefficiencies) lie. In doing so, we also demonstrate, for the first time, how the efficient frontier technique dynamic network data envelopment analysis (DN-DEA) can be applied in evaluating the productivity of residential aged care networks in a scenario analysis setting.
The scenario analyses demonstrated would hopefully be of use to policy makers and other key decision makers alike. The main scenario put forward in this study demonstrates how various targets can be determined first, followed by observation of the consequences of implementing them. In the main scenario of growing high-level care bed numbers, it takes 9 years for 90 % of the RAC networks to have 85 % or more of the total beds in high-level care. As efficiency estimates are scrutinized, an optimal bed capacity is observed by the end of year 7 based on organizational efficiency, and inefficiencies do not begin to rise substantially until year 7. Year 8 brings the highest inefficiency growth with undesirable outputs and discretionary inputs. Among the inputs under management control, number of beds and registered nurses employed make the largest contribution to inefficiencies.
Relying on progressive DN-DEA enables an analysis of the impact of cumulative managerial decisions as the period under analysis is expanded by 1 year at a time. Identifying the common core inefficient cohort across periods under study reveals a sub-group of RAC networks more deserving of closer managerial attention. Findings from investigating the relationship between efficiency estimates based on the full sample and ratio of high-level to low-level care beds suggests a moderate but negative impact on operating efficiency as more high care beds are introduced. This insight points to added pressure on resources if an RAC re-structure were to incorporate a growth in high-level care beds as modeled in the current study based on the proposed government reform.
The current study brings a level of sophistication not previously encountered in studies of technical efficiency of nursing homes. Simulated longitudinal data are used with non-radial DEA formulations that account for organizational structure (i.e., performance of divisions in a network structure) and the impact of carry-overs (i.e., the dynamic dimension in efficiency measurement). Quality of care is represented on both sides of the efficiency equation.
In conclusion, we anticipate the need for increasingly sophisticated modeling tools and research designs similar to that demonstrated in this study in order to better model residential aged care or nursing home facilities. Modeling, in turn, requires what-if analysis to facilitate planning for feasible service delivery in an environment of limited resources. The modeling illustrated and the efficiency measurement equations developed can be adapted for care facilities in other countries as well—first by identifying networks of interest and then the divisions therein.
References
Productivity Commission (2011) Caring for older Australians: overview. Final inquiry report no. 53. Canberra
Ozcan YA (2008) Health care benchmarking and performance evaluation: an assessment using Data Envelopment Analysis (DEA). Springer, Newton
Hollingsworth B (2008) The measurement of efficiency and productivity of health care delivery. Health Econ 17(10):1107–1128. doi:10.1002/Hec.1391
Zhang NJ, Unruh L, Wan TTH (2008) Has the Medicare prospective payment system led to increased nursing home efficiency? Health Serv Res 43(3):1043–1061. doi:10.1111/j.1475-6773.2007.00798.x
Kleinsorge IK, Karney DF (1992) Management of nursing homes using data envelopment analysis. Socio Econ Plan Sci 26(1):57–71. doi:10.1016/0038-0121(92)90026-2
Fizel JL, Nunnikhoven TS (1993) The efficiency of nursing home chains. Appl Econ 25(1):49–55. doi:10.1080/00036849300000112
Kooreman P (1994) Nursing home care in The Netherlands: a nonparametric efficiency analysis. J Health Econ 13(3):301–316. doi:10.1016/0167-6296(94)90029-9
Chattopadhyay S, Ray SC (1996) Technical, scale, and size efficiency in nursing home care: a nonparametric analysis of Connecticut homes. Health Econ 5(4):363–373. doi:10.1002/(Sici)1099-1050(199607)5:4<363::Aid-Hec217>3.0.Co;2-1
Ozcan YA, Wogen SE, Mau LW (1998) Efficiency evaluation of skilled nursing facilities. J Med Syst 22(4):211–224. doi:10.1023/A:1022657600192
Bjorkgren MA, Hakkinen U, Linna M (2001) Measuring efficiency of long-term care units in Finland. Health Care Manag Sci 4:193–200
Laine J, Finne-Soveri UH, Bjorkgren M, Linna M, Noro A, Hakkinen U (2005) The association between quality of care and technical efficiency in long-term care. Int J Qual Health Care 17(3):259–267. doi:10.1093/intqhc/mzi032
Lee RH, Bott MJ, Gajewski B, Taunton RL (2009) Modeling efficiency at the process level: an examination of the care planning process in nursing homes. Health Serv Res 44(1):15–32. doi:10.1111/j.1475-6773.2008.00895.x
Lenard ML, Shimshak DG (2009) Benchmarking nursing home performance at the state level. Health Serv Manag Res 22:51–61
Shimshak DG, Lenard ML, Klimberg RK (2009) Incorporating quality into data envelopment analysis of nursing home performance: a case study. OMEGA Int J Manag Sci 37:672–685
Garavaglia G, Lettieri E, Agasisti T, Lopez S (2011) Efficiency and quality of care in nursing homes: an Italian case study. Health Care Manag Sci 14(1):22–35. doi:10.1007/s10729-010-9139-2
Chesteen S, Helgheim B, Randall T, Wardell D (2005) Comparing quality of care in non-profit and for-profit nursing homes: a process perspective. J Oper Manag 23(2):229–242. doi:10.1016/j.jom.2004.08.004
Tone K, Tsutsui M (2014) Dynamic DEA with network structure: a slacks-based measure approach. OMEGA Int J Manag Sci 42:124–131
Hollingsworth B, Peacock SJ (2008) Efficiency measurement in health and health care. Routledge, Abingdon
Lobo MSC, Lins MPE, da Silva ACM, Fiszman R (2010) Assessment of teaching-health care integration and performance in university hospitals. Rev Saude Publica 44:1–10
Ozcan YA (2009) Quantitative methods in health care management: techniques and applications. Jossey-Bass, San Fransisco
Avkiran NK, McCrystal A (2013) Dynamic network range-adjusted measure vs. dynamic network slacks-based measure. Workshop on Dynamic and Network DEA 2013, January 29-30, National Graduate Institute for Policy Studies, Tokyo
Cooper WW, Park KS, Pastor JT (2001) The range adjusted measure (RAM) in DEA: a response to the comment by Steinmann and Zweifel. J Prod Anal 15(2):145–152. doi:10.1023/A:1007882606735
Charnes A, Cooper WW, Rhodes E (1978) Measuring the efficiency of decision-making units. Eur J Oper Res 2(6):429–444
Banker RD, Charnes A, Cooper WW (1984) Some models for estimating technical and scale inefficiencies in data envelopment analysis. Manag Sci 30(9):1078–1092
Avkiran NK, Morita H (2010) Predicting Japanese bank stock performance with a composite relative efficiency metric: a new investment tool. Pac Basin Financ J 18(3):254–271. doi:10.1016/j.pacfin.2010.01.002
Tone K, Tsutsui M (2010) Dynamic DEA: a slacks-based measure approach. Omega Int J Manag Sci 38(3–4):145–156. doi:10.1016/j.omega.2009.07.003
Avkiran NK, McCrystal A (2012) Sensitivity analysis of network DEA: NSBM versus NRAM. Appl Math Comput 218:11226–11239
Barr RS, Durchholz ML, Seiford L (1994) Peeling the DEA onion: layering and rank-ordering DMUs using tiered DEA. Southern Methodist University Technical Report
Charnes A, Cooper WW, Rhodes E (1981) Evaluating program and managerial efficiency—an application of data envelopment analysis to program follow through. Manag Sci 27:668–697
Gelade G, Gilbert P (2003) Work climate and organizational effectiveness: the application of data envelopment analysis in organizational research. Organ Res Methods 6:482–501
Cooper WW, Seiford LM, Zhu J (2011) Handbook on data envelopment analysis, 2nd edn. Kluwer Academic Publishers, Norwell
Bougnol ML, Dula JH, Lins MPE, da Silva ACM (2010) Enhancing standard performance practices with DEA. Omega Int J Manag Sci 38(1–2):33–45. doi:10.1016/j.omega.2009.02.002
Australian Institute of Health and Welfare (2010) Residential aged care in Australia 2008–09: A statistical overview. Aged Care Statistics Series No. 31. Cat. no. AGE 62. AIHW, Canberra
Schnelle JF, Simmons SF, Harrington C, Cadogan M, Garcia E, Bates-Jensen BM (2004) Relationship of nursing home staffing to quality of care. Health Serv Res 39(2):225–250. doi:10.1111/j.1475-6773.2004.00225.x
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendices
1.1 Appendix A
1.1.1 An introduction to traditional data envelopment analysis
This brief introduction is for the benefit of those who may not be familiar with traditional DEA (TDEA); network DEA and dynamic network DEA are extensions of TDEA. TDEA is a non-parametric efficient frontier technique that calculates a comparative ratio of weighted outputs to weighted inputs for the modeled production in each organizational unit—often reported as an estimate of relative technical efficiency.
TDEA operates under the condition of Pareto optimality where a decision-making unit (DMU), or in the current study, an RAC network, is not efficient if an output can be raised without raising any of the inputs and without lowering any other output. Similarly, a DMU is not efficient if an input can be decreased without decreasing any of the outputs and without increasing any other input (Charnes, Cooper and Rhodes [29]). We also note that there are many different ways a DMU and its divisions or sub-units can be conceptualized and such divisions do not have to be physical units. For example, a DMU could be a particular demographic such as 65–75 year-olds in a suburb, and divisions could be males and females in this age group or various income brackets before health care is investigated.
TDEA generates information on whether performance can be improved relative to observed benchmark behavior in a peer group, rather than relative to measures of central tendency. The relative efficiency estimate (or score) is often written as a number between 0 and 1, and a DMU with an estimate of less than 1 is labeled inefficient. Those units on the efficient frontier (benchmark units) then determine the potential improvements for the inefficient units that lie off the frontier.
Key advantages of DEA include the property that no functional structure is imposed on the data in estimating relative efficiency. In other words, DEA does not pre-suppose a particular production technology found in all the DMUs in a sample. The significance of this approach is that an organization’s efficiency can be estimated based on other observed performance in that sample by benchmarking peers that are better at managing their inputs and outputs. Similarly, variable weights are endogenously determined rather than relying on subjective weights. Another advantage of DEA is its ability to process multiple inputs and multiple outputs in arriving at a single estimate for a DMU—something which cannot be achieved with ratio analysis because individual ratios are most unlikely to be independent. Gelade and Gilbert ([30], p. 497) state that, “… the way in which performance measures are combined in DEA rests on strong theoretical foundations of production economics, allowing overall efficiency to be computed in circumstances in which additive scales cannot be legitimately constructed.”
In summary, DEA captures the interactions among multiple inputs and multiple outputs that can be traced to operational processes, and locates relative weaknesses of an inefficient organization against its best performing peers. The reader is encouraged to refer to Cooper, Seiford and Zhu [31] for a more in-depth treatment of DEA. A paper that bridges theory and practice by demystifying DEA mathematics is Bougnol, Dula, Lins and da Silva [32].
1.2 Appendix B
1.2.1 Background to data generation
In order to operationalize data simulation, and thus, the illustration of DN-DEA in residential aged care, a number of assumptions are made regarding the organization of RAC, the two care levels therein, and the various interacting variables of service delivery. For example, in profiling metropolitan residential aged care, full occupancy is assumed at any given point in time, which is often what is seen in real life. In fact, the statistics compiled on RAC by the Australian Institute of Health and Welfare [33] indicate an occupancy rate of 93 % as at 30 June 2009. Furthermore, all else the same, the length of stay for a resident at a given care level is assumed to be prolonged when more staff resources are available. Similar to Laine et al. [11], Schnelle, Simmons, Harrington, Cadogan, Garcia and Bates-Jensen [34] also conclude that higher quality of care in nursing homes is associated with higher staffing levels.
Once again all else the same, ALOS would drop when ARCS rises because of a higher level of care needed, which may trigger relocation to another care level. Australian Institute of Health and Welfare ([33], p.79) reports that approximately 10 % of the low-care residents were reclassified as high-care in 2008–09. This figure is used to determine the proportion of residents to be annually transferred from LLC to HLC. Nevertheless, such relocation is unlikely to involve a change of address since the ‘ageing in place’ policy introduced by the Aged Care Act of 1997. According to the Australian Institute of Health and Welfare [33], only 2 % of permanent residents who moved from low-level to high-level care in 2008–09 were actually relocated to another facility; the report indicates ALOS at the time of separation to be about 3 years.
The same report identifies roughly three-quarters of permanent admissions as aged 80 years or older. In Australia, resident dependency levels are determined by the Aged Care Funding Instrument (http://www.health.gov.au/acfi). According to Australian Institute of Health and Welfare ([33], p.83), about three-quarters of permanent residents were appraised as high-care as at 30 June 2009. This ratio guides the initial data generation for number of beds.
Interactions among the five inputs lead to the primary output of length of stay, as well as the undesirable carry-overs such as hospitalization and mortality. Assuming a performance evaluation period of 1 year, the relationships put forward below depict interactions among the variables and divisions outlined in Fig. 1 in the associated paper. Various assumed data ranges and weights, while arbitrary for illustrative purposes because we are not privy to real-world data where we could observe distributions, follow reasonable expectations and can be easily changed for further what-if analyses. For example, to reflect the increased focus by policy makers on high-level care beds within an RAC network, the divisional weights LLC (0.20) and HLC (0.80) are allocated for the purpose of computing overall efficiency estimates. Essentially, an algorithm is modeled where the number of beds primarily determines RN-FTE, which in turn drives OC-FTE; the average resident classification score for a division determines the average length of service for registered nurses; the average length of stay is affected by ARCS and RN-ALS in opposite directions; and, the annual number of hospitalizations are linked to the number of beds and ARCS.
We allow a small range of variation in determining staffing levels in order to reflect differences in managerial decision-making and regional differences in the availability of labor. Thus, initially the number of beds is randomly generated in the range of 50–100 for an LLC division, followed by randomly generated numbers of registered nurses in a narrower range. For each bed, we allocate 0.10–0.12 of an RN-FTE (i.e., a minimum of 5 RN-FTE for 50 residents); similarly, for each RN-FTE, 1.5–2.5 other caregivers are allocated, where once again, random number generation proceeds in the assumed ranges. For an HLC division, the number of beds range between 150 and 300. For each bed, 0.12–0.15 of an RN-FTE is allocated, and for each RN-FTE 2–3 other caregivers are allocated, thus reflecting the more intensive care at this level.
The average length of service (RN-ALS) of registered nurses—considered to be the key caregivers—is linked to the average resident classification score (ARCS) that captures the overall health of residents in a division. That is, as the health of residents deteriorates and ARCS rises, we assume that registered nurses with greater experience would be recruited to better meet the more complex care needed. Residential classification scores (on a scale of 1–10) are allowed to randomly vary where the distribution for LLC is skewed towards the lower end, and a corresponding RN-ALS of 0.5–1.0 year is allowed for every point in the ARCS. Similarly, the residential classification scores for an HLC division are skewed towards the higher end.
In determining the average length of stay of residents (years) in a division, we begin with random number generation between these ranges: LLC (2–5); HLC (1–4). ALOS is then adjusted to reflect ARCS. That is, for every point in ARCS above 1, ALOS is reduced by 1/10th of a year in recognition of the non-discretionary element in managing residents’ health. We adjust ALOS for the second time by raising it by 1/10th of a year for every year of RN-ALS above 2 years in recognition of the discretionary element in residents’ health which can be shaped by the quality of care. Here, the focus is specifically on the experience of registered nurses rather than just physical staffing levels.
Finally, the undesirable outputs from divisions (carry-overs) are modeled. Random data generations adhere to the following ranges: for each bed in an LLC division, the annual number of hospitalizations or ANH equals (0.01–0.08); this number is then multiplied with ARCS. For an HLC division, the annual number of hospitalizations varies in the range of 0.06–0.10, followed by factoring in ARCS. The average severity of hospitalizations (ASH) is considered generally unpredictable and modeling adheres to random number generation, but a distributional skew towards 1 for an LLC and towards 10 for an HLC division is included. Progressively higher ranges in the form of (5–15) for an LLC division, and (10–30) for an HLC division, are assumed for MR or mortality rate (%)—allowed to vary randomly.
The following algorithm summarizes the steps in generating initial data for 526 RAC networks. Data generation incorporates the variable relationships shown in Fig. 1. The tilde symbol (∼) is used to indicate how the values for a given variable are distributed. All figures below are at the DMU level unless stated otherwise.
Generate RAC networks and number of high- and low-care beds:
-
The number of residents is approximately based on Table A5.2 found in the Australian Institute of Health and Welfare [33]. In this report, the overall ratio of high-care to low-care beds is about 3:1, which we use to set the parameters for generating the number of beds. Thus,
-
Number of HLC beds (input):
-
∼ U[150,300], integers only.
-
526 RAC networks are generated. The total number of generated HLC residents is 117,940 which closely approximates the figure of 117,884 from Table A5.2 (Australian Institute of Health and Welfare [33]).
-
-
Number of LLC beds (input):
-
∼ U[50,100], integers only.
-
This produces an LLC population of 39,804.
-
-
Select networks to be grown and apply growth rates:
-
A compound growth rate ∼ U[0.05,0.10] is applied to high-level care beds in those networks that have a proportion of high-level care beds below 85 % of the total beds. The number of beds is rounded to an integer in each year. This gives rise to the variables of hlbeds, llbeds for each network-year.
-
In each year, the growth in hlbeds simultaneously reduces llbeds without dropping lower than a minimum number of 50 llbeds for a given network.
-
The variables below are generated for each network-year:
-
Number of Registered Nurses (input):
-
hlrn ∼ U[0.12,0.15] * hlbeds
-
llrn ∼ U[0.1,0.12] * llbeds
-
-
Number of Other Caregivers (input):
-
hloc ∼ U[2, 3] * hlrn
-
lloc ∼ U[1.5, 2.5] * llrn
-
-
Average Resident Classification Score (input):
-
Underlying HLC RCS ∼ Triangular distribution with minimum 0.5, maximum 10.5, mode 8.57, rounded to integers that result in values 1–10.
-
Underlying LLC RCS ∼ Triangular distribution with minimum 0.5, maximum 10.5, mode 1.43, rounded to integers that result in values 1–10.
-
The underlying RCS’s are fully randomized across network-years. The average is then taken for each network-year to form hlarcs and llarcs.
-
-
Average Length of Service of Registered Nurses (input):
-
hlals ∼ U[0.5, 1] * hlarcs
-
llals ∼ U[0.5, 1] * llarcs
-
-
Average Length of Stay (output):
-
hlalos ∼ U[1, 4] − 0.1 * (hlarcs − 1) + 0.1 * (hlals - 2)
-
llalos ∼ U[2, 5] − 0.1 * (llarcs − 1) + 0.1 * (llals - 2)
-
-
Number of Hospitalizations (undesirable carry-over):
-
hlh ∼ ceil(U[0.06, 0.10] * hlbeds * hlarcs)
-
llh ∼ ceil(U[0.01, 0.08] * llbeds * llarcs)
-
-
Average Severity of Hospitalizations (undesirable carry-over):
-
Underlying HLC severity of hospitalization ∼ Triangular distribution with minimum 0.5, maximum 10.5, mode 8, rounded to integers that result in values 1–10.
-
Underlying LLC severity of hospitalization ∼ Triangular distribution with minimum 0.5, maximum 10.5, mode 3, rounded to integers that result in values 1–10.
-
The underlying hospitalization severities are fully randomized across network-years. The average is then taken for each network-year to form hlash and llash.
-
-
Mortality Rate (%) (undesirable carry-over):
-
hlmort ∼ U[10, 30]
-
llmort ∼ U[5, 15]
-
Number of Residents Transferred from low-care to high-care (intermediate product): Permanent residents in low-care are ranked in descending order on their residential classification scores (RCS) and the top 10 % is winsorised. This top 10 % represents the total number of residents transferred from low-care to high-care.
1.3 Appendix C
1.3.1 Dynamic network range-adjusted measure of efficiency (DN-RAM)
subject to
where,
- o :
-
the observed DMU, o = 1,…, N
- N :
-
the number of DMU’s
- k, h :
-
a division (K = number of divisions)
- m k :
-
number of inputs for division k
- r k :
-
number of outputs for division k
- i k :
-
number of input links for division k
- b k :
-
number of bad carry overs for division k
- s t − ok :
-
input slack for division k, time t
- s t + ok :
-
output slack for division k, time t
- s t o(k,h) :
-
slack for intermediate product link between division k and division h, time t
- s (t,t + 1) ok :
-
slack for bad carry over for division k from time t to time (t + 1)
- λ t k :
-
intensity vector for division k, time t
- X t k :
-
is the input matrix for division k, time t where \( {X}_k^t=\left({x}_1^t,\dots, {x}_K^t\right)\in {R}^{{\mathrm{m}}_k\times T} \)
- Y t k :
-
is the output matrix for division k, time t where \( {Y}_k^t=\left({y}_1^t,\dots, {y}_K^t\right)\in {R}^{r_k\times T} \)
- Z t(k,h) :
-
intermediate product input link between division k and division h at time t
- Z (t,t + 1) k :
-
bad carry over for division k from time t to time (t + 1)
- R t − mk :
-
range of input m, division k, time t = max(x t − mk ) − min(x t − mk )
- R t l(k,h) :
-
range of l th, input link variable between division k and h, time t = max(z t l(k,h) ) − min(z t l(k,h) )
- R (t,t + 1) nk :
-
range of n th, bad carry over variable, division k, time t = max(z (t,t + 1) nk ) − min(z (t,t + 1) nk )
- ∑ K k = 1 w k = 1, w k ≥ 0(∀ k):
-
where w k is the relative weight of division k determined exogenously
- ∑ T t = 1 W t = 1, W t ≥ 0(∀ t):
-
where W t is the relative weight of time t determined exogenously
Rights and permissions
About this article
Cite this article
Avkiran, N.K., McCrystal, A. Intertemporal analysis of organizational productivity in residential aged care networks: scenario analyses for setting policy targets. Health Care Manag Sci 17, 113–125 (2014). https://doi.org/10.1007/s10729-013-9259-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10729-013-9259-6