
Abstract
Patients with advanced dementia are less likely than those with other terminal illnesses to receive palliative care. Due to the nature and course of dementia, there may be a failure to recognize the terminal stage of the disease. A possible and under-investigated explanation for this healthcare disparity is the healthcare practitioner who plays a primary role in end-of-life decision-making. Two potential areas that might impact provider decision-making are cognitive biases and moral considerations. In this analysis, we demonstrate how the cognitive biases and moral considerations of practitioners related to clinical decision-making are inherent in clinical practice and may impact on providers’ accuracy related to diagnostic and treatment related decision-making associated with patients with advanced dementia. Anchoring, default, availability, representativeness and framing biases are cognitive biases based on the "Two System Model" that relate to decision-making in end-of-life care. In patients with advanced dementia, those biases may result in a tendency to adhere to traditional mandatory care, involving an aggressive approach to care, which values saving lives at all costs, without taking into account the possible suffering and long-term consequences. Aspects such as moral sensitivity and moral courage play an important role in ethical decision-making related to advanced dementia. Investigations of clinical decision-making that include the cognitive biases and ethical considerations of practitioners might advance the comprehensive understanding of the clinical decision-making process related to care of patients with advanced dementia and promote the quality of care given to this population.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Dementia is a progressive, incurable disease often leading to death [65, 69]. The advanced stages of dementia are associated with complete dependence on long-term care, often resorting to artificial and aggressive therapies requiring treatment with drugs and devices [48]. Differences in the presentation of patients with dementia and a lack of knowledge and training in geriatrics among medical teams results in a poor understanding of the course and nature of the disease, with decreased recognition of its terminal stages [39].
Terminal disease decision-making resolves around two basic types of medical decisions. The first is to continue routine care and extend life, often involving an aggressive, acute approach, more associated with curing illness. The second is to change the goal of treatment from routine care that extends life to an approach primarily concerned with symptom management and improvement of the quality of life, which might or might not extend life. Moving from the first to the second model is termed changing the goals of care [53].
When a patient approaches the terminal stages of a chronic illness, it is common to change the goal of care from curing the patient to comfort or palliative care [54, 65]. Goals of care decision-making for patients with advanced dementia present a common clinical challenge among various medical specialties. Despite reports of the benefits of palliative care for this population, and evidence that life-sustaining medical interventions are not always desirable [54, 69], patients with dementia have been shown to receive routine care focusing on the acute and immediate, known as the “local approach” [35]. Usually, in the acute care setting, the medical staff adopts a traditional treatment approach based on aggressive life-prolonging therapy. Studies have shown that this does not lead to an improved prognosis or better quality of life [9, 26, 54]. In addition, those with advanced dementia receive less or sub-optimal palliative care than patients with other terminal diseases [62, 65, 68, 72, 77].
Several barriers are associated with decreased use of palliative or comfort care in the advanced dementia patient population. These include administrative influences, regulatory and organizational policy, education and training, communication in its various aspects, and socio-demographic variables of the healthcare provider [23]. Another major barrier is the poor level of end-of-life prognostication [4]. Previous studies that investigated the process of decision-making related to goals of care and the barriers associated with such decisions rarely took human factors into account.
The question often arises as to whether it is necessary to sustain a life that some people may consider not worth living [48]. Decisions regarding goals of care among this patient population are different from other chronic, life-threatening diseases [76]. During the end stage of dementia the patient cannot communicate preferences or take an active part in treatment decisions. Therefore, caregivers cannot know the patient’s preferences with certainty, and thereby make their decisions based on prior discussions, their acquaintance with the patient, or documented advance directives. Treatment decisions should be made using a surrogate or legally valid proxy, in accordance with local laws, perceived as the patient's best interest, and based on the patient's prior wishes [53]. This process is particularly challenging, due to the emotional and value-laden choices that must be made on behalf the patient. Studies have shown that some treatment options are often not sufficiently utilized and goals of care discussions are missing [76]. In some situations, it seems that decisions express the position of the surrogate decision-maker, which does not necessarily match the known prior preferences of the patient.
In addition, our understanding of neurodegenerative diseases is inadequate, including a lack of a true understanding of the patient’s experiences and sense of wellbeing [28, 34]. In light of this epistemic gap, intuition and bias can either contribute to decision-making or significantly impair the process. While theoretical knowledge is gained during professional training, practitioners rely on their own personal characteristics, resources, experiences, and understanding when practicing in their field. All of these characteristics are integrated into an overall fabric and result in a personal “art of practice” [34]. It is possible that this “art” can be also be a source of bias.
The objective of this paper is to highlight a missing link: the thought processes and potential biases of a primary decision-maker, the medical practitioner, that may influence clinical decisions. We explore the decision-making process as defined by the “Two-System Model”, which includes cognitive bias as well as moral judgment, moral sensitivity, and moral courage as they relate to ethical decision-making. We analyze the impact and potential influences of these components on the clinical decision-making process for patients with advanced dementia.
The Decision-Making Process
The “Two-System Model”
Understanding individual thought processes is important when investigating clinical decision-making, as thinking is the core of healthcare professional practice [70]. Decisions may take place in a rapid, intuitive, automatic, emotional, and stereotypic manner (system 1), or under slow, effortful, logical, calculating and conscious thought (system 2). Daniel Kahneman defines these two options as a two-system approach (or the Dual Process Theory) that acts as two distinct subsystems competing within reasoning processes [31, 42]. Functional magnetic resonance imaging has demonstrated that the two processes involve different cortical mechanisms with associated neurophysiological and neuroanatomical substrates [15]. This dual system model is applicable to medical decision-making. Mental shortcuts or heuristics use the first system and can speed up decision-making. The use of heuristics may be a practical tool that directs and guides decision-making, and is applicable in many areas, including decision-making related to patients with dementia [42]. These quick solutions can lead to bias since not all of the alternatives are evaluated when making a decision.
Cognitive Bias
Cognitive Bias in Clinical Settings
Unlike error, which results from incorrect or inaccurate information and/or impaired judgment, cognitive bias refers to a pattern of thinking and judgment resulting from disproportionally deciding in favor of or against one position based on missing data or partial data [58]. There are many forms of cognitive bias that affect decision-making, thereby deviating thoughts from what is commonly considered the norm or rational thinking [21]. We assume that clinical decision-making is entirely rational. However, when a decision is made in an environment of uncertainty, emotion or stress (situations common in the medical workplace) [2, 45, 70], then the decision tends not to be rational and might be biased [3, 7, 59].
Bioethicists have recently begun to look at how cognitive biases influence medical choices and actions. If clinicians are trained to prefer the use of heuristics when making a clinical decision, then the provider will tend to make a decision based on the heuristic and not on all of the medical evidence or patient signs and symptoms. For example, a physician might diagnose a patient who presents with respiratory symptoms as having aspiration pneumonia, rather than a pulmonary embolism, due to an assumption that the patient has previously been diagnosed with swallowing disorder and is more likely to contract pneumonia than have a pulmonary embolism. There is cause for concern regarding how these cognitive biases may diminish and distort a person's understanding of the nature of a decision and its foreseeable consequences, change the "feeling" about a situation, and the way relevant information is processed [6].
Decision-making also occurs within a social context. Hospitals, for the most part, use traditional hierarchical chains of command [59]. In addition, healthcare providers are socialized into conformity behavior and perceived professional norms. In other words, workers' beliefs about what is considered proper behavior is partially determined by the healthcare professional's perception of how colleagues and superiors would behave in similar circumstances. These perceived professional norms along with perceptions gained during professional training direct clinical decision-making [38, 58, 63], and often lead to unintentional biases when making clinical decisions.
Anchoring and Default Bias
The human brain prefers to work under lower levels of cognitive effort [42]. As a result, humans intuitively think and act according to system I, or use heuristics and other mental shortcuts. This type of thinking creates a cognitive bias, called an anchoring bias, and refers to the tendency to judge a situation based on the familiar. A decision is based on what is known and is considered to be the acceptable norm [38, 57, 74]. This may result in passively making a decision that requires less psychological and cognitive effort, with less potential burden on the decision-maker [57]. The use of these anchoring biases can reduce uncertainty and insecure feelings [2, 19, 38, 45]. On the other hand, biases lead to an automatic way of thinking, based on context, previous learning and experience, social and professional orientation, and organizational climate. Such a decision also maintains emotional distance and withdrawal or avoidance of the patient and family in order to prevent potential conflicts and moral distress [2, 45, 63, 70].
For example, extending life at any cost is an embedded and anchored medical bias. Practitioners who believe in this axiom may try to defend such practices even if their argument for doing so is invalid. In many Western cultures, patient's autonomy and the patient's right to quality of life is highly valued. Do the patient and the patient’s family prefer to extend life knowing that there might be increased pain and suffering, or do they prefer quality of life above extending life? Caregivers acknowledge that a patient is nearing the end of life, but due to the common anchoring bias of saving life at any cost, medical decisions are often made without considering the patient's autonomy or quality of life. Aggressive care may be continued, despite the wishes of the patient [10]. Less common, but also possible, is the possibility of an inherent practitioner or institutional bias towards preserving quality of life, and, in this case, clinical decisions will be biased towards palliative care treatment decisions. Anchoring bias may therefore lead to a lack of consideration of alternative options when making clinical decisions [42].
Another parameter that may act as a catalyst to decision-making in patient care is emotional arousal. This emotional state may be the outcome of many stimuli such as end-of-life decisions, legal considerations, feedback of senior staff, or other. These stimuli may lead to a desire to refrain from taking a stand, and passively choose the default. In our case, this would be the traditional treatment focusing on rescuing the patient and preventing death without fully weighing the implications. Paradoxically, this actually becomes a position with real effect; it is called the “default bias” and “serves” the need to eliminate complex and/or emotional decisions [1].
In summary, clinical decision-making related to a terminally-ill patient is associated with high levels of emotion, stress, and discomfort. Under such conditions, the practitioner may automatically revert to anchoring and/or default biases and not consider all treatment options.
Availability, Representativeness and Framing Biases
Other potential cognitive biases that affect decision-making are availability, representativeness, and framing biases. People make decisions based on the constructions, perceptions or cognitive models of their world. We use our model to understand events and predict the future. A cognitive model is based on cues, schematic thinking, and classification of situations according to fixed frameworks, while prioritizing objective evidence over perception. In addition, many behaviors are based on habits and experiences at an unconsciousness level [49].
These biases might negatively influence the understanding of a situation by decreasing the ability to assess all possible aspects of a clinical situation [6]. When practitioners encounter a new situation, they assess the frequency of such situations by “scanning” their memory and searching for relevant cases. Memories of similar situations that involved increased emotions, unusual risks, fear or losses, are more easily recalled or more cognitively available and more likely to be used to assess the new situation. This is called ‘availability’ bias [11, 13, 14, 46, 70, 71]. For example, once a physician has been involved with a medical negligence case, that same physician may be unwilling to use the same treatment in cases with a similar diagnosis and prognosis despite its demonstrated success.
In addition, the current healthcare environment forces practitioners to constantly consider the negative legal implications and the opinions of senior staff when making medical decisions. These considerations lean towards the use of the traditional care decisions and compliance with availability biases. We assume that in situations that include end-of-life decisions, including patients with advanced dementia, all of the above may occur. Such biases also play a role when practitioners fear experiencing feelings of regret and guilt when deciding to forgo aggressive care and, as such, prefer the 'easy' choice of familiar, aggressive care. This is a deontological approach that focuses on the immediate consequences of decision-making without fully considering the repercussions of the decision [30].
People also tend to base their decisions on more frequent cases that are presented in a positive light, even if the current situation is not the same. This bias is called ‘representativeness’ [70]. Representativeness is a tendency to relate a situation to a certain category without taking into consideration the number of times this category is consistent with the specific situation. For example, a group of symptoms can be associated with two different diagnoses, one common and the other rare. Once clinicians have encountered the rare condition, they are more likely to diagnose the condition the next time they encounter these same symptoms. This conclusion is supported by objective evidence even though there are other objective and subjective aspects that are not taken into account [11, 46]. Once a situation is ascribed to a specific category, a label is attached. This label becomes the default and causes the practitioner to search for evidence to support the chosen diagnosis. For example, when treating people with advanced dementia, the same medical condition can lead a practitioner to interpret the condition as an acute state requiring intermediate intervention or as a situation requiring symptom control and palliative care.
Often this process leads to a premature conclusion and an early discontinuation of the scanning process, potentially missing co-pathology needed to assess the entire clinical picture [53]. Such biases can also lead to an instinctive or emotional response leading to a reduction of rational thinking and poorer decision-making [11, 46]. For example, a patient may present with a certain symptom. The practitioner will automatically tend to ascribe that symptom or set of symptoms to the most common cause and might overlook other underlying causes and aspects of the case. This tendency may result in decreasing the quality of care. This is often the case when patients with advanced dementia present with atypical symptoms and all diagnostic options must be considered.
Similar to representativeness bias, "framing bias" refers to the conceptual structure used to represent a situation. Framing bias may occur when the same argument or situation is presented in a positive or in a negative light [20]. People tend to prefer an option that is presented positively. For example, patients are more likely to choose a treatment option described as providing an 80% chance of survival as opposed to a 20% chance of mortality, even though both options express the same outcome [57]. For the purpose of our discussion, goals of care for a patient with advanced dementia may be described in positive or negative terms. When discussing goals of care, clinicians can present the option of full acute care treatment as either sustaining life (positive) or as continuing aggressive, futile treatment (negative). On the other hand, palliative care can be presented as either discontinuing active treatment (negative) or as increasing quality of life, decreasing suffering and discomfort (positive). The clinician's choice of terminology or framing of the situation may result from their personal beliefs, values, prior experience, perceived professional norms, and education all of which may unconsciously result in presenting goals of care consistent with their own preferences [57]. Evidence of this has been shown in studies reporting discrepancies between patient preferences and practitioners’ decisions regarding treatment and treatment goals, especially related to end-of-life care. In a study that surveyed 125 nephrologists to assess their attitudes towards death and their care of terminal patients, Rutekci et al. found that the more uncomfortable physicians were with dying patients, the more likely they were to initiate or continue life-prolonging treatments. Approximately 25% of the sample reported difficulty honoring and following advance directives when these directives were different from what the physician considered to be best care [60]. This study supports the argument that practitioner bias is more influential in care decisions than patient values [60].
A unique bias associated with patients with advanced dementia stems from the transparency of these patients in the eyes of caregivers due to the significant cognitive disabilities and the perception of the patient’s lack of personhood. This bias may result in inadequate consideration of the patient’s needs, values, and beliefs and may result in attributing less value to the lives of patients with advanced dementia by their healthcare providers or family members. Health practitioners may objectify people with dementia, and fail to uphold the patient’s human rights, impinging on the quality of care delivered [8]. Treating patients as lacking in personality or preferences nullifies their rights as a party in the decision-making process [36]. Kitwood, a prominent researcher in the field, argued that personhood should be conceptualized broadly [44], where in addition to the criteria of autonomy and rationality, relationships and moral status must be included. One attempt at addressing the issue of dementia being perceived as a negative stereotype is to change the term “dementia” to "neurocognitive disorder".
Moral Judgment in Decision-Making
Just as cognitive biases and heuristics impact on the type of decision, moral biases can impact moral judgment [43]. In this section, we will review the terms moral sensitivity and moral courage as forms of moral biases and show how they affect moral judgment and decision-making.
Moral Judgment and Cognitive Biases
A judgment is an opinion held or expressed after giving consideration to something [16, 31]. Moral judgments refer to judgments that have moral content and are used to evaluate situations and courses of action (Seven-Pillars Institute) [66]. Singer ties moral judgment to the two-system model of decision-making [66]. Moral judgments are made using one of two distinct mental processes that are characterized as either deontological, based on intuitive, default automatic emotional process, (system I); or utilitarian, based on conscious, controlled reasoning processes (system II) [16, 29, 66].
Theories of moral judgment address the impact of context and environment on the way the human mind works related to ethical decision-making [27, 52]. The issue is not whether one is deviating from objective standards, as there are no objective moral standards, but rather deviating from rational decision-making [33]. For example, a decision in favor of aggressive treatment that has no potential medical benefit for a patient at the end of life is conceivably an irrational, yet common, decision. Therefore, moral judgments are not only made on the basis of rational thought, but also on subjective perceptions and unconscious cognitive biases [33].
Previous research has shown that both deontological and utilitarian moral judgments can be manipulated through surrounding elements and components [16, 29, 66]. The multitude of demands and pressures practitioners face in healthcare settings, their cognitive loads, organizational hierarchical power, organizational culture, and perceived clinical norms create a dynamic multidimensional environment that can affect moral behavior and moral judgment [51]. People do not always act in accordance with the values they claim to espouse, because cognitive biases influence moral decisions. Inherent characteristics and values may be over-ridden when the impact of external influences is strong [51]. For example, a sense of belonging and organizational climate may have an impact on moral decisions [29]. A clinician might believe that palliative care is most appropriate for a specific patient, but might continue with aggressive care because the cultural norm, the opinion of senior staff and the work environment supports such care. Therefore, moral and ethical aspects may override default clinical decisions, depending on the practitioner, the working environment, and the specific clinical situation.
An ideal bioethical framework to guide decision-making related to goals of care would be based on ethical principles and evidence-based practice. Medical ethics is based on the principles of autonomy, beneficence, non-maleficence and justice. In practice, this framework may prompt conflicts within the health team, or between the healthcare team and the family/surrogates. For example, healthcare providers might prefer the principle of beneficence or non-maleficence over autonomy in such situations. Based on their medical expertise, they might decide to forgo non-beneficial treatment that might cause increased patient suffering and choose goals of care related to improving quality of life over extending life. On the other hand, family members might prefer the value of autonomy, namely their right to decide to continue with aggressive care [24].
Moral Sensitivity
Another aspect of clinical decision-making related to this patient population is moral sensitivity. Moral sensitivity is a subjective “sense” that bridges the gap between moral knowledge and actual behavior. Moral sensitivity may be defined as, “making decisions not by choosing to do this or that, but about being the kind of person who is alive to moral possibilities” [43]. Moral sensitivity defines how people perceive their situation and how they respond to it. Those possessing moral sensitivity are inclined to take the time and mental effort to consciously assess the ethical aspects of a decision. It is acquired slowly through repeated experiences and is based on intelligence and the capacity to be imaginative. Moral sensitivity is needed to remain open-minded [43].
Personal and contextual factors have a great impact on the formation of moral sensitivity, including affection, skill, responsibility, education and knowledge [61]. These domains are associated with culture, organizational climate, and professional experience [55]. A clinician with moral sensitivity expends mental effort in order to arrive at a decision perceived as morally/ethically beneficial and takes into consideration the patient's vulnerable situation, the moral/ethical implications of decisions made on the patient's behalf [25], and the long-term goals that may be in conflict with short term goals.
In our context, barriers to palliative care for patients with advanced dementia can be considered representativeness bias as a result of low moral sensitivity and not perceiving the patient's health state as terminal. These barriers include lack of knowledge, little exposure to and experience with this population, organizational support for certain therapies, institutional policy, and professional orientation [47]. A clinician might not even recognize that a moral/ethical dilemma exists when choosing treatment and may continue with the default traditional, aggressive treatment without considering other options. Increased levels of moral sensitivity are associated with a more in-depth evaluation of the situation, recognizing that there is a moral/ethical dilemma instead of continuing with the default. Decreased moral sensitivity may lead to decreased consideration of ethical issues in the busy professional lives of decision-makers [43].
Moral Courage
An additional moral aspect of clinical decision-making is moral courage. Moral courage is defined as the ability to act differently from patterns of traditional, conventional behavior [56]. Decision-makers should act or practice according to their moral or ethical principles. However, this is often not the case. For example, a new medical resident might prefer palliative care to curative care for their patients with advanced dementia. However, if the norm is to continue with “normal” care, then the resident would likely continue to prescribe tests and treatments, creating moral conflict and distress [12]. In order to avoid moral distress, the resident should display moral courage, which may result in personal opposition to group pressure. Such courage arises from internal forces including self-confidence and empathy and involves taking a stand and acting from a humane, pro-social, moral perspective, which has little or no direct personal benefit [22, 50, 56]. Moral courage is affected by organizational factors such as class, hierarchy, lack of organizational support, and fear of negative personal consequences, that in some cases may lead to avoidance and repression and induce moral/ethical dilemmas [22, 56].
Moral courage is also relevant when dealing with decision-making. Often patients and family members pressure clinicians to continue aggressive treatment. Many clinicians would continue with such therapy believing that it is in accordance with the value of patient autonomy to avoid medical paternalism. They might feel an obligation to follow patient preferences, even when doing so conflicts with their professional moral obligations [12]. The patient/family member may demand treatment that the practitioner finds inappropriate, leading to a psychological burden and moral distress, from a professional standpoint, and fear of potential litigation.
Moral courage refers to taking a position in opposition to the accepted norm. It might mean recommending palliative care to family members who insist on “doing everything”. Or, in contrast, when a patient's family/proxy underestimates the value and quality of the patient’s life due to the patient’s cognitive deficits. In this case, the family would perceive aggressive care as futile. This conclusion might be in conflict with that of a practitioner with more experience in treating patients with advanced dementia, who understands that quality of life might mean something different to patients in this state, and who might need moral courage to suggest an approach different from that of the family.
The Healthcare Provider as a Decision-Maker
After consideration of the complexity of the phenomena and the recognized biases that are important factors in the decision-making process, it is clear that one of the key determinants in the decision-making process is the healthcare provider who may, at least partially, account for the palliative care disparity in this patient population.
Characteristics of the healthcare provider that can affect decision-making are numerous. Professional aspects, including levels of knowledge and training, experience and previous exposure to patients with dementia, orientation and professional status [13, 14, 71] are associated with decision-making. Attitudes and perceptions towards longevity and quality of life [71], as well as adherence to policy and regulations [7] have also been investigated. In addition, decision-making is related to personal characteristics such as religiosity and morality [48, 71].
The health practitioner is the "agent of knowledge" while at the same time is professionally obligated to act as the representative and advocate of the patient, guiding the therapeutic approach, and influencing the choice of treatment [12, 72]. The practitioner's role also includes discussion of treatment options with patients and family members, and as such, have a significant impact upon treatment decisions. However, the final authority usually rests with the patient or the patient’s representatives (surrogate/proxy) [5, 40, 41, 75].
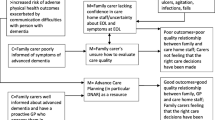
It should be noted that the preferences and attitudes of the family, in the case of advanced dementia, is greatly influenced by the quality and scope of the information provided by the medical staff, a factor that is strongly linked to goals of care, and correlated with the "aggressiveness" of the medical care provided [37, 41]. Evidence indicates a reduction in life-prolonging treatments when the patient's family is aware of and understands the issue of quality of life and prevention of suffering [73].
The interaction between patient, family member(s) and healthcare provider also impacts on clinical decision-making. While informal caregivers can promote the decision-making process, they may influence the practitioner in a way that leads to cognitive bias, including evoking feelings of a lack of confidence, a lack of clarity about the goals of care, and a fear of conflicts and legal concerns [4, 29, 52]. On the other hand, practitioners sometimes avoid their decision-making responsibility and delegate difficult treatment choices to the patient's surrogate [51]. When the situation is accompanied by practitioner uncertainty, fear of feelings of regret and guilt, and conflict avoidance, the practitioner will focus on the present, choosing the default treatment option, often neglecting the future [5, 17, 18, 32, 61, 64, 67, 68, 70, 72].
In conclusion, although in the case of the patient with advanced dementia the final decision on the goals of care and the treatment belongs to the family or another individual acting on behalf of the patient, the health practitioner has professional authority that can significantly influence and direct the treatment. Taking a stand in disagreement with that of the family in favor of the right to choose palliative or end-of-life care requires moral sensitivity and moral courage. This includes acceptance of the medical prognosis and advocacy for underutilized palliative care services, often not considered the norm for patients with advanced dementia [65].
Conclusions
There is an observed gap in the acute and chronic clinical settings between professional guidelines that recommend treatments to enhance quality of life/palliative care, and routine care that focuses on acute or life-prolonging therapies that often do not result in beneficial effects. Two aspects of clinical decision-making related to patients with advanced dementia that have rarely been investigated are the cognitive biases of practitioners and the moral aspects related to the decision-making process. Practitioners may benefit from a closer analysis of existing data regarding cognitive biases, moral aspects of medical decision-making, and non-clinical influences that affect the autonomy of the decision-maker. Such an analysis will potentially result in better clinical practice.
The “art of medicine” represents the integration of many different sources of knowledge in a clinical environment. This approach can also contribute to research related to the process of healthcare professional, ethical decision-making for advanced dementia. We recommend that investigations in this area of research be based on the “Two-System Model” since clinical decisions are often made via cognitive biases. We also suggest that investigations include moral variables as well as personal ones, from different disciplines, using several methodological approaches. This mixed methods approach may advance the existing professional literature and promote the quality of care given to this population.
References
Ariely, D. (2008). Predictably irrational: The hidden forces that shape our decisions. New York: Harper Collins Publihsers.
Avorn, J. (2018). The psychology of clinical decision making—Implications for medication use. The New England Journal of Medicine, 378(8), 689–691. https://doi.org/10.1056/NEJMp1714987.
Ayal, S., & Hochman, G. (2009). Ignorance or integration: The cognitive processes underlying choice behavior. Journal of Behavioral Decision Making, 22(4), 455–474. https://doi.org/10.1002/bdm.642.
Bartley, M. M., Suarez, L., Shafi, R. M. A., Baruth, J. M., Benarroch, A. J. M., & Lapid, M. I. (2018). Dementia care at end of life: Current approaches. Current Psychiatry Report, 20(7), 50. https://doi.org/10.1007/s11920-018-0915-x.
Birch, D., & Draper, J. (2008). A critical literature review exploring the challenges of delivering effective palliative care to older people with dementia. Journal of Clinical Nursing, 17(9), 1144–1163. https://doi.org/10.1111/j.1365-2702.2007.02220.x.
Blumenthal-Barby, J. S. (2016). Biases and heuristics in decision making and their impact on autonomy. The American Journal of Bioethics, 16(5), 5–15. https://doi.org/10.1080/15265161.2016.1159750.
Bornstein, B. H., & Emler, A. C. (2001). Rationality in medical decision making: A review of the literature on doctors’ decision-making biases. Journal of the Evaluation of Clinical Practice, 7(2), 97–107. https://doi.org/10.1046/j.1365-2753.2001.00284.x.
Bosco, A., Schneider, J., Coleston-Shields, D. M., & Orrell, M. (2019). Dementia care model: Promoting personhood through co-production. Archives of Gerontology and Geriatrics, 81, 59–73. https://doi.org/10.1016/j.archger.2018.11.003.
Brazil, K., Carter, G., Galway, K., Watson, M., & van der Steen, J. T. (2015). General practitioners perceptions on advance care planning for patients living with dementia. BMC Palliative Care, 14, 14. https://doi.org/10.1186/s12904-015-0019-x.
Brooks, M. (2020). End-of-life wishes may not be honored in the hospital. Medscape. Feb 21, 2020. Retrieved December 17, 2020, from https://www.medscape.com/viewarticle/925422.
Calabria, M. A. (2014). Behavioral economics and fed policymaking. Cato Journal, 36(3), 573–587. Retrieved November 8, 2019, from https://www.cato.org/sites/cato.org/files/serials/files/cato-journal/2016/9/cj-v36n3-6.pdf.
Cave, E. (2019). Selecting treatment options and choosing between them: Delineating patient and professional autonomy in shared decision-making. Health Care Analysis, 28(1), 4–24. https://doi.org/10.1007/s10728-019-00384-8.
Chibnall, J. T., Bennett, M. L., Videen, S. D., Duckro, P. N., & Miller, D. K. (2004). Identifying barriers to psychosocial spiritual care at the end of life: A physician group study. American Journal of Hospital Palliative Care, 21(6), 419–426. https://doi.org/10.1177/104990910402100607.
Christakis, N. A., & Asch, D. A. (1995). Physician characteristics associated with decisions to withdraw life support. American Journal of Public Health, 85(3), 367–372. https://doi.org/10.2105/ajph.85.3.367.
Croskerry, P. (2013). From mindless to mindful practice — cognitive bias and clinical decision making. The New England Journal of Medicine, 368(26), 2445–2448. https://doi.org/10.1056/NEJMp1303712.
Cushman, F., Young, L., & Greene, J. D. (2010). Multi-system moral psychology. In J. M. Doris (Ed.), The moral psychology handbook (pp. 47–71). Oxford, U.K.: Oxford University Press.
Davies, N., Maio, L., Vedavanam, K., Manthorpe, J., Vernooij-Dassen, M., Iliffe, S., & IMPACT research team. (2014). Barriers to the provision of high-quality palliative care for people with dementia in England: A qualitative study of professionals’ experiences. Health and Social Care in the Community, 22(4), 386–394. https://doi.org/10.1111/hsc.12094.
Davies, N., Manthorpe, J., Sampson, E. L., Lamahewa, K., Wilcock, J., Mathew, R., & Iliffe, S. (2018). Guiding practitioners through end of life care for people with dementia: The use of heuristics. PLoS ONE, 13(11), e0206422. https://doi.org/10.1371/journal.pone.0206422.
Dening, K. H., Greenish, W., Jones, L., Mandal, U., & Sampson, E. L. (2012). Barriers to providing end-of-life care for people with dementia: A whole-system qualitative study. British Medical Journal: Supportive and Palliative Care, 2(2), 103–107. https://doi.org/10.1136/bmjspcare-2011-000178.
Druchman, J. (2001). Evaluating framing effects. Journal of Economic Psychology, 22(1), 96–101. https://www.sciencedirect.com/science/article/abs/pii/S0167487000000325?via%3Dihub.
Ehrlinger, J., Readinger, W. O., & Kim, B. (2015). Decision-making and cognitive biases. In H. S. Friedman (Ed.), Encyclopedia of mental health (2nd ed., pp. 5–12). Philadelphia: Elsevier.
Epstein, E. G., & Hamric, A. B. (2009). Moral distress, moral residue, and the crescendo effect. Journal of Clinical Ethics, 20(4), 330–342.
Erel, M., Marcus, E. L., & Dekeyser-Ganz, F. (2017). Barriers to palliative care for advanced dementia: A scoping review. Annals of Palliative Care, 6(4), 365–379. https://doi.org/10.21037/apm.2017.06.13.
Forte, D. N., Kawai, F., & Cohen, C. (2018). A bioethical framework to guide the decision-making process in the care of seriously ill patients. BMC Medical Ethics, 19(1), 78. https://doi.org/10.1186/s12910-018-0317-y.
Gholami, K., & Tirri, K. (2012). The cultural dependence of the Ethical Sensitivity Scale Questionnaire: The case of Iranian Kurdish teachers. Education Research International, 2012, Article ID 387027. https://doi.org/10.1155/2012/387027.
Di Giulio, P., Toscani, F., Villani, D., Brunelli, C., Gentile, S., & Spadin, P. (2008). Dying with advanced dementia in long-term care geriatric institutions: A retrospective study. Journal of Palliative Care, 11(7), 1023–1028. https://doi.org/10.1089/jpm.2008.0020.
Goel, V., & Dolan, R. J. (2003). Explaining modulation of reasoning by belief. Cognition, 87(1), B11-22. https://doi.org/10.1016/s0010-0277(02)00185-3.
Golan, O., & Marcus, E-L. (2012). Should we provide life-sustaining treatments to patients with permanent loss of cognitive capacities?" Rambam Maimonides Medical Journal. 3(3), e0018. https://doi.org/10.5041/RMMJ.10081.
Greene, J. D. (2014). Beyond point-and-shoot morality: Why cognitive (neuro)science matters for ethics. Ethics, 124(4), 695–726. https://psychology.fas.harvard.edu/files/psych/files/beyond-point-and-shoot-morality.pdf.
Greene, J. D. (2007). The secret joke of Kant’s soul. In W. Sinnott-Armstrong (Ed.), Moral psychology. The neuroscience of morality: Emotion, brain disorders, and development (Vol. 3, pp. 35–80). Cambridge, MA, USA: MIT Press.
Greene, J. D., Nystrom, L. E., Engell, A. D., Darley, J. M., & Cohen, J. D. (2004). The neural bases of cognitive conflict and control in moral judgment. Neuron, 44(2), 389–400. https://doi.org/10.1016/j.neuron.2004.09.027.
Hajjaj, F. M., Salek, M. S., Basra, M. K., & Finlay, A. Y. (2010). Non-clinical influences on clinical decision-making: A major challenge to evidence-based practice. Journal of the Royal Society of Social Medicine, 103(5), 178–187. https://doi.org/10.1258/jrsm.2010.100104.
Herman, M. (2014). Moral heuristics and biases. Journal of Cognition and Neuroethics, 2(1), 127–142. http://jcn.cognethic.org/jcnv2i1_Herman.pdf.
Heschel, A. J. (1966). The patient as a person. In A. J. Heschel (Ed.), The insecurity of freedom: Essays on human existence (pp. 24–38). New York: Farrar, Strauss & Girox.
Heyd, D. (1995). The medicalization of health: Plato's warning. Revue Internationale de Philosophie, 49(19), 375–393. Retrieved November 8, 2019, from https://www.jstor.org/stable/23954802?seq=1#page_scan_tab_contents.
Higgs, P., & Gilleard, C. (2016). Interrogating personhood and dementia. Aging and Mental Health, 20(8), 773–780. https://doi.org/10.1080/13607863.2015.1118012.
Hill, E. M. (2014). Investigating barriers to access and delivery of palliative care for persons with dementia in London Ontario. Electronic dissertation repository.2455 Retrieved December 17, 2020, from https://ir.lib.uwo.ca/etd/2455?utm_source=ir.lib.uwo.ca%2Fetd%2F2455&utm_medium=PDF&utm_campaign=PDFCoverPages.
Hintea, C. E., Mora, C., & Ţiclău, T. (2009). Leadership and management in the health care system: Leadership perception in Cluj County Children’s Hospital. Transylvanian Review of Administration Science, 27(27E), 89–104. Retrieved November 8, 2019, from https://www.researchgate.net/publication/228437679_Leadership_and_Management_in_the_Health_Care_System_Leadership_Perception_in_Cluj_County_Children's_Hospital.
Hughes, J. C., Volicer, L., & van der Steen, J. T. (2018). Complexity and gaps: The high-hanging fruit of dementia and palliative care research. Palliative Medicine, 32(3), 591–593. https://doi.org/10.1177/0269216318755280.
Jacobs, L. G., Bonuck, K., & Burton, W. (2002). Can “palliative care reports” improve end-of-life care for hospitalized patients? Journal of Pain and Symptom Management, 24(3), 299–311. https://doi.org/10.1016/s0885-3924(02)00492-x.
Jethwa, K. D., & Onalaja, O. (2015). Advanced care planning and palliative medicine in advanced dementia: A literature review. British Journal of Psychiatry Bulletin, 39(2), 74–78. https://doi.org/10.1192/pb.114.046896.
Kahneman, D. (2011). Thinking fast and slow. New York: Farrar Straus and Giroux.
Kekes, J. (1984). Moral sensitivity. Philosophy, 59(227), 3–19.
Kitwood, D., & Bredin, K. (1992). Towards a theory of dementia care: Personhood and well-being. Aging and Society, 12(3), 269–287. https://doi.org/10.1017/so144686x0000502x.
Kozlowski, D., Hutchinson, M., Hurley, J., Rowley, J., & Sutherland, J. (2017). The role of emotion in clinical decision making: An integrative literature review. BMC: Medical Education, 17(1). 255, https://doi.org/10.1186/s12909-017-1089-7.
Lockton, D. (2012). Cognitive biases, heuristics, and decision-making in design for behaviour change. Working paper. SSRN Electronic Journal. August 5. Retrieved December 17, 2020, from https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2124557.
Lützén, K., Blom, T., Ewalds-Kvist, B., & Winch, S. (2010). Moral stress, moral climate and moral sensitivity among psychiatric professionals. Nursing Ethics, 17(2), 213–224. https://doi.org/10.1177/0969733009351951.
Marcus, E-L., Golan, O., & Goodman, D. (2016). Ethical issues related to end of life treatment in patients with advanced dementia - the case of artificial nutrition and hydration. Diametros, 50, 118–137. Retrieved November 8, 2019, from https://www.diametros.iphils.uj.edu.pl/diametros/article/view/982.
Marom, S. (2015). Science, psychoanalysis, and the brain: Space for dialogue. New York: Cambridge Univ Press. Retrieved November 8, 2019, from https://marom.net.technion.ac.il/files/2016/07/9781107101180_CUPExcerpt.pdf.
Martinez, W., Bell, S. K., Etchegaray, J. M., & Lehmann, L. S. (2016). Measuring moral courage for interns and residents: Scale cevelopment and initial psychometrics. Academic Medicine, 91(10), 1431–1438. https://doi.org/10.1097/ACM.0000000000001288.
Merritt, A. C., Effron, D. A., & Monin, B. (2010). Moral self-licensing: When being good frees us to be bad. Social and Personality Psychology Compass, 4/5, 344–357. Retrieved February 17, 2020, from http://www.ask-force.org/web/Fundamentalists/Merritt-Moral-Self-Licensing-2010.pdf.
Milliken, A. (2018). Refining moral agency: Insights from moral psychology and moral philosophy. Nursing Philosophy 19(1), e12185. https://doi.org/10.1111/nup.12185.
Mitchell, S. L. (2015). CLINICAL PRACTICE. Advanced dementia. The New England Journal of Medicine, 372(26), 2533–2540. https://doi.org/10.1056/NEJMcp1412652.
Mitchell, S. L., Kiely, D. K., & Hamel, M. B. (2004). Dying with advanced dementia in the nursing home. Archives of Internal Medicine, 164(3), 321–326. https://doi.org/10.1001/archinte.164.3.321.
Nora, C. R. D., Zoboli, E., & Vieira, M. (2017). Moral sensitivity of nurses assessed through scoping review. Cognitare Enfermagem Journal, 22(2), e47162. Retrieved 8 November, 2019, from https://revistas.ufpr.br/cogitare/article/view/47162.
Osswald, S., Greitemeyer, G., Fischer, P., & Frey, D. (2019). What is moral courage? Definition, explication, and classification of a complex construct. In C. L. S. Pury, & S. J. Lopez (Eds.), The psychology of courage: Modern research on an ancient virtue (pp. 149–164). American Psychological Association. https://doi.org/10.1037/12168-008.
Ozdemir, S., & Finkelstein, E. A. (2018). Cognitive bias: The downside of shared decision making. JCO Clinical Cancer Informatics, 2, 1–10. https://doi.org/10.1200/cci.18.00011.
Rimal, R. N., & Real, K. (2006). Understanding the influence of perceived norms on behaviors. Communication Theory, 13(2), 184–203. https://doi.org/10.1111/j.1468-2885.2003.tb00288.x.
Riskin, A., Erez, A., Foulk, T. A., Kugelman, A., Gover, A., Shoris, I., Riskin, K. S., & Bamberger, P. A. (2015). The impact of rudeness on medical team performance: A randomized trial. Pediatrics, 136(3), 487–495. https://doi.org/10.1542/peds.2015-1385.
Rutecki, G. W., Cugino, A., Jarjoura, D., Kilner, J. F., & Whittier, F. C. (1997). Nephrologists’ subjective attitudes towards end-of-life issues and the conduct of terminal care. Clinical Nephrology, 48(3), 173–180.
Ryan, T., Gardiner, C., Bellamy, G., Gott, M., & Ingleton, C. (2012). Barriers and facilitators to the receipt of palliative care for people with dementia: The views of medical and nursing staff. Palliative Medicine, 26(7), 879–886. https://doi.org/10.1177/0269216311423443.
Sachs, G. A., Shega, J. W., & Cox-Hayley, D. (2004). Barriers to excellent end-of-life care for patients with dementia. Journal of General Internal Medicine, 19(10), 1057–1063. https://doi.org/10.1111/j.1525-1497.2004.30329.x.
Salvatore, D., Numerato, D., & Fattore, G. (2018). Physicians' professional autonomy and their organizational identification with their hospital. BMC: Health Services Research, 18(1), 775, https://doi.org/10.1186/s12913-018-3582-z.
Schreiner, A. S., Hara, N., Terakado, T., & Ikegami, N. (2004). Attitudes towards end-of-life care in a geriatric hospital in Japan. International Journal of Palliative Nursing, 10(4), 185–193; discussion 193. https://doi.org/10.12968/ijpn.2004.10.4.12796.
Shaulov, A., Frankel, M., Rubinow, A., Maaravi, Y., & Brezis, M. (2015). Preparedness for end of life - a survey of Jerusalem District nursing homes. Journal of the American Geriatrics Society, 63(10), 2114–2119. https://doi.org/10.1111/jgs.13645.
Singer, P. (2005). Ethics and intuitions. The Journal of Ethics, 9(3/4), 331–352. https://doi.org/10.1007/s10892-005-3508-y.
Sulmasy, D. P., & Snyder, L. (2010). Substituted interests and best judgments: An integrated model of surrogate decision making. Journal of the American Medical Association, 304(17), 1946–1947. https://doi.org/10.1001/jama.2010.1595.
Thuné-Boyle, I. C. V., Sampson, E. L., Jones, L., King, M., Lee, D. R., & Blanchard, M. R. (2010). Challenges to improving end of life care of people with advanced dementia in the UK. Dementia, 9(2), 259–284. https://doi.org/10.1177/1471301209354026.
Toye, C., Lester, L., Popescu, A., McInerney, F., Andrews, S., & Robinson, A. L. (2014). Dementia Knowledge Assessment Tool Version Two: Development of a tool to inform preparation for care planning and delivery in families and care staff. Dementia (London), 13(2), 248–256. https://doi.org/10.1177/1471301212471960.
Trimble, M., & Hamilton, P. (2016). The thinking doctor: Clinical decision making in contemporary medicine. Clinical Medicine (London), 16(4), 343–346. https://doi.org/10.7861/clinmedicine.16-4-343.
Vejlgaard, T., & Addington-Hall, J. M. (2005). Attitudes of Danish doctors and nurses to palliative and terminal care. Palliative Medicine, 19(2), 119–127. https://doi.org/10.1191/0269216305pm988oa.
De Vleminck, A., Pardon, K., Beernaert, K., Deschepper, R., Houttekier, D., Van Audenhove, C., Deliens, L., & Vander Stichele, R. (2014). Barriers to advance care planning in cancer, heart failure and dementia patients: A focus group study on general practitioners’ views and experiences. PLoS ONE, 9(1), e84905. https://doi.org/10.1371/journal.pone.0084905.
Volicer, L. (2017). The development of palliative care for dementia. Annals of Palliative Medicine, 6(4):302–305. https://doi.org/10.21037/apm.2017.06.12.
Weinstein, I. (2003). Don't believe everything you think: Cognitive bias in legal decision making. Clinical Law Review, 9, 783–834. Retrieved November 8, 2019, from https://ir.lawnet.fordham.edu/cgi/viewcontent.cgi?article=1421&context=faculty_scholarship.
Wenger, N. S., & Carmel, S. (2004). Physicians religiosity and end-of-life care attitudes and behaviors. Mount Sinai Journal of Medicine, 71(5), 335–343.
Wolfs, C. A., de Vugt, M. E., Verkaaik, M., Haufe, M., Verkade, P. J., Verhey, F. R., & Stevens, F. (2012). Rational decision-making about treatment and care in dementia: A contradiction in terms? Patient Education and Counseling, 87(1), 43–48. https://doi.org/10.1016/j.pec.2011.07.023.
Wollaston, S., Cooper, R., George, A., Jenrick, R., Keeley, B., Leslie, C., Morris, J. M., Percy, A., Sharma, V., & Tredinnick, D., & Vaz V. (2015). End of life care. London: Health Committee, House of Commons of the United Kingdom. Retrieved November 9, 2019, from https://publications.parliament.uk/pa/cm201415/cmselect/cmhealth/805/805.pdf.
Funding
No funding was received to assist with the preparation of this manuscript. This research did not receive any specific support from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Meira Erel and Esther‑Lee Marcus provided equal contribution as first authors.
Rights and permissions
About this article

Cite this article
Erel, M., Marcus, EL. & Dekeyser-Ganz, F. Practitioner Bias as an Explanation for Low Rates of Palliative Care Among Patients with Advanced Dementia. Health Care Anal 30, 57–72 (2022). https://doi.org/10.1007/s10728-021-00429-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10728-021-00429-x