
Abstract
Obesity is a complex global health problem because it is a risk factor for multiple chronic pathologies such as cardiovascular, endocrine, metabolic, and neoplastic diseases. It is considered a multicausal disease, and one of the determining factors is nutritional imbalances, which include high-fat diets. In this paper, we use the zebrafish model to assess the impact of overfeeding and a high-fat diet in somatic and cardiac parameters in young and adult zebrafish. The results show that fish receiving a high-fat diet showed greater weight gain compared to fish receiving a standard fat diet. Additionally, changes in the heart, including increases in size, a change in the triangular shape of the ventricle to a globular shape, and an increase in the thickness of the trabeculae of the spongy myocardium were observed. These changes could be indicators of cardiovascular overload. The results show that there is a direct relationship between the intake of a high-fat diet and obesity, which in turn can induce cardiac changes, supporting the hypothesis of the relationship between high-fat diets and cardiovascular risk factors. Given the genetic similarity between zebrafish and humans, these results could be extrapolated to human beings, and the findings similarly highlight the importance of incorporating a balanced diet from the early life stages to reduce the risk of cardiovascular disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is an epidemic health problem in the world, and it is currently one of the most important risk factors for the development of several chronic diseases such as hypertension, heart failure, liver disease, type 2 diabetes mellitus, and some cancers (Visscher and Seidell 2001; Frankel 2003; Bender et al. 2006; Guh et al. 2009). Although obesity is a chronic disease that occurs predominantly in adults, childhood obesity has increased in recent decades at an alarming rate and is now considered a worldwide epidemic (Lobstein et al. 2004; Cali and Caprio 2008; Xu and Xue 2016). The exaggerated increase in adipose tissue during childhood can lead to health problems such as glucose intolerance, hypertension, dyslipidemia, fatty liver disease, and metabolic syndrome (Weiss et al. 2004; Boney et al. 2005). Similarly, childhood overweight and obesity may represent a risk factor for developing various chronic diseases in adulthood that can be extremely difficult to manage and generate enormous costs for the National Health Systems (Dietz 1998; Rössner 1998; Flint and Rimm 2006). Obesity has many causes, and one of the contributory factors is an unbalanced diet, particularly a high-fat diet (HFD), which leads to a positive energy imbalance between caloric intake and energy expenditure. The extra calories ingested via the diet lead to storage of the excess nutrients within fat cells, where they accumulate it as triglycerides or neutral lipids. This phenomenon favors the development of overweight and obesity. Basic biomedical research employing animal models of obesity, clinical, and epidemiological studies shows a direct link between fat intake and obesity (Boozer et al. 1995; West and York 1998; Bray et al. 2004). Although the zebrafish model has frequently been used in basic biomedical research due to its numerous advantages (Lawrence 2007), it has only rarely been used for obesity and diet-related studies. In 2010, a protocol was reported by Oka et al. to establish a model of diet-induced obesity (DIO) in adult zebrafish, and in 2011, a test to evaluate obesity in larvae was proposed; these are key tools for the study of this disease in this model (Oka et al. 2010; Tingaud-Sequeira et al. 2011). Another study provided information related to the normal distribution of white adipose tissue in adult zebrafish (Imrie and Sadler 2010). More recently, several studies related to diet and various aspects of development and reproduction in zebrafish have been published (Nekoubin et al. 2013; Leibold and Hammerschmidt 2015). The development and structure of the zebrafish heart with its four compartments (one venous sinus, one atrium, one ventricle, and one arterial bulb) have been reported (Bakkers 2011), although there are no reports regarding the relationship between diet, obesity, and changes in cardiosomatic parameters in the zebrafish model. The aim of this study was to determine whether chronic overfeeding and HFD intake modify cardiosomatic parameters in young and adult zebrafish and to evaluate the impact on cardiac structures. The data obtained here can be used as reference parameters in future studies related to obesity and cardiovascular disease.
Materials and methods
This study was conducted using wild-type zebrafish (longfin zebra danio reg); specimens were obtained from local suppliers. The fish were kept in a static system in aquariums under constant aeration, with daily replacement of 20% of the water and cycles of light/darkness of 14:10. The temperature and pH of the water were held constant at 25 °C and 7.4, respectively. Uneaten feed and waste were removed daily to avoid contamination. Goodwin et al. (2016) have shown that these strategies maintain the water quality parameters closer to the acceptable standards. The protocol for zebrafish care was approved by the Committee of Research and Ethics of the Faculty of Medicine and the IACUC of the Pontificia Universidad Javeriana. Forty-four specimens were used, complying with the principle of the three Rs, which encourages minimizing the number of samples and optimizing their use.
Diet
The feed used for all experiments was a form of commercial flake tropical fish food, Tetramin® (Tetra, Inc., Blacksburg, VA, USA), having the following defined composition: 47% protein, 10% lipids, fiber 3%, and 6% moisture. Initially, the amount of food required daily was determined by a test in which decreasing total doses of food (1, 0.8, 0.5, 0.3, and 0.15 g) were administered to groups of ten adult fish (aged 6 months, average weight 0.9462 ± 0.1318 g). The daily food required was defined as the quantity in which no residues were found at the bottom of the aquarium 24 h after administration. The total dose was set at 0.15 g/day for ten fish. Two trials were conducted at this dose; in the first test, this dose was administered to a group of young fish (3 months old), and a second trial was conducted with adult fish, where the amount of food administered daily was doubled (6 months old; 0.3 g/day per group). In both cases, the effect of enriching the diet with crude vegetable oil was compared.
First trial
For the first trial, 16 young zebrafish (90 days post-fertilization) were separated into two randomly selected groups (40% males and 60% females in each group). The first group received the normal diet for tropical commercial fish 0.15 g/day group (standard fat diet: SFD1). This amount guaranteed continuous food for 24 h. The second group received a mixture of normal diet plus crude vegetable oil: 0.15 + 0.04 g, corresponding to 26% additional weight (high-fat diet: HFD1). Periodic monitoring was performed for 491 days in total, including periodic measurements of weight and standard length.
Second trial
For the second trial, 20 adult specimens (6 months old) were selected and separated into two groups at random (40% males and 60% females in each group). The first group received twice the food given in the first test 0.3 g/day (SFD2), and the second group received a mixture of food and crude vegetable oil: 0.3 + 0.08 g, corresponding to 26% of additional weight (HFD2). Feeding and monitoring, including periodic measurements of weight and standard length, continued for 258 days.
In both trials, daily cleaning of the aquariums was performed, consisting of vacuuming residue from the bottoms of the aquariums in order to prevent the accumulation of food and contamination.
Anesthesia
For handling and performing measurements, the fish were anesthetized using a 0.6-mM solution of MS-222 (tricaine ethyl-3 aminobenzoate methanesulfonate, Sigma-Aldrich, St. Louis, MO, USA). At the end of each trial, euthanasia was performed using a 6-mM MS-222 solution.
Measurements
In this study, direct and indirect measurements were obtained. Direct basic measurements or the primary parameters, including the standard length and weight of each specimen, were performed during the monitoring period (Figs. 1a and 2), and weight and dimensions of the isolated heart or dimensions of the histological sections of the heart images were performed at the end of the trials (Fig. 1b–c). Indirect measurements or secondary parameters included body weight gain (BWG), daily growth rate (DGR), specific growth rate (SGR), feed conversion ratio (FCR), body mass index (BMI), condition factor (factor K), standard length/weight ratio (SL/W), and the cardiosomatic index (CSI). The weight and standard length were measured every 30 to 45 days to reduce the frequency of handling and to reduce stress, which can affect the development of the samples. In the first trial, 50% of the group was followed up for 129 days; at which time, they were sacrificed to evaluate the hearts. The remaining 50% were followed for 491 days; at which time, stabilization in the measurements of standard length and weight was observed. In the second trial, zebrafish groups were followed for 258 days in 100% of the specimens. In both trials, measurements of weight and standard length were performed with the fish under general anesthesia. To measure body weight, a Sartorius analytical balance (Sartorius Mechatronics T&H GmbH, Hamburg, Germany) was used. For the standard length measurement, images of each zebrafish were taken using a conventional camera ES65, 10.2 MP (Samsung Electronics, Seoul, Korea). Using these images and the free software ImageJ, the standard length of each fish was measured from the snout to the caudal peduncle (Figs. 1a and 2).

Measurements in zebrafish Danio rerio. a Adult D. rerio and method for measuring size. b Isolated D. rerio heart and measuring axes. c D. rerio heart, histological section, and measured parameters. AB arterial bulb, V ventricle, r1 major axis, r2 minor axis, α1, α2, α3 ventricular angles, CM compact myocardium, SM spongy myocardium (dotted line). In a, the bottom-left line represents 1 cm. In b and c, the lower-left line represents 0.5 mm

Control and experimental groups. a D. rerio receiving SFD at the beginning and b at the end of the trial. c D. rerio receiving HFD at the beginning and d at the end of the trial. No significant differences were found in size, but there were significant differences in weight. The bottom-left line represents 1 cm
At the end of the trials, the fish were sacrificed with an overdose of MS-222 solution, and they were then fixed in 4% paraformaldehyde for 24 h to ensure the integrity of the various structures of the heart during dissection.
Dissection and histology
Initially, the weight of each specimen, which serves as a reference for calculating the CSI, was registered and then the heart dissection was performed using the procedure from our previous reports (Vargas and Vásquez 2016). Briefly, a ventral incision to expose the viscera was performed for organ removal. Next, the abdominal walls were retracted with insect pins to visualize, identify, and extract the inner organs: gonads, stomach, intestine, liver, and heart. Once the heart was extracted, we proceeded to take the weight of the isolated organ. Then, images of the isolated heart were taken using a stereo microscope (XTD-217, Hinotek Ningbo Technology Co., Ltd., Zhejiang, China) and a 0.5-megapixel video camera (S3CMOS, Touptek Photonics, Hangzhou, China). The major axis (r1) and the minor axis (r2) of the isolated heart were measured on these images using the free software ImageJ (Fig. 1b). The hearts isolated from fish were fixed with 4% paraformaldehyde for 24 h, and then the histological procedures, including dehydration in an ascending ethanol series and paraffin embedding, were completed to obtain a final thickness of 20–50 μm sections. These sections were stained with hematoxylin-eosin (Fig. 1c). The processing of the samples was performed in the Department of Pathology, Faculty of Veterinary Medicine of the Universidad Nacional de Colombia. From these sections, ×4 and ×10 images were taken using a conventional camera (Optikam 2 Mp, Optika SRL, Ponteranica, BG, Italy) coupled with a light microscope (Accu-Scope® EXC-350, Accu-Scope Inc., Commack, NY, USA). On the images obtained, measurements of the ventricles and myocardium were made using ImageJ software (Fig. 1c).
In addition, a group of eight adult zebrafish was sacrificed at the end of the second trial. The zebrafish in this control group were the same age as those in the study group and were maintained under the same conditions and with the same care, with the exception that they had no dietary restrictions. As in the active groups, the hearts were dissected and the same histological procedures were performed, which allowed for comparisons among the samples collected from the SFD2, HFD2, and control groups.
Calculations and measurements
The calculations that were used, which have been validated in other studies, were as follows (Kowalska et al. 2012; Gonzales and Law 2013; Nekoubin et al. 2013; Vargas and Vásquez 2016):
Statistical analysis
Primary measurements were analyzed using basic descriptive statistics, including averages and standard deviations. A comparison between the group fed the normal fat (SFD) diet and the group that was administered the HFD was performed on each of the trials, using Student’s t test, 95% confidence intervals, and statistical significance at p < 0.05.
Results
Feeding
The amount of daily diet determined for zebrafish was 15 mg/g of body weight (bw)/day, which is close to that reported for other ornamental fish of similar size, such as neon tetra 3.8 mg/g bw/day; goldfish 25.79 mg/g bw/day; or leopard danio 7.2 mg/g bw/day (Pannevis and Earle 1994; Velasco-Santamaría and Corredor-Santamaría 2011). Similarly, it coincides with the diet reported by other authors such as Meguro and colleagues, who administered 160 mg/day of food divided into two portions to groups of eight zebrafish (Meguro et al. 2015). In the first trial of our study, the initial dose of feed was ten (SFD1) or 15 times (HFD1) higher due to the age and weight of the specimens (150 mg/day is equivalent to 197 mg/g fish/day; Fig. 3e and f). This dose was maintained throughout the first trial, which meant that over time and simultaneously with the specimen’s growth, the amount of food decreased proportionally to the weight gained, and by the end, both populations received similar quantities of food (<30 mg/g bw/day) with different compositions in terms of fat content (Fig. 3e). In the second trial, the amount of food provided was higher in the HFD2 group initially, but by the end, both populations received equivalent amounts of food (>20 mg/g bw/day) with different compositions (Fig. 3f).

Weight and length average of the control (SFD, solid line) and experimental groups (HFD, dashed line). a The average weight in trial 1. It is noted that in trial 1, from 3 months to the end, the increase in weight was higher in the HFD1 group. b Weight average in trial 2. It is noted that from the first month, weight increases in greater proportion in the HFD2 group. c Length average trial 1. d Length average trial 2. e Quantity of daily food administered in trial 1. f Quantity of daily food administered in trial 2. In both trials, food administered (grams of food per 1 g of body weight, g/g BW/day) gradually decreased
In both trials, unconsumed residual food (not quantified) was observed at 24 h, especially in the initial phases of both trials. In the SDF groups, a smaller amount of residual food and greater amount of detritus was observed. In the HFD groups, more unconsumed food was observed and less detritus. These observations suggest that intake is likely regulated similarly to other species, and it is possible that, despite the availability of food, hyperphagia did not develop (Poppitt and Prentice 1996). On the other hand, the lower intake in the HFD groups could be explained by the excess of calories due to the extra fat in the diet and fat-induced changes in gastric emptying and intestinal transit (Little et al. 2007).
Initial somatic parameters
In the first trial, weights and standard lengths between the SFD1 and HFD1 groups at the beginning of the experiment showed no significant difference (0.095 ± 0.017 vs. 0.077 ± 0.031 g, p < 0.05, n = 8; 1.63 ± 0.16 cm vs. 1.73 ± 0.13 cm, p > 0.05, n = 8; Fig. 3a and c). Additionally, no statistically significant differences in BMI, factor K, or the H/W ratio were observed (Fig. 4a, c, and e). Similar results were found in the initial measurement of the second trial (Figs. 3b and d and 4b, d, and f).

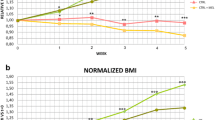
Secondary parameters trial 1 (left column) and trial 2 (right column). a Body mass index trial 1. b Body mass index trial 2. c Factor K trial 1. d Factor K trial 2. e Length/weight (L/W) ratio trial 1. f L/W ratio trial 2. g Cardiosomatic index trial 1. h Cardiosomatic index trial 2. SFD standard fat diet, HFD high-fat diet. Each bar represents the average ± SD. Asterisk represents a significant difference
Final somatic parameters
In the first trial, weights and standard lengths taken at 129 days showed significant differences only in terms of weight but not in size (0.428 ± 0.147 vs. 0.706 ± 0.172 g, p < 0.05, n = 8; 3.01 ± 0.32 cm vs. 3.32 ± 0.24 cm, p > 0.05, n = 8). No statistically significant differences in BMI, factor K, CSI, or the SL/W ratio factor were observed (Fig. 4a, c, and e). Primary parameters registered at the end of the trial (491 days) showed statistically significant differences only in weight (Fig. 3a and c). In the secondary parameters, statistically significant differences in BMI, CSI, and factor K were observed (Fig. 4a, c, and g).
In the second trial, significant differences were observed in the primary parameters, specifically in the weight data taken at 258 days (Fig. 3b and d). In the secondary parameters, it was observed that the BMI for the HFD2 group was greater than 0.08 g/cm2, indicating obesity, but no significant differences were observed in the SFD2 group, nor were there significant differences in the other parameters (Fig. 4b, c, f, and g).
Additionally, at the end of both trials, differences were observed between the SFD and HFD groups in BWG, DGR, SGR, and FCR (Table 1).
Measurements and cardiac structure
Measurements were made both in the isolated organs (Fig. 1b) and in histologic sections (Fig. 1c) of the different groups.
Isolated organ
The main measures of the isolated organ included a major axis, r1 and a minor axis, r2 (Pombo et al. 2012). In the first trial, an increase in both r1 and r2 was observed in the HFD1 group. This outcome was similar to the observed change from triangulated to globular shape in the histological sections (Fig. 5c and g). In the second trial, an increase in r1 and r2 in the HFD2 group was also observed.

Histology of the D. rerio heart in trial 1. Feeding and monitoring were performed for 491 days; 50% of the group was followed up for 129 days, at which time they were sacrificed to evaluate the hearts. The remaining 50% were followed for 491 days. a D. rerio heart SFD1 to 129 days. Image ×4. b D. rerio heart ventricle with SFD1 to 129 days. Image ×10. c D. rerio heart HFD1 to 129 days. Image ×4. d D. rerio heart ventricle with HFD1 to 129 days. Image ×10. e D. rerio heart SFD1 to 491 days. Image ×4. f D. rerio heart ventricle with SFD1 to 491 days. Image ×10. g D. rerio heart HFD1 to 491 days. Image ×4. h D. rerio heart ventricle with HFD1 to 491 days. Image ×10. Bars represent 0.5 and 0.05 mm in ×4 and ×10, respectively. In c, e, and g, a globular shape is observed, but in g, the size is much larger. r1 major axis, r2 minor axis, α3 apex angle, CM compact myocardium, SM spongy myocardium (dotted line)
Histology
Because it is not possible to obtain an ideal cut as the histological procedure can generate modifications to the samples, it was not always possible to compare data measurements from the isolated organs with the histological measurements. In trial 1, both r1 and r2 were greater in the HFD1 compared with the SFD1 group in the histological sections both at 129 and 491 days (Fig. 5). In these images, a change to a globular shape of the heart should also be noted to be associated with larger heart size in the HFD1 group at 129 days, compared to the triangular shape heart in the SFD1 group (Fig. 5a and c). Interestingly, at the end of the trial (491 days), the heart shape was globular in both groups (Fig. 5e and g). This globular shape makes it difficult to measure and compare cardiac angles, but it is obvious that the angles are markedly increased in globular hearts, especially the alpha-3 angle, which is the angle related to the ventricular apex.
In trial 2, both r1 and r2 were greater in the HFD2 group. Similarly, a triangular shape was observed in the control group and the SFD2 group, while a globular shape was observed in the HFD2 group (Fig. 6a, c, and e). These changes are similar to those observed on day 129 in trial 1 (Fig. 5a and c).

Histology D. rerio heart in trial 2. Feeding and monitoring were performed for 258 days in 100% of the specimens, at which time they were sacrificed to evaluate the hearts. a D. rerio heart control. Image ×4. b D. rerio heart ventricle control. Image ×10. c D. rerio heart SFD2. Image ×4. d D. rerio heart ventricle SFD2. Image ×10. e D. rerio heart HFD2. Image ×4. f D. rerio heart ventricle HFD2. Image ×10. Bars represent 0.5 and 0.05 mm in ×4 and ×10, respectively. r1 major axis, r2 minor axis, α3 apex angle, CM compact myocardium, SM spongy myocardium (dotted line)
Structurally, both in test 1 as in test 2, trabecular thickening of the spongy portion of the myocardium was observed in the HFD groups. This was most evident at 129 days in the first trial (Fig. 5d) and at the end of the second trial (Fig. 6d and f). Interestingly, although in the first trial, r1 and r2 increased at day 491, making it difficult to completely visualize the ventricle in the ×4 objective of the microscope (Fig. 5g), the trabecular thickening decreased (Fig. 4h). This finding, coupled with the highest values of r1 and r2 and the globular shape, could indicate the reversal of secondary hypertrophic changes, which occurred in parallel to the reduced amount of food at the end of the experiment. Another explanation is that these changes could also reflect a state of dilated cardiomyopathy and possibly heart failure, which was not assessed in this study. Previously, some authors have described changes in the angles and shape of the ventricle in various species of wild and domesticated fish, and they suggest that these measurements could be useful in determining the impact of environmental factors such as food availability on the structure and cardiac function (Pombo et al. 2012).
Discussion
The effects of overfeeding and HFDs in young and adult zebrafish specimens were evaluated in this study.
The HFD led to greater BWG than overfeeding. These changes can be considered to lead to obesity because the data reported here are consistent with the values published by Oka et al., where it was established that BMI values greater than 0.08 g/cm2 are indicators of obesity (Oka et al. 2010). Before the third month in the first trial, no differences were distinguished between the SFD1 and HFD1 group parameters, which could indicate an apparent resistance to DOI, as has been proposed by other authors (Leibold and Hammerschmidt 2015). However, it was observed that from the third month to the end of the trial, weight gain was greater in the HFD1 group. This outcome created statistically significant differences in BMI and factor K (4A, 4C, 4E), and these differences persisted throughout the trial. These results could indicate that the apparent resistance of juvenile fish to DIO is because they are still in the period of scale and tissue generation, including adipose tissue, which decreases the possibility of accumulating excess adipose tissue. From the sixth month, adult zebrafish can accumulate excess calories from the diet in storage tissues, which leads to significant differences in weight gain, BMI, and factor K among the SFD1 and HFD1 groups.
In the second trial, which included mature zebrafish, rapid weight gain in the HFD2 group was observed compared to the SFD2 group (Fig. 3a–b). This indicates that in adult fish, excess dietary fat generates weight gain due to the accumulation of surplus fat in storage tissues, and this intervention achieved a BMI higher than 0.08 g/cm2. However, although differences between average values exist, no statistically significant differences between SFD2 and HFD2 were observed (Fig. 4b, d, and f). This could indicate that not only a HFD but also overfeeding could cause obesity in some individuals. This would reinforce the theory that obesity is a multicausal disease, where factors such as genetics, gender (not tested here), or social behavioral factors that determine food availability, such as dominance in the group, are also determinants.
This study also showed that not only BMI and factor K are useful parameters in evaluating physical development but also the H/W ratio could be useful. The H/W ratio is higher in the early stages where the tissue growth is predominant, which is reflected in the fast increase in standard length with a slow weight gain. The value of the H/W ratio decreases with age to reach normal standard length values and is further reduced with progressive weight gain. This high reduction in the values of the H/W ratio was evident in the specimens that demonstrated obesity in trial 1, implying that a lower H/W ratio in comparison with the reference values at a certain stage of life could be due to obesity or could serve as a low-growth indicator.
Here, it was shown that the composition of the diet is a factor capable of inducing changes in cardiosomatic parameters, and the fat content in the diet is a decisive component. It has been suggested that nutritional imbalance in the early stages of development of the individual determines the biotype in its advanced stages of development (Galtier-Dereure et al. 2000; Boney et al. 2005; Risnes et al. 2011). It is postulated that when excess calories are supplied in the diet, it increases the likelihood of increasing the amount of adipose tissue and lipid accumulation. There are two mechanisms documented for this increase in adipose tissue: the hypertrophy or the hyperplasia of adipocytes (de Ferranti and Mozaffarian 2008). The contribution of one or the other mechanism depends on various factors, including age, diet, genetics, and neuroendocrine regulation (Bourgeois et al. 1983; Bray et al. 2004; Joe et al. 2009). These mechanisms determine the possibility that adipose tissue can expand between 2 and 70% of body weight in response to a positive energy balance in humans (Hussain et al. 2007).
Several authors argue that in humans, the increase in the number of adipocytes in the early stages of life is due to various factors including maternal obesity, gestational diabetes, and nutritional disorders, which favor an increased capacity to accumulate excess nutrients in the form of triglycerides and neutral fatty acids in adipocytes in adults. This could imply that the probability of overweight and obesity will be higher in individuals with a history of childhood overweight because they will have a greater number of adipocytes in fat tissue (Kaur et al. 2003; Boney et al. 2005; Cali and Caprio 2008; Risnes et al. 2011; Stuart and Panico 2016). On the other hand, from the cardiovascular standpoint, adipose tissue under normal conditions is an endocrine organ that normally participates in the regulation of cardiovascular function through balanced synthesis and release of proinflammatory and antiinflammatory adipokines. Obesity is considered to induce a state of subclinical chronic inflammation where the synthesis and release of proinflammatory adipokines that may lead to tissue damage and multiple organ dysfunction predominate (Mancuso 2016). Obesity is therefore a cardiovascular risk factor because it can cause direct damage, affecting the heart muscle and blood vessels or causing endothelial dysfunction through proinflammatory cytokines, or it may cause indirect damage due to cardiovascular overloading secondary to the necessity to guarantee perfusion to multiple organs with inflammatory lesions (Yiannikouris et al. 2010; Bhatheja et al. 2016; Mancuso 2016). However, further studies are required in humans to clarify the mechanisms underlying these phenomena and others as the beneficial and paradoxical relationship between heart failure and moderate obesity (Ebong et al. 2014; Bhatheja et al. 2016). To develop research around these topics, animal models such as zebrafish can be extremely useful tools.
Several studies in animal models have shown that diets rich in lipids induce proliferation of subcutaneous adipose tissue and hypertrophy of visceral adipose tissue. In mice, it has been confirmed that a HFD induces proliferation of cellular progenitors of adipocytes in subcutaneous adipose tissue (Bourgeois et al. 1983; Joe et al. 2009). Similarly, some studies in rodents have shown that weight gain is not always associated with hyperphagia because isocaloric diets may induce accumulation of visceral adipose tissue and this is related to the fat content in the diet (Boozer et al. 1995; West and York 1998). Additionally, it has been described in obese mice that some antiobesity interventions, such as lipectomy, stimulate lipogenesis and adipocyte differentiation (Nascimento et al. 2009).
In zebrafish, a direct correlation between HFD and the development of adipocytes in live larvae was recently reported. This has been documented by a test employing a vital dye, Nile red, which is incorporated in the forming tissue (Flynn et al. 2009; Tingaud-Sequeira et al. 2011). Likewise, hypertrophy and hyperplasia of adipocytes in the DIO model have been reported, and DIO resistance in young zebrafish has been reported (Leibold and Hammerschmidt 2015). In addition, it has been described that overfeeding stimulates the formation of pancreatic beta cells (Li et al. 2014). The high number of beta cells may promote a state of hyperinsulinemia and insulin resistance (Lichtenstein and Schwab 2000; Riccardi et al. 2004; Haag and Dippenaar 2005), which induce changes in metabolism that favor the accumulation of lipids in white adipose tissue. It must also be considered that insulin, by acting as a growth factor in different tissues, can induce cell proliferation and induce states of macrosomia (Nakae et al. 2001). The increase in tissue growth stimulated by growth factors released in the very early stages of development or growth factors that are persistently released could increase proliferation of precursors of adipocytes in adipose tissue. From the point of view of cardiac tissue, in zebrafish, the development of cardiac structures from the embryonic stage to adulthood has been documented, but under normal conditions (Singleman and Holtzman 2011). We believe that this is the first time where a possible link between obesity and the presence of changes in cardiosomatic parameters and cardiac structures has been reported. All of this evidence argues that the changes observed in the cardiosomatic parameters in this study are secondary to the stimulus generated by HFD regimen, which was administered chronically and early in the developmental stages. However, these results must be supplemented by additional studies that include more advanced biochemical, molecular, genetic, and functional techniques.
In conclusion, this study demonstrated that chronic administration of a HFD in zebrafish, both young and old, modifies somatic parameters in advanced stages. Specifically inducing a high-weight gain and high BMI, the values achieved in these parameters met the criteria that were previously established to define obesity in this model. Parallel changes were observed in the zebrafish heart, including increases in size and changes in morphology, and a globular shape in contrast to the triangular shape of the controls. Similarly, trabecular thickening of the myocardium forming spongy myocardium was observed. All of these changes can be considered to be due to nutritional imbalances inducing lipid accumulation and obesity. This state generates a subclinical inflammatory response, which in turn generates an overload to the cardiovascular system and induces adaptive changes in the heart. Given the genetic similarity between zebrafish and humans, these results could be extrapolated and information added that supports the hypothesis of the relationship between HFD content and cardiovascular risk factors. Similarly, it highlights the importance of incorporating a balanced diet from the early life stages to reduce the risk of cardiovascular disease.
References
Bakkers J (2011) Zebrafish as a model to study cardiac development and human cardiac disease. Cardiovasc Res 91(2):279–288. doi:10.1093/cvr/cvr098
Bender R, Zeeb H, Schwarz M, Jöckel K-H, Berger M (2006) Causes of death in obesity: relevant increase in cardiovascular but not in all-cancer mortality. J Clin Epidemiol 59(10):1064–1071. doi:10.1016/j.jclinepi.2006.01.006
Bhatheja S, Panchal HB, Ventura H, Paul TK (2016) Obesity cardiomyopathy: pathophysiologic factors and Nosologic reevaluation. Am J Med Sci 352(2):219–222. doi:10.1016/j.amjms.2016.05.014
Boney CM, Verma A, Tucker R, Vohr BR (2005) Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 115(3):e290–e296. doi:10.1542/peds.2004-1808
Boozer CN, Schoenbach G, Atkinson RL (1995) Dietary fat and adiposity: a dose-response relationship in adult male rats fed isocalorically. Am J Physiol Endocrinol Metab 268(4):E546–E550
Bourgeois F, Alexiu A, Lemonnier D (1983) Dietary-induced obesity: effect of dietary fats on adipose tissue cellularity in mice. Br J Nutr 49(1):17–26
Bray GA, Paeratakul S, Popkin BM (2004) Dietary fat and obesity: a review of animal, clinical and epidemiological studies. Physiol Behav 83(4):549–555. doi:10.1016/j.physbeh.2004.08.039
Cali AMG, Caprio S (2008) Obesity in children and adolescents. J Clin Endocrinol Metab 93(11 Suppl 1):S31–S36. doi:10.1210/jc.2008-1363
Dietz WH (1998) Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics 101(Supplement 2):518–525
Ebong IA, Goff DC, Rodriguez CJ, Chen H, Bertoni AG (2014) Mechanisms of heart failure in obesity. Obes Res Clin Pract 8(6):e540–e548. doi:10.1016/j.orcp.2013.12.005
de Ferranti S, Mozaffarian D (2008) The perfect storm: obesity, adipocyte dysfunction, and metabolic consequences. Clin Chem 54(6):945–955. doi:10.1373/clinchem.2007.100156
Flint AJ, Rimm EB (2006) Commentary: obesity and cardiovascular disease risk among the young and old—is BMI the wrong benchmark? Int J Epidemiol 35(1):187–189. doi:10.1093/ije/dyi298
Flynn EJ, Trent CM, Rawls JF (2009) Ontogeny and nutritional control of adipogenesis in zebrafish (Danio rerio). J Lipid Res 50(8):1641–1652. doi:10.1194/jlr.M800590-JLR200
Frankel PH (2003) Obesity and cancer. N Engl J Med 349(5):502–504
Galtier-Dereure F, Boegner C, Bringer J (2000) Obesity and pregnancy: complications and cost. Am J Clin Nutr 71(5):1242s–1248s
Gonzales JM, Law SHW (2013) Feed and feeding regime affect growth rate and gonadosomatic index of adult zebrafish (Danio rerio). Zebrafish 10(4):532–540. doi:10.1089/zeb.2013.0891
Goodwin N, Westall L, Karp NA, Hazlehurst D, Kovacs C, Keeble R, Bussell J (2016) Evaluating and optimizing fish health and welfare during experimental procedures. Zebrafish 13(S1):S–127. doi:10.1089/zeb.2015.1165
Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH (2009) The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health 9:88. doi:10.1186/1471-2458-9-88
Haag M, Dippenaar NG (2005) Dietary fats, fatty acids and insulin resistance: short review of a multifaceted connection. Med Sci Monit: Int Med J Exp Clin Res 11(12):RA359–RA367
Hussain A, Claussen B, Ramachandran A, Williams R (2007) Prevention of type 2 diabetes: a review. Diabetes Res Clin Pract 76(3):317–326. doi:10.1016/j.diabres.2006.09.020
Imrie D, Sadler KC (2010) White adipose tissue development in zebrafish is regulated by both developmental time and fish size. Dev Dyn 239(11):3013–3023. doi:10.1002/dvdy.22443
Joe AWB, Yi L, Even Y, Vogl AW, Rossi FMV (2009) Depot-specific differences in adipogenic progenitor abundance and proliferative response to high-fat diet. Stem Cells 27(10):2563–2570. doi:10.1002/stem.190
Kaur H, Hyder ML, Poston WSC (2003) Childhood overweight: an expanding problem. Treat Endocrinol 2(6):375–388
Kowalska A, Zakęś Z, Siwicki AK, Jankowska B, Jarmołowicz S, Demska-Zakęś K (2012) Impact of diets with different proportions of linseed and sunflower oils on the growth, liver histology, immunological and chemical blood parameters, and proximate composition of pikeperch Sander lucioperca (L.) Fish Physiol Biochem 38(2):375–388. doi:10.1007/s10695-011-9514-z
Lawrence C (2007) The husbandry of zebrafish (Danio rerio): a review. Aquaculture 269(1–4):1–20. doi:10.1016/j.aquaculture.2007.04.077
Leibold S, Hammerschmidt M (2015) Long-term hyperphagia and caloric restriction caused by low- or high-density husbandry have differential effects on zebrafish postembryonic development, somatic growth, fat accumulation and reproduction. PLoS One 10(3):e0120776. doi:10.1371/journal.pone.0120776
Li M, Maddison LA, Page-McCaw P, Chen W (2014) Overnutrition induces β-cell differentiation through prolonged activation of β-cells in zebrafish larvae. Am J Physiol Endocrinol Metab 306(7):E799–E807. doi:10.1152/ajpendo.00686.2013
Lichtenstein AH, Schwab US (2000) Relationship of dietary fat to glucose metabolism. Atherosclerosis 150(2):227–243
Little TJ, Russo A, Meyer JH, Horowitz M, Smyth DR, Bellon M et al (2007) Free fatty acids have more potent effects on gastric emptying, gut hormones, and appetite than triacylglycerides. Gastroenterology 133(4):1124–1131. doi:10.1053/j.gastro.2007.06.060
Lobstein T, Baur L, Uauy R (2004) Obesity in children and young people: a crisis in public health. Obes Rev 5:4–85. doi:10.1111/j.1467-789X.2004.00133.x
Mancuso P (2016) The role of adipokines in chronic inflammation. ImmunoTargets Ther 5:47–56. doi:10.2147/ITT.S73223
Meguro S, Hasumura T, Hase T (2015) Body fat accumulation in zebrafish is induced by a diet rich in fat and reduced by supplementation with green tea extract. PLoS One 10(3):e0120142. doi:10.1371/journal.pone.0120142
Nakae J, Kido Y, Accili D (2001) Distinct and overlapping functions of insulin and IGF-I receptors. Endocr Rev 22(6):818–835. doi:10.1210/edrv.22.6.0452
Nascimento CMO d, Ribeiro EB, Oyama LM (2009) Metabolism and secretory function of white adipose tissue: effect of dietary fat. An Acad Bras Cienc 81(3):453–466. doi:10.1590/S0001-37652009000300010
Nekoubin H, Rakhshanipour G, Hatefi S, Sudagar M, Montajami S (2013) Effects of feeding frequency on growth performance and survival rate of zebra fish (Danio rerio). Adv J Agric Res ResearchGate 1:7–10
Oka T, Nishimura Y, Zang L, Hirano M, Shimada Y, Wang Z, … Tanaka T (2010) Diet-induced obesity in zebrafish shares common pathophysiological pathways with mammalian obesity. BMC Physiol 10:21. doi:10.1186/1472-6793-10-21
Pannevis MC, Earle KE (1994) Maintenance energy requirement of five popular species of ornamental fish. J Nutr 124(12 Suppl):2616S–2618S
Pombo A, Blasco M, Climent V (2012) The status of farmed fish hearts: an alert to improve health and production in three Mediterranean species. Rev Fish Biol Fish 22(3):779–789. doi:10.1007/s11160-012-9259-5
Poppitt SD, Prentice AM (1996) Energy density and its role in the control of food intake: evidence from metabolic and community studies. Appetite 26(2):153–174. doi:10.1006/appe.1996.0013
Riccardi G, Giacco R, Rivellese AA (2004) Dietary fat, insulin sensitivity and the metabolic syndrome. Clin Nutr 23(4):447–456. doi:10.1016/j.clnu.2004.02.006
Risnes KR, Vatten LJ, Baker JL, Jameson K, Sovio U, Kajantie E, … Bracken MB (2011). Birthweight and mortality in adulthood: a systematic review and meta-analysis. Int J Epidemiol 40(3):647–661. doi:10.1093/ije/dyq267
Rössner S (1998) Childhood obesity and adulthood consequences. Acta Paediatr 87(1):1–5. doi:10.1111/j.1651-2227.1998.tb01375.x
Singleman C, Holtzman NG (2011). Heart dissection in larval, juvenile and adult zebrafish, Danio rerio. J Vis Exp (55). doi:10.3791/3165
Stuart B, Panico L (2016) Early-childhood BMI trajectories: evidence from a prospective, nationally representative British cohort study. Nutr Diabetes 6:e198. doi:10.1038/nutd.2016.6
Tingaud-Sequeira A, Ouadah N, Babin PJ (2011) Zebrafish obesogenic test: a tool for screening molecules that target adiposity. J Lipid Res 52(9):1765–1772. doi:10.1194/jlr.D017012
Vargas R, Vásquez IC (2016) Cardiac and somatic parameters in zebrafish: tools for the evaluation of cardiovascular function. Fish Physiol Biochem 42(2):569–577. doi:10.1007/s10695-015-0160-8
Velasco-Santamaría Y, Corredor-Santamaría W (2011) Nutritional requirements of freshwater ornamental fish: a review. Rev MVZ Córdoba 16(2):2458–2469
Visscher TL, Seidell JC (2001) The public health impact of obesity. Annu Rev Public Health 22(1):355–375. doi:10.1146/annurev.publhealth.22.1.355
Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, … Caprio S (2004) Obesity and the metabolic syndrome in children and adolescents. N Engl J Med 350(23):2362–2374. doi:10.1056/NEJMoa031049
West DB, York B (1998) Dietary fat, genetic predisposition, and obesity: lessons from animal models. Am J Clin Nutr 67(3):505S–512S
Xu, Xue (2016) Pediatric obesity: causes, symptoms, prevention and treatment (review). Exp Ther Med 11(1):15–20. doi:10.3892/etm.2015.2853
Yiannikouris F, Gupte M, Putnam K, Cassis L (2010) Adipokines and blood pressure control. Curr Opin Nephrol Hypertens 19(2):195–200. doi:10.1097/MNH.0b013e3283366cd0
Acknowledgements
This work was supported by Research Grant from the Pontificia Universidad Javeriana, Bogotá, Colombia. Project: 5605, budget code 120112Z0401200.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical statement
No ethical issues are involved in this work.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Vargas, R., Vásquez, I.C. Effects of overfeeding and high-fat diet on cardiosomatic parameters and cardiac structures in young and adult zebrafish. Fish Physiol Biochem 43, 1761–1773 (2017). https://doi.org/10.1007/s10695-017-0407-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10695-017-0407-7