
Abstract
Lynch syndrome (LS) is caused by inherited germline mutations in mismatch repair (MMR) genes. It is one of the commonest forms of inherited predisposition to colorectal cancer (CRC), accounting for 2–5% of all CRC. LS is characterized by early age of onset, with a tendency for multiplicity and an increased risk for extra-colonic tumors at particular sites. In this study we have evaluated the frequency of extra-colonic tumors in 60 unrelated LS families fulfilling the Amsterdam criteria (ACI. ACII) from the Oncotree database of the Hereditary Colorectal Cancer Registry of the AC Camargo Hospital. All families’ pedigree was extensively analyzed, varying from 2 to 6 generations with a total of 2,095 individuals evaluated. As expected, colorectal cancer was the most frequent tumor in the families (334 cases). We found 200 extracolonic tumors among all individuals with a higher ratio in women (123 cases) than men (77 cases). By far, breast cancer (32 cases) was the most frequent extracolonic manifestation in women followed by endometrial (20 cases) and uterine cervix cancer (20 cases). For man, prostate (16 cases) and stomach (12 cases) cancer were the most frequent extracolonic tumors. It is well know that establishing the diagnosis is challenging and requires knowledge and surveillance. Thus, recognition of individuals and families with hereditary predisposition to cancer according to clinical and molecular features, combined with intensive surveillance and management programs, can contribute substantially to improve results related to the diagnosis and characterization of LS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is one of the most common forms of all familial cancers. Several studies indicate that familial colorectal cancer accounts for about 30% of all CRC cases. Worldwide, CRC mortality is just below lung and gastric cancer. Inherited factors are a common risk factor for CRC and first-degree relatives’ exhibit two to three fold increased risk for large bowel cancer [1–5]. Additionally, over the past century, familial aggregations of CRCs have frequently been documented [6–9] leading to the characterization of inherited colorectal syndromes, including Lynch syndrome (LS) [10]. In Brazil, the number of CRC new cases estimated for 2010 is 13,310 in men and 14,800 in women, which represents an incidence rate of 13,73/100,000 (men) and 14,80/100,000 (women) [11]. The estimated base for the year 2010 is approximately 8,100 (30%) new cases with an inheritable factor for CRC.
Lynch syndrome, also known as Hereditary non-polyposis colorectal cancer (HNPCC) is the most common form of inherited predisposition to colorectal cancer, accounting for 2–5% of all CRC [12]. Colorectal cancer in LS differs from sporadic cases by an earlier age of diagnosis (mean age approximately 44 years), a predominance of proximally-sited colon cancers (60–70%) and an increased propensity to synchronous or metachronous CRCs (25%) [13, 14]. Individuals with LS have an 80% probability of developing CRC at 65 years, and they are at an elevated risk of developing a second primary CRC [15] as well as at an increased risk for extra-colonic malignancies, including gastric, small bowel, urological tract, ovary, pancreas and brain cancer [16].
In 1991, Vasen et al. reported efforts by the International Collaborative Group on Hereditary Nonpolyposis Colorectal Cancer (ICG-HNPCC) to establish a set of selection criteria for families with LS (Amsterdam Criteria I [AC-I]): (1) at least three relatives must have histologically verified CRC; (2) one must be a first-degree relative of the other two; (3) at least two successive generations must be affected; (4) at least one of the relatives with CRC must have received the diagnosis before age 50; and (5) familial adenomatous polyposis must have been excluded. Different primary sites had been described in families with a possible diagnostic of LS: endometrial, stomach, ovaries, small bowel, ureter, renal pelvis, brain, and hepatobiliary tract cancer. Among these tumors, endometrial, ureter, renal pelvis, and small bowel cancers present the highest relative risk, and are therefore the most specific for LS. At the 1998 meeting, an agreement was reached that these extracolonic tumors should be included, and a set of new clinical criteria was then proposed (Amsterdam Criteria II, ACII) [17, 18] (Table 1).
LS is an autosomal dominant syndrome with high penetrance (about 85%), due to mutations in the mismatch repair genes (MMR) [19–22]. The main genes involved are MSH2, MLH1, MSH6, PMS2 and PMS1 [18, 23, 24]. In different geographical areas the frequency and the types of mutations are widely variable. Therefore, the frequency of extra-colonic tumors associated with LS may be different in different countries [25–27].
So far, relatively little information has became available on the spectrum of tumors related to LS in South America. Thus, this study aims to make an update from a previous report [28] describing the frequency of malignant tumors in larger group of Brazilian families with clinical HNPCC in an Institutional Hereditary Colorectal Cancer Registry.
Materials and methods
In order to evaluate the frequency of CRC and extracolonic tumors, the study used the Oncotree database of the Hereditary Colorectal Cancer Registry of the Pelvic Surgery Department of Hospital AC Camargo (São Paulo, Brazil). The families analyzed were classified as LS according to Amsterdam Criteria I or II and were registered in the period between January 1998 and June 2009.
Patients and relatives were interviewed after informed consent. The following data were evaluated in each family: total number of members, number of patients with CRC, number of patients with extra-colonic tumors, primary sites of the extra-colonic tumors, age at diagnosis and number of generations evaluated. The diagnosis of extra-colonic tumor was based on verbal report and confirmed clinical or pathological information, whenever possible. Cases with uncertain information were not considered. When it was not possible to identify the main organ of the primary tumor, the site was classified as unknown.
Results
This study included 1,040 men and 1,055 women (2,095 total) from 60 LS families (53 Amsterdam I and 7 Amsterdam II). The number of individuals in LS families ranged from 5 to 139 (mean 34.9; median 29.5), with evaluation of 6 generations in 1 family (1.6%), 5 generations in 19 families (31.6%), 4 generations in 33 families (55%), 3 generations in 6 families (10%) and 2 generations in 1 family (1.6%).
As expected, CRC was the most common tumor type in these LS families. We identified 334 individuals with CRC in all generations evaluated (2,095 individuals) that revealed 361 CRC. In total, we identify 482 individuals with cancer, showing 561 CRC and extra-colonic tumors (Table 2).
In these 60 LS families, extra-colonic tumors were more frequent in women (123 cases) than in men (77). Applying the qui square test, women had significant difference for the presence of extra-colonic tumors when compared with men. The test was applied in both Amsterdam criteria and was statistically significant between genders.
The age at diagnosis was documented in 76.3% (428/561) of all cancers, and ranged from 9 to 93 years (mean age of the first primary tumor was 34 and 46 years overall). 67 patients had more than 1 tumor (53 patients had 2 tumors, 10 patients had 3 tumors, and 4 patients had 4 tumors).
Figure 1 shows that the most frequent extra-colonic tumors in men were prostate (16 cases), followed by gastric (12 cases), hepatobiliary tract (4 cases), pancreas (4 cases), lung (4 cases), skin (4 cases), brain (4 cases), oral (4 cases), leukemia (4 cases), kidney (3 cases), bladder (3 cases), renal pelvis/ureter (3 cases), small bowel (1 case) and other sites including non-specific location tumors (10 cases).

Frequency of extra-colonic tumors in men (60 HNPCC families)
In women, the most frequent primary site in these families were breast (32 cases), followed by uterine cervix (20 cases), endometrium (20 cases), stomach (12 cases), ovary (4 cases), oral (4 cases), leukemia (4 cases), pelvis renal (3 cases), small bowel (3 cases), brain (3 cases), sebaceous (2 cases), skin (2 cases) and other sites including non-specific location tumors (16 cases) (Fig. 2).

Frequency of extra-colonic tumors in women (60 HNPCC families)
Table 3 shows the percentage of all extra-colonic tumors in men and women in 60 LS families. Breast cancer was, by far, the most frequent tumors in women with 32 cases, representing 26% of the cases. In men, the most frequent primary site was the prostate, which represents 21% of the cases.
Discussion
In Brazil, the incidence rate for breast cancer is 49.27/100.000 and for these LS families the rates would considerably increase to 3,408/100.000 [11]. Moreover, the median age of diagnosis was 42 (25–84) years old, which is almost 20 years earlier than general population [29]. Although breast cancer is not considered part of the tumor spectrum, several studies have found a higher incidence of breast cancer among LS relatives [30–35] and MMR defective breast cancer has been described in a number of mutation carriers, pointing out its probable involvement in LS spectrum of extra-colonic tumors [28].
Although studies on the role of MMR defects in breast cancer have reached different conclusions about its possible link to HNPCC [31, 36–40], recently, Jensen et al. studied 164 families in Denmark with disease-predisposing MMR gene mutations and have identified 20 mutation carriers affected with breast cancer at mean age of 51 years. They have found loss of MMR protein expression in 43% of breast cancer patients (7/16), demonstrating that MMR plays a role in a substantial proportion of cases. According to the authors, lymphocytic reactions, a common feature of colorectal cancer [41], could represent a potential marker for MMR defective breast cancer in individuals with LS [42].
It is possible that the findings of this series may be due to other syndromes of colorectal cancer predisposition. MEIJERS-Heijboer et al. published a study on families with colorectal cancer and breast cancer, which were tested for mutation in BRCA1, BRCA2 and mismatch repair genes. A set of non-mutation carries, but with phenotype of breast-colon syndrome, had a significant increase in the incidence of CHEK2 1100delC mutation (18.2%) compared to families without breast-colon cancer. Their findings may suggest an association between CHEK2 1100delC in breast-colon syndrome [43], nevertheless, our study showed 21 Amsterdam families with cases of breast cancer and no CHEK2 1100delC mutation was found (data not published), suggesting that the CHEK2 1100delC variant is not relevant in Brazilian LS families with high rates of breast cancer. Additionally, we can speculate the possibility of an overlapping between hereditary breast-ovary cancer and HNPCC syndromes, due the fact that some families fulfill both criteria, creating a confusion factor for the correct interpretation.
LS women have a 24–62% risk of developing endometrial cancer [36, 44–47] and, indeed, ours results showed high frequency of endometrial cancer,and also uterine cervical cancer. Due to the fact that families’ pedigree, in some cases, are filled based on verbal report of the index patient, the difference between cervical uterine and endometrial tumors can be a confounding factor, so that the correct number of endometrial cancer among families can be higher than we think. This high frequency of endometrial tumors can be supported by the recent study which states that 1.6% of all endometrial cancers are related to germline mutations in hMSH6 gene [48]. Germline MSH6 mutations are responsible for approximately 10% of Lynch syndrome cases, [49] suggesting that the total of LS-related endometrial cancers are underestimated and may be considerably higher than the imagined.
The greater incidence rate of women affected by extra-colonic tumors when compared to men, again, highlights the significant proportion of endometrial cancer in LS families. In addition, breast cancer was found with the highest frequency among families, contributing to this greater incidence of extra-colonic tumors.
Cervical cancer is the second most common type of cancer in women worldwide. Several human papillomavirus (HPV) genotypes, sexual behavior, and socioeconomic profile represent major risk factors for the development of this carcinoma.
Many studies found a direct association of HPV infection with number of sexual partners [50–52]. Generally, the trend in many Western countries is that sexual behaviors and attitudes have become more permissive over time. Several studies have reported that earlier sexual debut or shorter intervals between menarche and sexual debut are risk factors for prevalent HPV infection. In addition, numbers of new and recent sexual partners and likelihood of detecting HPV in female is strong and consistent [53]. Cervical cancer is the second most common tumor in Brazil which is characterized by great socioeconomic and cultural discrepancies, making this type of tumor less likely to be associated with Lynch syndrome.
Despite the fact that gastric cancer is the second most common extra-colonic malignancy in LS [36, 54] and in some populations is the most frequent extra-colonic manifestation [55, 56], at present, it is not included in the Amsterdam criteria.
It is known that the incidence of gastric cancer varies widely in different geographic regions, being relatively higher in eastern countries (Japan, Korea and China) and Latin America. There are two main histologic variants of gastric cancer, the intestinal type and diffuse type [57]. The diffuse type has often been related to changes in the CDH1 gene [58–60], while the intestinal type is the most frequently found in the general population and commonly related to environmental exposures which include a diet rich in meats, smoked foods, tobacco, alcohol consumption and H. Pylori infection. However, Gylling et al. have conducted a study with 13 HNPCC gastric cancer patients demonstrating that the age of diagnosis of HNPCC gastric cancer was 58 years against 76 years in sporadic gastric cancer, 92% of the tumors had intestinal histology, MSI-high, absence of the MMR protein, frequent APC-LOH as typical of intestinal gastric cancer and a number of other tumourigenic events typical of MMR deficiency; suggesting that all these findings justify considering gastric cancer as a true LS spectrum of malignancy [61].
The mean age of onset for gastric cancer in these 60 families was 53 years, and the estimated risk for 2010 in Brazil for gastric cancer is 14:100.000 and 7:100.000 for women. Evaluating these affected families the rates would rise to 1,326/100.000 and 1,065/100.000, respectively. Despite the elevated risk in these LS families, gastric cancer is high frequent in the Brazilian general population, making the specificity of the association with LS remains poor and challenging, so that further analysis needs to be set.
For prostate cancer, most of the cases, the age of diagnosis was over 70 years, and because of this, prostate cancer is unlikely to be part of LS spectrum of tumors and more likely to be associated with environmental exposure as aforementioned for gastric cancer.
Genotype-phenotype correlation
Originally, HNPCC was described as a familial clustering of colorectal cancer through the Amsterdam criteria which is based only in personal and family histories of cancer [62]. However, about 50% of HNPCC families fulfilling the stringent AC-I do not have mutations in DNA repair, in addition, families who do not meet the Amsterdam criteria, less than 30% have mutations [63, 64].
Some of the possible explanations for the low rate of mutation-positive on the Amsterdam criteria lies on the accuracy of the reported family history, as the clinical criteria for HNPCC diagnosis is only reliable if the diagnosis of family members is confirmed [65]. One limitation of this study is the possibility of underreporting or misreporting of cancers. Murff HJ et al. post that patient-reported family cancer histories are accurate and valuable for assessing the risk of breast cancer and colorectal cancer, but are less accurate for more rare types of cancer [66]. Efforts were made to verify reported cancers, but this was not always feasible.
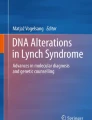
Detection of microsatellite Instability is one of the most used techniques among colorectal cancer patients. Individuals with microsatellite instability indirectly show abnormalities in MMR genes that causes protein deficiencies and loss of repair. However, even among families that meet the Amsterdam criteria and show microsatellite instability (MSI) in tumor tissue, a third fails to display any structural change in the MMR genes [67]. According to Renkonen et al. these presumable patients are “hidden” MMR gene mutation-carries that escape detection by conventional techniques [68]. On the other hand, patients who meet the Amsterdam criteria, but have no identifiable mutations or microsatellite instability, have been reported with a new entity called “familial colorectal cancer type X” that can reach 40% of AC-I positive probands [69].
Immunohistochemistry has been very useful to complement MSI testing. IHC is problably 95% sensitive for MMR deficiency and has been used in hospitals either to complement MSI testing or as a substitute [67]. In this series, we evaluate the immunohistochemical expression of MMR genes in 23 out of 60 colorectal cancer patients, where 8 (35%) showed normal expression for all MMR genes.
One of the main features of hereditary nonpolyposis colorectal cancer is the proximal colonic cancer predilection, which can be found in approximately 70% of HNPCC CRCs [70]. Indeed, In our series most patients had right-side CRCs, but a considerable proportion of rectal cancer was reported.
It has been postulated that the Amsterdam criteria have a limited set of clinical characteristics that have failed to diagnose HNPCC patients, whereas today there is clear evidence that families that meet the Amsterdam criteria are clinically heterogeneous. Currently, the use of these criteria has became obsolete due the advances in the pathology of HNPCC tumors and the emergence of microsatellite instability and immunohistochemistry testing. However, the Amsterdam criteria is not completely worthless, since it is still very useful in the acquisition of a comprehensive family history and more recently, in the identification of another subset of possibly hereditary colorectal cancers, which is currently referred to familial colorectal cancer type X.
Even in the absence of typical clinical characterization, there need to be criteria for directing the search for inherited conditions. Hence, correct interpretation of the spectrum of extra-colonic tumors in Lynch syndrome cases acquires great importance. The frequent new molecular findings have been of great importance for better defining the genotype-phenotype correlation and thus the spectrum of extra-colonic tumors for LS.
It is well known that establish the diagnosis is challenging and requires knowledge and surveillance. Due the lack of sensitivity and specificity of clinical criteria, occurrence of de novo mutations and the failure in identify MMR genes mutations, the incidence of LS can be underdiagnosed. It is believed that LS is one of the most common hereditary syndromes in humans, with incidence ranging from 1:350 to 1:2000 [71, 72]. It is vital that families at high risk should accomplish screening programs and management protocols in order to prevent cancer.
Conclusions
We have shown an update of a previous report from Oliveira et al. [28] consolidating some important findings in the spectrum of extra-colonic tumors in Brazil. In summary, we have reported a high incidence of breast and gastric cancer with strong evidence of their role in LS tumorigenesis, supported by previous findings that breast and gastric cancer do arise through mismatch repair defects in LS kindreds. On the other hand, there is a possible involvement of other yet unknown genes due to the differential diagnosis of the Amsterdam criteria associated with immunohistochemistry and microsatellite instability testing.
Diagnostics criteria for LS are controversial due to variations in clinical phenotypes in different areas and countries. Thus, recognition of individuals and families with hereditary predisposition to cancer according to clinical and molecular features, combined with intensive surveillance and management programs, can contribute substantially to improve results related to the diagnosis and characterization of LS.
Abbreviations
- HNPCC:
-
Hereditary non-polyposis colorectal cancer
- CRC:
-
Colorectal cancer
- MMR:
-
Mismatch repair gene
- LS:
-
Lynch syndrome
- ACI:
-
Amsterdam criteria I
- ACII:
-
Amsterdam criteria II
References
Woolf CM (1958) A genetic study of carcinoma of the large intestine. Am J Hum Genet 10(1):42–47
Lovett E (1976) Family studies in cancer of the colon and rectum. Br J Surg 63(1):13–18
Macklin MT (1960) Inheritance of cancer of the stomach and large intestine in man. J Natl Cancer Inst 24:551–571
Duncan JL, Kyle J (1982) Family incidence of carcinoma of the colon and rectum in north-east Scotland. Gut 23(2):169–171
Potter JD (1999) Colorectal cancer: molecules and populations. J Natl Cancer Inst 91(11):916–932
Warthin AS (1913) Heredity with reference to carcinoma as shown by the study of the cases examined in the pathological laboratory of the University of Michigan. Arch Int Med 12:546–555
Savage D (1956) A family history of uterine and gastro-intestinal cancer. Br Med J 2(4988):341–343
Kluge T (1964) Familial cancer of the colon. Acta Chir Scand 127:392–398
Lynch HT, Krush AJ (1971) Cancer family “G” revisited: 1895–1970. Cancer 27(6):1505–1511
Boland CR, Troncale FJ (1984) Familial colonic cancer without antecedent polyposis. Ann Intern Med 100(5):700–701
Ministry of Health/National Institute of Cancer-Inca (2010) Available from: http://www1.inca.gov.br/estimativa/2010/index.asp?link=tabelaestados.asp&UF=BR. Cited 1 May 2010
Geary J, Sasieni P, Houlston R et al (2008) Gene-related cancer spectrum in families with hereditary non-polyposis colorectal cancer (HNPCC). Fam Cancer 7(2):163–172
Lynch HT, Ens J, Lynch JF, Watson P (1988) Tumor variation in three extended Lynch syndrome II kindreds. Am J Gastroenterol 83(7):741–747
Lynch HT, Lynch JF (1993) The Lynch syndromes. Curr Opin Oncol 5(4):687–696
Lin KM, Shashidharan M, Ternent CA et al (1998) Colorectal and extracolonic cancer variations in MLH1/MSH2 hereditary non-polyposis colorectal cancer kindreds and the general population. Dis Colon Rectum 41(4):428–433
Watson P, Riley B (2005) The tumor spectrum in the Lynch syndrome. Fam Cancer 4(3):245–248
Vasen HF, Mecklin JP, Khan PM, Lynch HT (1991) The International Collaborative Group on Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC). Dis Colon Rectum 34(5):424–425
Vasen HF, Watson P, Mecklin JP, Lynch HT (1999) New clinical criteria for hereditary non-polyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology 116(6):1453–1456
Lynch HT, Smyrk TC, Watson P et al (1993) Genetics, natural history, tumor spectrum, and pathology of hereditary non-polyposis colorectal cancer: an updated review. Gastroenterology 104(5):1535–1549
Marra G, Boland CR (1995) Hereditary non-polyposis colorectal cancer: the syndrome, the genes, and historical perspectives. J Natl Cancer Inst 87(15):1114–1125
Lynch HT, Smyrk T (1996) Hereditary non-polyposis colorectal cancer (Lynch syndrome): an updated review. Cancer 78(6):1149–1167
Lynch HT, Smyrk T, Lynch J (1997) An update of HNPCC (Lynch syndrome). Cancer Genet Cytogenet 93(1):84–99
Peltomäki P, Vasen HF (1997) Mutations predisposing to hereditary non-polyposis colorectal cancer: database and results of a collaborative study. The International Collaborative Group on Hereditary Non-Polyposis Colorectal Cancer. Gastroenterology 113(4):1146–1158
Giardiello FM (1997) Genetic testing in hereditary colorectal cancer. JAMA 278(15):1278–1281
Bai YQ, Akiyama Y, Nagasaki H et al (1999) Predominant germ-line mutation of the hMSH2 gene in Japanese hereditary non-polyposis colorectal cancer kindreds. Int J Cancer 82(4):512–515
Kim JC, Kim HC, Roh SA et al (2001) hMLH1 and hMSH2 mutations in families with familial clustering of gastric cancer and hereditary non-polyposis colorectal cancer. Cancer Detect Prev 25(6):503–510
Rossi BM, Lopes A, Oliveira Ferreira F et al (2002) hMLH1 and hMSH2 gene mutation in Brazilian families with suspected hereditary non-polyposis colorectal cancer. Ann Surg Oncol 9(6):555–561
Oliveira Ferreira F, Napoli Ferreira CC, Rossi BM et al (2004) Frequency of extracolonic tumors in hereditary non-polyposis colorectal cancer (HNPCC) and familial colorectal cancer (FCC) Brazilian families: An analysis by a Brazilian Hereditary Colorectal Cancer Institutional Registry. Fam Cancer 3(1):41–47
Henderson TO, Amsterdam A, Bhatia S et al (2010) Systematic review: surveillance for breast cancer in women treated with chest radiation for childhood, adolescent, or young adult cancer. Ann Intern Med 152(7):444–455
Vasen HF, Morreau H, Nortier JW (2001) Is breast cancer part of the tumor spectrum of hereditary non-polyposis colorectal cancer? Am J Hum Genet 68(6):1533–1535
Westenend PJ, Schütte R, Hoogmans MM et al (2005) Breast cancer in an MSH2 gene mutation carrier. Hum Pathol 36(12):1322–1326
Risinger JI, Barrett JC, Watson P et al (1996) Molecular genetic evidence of the occurrence of breast cancer as an integral tumor in patients with the hereditary non-polyposis colorectal carcinoma syndrome. Cancer 77(9):1836–1843
Nelson CL, Sellers TA, Rich SS et al (1993) Familial clustering of colon, breast, uterine, and ovarian cancers as assessed by family history. Genet Epidemiol 10(4):235–244
de Leeuw WJ, van Puijenbroek M, Tollenaar RA et al (2003) Correspondence re: A. Müller et al., Exclusion of breast cancer as an integral tumor of hereditary non-polyposis colorectal cancer. Cancer Res., 62: 1014–1019, 2002. Cancer Res 63(5):1148–1149
Boyd J, Rhei E, Federici MG et al (1999) Male breast cancer in the hereditary non-polyposis colorectal cancer syndrome. Breast Cancer Res Treat 53(1):87–91
Scott RJ, McPhillips M, Meldrum CJ et al (2001) Hereditary non-polyposis colorectal cancer in 95 families: differences and similarities between mutation-positive and mutation-negative kindreds. Am J Hum Genet 68(1):118–127
Müller A, Edmonston TB, Corao DA et al (2002) Exclusion of breast cancer as an integral tumor of hereditary non-polyposis colorectal cancer. Cancer Res 62(4):1014–1019
Itoh H, Houlston RS, Harocopos C, Slack J (1990) Risk of cancer death in first-degree relatives of patients with hereditary non-polyposis cancer syndrome (Lynch type II): a study of 130 kindreds in the United Kingdom. Br J Surg 77(12):1367–1370
Watson P, Lynch HT (1993) Extracolonic cancer in hereditary nonpolyposis colorectal cancer. Cancer 71(3):677–685
Aarnio M, Sankila R, Pukkala E et al (1999) Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer 81(2):214–218
Jass JR (2000) Pathology of hereditary non-polyposis colorectal cancer. Ann NY Acad Sci 910:62–73
Jensen UB, Sunde L, Timshel S et al (2010) Mismatch repair defective breast cancer in the hereditary non-polyposis colorectal cancer syndrome. Breast Cancer Res Treat 120:777–782
Meijers-Heijboer H, Wijnen J, Vasen H et al (2003) The CHEK2 1100delC mutation identifies families with a hereditary breast and colorectal cancer phenotype. Am J Hum Genet 72(5):1308–1314
Parc Y, Boisson C, Thomas G et al (2003) Cancer risk in 348 French MSH2 or MLH1 gene carriers. J Med Genet 40(3):208–213
Aarnio M, Mecklin JP, Aaltonen LA et al (1995) Life-time risk of different cancers in hereditary non-polyposis colorectal cancer (HNPCC) syndrome. Int J Cancer 64(6):430–433
Vasen HF, Stormorken A, Menko FH et al (2001) MSH2 mutation carriers are at higher risk of cancer than MLH1 mutation carriers: a study of hereditary non-polyposis colorectal cancer families. J Clin Oncol 19(20):4074–4080
Watson P, Lynch HT (2001) Cancer risk in mismatch repair gene mutation carriers. Fam Cancer 1(1):57–60
Goodfellow PJ, Buttin BM, Herzog TJ et al (2003) Prevalence of defective DNA mismatch repair and MSH6 mutation in an unselected series of endometrial cancers. Proc Natl Acad Sci USA 100(10):5908–5913
Wagner A, Barrows A, Wijnen JT et al (2003) Molecular analysis of hereditary non-polyposis colorectal cancer in the United States: high mutation detection rate among clinically selected families and characterization of an American founder genomic deletion of the MSH2 gene. Am J Hum Genet 72(5):1088–1100
Franco EL, Villa LL, Ruiz A et al (1995) Transmission of cervical human papillomavirus infection by sexual activity: differences between low and high oncogenic risk types. J Infect Dis 172(3):756–763
Kjaer SK, Chackerian B, van den Brule AJ et al (2001) High-risk human papillomavirus is sexually transmitted: evidence from a follow-up study of virgins starting sexual activity (intercourse). Cancer Epidemiol Biomark Prev 10(2):101–106
Peyton CL, Gravitt PE, Hunt WC et al (2001) Determinants of genital human papillomavirus detection in a US population. J Infect Dis 183(11):1554–1564
Burchell AN, Winer RL, de Sanjosé S et al (2006) Chapter 6: epidemiology and transmission dynamics of genital HPV infection. Vaccine 24(Suppl 3):S52–S61
Goecke T, Schulmann K, Engel C et al (2006) Genotype-phenotype comparison of German MLH1 and MSH2 mutation carriers clinically affected with Lynch syndrome: a report by the German HNPCC Consortium. J Clin Oncol 24(26):4285–4292
Park YJ, Shin KH, Park JG (2000) Risk of gastric cancer in hereditary non-polyposis colorectal cancer in Korea. Clin Cancer Res 6(8):2994–2998
Zhang Y, Sheng J, Li S et al (2005) Clinical phenotype and prevalence of hereditary non-polyposis colorectal cancer syndrome in Chinese population. World J Gastroenterol 11(10):1481–1488
Lynch HT, Grady W, Suriano G et al (2005) Gastric cancer: new genetic developments. J Surg Oncol 90(3):114–133 (discussion 133)
Gayther SA, Gorringe KL, Ramus SJ et al (1998) Identification of germ-line E-cadherin mutations in gastric cancer families of European origin. Cancer Res 58(18):4086–4089
Guilford P, Hopkins J, Harraway J et al (1998) E-cadherin germline mutations in familial gastric cancer. Nature 392(6674):402–405
Bevan S, Houlston RS (1999) Genetic predisposition to gastric cancer. QJM 92(1):5–10
Gylling A, Abdel-Rahman WM, Juhola M et al (2007) Is gastric cancer part of the tumour spectrum of hereditary non-polyposis colorectal cancer? A molecular genetic study. Gut 56(7):926–933
Mueller-Koch Y, Vogelsang H, Kopp R et al (2005) Hereditary non-polyposis colorectal cancer: clinical and molecular evidence for a new entity of hereditary colorectal cancer. Gut 54(12):1733–1740
Wijnen J, Khan PM, Vasen H et al (1997) Hereditary nonpolyposis colorectal cancer families not complying with the Amsterdam criteria show extremely low frequency of mismatch-repair-gene mutations. Am J Hum Genet 61(2):329–335
Nyström-Lahti M, Wu Y, Moisio AL et al (1996) DNA mismatch repair gene mutations in 55 kindreds with verified or putative hereditary non-polyposis colorectal cancer. Hum Mol Genet 5(6):763–769
Katballe N, Juul S, Christensen M et al (2001) Patient accuracy of reporting on hereditary non-polyposis colorectal cancer-related malignancy in family members. Br J Surg 88(9):1228–1233
Murff HJ, Spigel DR, Syngal S (2004) Does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA 292(12):1480–1489
Liu B, Parsons R, Papadopoulos N et al (1996) Analysis of mismatch repair genes in hereditary non-polyposis colorectal cancer patients. Nat Med 2(2):169–174
Renkonen E, Zhang Y, Lohi H et al (2003) Altered expression of MLH1, MSH2, and MSH6 in predisposition to hereditary nonpolyposis colorectal cancer. J Clin Oncol 21(19):3629–3637
Lindor NM, Rabe K, Petersen GM et al (2005) Lower cancer incidence in Amsterdam-I criteria families without mismatch repair deficiency: familial colorectal cancer type X. JAMA 293(16):1979–1985
Lynch HT, Lynch PM, Lanspa SJ et al (2009) Review of the Lynch syndrome: history, molecular genetics, screening, differential diagnosis, and medicolegal ramifications. Clin Genet 76(1):1–18
Roy HK, Lynch HT (2003) Diagnosing Lynch syndrome: is the answer in the mouth? Gut 52(12):1665–1667
de la Chapelle A (2005) The incidence of Lynch syndrome. Fam Cancer 4(3):233–237
Acknowledgment
Supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
da Silva, F.C., de Oliveira, L.P., Santos, É.M. et al. Frequency of extracolonic tumors in Brazilian families with Lynch syndrome: analysis of a hereditary colorectal cancer institutional registry. Familial Cancer 9, 563–570 (2010). https://doi.org/10.1007/s10689-010-9373-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10689-010-9373-2