
Abstract
Waste remains a very complex problematic issue on human society due to its health and environmental effects, economic aspects and social impacts. Medical waste is in a special classification and is supposed to be more hazardous compared to municipal wastes. Therefore, collection, storage, transfer and disposal of medical waste need more delicate measures. These four cycles of waste handling comprise the waste management system. The amount of future medical waste is important in studies on waste management. In order to form an accurate strategy, the amount of waste that is generated must be known with high precision. Accurate estimation can help both planning and designing medical waste management systems. In the present work, a regression model was performed in order to estimate the amount of waste generated by the hospitals in Aksaray city. The inputs of the model were the patient number in three different age classes (0–15; 15–65; 65 <) and gross domestic product per capita. The model had very high determination coefficient of 0.979. This model provides important inputs to ready-to-use solutions to decision makers in medical waste management, which has dynamic conditions due to activities in health services.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Nowadays, one of the biggest problems of human society is the increase in waste amount and diversity due to environmental pollution and health hazards (Alam et al. 2019; Dehghani et al. 2019). The waste term covers all types of wastes from human and animal activities. One of the most hazardous among these wastes is medical waste. Medical waste is a special waste category which is very dangerous due to its infectious and/or toxic properties. This kind of waste is the second most hazardous after radioactive waste. Dangerous and contagious medical wastes can pose a serious threat to public and environmental health, as they can pollute the air and contaminate oil and water resources (Farzadkia et al. 2015; Dehghani et al. 2008).
Among the various types of wastes, healthcare waste, hospitals, research centers, the presence of various hazardous compounds and their harmful effects on healthcare materials and the surrounding population are very important (Vasistha et al. 2018; Ali and Jasim 2018; Shakiba and Mohagheghian 2018). With the increase in population and the shift of technology, the quantitative and qualitative properties of the wastes of healthcare services have changed and have become more toxic (Goyal et al. 2017; Yousefi and Rostami 2017). Medical wastes may contain highly toxic chemicals and may provide a medium for the transportation of diseases (Dehghanifard and Dehghani 2018). The worldwide growth of the medical sector in the last decade (Najafi et al. 2017; Mantzaras and Voudrias 2017) has substantially contributed to an increase in medical waste production with an increase in the use of disposable medical products (Haregu et al. 2017). Medical wastes include highly toxic chemicals, toxic metals, pathogenic viruses and bacteria that can lead to pathological dysfunction on the human body (Mazloomi et al. 2019, Zamparas et al. 2019). Medical waste poses a high risk for physicians, nurses, technicians, sweepers, hospital visitors and patients for arbitrary use and management (Tchobanoglous 1993; Mohammed and Elias 2017; Duca and Mereuta 2017). According to European Union, medical waste items are those related to the chapter 18 of the European Waste Catalogue, defined as the wastes from human or animal health care and/or related investigation, while in the USA, the Medical Waste Tracking Act of 1988 identifies medical waste as ‘any solid waste that is created in the diagnosis, treatment, or immunization of human beings or animals, in study pertaining thereto, or in the production or testing of biologicals.’ In Turkey, medical waste is defined as infectious, pathological and sharp objects originating from the healthcare sector. The explanation of medical waste can vary meaningfully among countries.
General statistics on the production of hospital waste per daybed are as follows: the UK—2.5 kg, USA—4.5 kg, France—2.3 kg, India—1.5 kg (Blenkharn 2006; Mühlich et al. 2003; Patil and Shekdar 2001). There is increasing investment in the health sector in Turkey. Therefore, the medical waste generation trend was as follows: 0.43 kg/daybed in 2000 (Korkut 2018); 0.63 kg/daybed in 2009 (Birpinar et al. 2009); and 1.68 kg/daybed in 2017 (Korkut 2018). Waste generation within different years must be accurately estimated in order to constitute a successful medical waste management system.
Aksaray is a developing city with a rapidly growing urban population, extensive health problems, environmental pollution and low educational status relative to other cities in Turkey. The surface area of the province is 7.991 km2. According to the Turkish Statistical Institute (TÜİK) data, the population of Aksaray was 402.404 in 2017. Of the population, 289,778 live in city center and districts, while 112,626 live in villages and towns.
In order to develop proper waste management strategies, it is important to characterize the waste amount and composition of the waste stream. In some circumstances, it is not possible to estimate waste formation due to term-based formation of the wastes (Abdulredha et al. 2018). However, waste amount projection is mandatory when able, in order to increase management capacity. The quantity of medical waste depends upon several factors such as the size of healthcare facility, the segregation program of medical wastes and type of the medical activities (Hassan et al. 2008). Therefore, in this study, we aimed to (1) evaluate the medical waste trend that is originated from hospitals in Aksaray, Turkey, and (2) propose an estimation model for medical waste generation, which is mandatory for accurate future waste management strategy.
2 Materials and methods
This is a hospital-based cross-sectional study to assess the waste management system in all hospitals of Aksaray and to develop a waste estimation model. Aksaray is located in the central Anatolia, and the gender share of the population is as follows: 200,233 males and 202,171 females. There are two hospitals in Aksaray including one public hospital and one private hospital providing health facilities at the second and third levels of prevention. A general hospital contains all disciplines, which are internal medicine section, surgery department, psychiatric, neurological diseases, blood diseases, oncology treatment, women’s section, children’s section, laboratories, as well as emergency and the private section.
In Turkish healthcare system, collection, handling, transfer and disposal of medical waste are regulated according to Medical Waste Control Legislation, which was last amended on January 25, 2017 (MWCR 2017). According to the aforementioned legislation, the wastes from healthcare units are classified as follows: (1) general wastes, (2) infectious wastes, (3) genotoxic waste, (4) pathological wastes, (5) sharp wastes and (6) hazardous wastes. Infectious, pathological and sharp wastes are defined as medical waste.
According to the Aksaray municipality, approximately 280 tons of medical waste was generated from both state and private health facilities in 2017. Collection, handling and transfer of the medical wastes are conducted according to MWCR (2017). Therefore, we intended to give a short summary of the whole process due to the fact that those steps are integral part of our methods section. Red bags made of medium-density polyethylene, having an international ‘biohazard’ sign in the middle, are used in the collection of medical wastes. Sharp wastes are collected in a plastic container. Liquid medical wastes are concentrated with appropriate sorption materials. Then, the containers and bags are transferred to a temporary storage area. Weigh process is repeated at each step (from transfer until disposal) following the collection of medical waste. The production amount and sources of medical wastes from two hospitals in Aksaray, treatment methods and disposal, and cost-effective waste flow analysis methods were investigated in this study. Among 81 cities in Turkey, Aksaray remained in the middle of population list. Therefore, the city population characteristics were used to represent most Turkish cities.
2.1 Waste amount prediction model
Modeling section is a crucial and integral part of the waste management system. Al-Khatib et al. (2015) applied a system dynamics model in order to predict both waste amount and disposal costs. A multiregression model was applied to determine the medical waste amount in Palestine (Al-Khatib et al. 2016). Similarly, Bel and Mur (2009) applied multivariable regression analysis for solid waste management in industrialized countries. Beigl et al. (2008) stated that multivariate methods are complicated due to the relation among the parameters. Furthermore, it is difficult to validate the multivariate models (Beigl et al. 2008). The linear regression technique is successful in waste generation estimation and widely used for that purpose (Hoang et al. 2017). Multiple linear regression (MLR) is a frequently used method by diverse disciplines to examine the case where a variable is influenced by more than one independent variables. The form of the general equation is shown in Eq. (1):
In the above equation, y is a dependent variable, which changes by alterations of independent variables. Independent variables are shown as x1, x2,…, xn. The a value is a constant and b, c,…, z values are coefficients. Coefficients link the relationship between dependent and independent variables. Sign (as negative and positive) of the coefficients gives information about how the independent variables affect the dependent variable.
3 Results and discussion
3.1 Evaluation of medical waste management in Aksaray
It is important to have accurate information about the production rate of medical wastes in order to develop a sustainable medical waste management system. It depends on various factors such as bed occupancy ratio, separate collection program of medical wastes, location of the facility, type of health facility and type of services provided. The hospital waste is considered to be a medical waste, and 10–15% of hospital wastes are considered as contagious (USC 1988). It is clear that the amount of medical waste collected by the Aksaray medical waste sterilization plant, which started to accept waste in 2011, has increased consistently.
Age classification of the patients stands crucial as the age distribution usually determines the treatment type. High disease rates are observed in the first decade of life. However, the aging factor should cause a significant increase in disability days due to disease, because the average duration of the disease increases with age. Diseases are more common in childhood. Therefore, when an increase in chronic diseases occurs, the disability rate is relatively low before middle and old age (Ezzati et al. 2002).
As can be seen from Table 1, the birth rate in Aksaray is varying but the net trend is toward decreasing and the number of people in the middle ages increases. For this reason, the number of polyclinic admission rates increased regularly between 2011 and 2017 (Fig. 1). However, the only reason for this increase is not the increase in the population of elderly people. The investment in the healthcare sector and the introduction of the online technologies, which lead to ease of hospital admissions, seem to elevate the number of people who make hospital admissions. Besides, as the education level increases, the awareness of diseases increases and in turn hospital admissions increase (Birpinar et al. 2009).

Number of outpatients change by time
The polyclinic admission number turned to be steady after 2014. This is due to the reduction in the number of people benefiting from free health services. The Green Card system, which provided free access to health service by the state to the poor citizens, was lifted in 2014. Instead, a new system called compulsory health insurance was introduced. Thus, the number of people benefiting from free health services has decreased.
The increase in the inpatient number was analogical to clinical patient number. But after 2014, the trend of inpatient number was decreasing. In recent years, the hospitalization rates of patients have decreased. The main reason for this is the widespread use of outpatient health services, including surgical and interventional procedures in outpatient settings. Complex procedures and operations are possible in outpatient facilities because of new medical technologies that prevent complications such as minimally invasive surgical techniques, new anesthesia and pain control techniques and enable patients to return home more quickly. It raised healthcare costs but contributed to the transition from inpatient to outpatient care. The whole trend is shown in Fig. 2.

Number of hospitalized patients
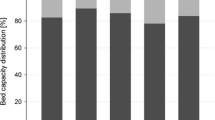
Hospital bed occupancy ratios are an important indicator of a hospital’s ability to properly care for patients. The summary statistics of the number of beds and bed occupancy in hospitals in Aksaray are shown in Fig. 3.

Bed occupancy rate and bed number in hospitals
The bed occupancy ratio and the number of beds are presented separately for the state and private hospital. The number of beds increased at about 50% in the state hospital between 2011 and 2013. A 25% increase in the number of beds was present at the private hospital after 2013. In 2017, there were 605 beds in the hospitals in Aksaray. As a result of the studies, the number of hospital beds has increased and the demand has been met. Two opposite trends in total bed number and inpatient number yielded reduced bed occupancy ratio in Aksaray (Figs. 2, 3).
Figure 4 shows that the quantity of medical waste from the hospitals was about 760 kg/day, representing an average waste production rate of 1.3 kg/bed-day in 2017.

Gross medical waste amount and waste amount per bed-person
Several medical waste generation rates around the world are given in Table 2.
The highest waste generation can be sorted as follows: USA > Italy > Portugal > Iran > France. These countries have a rate of higher than 3 kg/bed/day. However, some countries had variable values among different hospitals. The waste generation rate below 1 kg/bed/day was in India, Peru, Jordan Tanzania, in the ascending order. In some parts of India, the rate was 2 kg/bed/day. The closest waste generation rate to Aksaray was in Vietnam with 1.42 kg/bed/day. Eker and Bilgili (2011) conducted a study in the biggest city in Turkey. They reported a waste rate of 2.11 kg/bed/day in Istanbul. Higher waste generation rate than Aksaray was observed in Istanbul due to its economic development. The waste generation rates in Pakistan and Greece were close to those of Istanbul.
3.2 Medical waste estimation
The available data were age classification, gross domestic product, number of polyclinics, number of beds and number of inpatients. Age classification and gross domestic product per capita were chosen to be the best indicators in order to estimate the medical waste amount. Three major groups were formed for age classification. The groups were 0–15, 15–65 and > 65 ages. The gross national product was in US dollars ($). The independent variables are given in Table 1.
The multiple linear regression equation generated by the values in Table 1 is given as Eq. (2):
where x1, x2, and x3 are age classes of 0–15, 15–65 and > 65, respectively. x4 is the gross domestic product. The relation was statistically significant (p < 0.05). The adjusted R2 of the model was 0.94, which means 94% of the independent variable can be explained by the dependent variable. The standard error of the model was 9.9. The regression had extremely high determination coefficient (0.979) as shown in Fig. 5.

Plot of actual and predicted waste amount
Further statistical indicators were used to test the performance of the proposed model. The exploited indicators were factor of two (FA2), index of agreement (IA), mean bias error (MBE) and mean absolute percentage error (MAPE). Equations of the statistical indicator are given as Eqs. (3), (4), (5) and (6):
where \(O_{i}\), \(\bar{O}\) and \(P_{i}\) are observed value, mean observed value and predicted value, respectively. FA2 gives the percentage of predicted cases in which observed-to-predicted ratio is between 0.5 and 2 (Agirre-Basurko et al. 2006). FA2 value close to the unity shows the best estimate. FA2 varied between 0.94 and 1.04 with a mean of 1.00. IA ranges between 0 and 1, which is a standardized measure of the degree of the model estimation error (Willmott 1981). The values close to the unity show the perfect estimation. IA was calculated as 0.995, which showed a very good model performance. MBE is used to understand whether the prediction is overestimated or underestimated. The calculated MBE was − 0.014, which showed that the mean predicted values were slightly higher than the mean observed values. MAPE calculates the extent of the error in percentage. MAPE was 2.2%, which showed a low error level.
Hocket et al. (1995) applied regression models for statistical analysis of per capita waste generation that is expressed by demographic, economic and structural determinants. Their study concluded that the per capita purchase of goods and waste treatment fees were effective parameters of waste generation; on the other hand, demographic factors did not affect waste production. According to Thøgersen (1996), gross domestic product (GDP) per capita explained 50% of the variations in per capita waste generation in 18 OECD countries. The linear regression analyses in his study showed that there was a considerable correlation between GDP per capita and waste produced per capita. Previously, the estimation of medical waste generation was executed by artificial neural network (ANN) and MLR by Jahandideh et al. (2009). In that study, ANN (R2 = 0.99) had a higher prediction capacity than MLR (R2 = 0.99). Su and Chen (2018) applied environmental Kuznets curve (EKC) model to estimate medical waste amount. The EKC model had a low determination coefficient (R2 = 0.6269). This study had a higher determination coefficient than EKC model in Su and Chen (2018) and MLR model in Jahandideh et al. (2009). The reason for the high estimation potential can be attributed to the generalizability of the selected independent variables. Therefore, this model can be applied in a broader sense.
4 Conclusion
There is a great need to create and implement an appropriate medical waste management program to control and improve the current situation in the mid-populated city of Aksaray. Accurate estimation of the rate of production of medical waste plays an important role in the hospital waste management system. Sustainable management of medical wastes can only be implemented only if a precise waste prediction is made, unless investment in the sector would be inefficient. Therefore, the purpose of this research was to provide a suitable model for estimating the generated waste amount. The discovered results are promising and can play a useful role in establishing an appropriate medical waste management system in health care. In particular, age-class distribution data and GDP per capita are proved to be significant determinants of waste production.
References
Abdulla, F., Qdais, H., & Rabi, A. (2008). Site investigation on medical waste management practices in northern Jordan. Waste Management, 28, 450–458. https://doi.org/10.1016/j.wasman.2007.02.035.
Abdulredha, M., Kot, P., Al Khaddar, R., Jordan, D., & Abdulridha, A. (2018). Investigating municipal solid waste management system performance during the Arba’een event in the city of Kerbala, Iraq. Environment, Development and Sustainability. https://doi.org/10.1007/s10668-018-0256-2.
Agirre-Basurko, E., Ibarra-Berastegi, G., & Madariaga, I. (2006). Regression and multilayer perceptron-based models to forecast hourly O3 and NO2 levels in the Bilboa area. Environmental Modelling and Software, 21, 430–446. https://doi.org/10.1016/j.envsoft.2004.07.008.
Alam, I., Alam, G., Ayub, S., & Siddiqui, A. A. (2019). Assessment of bio-medical waste management in different hospitals in Aligarh city. In A. Kalamdhad, J. Singh, & K. Dhamodharan (Eds.), Advances in Waste Management (pp. 501–510). Singapore: Springer. https://doi.org/10.1007/978-981-13-0215-2_36.
Ali, S. K., & Jasim, D. T. (2018). Assessment of medical solid waste generation rates for teaching hospitals in Baghdad city, Association of Arab Universities. Journal of Engineering Science, 25(1), 160–169. https://doi.org/10.1007/978-981-13-0215-2_36.
Al-Khatib, I. A., Eleyan, D., & Garfield, J. (2015). A system dynamics model to predict municipal solid waste generation and management costs in developing areas. The Journal of Solid Waste Technology and Management, 41(2), 109–120. https://doi.org/10.5276/JSWTM.2015.109.
Al-Khatib, I. A., Fkhidah, I. A., Khatib, J. I., & Kontogianni, S. (2016). Implementation of a multi-variable regression analysis in the assessment of the generation rate and composition of hospital solid waste for the design of a sustainable management system in developing countries. Waste Management and Research, 34(3), 225–234. https://doi.org/10.1177/07342242X15622813.
Askarian, M., Vakili, M., & Kabir, G. (2004). Results of a hospital waste survey in private hospitals in Fars province, Iran. Waste Management, 24(4), 347–352. https://doi.org/10.1016/j.wasman.2003.09.008.
Bdour, A., Altrabsheh, B., Hadadin, N., & Al-Shareif, M. (2007). Assessment of medical wastes management practice: A case study of the northern part of Jordan. Waste Management, 27(6), 746–759. https://doi.org/10.1016/j.wasman.2006.03.004.
Beigl, P., Lebersorger, S., & Salhofer, S. (2008). Modelling municipal 400 M.G. solid waste generation: A review. Waste Management, 28(1), 200–214. https://doi.org/10.1016/j.wasman.2006.12.011.
Bel, G., & Mur, M. (2009). Intermunicipal cooperation, privatization and waste management costs: Evidence from rural municipalities. Waste Management, 29(10), 2772–2778. https://doi.org/10.1016/j.wasman.2009.06.002.
Birpinar, M. E., Bilgili, M. S., & Erdogan, T. (2009). Medical waste management in Turkey: A case study of Istanbul. Waste Management, 29, 445–448. https://doi.org/10.1016/j.wasman.2008.03.015.
Blenkharn, J. I. (2006). Standards of clinical waste management in UK hospitals. Journal of Hospital Infection, 62(3), 300–303. https://doi.org/10.1016/j.jhin.2005.08.005.
Dehghani, M. H., Ahrami, H. D., Nabizadeh, R., Heidarinejad, Z., & Zarei, A. (2019). Medical waste generation and management in medical clinics in South of Iran. MethodsX, 6, 727–733. https://doi.org/10.1016/j.mex.2019.03.029.
Dehghani, M. H., Azam, K., Changani, F., & Fard, E. D. (2008). Assessment of medical waste management in educational hospitals of Tehran university medical sciences. Journal of Environmental Health Science & Engineering, 5(2), 131–136.
Dehghanifard, E., & Dehghani, M. H. (2018). Evaluation and analysis of municipal solid wastes in Tehran, Iran. MethodsX, 5, 312–321.
Diaz, L. F., Eggerth, L. L., Enkhtsetseg, S. H., & Savage, G. M. (2008). Characteristics of healthcare wastes. Waste Management, 28(7), 1219–1226. https://doi.org/10.1016/j.wasman.2007.04.010.
Duca, G., & Mereuţa, A. (2017). Solid Waste Management in the Republic of Moldova. In International conference on management science and engineering management (pp. 1283–1295). Springer, Cham. https://doi.org/10.1007/978-3-319-59280-0_107.
Eker, H. H., & Bilgili, M. S. (2011). Statistical analysis of waste generation in healthcare services: A case study. Waste Management and Research, 29(8), 791–796. https://doi.org/10.1177/0734242X10396755.
Ezzati, M., Lopez, A. D., Rodgers, A., Vander Hoorn, S., Murray, C. J., & Comparative Risk Assessment Collaborating Group. (2002). Selected major risk factors and global and regional burden of disease. The Lancet, 360(9343), 1347–1360. https://doi.org/10.1016/S0140-6736(02)11403-6.
Farzadkia, M., Emamjomeh, M. M., Golbaz, S., & Sajadi, H. S. (2015). An investigation on hospital solid waste management in Iran. Global NEST Journal, 17(4), 771–783.
Goyal, K. C., Goyal, S. N., & Goyal, R. (2017). Analysis of bio-medical waste management in private hospital at Patiala State of Punjab, India. Octa Journal of Environmental Research, 5(1), 001–005.
Haregu, T. N., Ziraba, A. K., Aboderin, I., Amugsi, D., Muindi, K., & Mberu, B. (2017). An assessment of the evolution of Kenya’s solid waste management policies and their implementation in Nairobi and Mombasa: Analysis of policies and practices. Environment and Urbanization, 29(2), 515–532. https://doi.org/10.1177/0956247817700294.
Hassan, M. M., Ahmed, S. A., Rahman, K. A., & Biswas, T. K. (2008). Pattern of medical waste management: Existing scenario in Dhaka city, Bangladesh. BMC Public Health, 8(1), 36. https://doi.org/10.1186/1471-2458-8-36.
Hoang, M. G., Fujiwara, T., Pham Phu, S. T., & Nguyen Thi, K. T. (2017). Predicting waste generation using Bayesian model averaging. Global Journal of Environmental Science Management, 3(4), 385–402. https://doi.org/10.22034/gjesm.2017.03.04.005.
Hocket, D., Lober, D. J., & Pilgrim, K. (1995). Determinants of per capita municipal solid waste generation in the Southeastern United States. Journal of the Environmental Management, 45(3), 205–217. https://doi.org/10.1006/jema.1995.0069.
Jahandideh, S., Jahandideh, S., Asadabadi, E. B., Askarian, M., Movahedi, M. M., Hosseini, S., et al. (2009). The use of artificial neural networks and multiple linear regression to predict rate of medical waste generation. Waste Management, 29, 2878–2879. https://doi.org/10.1016/j.wasman.2009.06.027.
Kerdsuwan, S. (2000). Case study of using hospital waste incinerator in Thailand. In Proceedings of the 93rd annual meeting and exhibition.
Korkut, E. N. (2018). Estimations and analysis of medical waste amounts in the city of Istanbul and proposing a new approach for the estimation of future medical waste amounts. Waste Management, 81, 168–176. https://doi.org/10.1016/j.wasman.2018.10.004.
Lee, B. K., Ellenbecker, M. J., & Moure-Ersaso, R. (2004). Alternatives for treatment and disposal cost reduction of regulated medical wastes. Waste Management, 24(2), 143–151. https://doi.org/10.1016/j.wasman.2003.10.008.
Mantzaras, G., & Voudrias, E. A. (2017). An optimization model for collection, haul, transfer, treatment and disposal of infectious medical waste: Application to a Greek region. Waste Management, 69, 518–534. https://doi.org/10.1016/j.wasman.2017.08.037.
Mazloomi, S., Zarei, A., Alasvand, S., Farhadi, A., Nourmoradi, H., & Bonyadi, Z. (2019). Analysis of quality and quantity of health-care wastes in clinical laboratories: A case study of Ilam city. Environmental Monitoring and Assessment, 191(4), 207.
Mohammed, A., & Elias, E. (2017). Domestic solid waste management and its environmental impacts in Addis Ababa city. Journal of Environmental and Waste Management, 4(1), 194–203. https://doi.org/10.1007/s12665-011-1480-3.
Mühlich, M., Scherrer, M., & Daschner, F. D. (2003). Comparison of infectious waste management in European hospitals. Journal of Hospital Infection, 55(4), 260–268. https://doi.org/10.1016/j.jhin.2003.08.017.
MWCR (2017). Medical Waste Control Regulation, Turkey Ministry of Environment and Forestry. Official Gazette No: 29959. Ankara, Turkey.
Najafi, A., Hallaji, S. M., Saleh, E., Hashemolhosseini, N., & Pootehrigi, M. (2017). Analysis of waste management in Zahedan City and assessment of the municipality’s performance (case region: Zahedan). Journal of Applied Environmental Bioscience, 7(7), 9–18. https://doi.org/10.1006/jema.2001.0453.
Patil, A. D., & Shekdar, A. V. (2001). Health-care waste management in India. Journal of Environmental Management, 63(2), 211–220. https://doi.org/10.1006/jema.2001.0453.
Prüss-Üstün, A., & Townend, W. K. (1999). Safe management of wastes from health-care activities. Geneva: World Health Organization.
Shakiba, M., & Mohagheghian, A. (2018). Hospital waste generation and management status in Rasht, north of Iran. Caspian Journal of Health Research, 3(1), 20–23. https://doi.org/10.1016/j.wasman.2012.09.008.
Su, E. C. Y., & Chen, Y. T. (2018). Policy or income to affect the generation of medical wastes: An application of environmental Kuznets curve by using Taiwan as an example. Journal of Cleaner Production, 188, 489–496. https://doi.org/10.1016/j.jclepro.2018.04.011.
Tchobanoglous, G. (1993). Integrated solid waste management engineering principles and management issues (No. 628 T3).
Thøgersen, J. (1996). Wasteful food consumption: Trends in food and packaging waste. Scandinavian Journal of Management, 1(3), 291–304. https://doi.org/10.1016/0956-5221(96)00011-5.
Tsakona, M., Anagnostopoulou, E., & Gidarakos, E. (2007). Medical waste management and toxicity evaluation: A case study. Waste Management, 27, 912–920. https://doi.org/10.1016/j.wasman.2006.04.019.
United Nations Environment Programme. (2012). Compendium of technologies for treatment/destruction of healthcare waste (Osaka).
Vasistha, P., Ganguly, R., & Gupta, A. K. (2018). Biomedical waste generation and management in public sector hospital in Shimla City. In V. Singh, S. Yadav, & R. Yadava (Eds.), Environmental Pollution (pp. 225–232). Singapore: Springer. https://doi.org/10.1007/978-981-10-5792-2_19.
Willmott, C. J. (1981). On the validation of the models. Physical Geography, 2(2), 184–194. https://doi.org/10.1080/02723646.1981.10642213.
Yousefi, Z., & Rostami, M. A. (2017). Quantitative and qualitative characteristics of hospital waste in the city of Behshahr-2016. Environmental Health Engineering and Management. https://doi.org/10.15171/ehem.2017.09.
Zamparas, M., Kapsalis, V. C., Kyriakopoulos, G. L., Aravossis, K. G., Kanteraki, A. E., Vantarakis, A., et al. (2019). Medical waste management and environmental assessment in the Rio University Hospital, Western Greece. Sustainable Chemistry and Pharmacy, 13, 100163. https://doi.org/10.1016/j.scp.2019.100163.
Acknowledgements
The authors wish to thank all who assisted in conducting this work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Çetinkaya, A.Y., Kuzu, S.L. & Demir, A. Medical waste management in a mid-populated Turkish city and development of medical waste prediction model. Environ Dev Sustain 22, 6233–6244 (2020). https://doi.org/10.1007/s10668-019-00474-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10668-019-00474-6