
Abstract
The aquatic environment is under increased pressure by pharmaceutically active compounds (PhACs) due to anthropogenic activities. In spite of being found at very low concentrations (ng/L to μg/L) in the environment, PhACs represent a real danger to aquatic ecosystems due to their bioaccumulation and long-term effects. In this study, the presence in the aquatic environment of six non-steroidal anti-inflammatory drugs (ibuprofen, diclofenac, acetaminophen, naproxen, indomethacin, and ketoprofen), caffeine, and carbamazepine were monitored. Moreover, their aquatic risk and ecotoxicity by three biological models were evaluated. The monitoring studies performed in Romania showed that all studied PhACs were naturally present at concentrations >0.01 μg/L, pointing out the necessity to perform further toxicity tests for environmental risk assessment. The toxicity studies were carried out on aquatic organisms or bacteria and they indicated, for most of the tested PhACs, an insignificant or low toxicity effects: lethal concentrations (LC50) on fish Cyprinus carpio ranged from 42.60 mg/L to more than 100 mg/L; effective concentrations (EC50) on planktonic crustacean Daphnia magna ranged from 11.02 mg/L to more than 100 mg/L; inhibitory concentrations (IC50)/microbial toxic concentrations (MTC) on Vibrio fischeri and other bacterial strains ranged from 7.02 mg/L to more than 100 mg/L. The PhAC aquatic risk was assessed by using the ratio between measured environmental concentration (MEC) and predicted no effect concentration (PNEC) calculated for each type of organism. The average of quotient risks (RQs) revealed that the presence of these compounds in Romania’s aquatic environment induced a lower or moderate aquatic risk.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The continuous increase of the human population has been associated to a tremendous increase of the amount and structural diversity of the chemical compounds released into the environment. A wide range of pharmaceutically active compounds (PhACs) have been detected in the surface waters (Christen et al. 2010), raising the concern about their harmful effects on the biological systems (Fernández et al. 2014). Unfortunately, PhACs are continuously introduced into the aquatic environment by various industrial or domestic wastewater sources (Kümmerer 2008), such as intensive medical practices (Bound and Voulvoulis 2006), expired drugs, intensive farming, and aquaculture (Wollenberger et al. 2000). Moreover, ingested PhACs are not completely metabolized and they are returned into the environment via Waste Water Treatment Plant (WWTP) effluents as parent compounds, metabolites, and/or conjugates secreted by bodily functions (urine and feces). For instance, approximately 72 % of the usually administered carbamazepine is absorbed by the human body, and the remaining 28 % is eliminated in unchanged chemical form through feces (Zhang et al. 2008). On the other hand, numerous studies conducted worldwide reported an occurrence of over 80 PhACs (concentrations ranging from 0.017 ng/L to 30 μg/L) in most rivers and lakes from Germany, Spain, China, Taiwan, Korea, Kenya, Finland, Sweden, and Portugal (Wiegel et al. 2004; Bendz et al. 2005; Kim et al. 2007a, b; Kim and Aga 2007; Vieno et al. 2007; Peng et al. 2008; Chen et al. 2008; Zhao et al. 2009; Madureira et al. 2010; Valcárcel et al. 2011, 2013; Koreje et al. 2012). In Romania, the total consumption of the most commonly used PhACs was estimated at more than 100 t/year. The consumption for analgesic compounds such as diclofenac, acetaminophen, and ibuprofen was estimated to more than 2–3 t/year per 19 million permanent inhabitants in 2012 (www.anm.ro, accessed in June 2015). The PhAC consumption in Romania increased 71 % during the last 10 years, but still, it is fourfold lower compared to other European countries (www.antibiotice.ro, accessed in June 2016).
Accordingly, more chemical compounds are discharged to the environment increasing the probability to induce harmful effects on living organisms and subsequently affecting the ecosystems (Bound and Voulvoulis 2006; Tsiaka et al. 2013). PhAC biodegradation studies reported low removal efficiencies by activated sludge from WWTPs (Stuer-Lauridsen et al. 2000; Kosjek 2006; Gartiser et al. 2007; Homem and Santos 2011; Muhammad et al. 2013). As a consequence, a large percentage of PhACs is released and could accumulate into the aquatic environment posing an ecological risk for the natural water reservoirs.
In this context, worldwide organizations, such as the European Medicines Evaluation Agency (EMEA) and the US Food and Drug Administration (FDA), have developed and implemented various environmental risk assessment guidelines (Fent et al. 2006) for the safety of the ecosystems. The Drugs Environmental Risk Assessment (ERA) was stipulated by EU Directive 93/39/EEC amending Directive 65/65/EEC and by the Guideline of Environmental Risk Assessment of medicinal products for human use (Straub 2001; EMEA 2006). The EU Commission through European Centre for the Validation of Alternative Methods (ECVAM) recommend for acute toxicity detection of new and existing chemicals, including pesticides and PhACs, the “Step-down approach” by unravelling new strategies based initially on small testing organisms such as crustacean, algae, or bacteria. In the second phase, the testing organisms are upgraded to fish only for the upper threshold concentration (UTC) of the first tested organisms (ESAC 2005). According to OECD, EPA, and ISO testing methodologies, current evaluation of PhAC toxicity effects on aquatic biota requires short-term exposure (24–96 h) for serial PhAC concentrations (Gheorghe et al. 2010; Nita-Lazar et al. 2016).
At the present, the researches focus on the fate and effects of PhACs in the aquatic environment (Tsiaka et al. 2013) and it is based on multichannel approaches such as (i) compound detection and concentration determination; (ii) identification of the pollution source as well as the evacuation routes into environment; and (iii) evaluation of the toxic effects of PhACs on aquatic organisms at different trophic levels (microorganisms, invertebrate, vertebrate, and plants).
The scientific community as well as the European Commission composed a list of priority substances which is regularly upgraded under Water Framework Directive (WFD 2000/60/EC). Recently, a “watch list” of 12 new emerging pollutants that could be added to the priority list was composed. For the first time, the watch list included three pharmaceutical compounds, diclofenac (a commonly used generic painkiller which is suspected for fish mortality) and two hormones (17 alpha-ethinylestradiol and 17 beta-estradiol), which can disrupt the endocrine system in humans and harm fish reproduction (EU Directive 2013).
The aim of the present work was to monitor the input of PhACs from three major WWTP stations into four Romanian surface water rivers and subsequently to study their toxic effects on these surface waters. We assessed the toxic effect of the most eight frequently used PhACs (six analgesics, one antiepileptic drug, and one nervous stimulant) on different aquatic organisms (fish, crustacean, and bacteria). Moreover, this study, based on our experimental monitoring and toxicity data, intended to correlate the aquatic risk of these PhACs on three Romanian surface waters with the International Guidelines for Risk Assessment.
To our knowledge, this is the first study of PhAC risk assessment in Romania providing valuable information for future environmental and human risk studies.
Material and methods
Chemicals and materials
PhACs selected for this study (Table 1) were purchased from Sigma-Aldrich (Seelze, Germany) and their standards had a purity higher than 98 %. HPLC-grade methanol, acetonitrile, and sodium hydroxide were supplied by Sigma-Aldrich (Steinheim, Germany). EDTA disodium salt (Na2-EDTA) and hydrochloric acid (HCl) were purchased from Merck (Darmstadt, Germany). Reagent-grade formic acid (99.9 % purity) was supplied by Agilent Technologies (CA, USA). HPLC-grade water was obtained with a Simplicity UV ultrapure water system from Millipore (Milford, MA, USA). Individual stock standard solutions of 500–1000 mg/L were prepared in methanol and stored in amber glass vials at −18 °C. Working solutions (containing a mixture of all analysts) were freshly prepared in methanol and stored at 4 °C.
Sampling
Wastewater samples were collected monthly during 2014 from Pitesti, Brasov, and Targu Mures WWTPs (influents and effluents) as well as from upstream and downstream WWTP surface waters such as Ghimbasel Stream (Brasov town area), Mures River (Targu Mures town area), and Arges River (for Pitesti town area). In addition, water samples were collected from different sites on Danube River (Romanian sector) and Danube Delta (Sf. Gheorghe Branch): Bazias, Giurgiu, Tulcea, Mahmudia, Uzlina, Murighiol, Sf. Gheorghe, and Black Sea Confluence.
Analytical procedure
The occurrence of the tested PhACs from environment samples was detected using the following two analytical methods.
LC-UV analysis
The LC-UV method was used to detect diclofenac, acetaminophen, ketoprofen, indomethacin, naproxen, and ibuprofen. The chromatographic protocol was modified and adapted from an analytical method previously developed and described elsewhere (Santos et al. 2005). Liquid-chromatographic separation of selected PhACs was investigated by using an Agilent 1100 (Agilent Technologies, USA) system equipped with a degasser, quaternary pump, autosampler, column thermostat, and multiple wavelength detectors (MWDs). The separations were performed on a LiChrosphere® 100 RP-18 analytical column (125 mm length, 4 mm i.d; 5 μm particle size) acquired from Merck (Darmstadt, Germany) and protected by a LiChrosphere® 100 RP-18 (4 mm × 4 mm i.d., 5 μm) guard column. System control and data acquisition were controlled by an Agilent ChemStation program. The mobile phase (1 mL/min) was a gradient of 50-mM potassium dehydrogenate phosphate in water (pH 4.6) (solvent A) and acetonitrile (solvent B). The HPLC separations were carried out at 25 °C and the MWD detection was performed at 254 nm. Sample treatment was based on solid phase extraction (SPE) using Oasis HLB (60 mg, 3 mL; Waters, Milford, MA, USA) extraction cartridge. Before extraction, the surface and wastewater samples were filtered through 1.6-μm Whatman glass fiber filters to remove any solid particulates, and then, the samples were adjusted to pH = 2 with hydrochloric acid (2 M) in order to prevent the analytes from taking their ionic form. Oasis HLB cartridges were conditioned with 3 mL of ethyl acetate, 3 mL of methanol, and 3 mL of acidified water (pH 2) at a flow rate of 5 mL/min. After loading the sample (1000 mL at 10 mL/min) and subsequent washing with 5 mL of HPLC water at 5 mL/min, the cartridges were dried under vacuum for 30 min. The elution of PHCs was performed with 3 mL of ethyl acetate at a flow rate of about 1 mL/min. The extract was evaporated to dryness in a nitrogen stream and finally reconstituted in 1 mL of methanol and injected into the HPLC system.
HPLC-MS/MS analysis
This analytical procedure for carbamazepine and caffeine was developed based on the EPA Method 1694 (USEPA 2007) with some modifications. Before extraction, water samples were filtered through 1.6-μm glass fiber filters (Whatman, Maidstone, UK). In the filtered aliquots of wastewater (100 mL for influent and 250 mL for effluent), Na2EDTA chelating agent was added to achieve a final concentration of 0.1 % in the samples. The measured volumes were subsequently enriched onto Oasis HLB cartridges (60 mg, 3 mL; Waters, Milford, MA, USA) using the protocol described in the EPA Method 1694 for extraction of acid fractions of aqueous samples. Briefly, samples were acidified with 12 N HCl to obtain pH 2 ± 0.5. HLB cartridges were conditioned with 20-mL methanol and 6-mL water at pH 2 ± 0.5. The cartridges were loaded with 100 mL of influent and 250 mL of effluent, respectively, at a constant flow rate of 5–6 mL/min. After sample preconcentration, cartridges were rinsed with 10-mL HPLC water to remove the EDTA and dried under vacuum for approximately 5 min to remove excess water. The target analytes were eluted with 12 mL of methanol. Using a gentle stream of nitrogen gas, the extract volumes were reduced to near dryness in a water bath held at 50 ± 5 °C and reconstituted in 1 mL of methanol. LC-MS/MS measurements were carried out with an HPLC system Agilent 1290 Infinity coupled to an Agilent 6410 triple quadrupole MS equipped with an electrospray ionization (ESI) source (Agilent Technologies, Waldbronn, Germany) in multiple reaction monitoring mode (MRM). Instrument control and data processing were carried out by means of MassHunter software (A GL Sciences, Tokio, Japan). The separation of the analytes was performed at 40 °C on a Zorbax SB-C18 Rapid Resolution HT column 50 mm × 2.1 mm i.d., 1.8-μm particle size, at a flow rate of 0.3 mL/min. A gradient program was used with the mobile phase, combining solvent A (with 0.1 % formic acid in ultrapure water) and solvent B (acetonitrile) as follows: from 2 to 58 % B in 5 min and from 58 to 79 % B in 5 min and equilibration for 10 min. The injection volume was 1 μL and all the analytes were eluted within 10 min. Nitrogen gas was used as collision and nebulizing gas (9 L/min, nebulizer pressure 40 psi).The analyses were done in the positive ion mode. The source temperature was 300 °C. The capillary voltage was 4000 V. Quantification was performed using external calibration and peak area measurements. Enhancement or suppression of analyte responses by matrix effect encountered in methods based on electrospray mass spectrometry are corrected automatically with an isotopically labeled internal standard. Due to the lack of a specific internal standard, all the analytical results reported in this work are only qualitative.
Ecotoxicological test methods
Toxicity assays were carried out according to OECD and ISO methodologies using conventional and alternative methods based on the following aquatic organisms: fish (Cyprinus carpio), planktonic crustacean (Daphnia magna), luminescent bacteria (Vibrio fischeri), and other bacteria (Gram-negative and Gram-positive bacteria) (Table 2). The tested fish species are specific for Romanian surface waters, are easy to acclimatize in a laboratorium, and are sensitive to various contaminants. The experimental testing was performed considering the fish number reduction. Also, the tested crustaceans and bacteria were selected on the recommendation of international practices for acute toxicity tests.
Sample preparation
Stock solutions were prepared from a known quantity of PhACs dissolved into a specified volume of dilution water or growth medium. No added solvents were used and all concentrations were tested under their solubility threshold. The solutions were stirred for 24 h in the dark at 25 °C. The testing solutions were prepared by mixing the appropriate volumes of stock solutions with dilution water or growth medium in order to obtain the final concentrations used for testing. Finally, the pH of tested solutions was between 6.5 and 8.5 pH units.
Fish toxicity test procedure
The fish acute static toxicity test was performed on C. carpio and their mortality was measured at 96 h of PhAC exposure in accordance to OECD 203.
Briefly, one-year-old fish, with health and origin certificates, were purchased from selected fish lots from a Romanian authorized fish farm. The fish with similar lengths were acclimatized in the laboratory for 3 weeks prior to the testing. The toxicity test was performed in duplicate on five fish (length 4 ± 2 cm) per 10-L aquariums untreated (control) or treated with different concentrations of PhACs ranging from 1 to 500 mg/L. The mortality and behavior modifications were registered every 24 h as well as registering after 96 h the lethal concentration for 50 % of the fish (LC50-96 h) which allows calculating the no observed effect concentration (NOEC).
Crustacean toxicity test procedure
The test determined the PhAC concentration that immobilizes or kills 50 % (EC50) of crustacean D. magna, after 24 or 48 h of chemical exposure at 20 ± 2 °C in the dark. The test procedure was performed according to OECD 202 and ISO 6341 using the Daphoxkit F Magna microbiotest provided by MicroBioTests Inc., Belgium. In short, the test was performed in three replicates in a multiwell test plates using 20 organisms for each concentration (at least 5 different concentrations for each PhACs) and control (untreated standard freshwater). The mortality/immobilization percentages of organisms were registered after 24 and 48 h. The NOEC values were determined as well.
Luminescent bacteria toxicity test procedure
Acute toxicity tests with luminescent bacteria V. fischeri were performed according to DIN EN ISO 11348–3 method using lyophilized bacteria (Multi-Shot kit) purchased from Macherey–Nagel GMbH and Co. KG, Germany. The pH of the samples was adjusted in the interval 6–8.5 units. The samples were enriched with 20 % NaCl to adjust the osmolality. The tests were performed at 15 ± 1 °C in three replicates using a bacteria inoculum of 108 cells/mL per each concentration (at least five different concentrations for each PhAC) and control (untreated media). The light intensity produced by the bacteria was measured using the “BioFix Lumi” system, before and after 15 min of incubation, in the presence of PhACs compared to the control (untreated bacteria). The intensity of luminescence is inversely proportional with the toxic effect of PhACs on microorganisms. The test endpoints, EC50, and NOEC values were calculated.
Microbial toxicity test procedure
Microbial assay for risk assessment (MARA) test, purchased from NCIMB Ltd., Scotland, is a multispecies toxicity test based on responses of 11 microorganisms (10 bacteria and 1 yeast strain) to toxic compounds. This toxicity test was performed on caffeine and carbamazepine. The microbial growth rates were determined by a redox dye (2, 3, 5-triphenyl tetrazolium salt) reduction which induces insoluble reaction products (red) that precipitate and form pellets. The pellet size was proportional with the rate of microbial growth. The microplates were scanned with a scanner HP Scajet XPA and the image was analyzed by MARA software for microbial toxic concentration (MTC) value determination. All the tests were performed in duplicates.
Data processing and statistics
The acute median effects of PhAC concentrations in fish (LC50) and crustacean (EC50) were calculated using the probity analysis method which is based on exponential regression relationship between cumulative percentages of mortality (expressed as probity units) for each exposure period of time and logarithmic concentrations of test substance. In the case of luminescent bacteria, the concentration-effect relationship was calculated using standard linear regression analysis. All the calculations were performed using Microsoft Excel—RegTox. The MTC values in MARA tests were calculated by comparing the area under and above the growth curve using the MARA software (provided by NCIMB Ltd, Scotland). Standard deviations (STDEVs) were calculated for every assay (chemical detection or toxicity assay).
Aquatic risk assessment
Risk characterization is required for all chemicals, including the PhACs, as an estimation of their exposure and adverse effects on the environmental compartment. Generally, this is based on predicted environmental concentration (PEC) and predicted no effect concentration (PNEC) calculation, in terms of exposure and assessment of effects. The aquatic risk assessment of the studied PhACs was conducted according to the environmental risk assessment (ERA) (EMEA 2006). The general principle of ERA procedures for conventional chemicals in Europe was also used (TDG 2003).
The evaluation of human PhAC risks generally encompasses three phases: phase I—a “prescreening” that requires the data collection in order to estimate the exposure restricted to aquatic PEC calculation using Eq. 1; phase II Tier A—“screening” that entails the aquatic toxicology and fate assessment for an initial risk prediction; phase II Tier B—an “extended” phase that allows a refinement of risk assessment using detailed data:
where PEC EMEA (water) is predicted environmental concentration for surface water and DOSEai is the maximum daily dose taken per inhabitant (in mg). These values were found in Romanian Pharmacopoeia (2015) and Romanian National Medicament Agency databases. Fpen (%) is a market penetration factor of active ingredients and has a recommended value of 1 % by the EMEA guideline or other values according to a wide range of individual market penetration factor (Hamre 2006); WASTEW inhab represents the total volume of wastewater generated per inhabitant and for Romania, it was estimated at 200 L/day/inhabitant (Grung et al. 2008); D is a dilution factor set to 10 for environmental extrapolation (Grung et al. 2008); 100 is the correction factor for percentages; 103 is the unit conversion factor from milligram in micrograms.
In order to estimate the current contamination of surface water with PhACs, three other PEC calculation models were applied (Eqs. 2, 3, and 4).
where: PECPharma (surface water) was calculated using statistical data of the predicted PhAC amount used per year in tons (A) estimated for 1 t/year/PhAC, removal rate in WWTPs (R) using our data, number of inhabitants in Romania (P) set at 19 million in 2012, volume of wastewater per inhabitant (V), a dilution factor set to 10 (D); a unit conversion factor from ton to micrograms (1012), and a conversion factor for percentages (100).
The phase II Tier A of the ERA was applied when the PEC of the PhACs exceeded the value of 0.01 μg/L in surface water. This phase involved the PNEC calculation using an assessment factor (AF) of 1000 applied for L(E)C50 or 10 applied for NOEC, which expresses the degree of uncertainty in the actual environmental extrapolation. In the end of phase II, the quotient risks (RQs) between PEC (or MEC) and PNEC were calculated: RQ <0.1, the substance has negligible risk; RQ between 0.1 and 1 has a low risk; RQ values between 1 and 10 show a moderate risk; and at an RQ value greater than 10, the substance is considered to have a high environmental risk.
This work presented the results obtained in phases I and II Tier A of the aquatic risk assessment for studied PhACs using our wastewater and surface water analytical data as well as the toxicity data.
Results and discussions
Occurrence of PhACs in WWTPs and surface waters
Detection and quantity monitoring of chemical compounds by physicochemical techniques are essential steps in assessing their potential toxic effect on the environment. The presence of PhACs in influents as well as in effluents from WWTPs seemed to be constant regardless of the location and collection period of time (data not shown). The same pattern of PhAC presence was observed for the surface waters (data not shown).
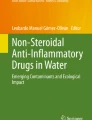
In WWTPs influents, ibuprofen and caffeine were found at the highest concentration, around 22 μg/L, then acetaminophen (12.42 μg/L) as well as diclofenac and ketoprofen (7 μg/L) (Fig. 1). Very small amounts of indomethacin, naproxen, and carbamazepine (<2 μg/L) (Fig. 1) were detected. In spite of the fact that based on DOSEai, the caffeine consumption (300 mg/patient) is four times less compared to ibuprofen (1200 mg/patient), their concentration in influents was almost identical. The extra caffeine input could come from other non-therapeutic sources such as coffee, tea, chocolate, or refreshments. Moreover, according to DOSEai based in Romanian Pharmacopoeia (2015) and National Agency Medicines and Medical Devices databases, the acetaminophen consumption was around of 3000 mg/patient, which was by far the highest among the tested PhACs. In spite of this fact, acetaminophen presence, as a contaminant, in the wastewaters (influent of 12.42 μg/L) was almost 50 % lower than caffeine and ibuprofen. Generally, this discrepancy could be explained by the short half-life of this compound (<5 % is excreted unchanged from the human body after a therapeutic dose) (Bessem and Vermeulen 2001) as well as by strong biodegradability and biosorption (Tsung et al. 2011).

The average values of PhAC concentrations detected in three WWTPs (Pitesti, Targu Mures, and Brasov) and in four Romanian surface waters (Ghimbasel Stream, Mures River, Arges River, and Danube River—Danube Delta)
The highest concentrations in WWTP effluents were found for caffeine (8.16 μg/L) and ibuprofen (7.60 μg/L). In addition, our previous results from 2009 to 2013 (Gheorghe et al. 2014) corroborated with our present results regarding the mean concentrations of diclofenac (3.45 μg/L), naproxen (0.18 μg/L), and carbamazepine (0.54 μg/L) in effluents showed higher concentrations compared to other international reports (Lin et al. 2005; Roberts and Thomas 2006).
The mean of PhAC removal rates (Fig. 2) in the monitored WWTPs was ≥60 % for all tested PhACs except for naproxen (57 %), which corroborate with another report mentioning that even advanced WWTP (using ultrafiltration, activated charcoal, and reverse osmosis after the primary biological treatment) were not efficient in naproxen removal (Mohannad et al. 2013). A particular case was at Targu Mures WWTP, where the removal rates of ketoprofen (<40 %) and carbamazepine (1–20 %) were lower compared to the other WWTPs (Pitesti and Brasov) that indicate a poor wastewater treatment system for those two compounds (data not shown).

Average of removal rates of studied PhACs
In general, the concentration of the tested PhACs in the surface waters was lower compared to the effluents (Fig. 1). This observation could be explained by the dilution factor when effluents reached the main water surface. The only exceptions were for ibuprofen (10.25 μg/L) and naproxen (0.44 μg/L) found at higher concentrations compared to wastewater effluents, and this could be explained by an addition from other pollution sources (industrial wastewater or livestock farms). In general, the wastewater release was the main PhAC source for Ghimbasel Stream (a natural receptor of Brasov WWTP effluents, with a flow of about 2 m3/s), Mures River (mean flow of 33.6 m3/s), Arges River (mean flow of 40 m3/s), Danube River (mean flow of 6500 m3/s), and Danube Delta (Sf. Gheorghe Branch—mean flow of 1500 m3/s). In the surface waters, the concentrations of diclofenac (2.21 μg/L), ketoprofen (0.82 μg/L), and caffeine (4.82 μg/L) decreased up to twofold compared to WWTPs, due to the dilution factor. Moreover, concentrations of acetaminophen (1.58 μg/L), indomethacin (0.26 μg/L), and carbamazepine (0.08 μg/L) from surface water were 1/3 at the same level to effluent concentrations, perhaps due to a high degradability and/or high absorption. Higher PhAC concentrations (diclofenac 4.91 μg/L, acetaminophen 4.55 μg/L, ketoprofen 2.45 μg/L, ibuprofen 30.71 μg/L, and caffeine 17.4 μg/L) were observed in the Ghimbasel Stream as a result of poor water dilution. In addition, this brook is receiving the WWTP effluents from Brasov which harbors a big drug manufacturing company. The PhAC concentrations from Arges River, Mures River, Danube River, and Danube Delta—Sf. Gheorghe Branch were lower than 1 μg/L, excepting the caffeine and ibuprofen.
A recent study on Somes River from Romania revealed analgesic, nervous stimulants, antirheumatic, and antiepileptic drug exposure concentrations ranging from 0.01 to 10 μg/L, which showed a decrease compared to previous years. This fact could be explained by a recent improvement of the municipal wastewater treatment processes in the city of Cluj Napoca (Moldovan et al. 2009). Moreover, 15 pharmaceuticals and personal care products (concentrations ranging from the 30 ng/L to 10 μg/L) were reported in the surface water of Somes River (Moldovan 2006; Moldovan et al. 2007).
Our results highlighted that PhAC concentrations detected in Romanian surface waters were higher than in other countries such as Germany, Slovenia, USA, or France (Jux et al. 2002; Kosjek 2006; Thaker 2005; Feitosa-Felizzola and Chiron 2009), and this fact could be explained by an excessive and unchecked PhAC consumption (Pop 2010) corroborated with a less efficient wastewater treatment process for PhACs.
The mean concentrations found in Romanian surface waters (MEC) (Fig. 1) were used as PEC in order to estimate the aquatic risks.
All the PhAC concentrations from surface waters, analyzed in this study, ranged between 0.01 to 1 μg/L and these values were used to calculate the risk assessment by the phase II Tier A—toxicity assessment using aquatic organisms.
Toxicity screening
The PhACs have been designed to induce specific biological effects, generally without negative effects on humans and animals. Unfortunately, once PhACs are released into the environment, no additional information of their biodegradability, toxic effects, and bioaccumulation in aquatic organisms from the contaminated area were found(Moldovan et al. 2009; Fernández et al. 2014).
Toxicity data, both acute and chronic toxicity, are very important to estimate the type and the degree of toxic effect of the emerging drugs on tested organisms (Li and Randak 2009). Two serious consequences of PhAC environmental contamination have been (i) the adaptation of bacteria and viruses to active compounds from PhACs by increasing their expression of resistance genes (Goni-Urriza et al. 2000; Edge and Hill 2005; Kim et al. 2007a; Peak et al. 2007; Kümmerer 2009a; Martinez 2009; Banciu et al. 2016), gene mutation (Kimiko et al. 2000), and/or acquiring of resistance genes by lateral transfer (Agnese et al. 2012) and (ii) the endocrine disruption in humans, terrestrial, and aquatic organisms (Roepke et al. 2005; Christen et al. 2010). For example, the anti-inflammatory drug diclofenac, frequently detected in wastewaters and surface waters, had been reported to have a harmful effect on rainbow trout. It accumulates in the trout’s liver and causes histological alterations in its early stages of life (Enick and Moore 2007; Triebskorn et al. 2007).
Table 3 shows acute toxicity data L(E,I)C50 (Gheorghe et al. 2013) and NOEC obtained in our laboratory. These data were used for PNEC calculation in order to estimate the level of aquatic risks on each target organism.
It seems that the tested compounds did not have an acute toxicity effects on fish for the majority of PhACs, and the LC50 values ranged between 42.60 mg/L for carbamazepine (low toxicity for fish) and 269.15 mg/L for naproxen (non-toxic for fish), similar values being reported in literature (EaSI-Pro(R) View Data base 2005). The non-effect concentrations of PhACs (determined in the acute toxicity tests) were in the range from 0.8 mg/L for carbamazepine to 25 mg/L for naproxen. Behavioral disturbances, but no mortality effects, induced by carbamazepine were observed in acute toxicity tests at low concentrations (<10 mg/L).
The PhAC concentrations used in vitro (mg/L) with an acute toxic impact on different biological models were much higher than in field concentrations (μg/L), suggesting no acute toxic effect on the aquatic organisms from the natural environment. In spite of no acute effects, on the long term, due to bioaccumulation, it could appear to have strong toxicity on fish embryos even at very low concentrations (i.e., 0.09–0.48 mg/L for diclofenac) highlighted by Ferrari et al. 2003 and EaSI-Pro(R) View Data base 2005.
Toxicity tests on D. magna crustaceans showed toxicity values ranging from 11.02 mg/L for acetaminophen to 162.18 mg/L for caffeine, similar with literature values that range from 9.2 mg/L for acetaminophen to 182 mg/L for caffeine (EaSI-Pro(R) View Data base 2005; Ferrari et al. 2003). The daphnia NOEC values of PhACs were in the range of 0.43 mg/L for indomethacin and 10 mg/l for caffeine.
Luminescent bacteria and other bacteria showed the highest sensitivity to the toxic effects of PhACs, with the exception of caffeine. The acetaminophen and indomethacin induced a toxic bacterial effect at concentrations smaller than 10 mg/L. Diclofenac, ketoprofen, naproxen, ibuprofen and carbamazepine showed harmful effects in the range of 16.21 to 54.21 mg/L, respectively. The PhAC NOEC values obtained for bacteria were in the range of 0.4 mg/L for carbamazepine and 10 mg/l for caffeine.
Risk characterization
In spite of the fact that many studies on PhACs toxicity are found in literature, there is still a lack of data necessary for supporting a valid risk assessment. Due to application of a conservative assessment factor (AF = 1000, 100 or 50) to the available ecotoxicological data, a great variation of PNECs has been observed (Chen et al. 2014). On the other hand, the absence of clear PhAC consumption data has been a major problem in ensuring a relevant risk assessment.
In order to estimate the environmental risk of the pharmaceuticals compounds, we used four different scenarios: PECEMEA(water) according to EMEA guideline; PECeffluents from PhAC concentrations measured in the wastewater effluents, adding a dilution factor; PECs (herein represented by MEC) from PhAC concentrations detected in surface water; and PECPharma integrating the PhAC removal rate in WWTPs, the predicted PhAC amounts used per year reported to number of inhabitants and wastewater volume per inhabitant.
All PEC values obtained in our study (Table 4) showed that PhACs from Romanian surface waters have the same level as from other EU countries. The range of PECs of diclofenac (0.04 to 5.2 μg/L), acetaminophen (0.06 to 39 μg/L), ketoprofen (0.03 to 1 μg/L), naproxen (0.01 to 2.5 μg/L), and carbamazepine (0.01 to 6 μg/L) identified in our studies were smaller than those specified in literature. For example, other literature data showed the following PECs: 0.048–18.05 μg/L for diclofenac, 15–65.4 μg/L for acetaminophen, 0.063–9.5 μg/L for ketoprofen, 0.19–2.1 μg/L for naproxen, and 0.19–19.25 μg/L for carbamazepine (Stuer-Lauridsen et al. 2000; Ferrari et al. 2003; Carlsson et al. 2006; Hamre 2006; Ying et al. 2009).
Our PEC values detected for ibuprofen (0.017 to 21.6 μg/L) and caffeine (0.07 to 1.5 μg/L) were higher compared to literature-reported data (ibuprofen 0.012–10 μg/L and caffeine 0.17 μg/L) (Stuer-Lauridsen et al. 2000; Carlsson et al. 2006; Hamre 2006; Ying et al. 2009), and this fact could be explained by an uncontrolled market consumption (Fpen = 3.6 % specified by Hamre 2006) of ibuprofen and of non-therapeutic uses of caffeine.
Data from Table 4 showed significant differences between PECEMEA(water) (Eq. 1), PECeffluent (Eq. 2), and PECPharma (Eq. 4) values compared to PECs, based on field monitoring (MEC from surface waters). This discrepancy was due to the lack of relevant Romanian databases regarding (i) maximum daily dose consumed per inhabitant, (ii) market penetration factor of active ingredient, (iii) effluent dilution factor in the receiving waters, (iv) predicted amount used per year, (v) medicine prescription and non-prescription, and (vi) direct discharge of untreated wastewater into the surface water. For this reason, the quotient risks were calculated by taking into consideration only the PECsurface water (as MEC) values obtained using the average of measured concentrations in surface water (Eq. 3). The data showed MEC values higher than 0.01 μg/L and it was followed by PNEC calculation on aquatic organisms for all investigated PhACs. The ketoprofen, indomethacin, naproxen, and carbamazepine concentrations were lower than 1 μg/L, but diclofenac, acetaminophen, ibuprofen, and caffeine concentrations from surface water were higher (similar results were obtained by Chen et al. 2014).
The estimated PNECs and RQs were summarized in Table 5. All EC50 and NOEC values (obtained in our laboratories on fish, crustaceans, and bacteria) as well as the extrapolation factor (1000 for EC50 values and 10 for NOEC values) were used for PNEC calculation.
The estimated PNEC values varied being dependent on the PhAC type and target organism. The laboratory results may not reflect the actual environmental situation because biodegradation, persistence, and adsorption were not analyzed during the laboratory toxicity tests. These factors could reduce the PhAC exposure concentration subsequently decreasing the risk level (Kümmerer 2009b).
The PhAC quotient risks were calculated as the ratio between MEC values estimated in the monitored Romanian waters and PNEC values calculated for each tested organism. The level of risk was estimated by the average of all RQs (total risk level) initially determined on every single target organism (based on EC50 or NOEC values). Results presented in Table 5 (risk level, last column) showed that sometimes, the higher risk for a particular organism was different than the average risk from all tested organisms. The results highlighted an overall insignificant risk for carbamazepine (0.03), but a low risk in fish (0.10) and bacteria (0.20). Acetaminophen had an overall low risk level (0.86), but a specific moderate risk to daphnia and bacteria. In addition, ketoprofen had an overall low risk level (0.54), but a specific moderate risk only to daphnia. Indomethacin (0.25), naproxen (0.12), and caffeine (0.22) induced a low risk for all target organisms. An overall moderate risk level was induced by diclofenac (1.25) and ibuprofen (1.75), but hazardous effects were induced only on daphnia and bacteria.
Literature shows different values of PEC (or MEC) and PEC/PNEC ratios (0.01 for caffeine to 1 for ibuprofen) estimated in studies concerning the predicted concentrations in surface waters and the risk coefficients. The risk data were influenced by the specific areas, consumptions, and number of inhabitants. In general, the PhAC compounds studied here were hazardous for the aquatic environment, especially when the studies were performed for hospitals and noncompliance WWTP discharge areas (Ferrari et al. 2003; Carlsson et al. 2006; Ying et al. 2009). Literature data on carbamazepine reported that it was a high risk coefficient in the range of 4.69–47 (Ferrari et al. 2003; Ying et al. 2009) in France and Germany, compared to Romania (0.03—insignificant risk).
In case of C. carpio, an important fish species with economic importance for Romania, negligible or low risk was observed for the majority of investigated PhACs, except for ibuprofen with an RQ of 1.03 (moderate risk level). Considering the RQs based on LC50 data, no risk was identified.
D. magna showed RQ (base on NOECs) values assigned to moderate risk (for diclofenac4.91; acetaminophen 1.58; ketoprofen 1.46; and ibuprofen 2.05) and low risk (for indomethacin 0.60; naproxen 0.44; and caffeine 0.48). If the EC50 values were used for PNEC calculation, the estimated RQs were ≤0.1 (insignificant risk) for all investigated PhACs.
The RQ (base on IC50) values for V. fischery and other bacteria showed low risk for diclofenac, acetaminophen, and ibuprofen. Moderate risks for bacteria (base on NOECs) were identified for the same PhACs.
The PhACs which induced aquatic risk conditions were ibuprofen, diclofenac, acetaminophen, and ketoprofen, especially because of their effects on crustacean and luminescent bacteria, as well as on the fish in case of Ibuprofen.
Further evaluations of the fate and effects of all studied PhACs is necessary not only at a global level (Romania) but also in regional areas, especially on a special site such as Ghimbasel Stream area where the aquatic risk of detected PhACs could be much higher.
In order to estimate the admissible limits of these contaminants in the natural waters and complete the national norms concerning the surface water quality, PNEC calculation based on chronic test data are needed. The risk level expressed, taking into account acute toxicity data, is not enough for a complete estimation of long-term impacts of PhACs on aquatic life. In addition, the environmental risk should be evaluated under toxicity endpoints due to various sensitivities of different aquatic species and testing procedures.
Conclusions
Due to larger amounts of PhACs as a result of population health issues, the PhACs have started to be found in the Romanian rivers. In this study, we analyzed for the first time the presence of eight PhACs commonly used in Romania (diclofenac, acetaminophen, ketoprofen, naproxen, ibuprofen, indomethacin, carbamazepine, and caffeine) in the wastewaters from three WWTPs and in the surface water from four rivers, including the Danube Delta, and we estimated their aquatic environmental risk.
Our studies revealed the occurrence of studied PhACs in all analyzed wastewater samples (influents—0.3 μg/L for naproxen to 21.48 μg/L for ibuprofen; effluents—0.18 μg/L for naproxen and 8.16 μg/L for caffeine) and their removal rates which were at least 50 % during WWTP treatment processes.
The monitoring studies in Romanian surface waters showed PhACs at low concentrations, but more than 0.01 μg/L indicating the need of risk assessment using ecotoxicological data. The surface water from Ghimbasel Stream have had high concentrations for the majority of PhACs (as a result of a poor water dilution and due to the nearby presence of pharmaceutical companies), but lower concentrations (up to 1 μg/L) in Arges River, Mures River, and Danube River.
The ecotoxicological laboratory tests revealed no acute toxicity effects on fish for the majority of PhACs, although low acute toxicity effects of PhACs were observed on planktonic crustaceans and bacteria, which showed the highest sensitivities.
This study pointed out that the PhACs detected in the Romanian surface water induced a total risk (obtained as average of all RQs of target organisms) classified as: insignificant risk for carbamazepine; low risk level for acetaminophen, ketoprofen, indomethacin, naproxen, and caffeine; and moderate risk for diclofenac and ibuprofen. The PhACs that create aquatic risk conditions were ibuprofen, diclofenac, acetaminophen, and ketoprofen, especially because of their effects on crustaceans and bacteria. Ibuprofen showed a specific moderate risk for fish considering acute no observable effect concentration for RQ calculation.
For a more realistic risk estimation concerning the fate and effects of PhACs in Romanian surface waters, sezonal distribution of pharmaceutical pollutants, long-term toxicological data, and studies of synergistic risks are needed.
References
Agnese, L., Sébastien, C., & Thomas, U. B. (2012). Origin and evolution of antibiotic resistance: the common mechanisms of emergence and spread in water bodies. Frontiers in Microbiology, 3, 18.
Banciu, A., Niculescu, D., Nita-Lazar, M., Lucaciu, I., Stoica, C., & Mihaescu, G. (2016). Potentially pathogenic and antibiotic resistant bacteria in the Danube Delta aquatic ecosystem. Journal of Environmental Protection and Ecology, 17(1), 127–135.
Bendz, D., Paxéus, N. A., Ginn, T. R., & Loge, F. J. (2005). Occurrence and fate of pharmaceutically active compounds in the environment, a case study: Hoje River in Sweden. Journal of Hazardous Materials, 122, 195–204.
Bessem, J. G., & Vermeulen, N. P. (2001). Paracetamol (acetaminophen)-induced toxicity: molecular and biochemical mechanisms, analogues and protective approaches. Critical Review in Toxicology, 31(1), 55–138.
Bound, J. P., & Voulvoulis, N. (2006). Pharmaceuticals in the aquatic environment—a comparison of risk assessment strategies. Chemosphere, 56, 1143–1155.
Carlsson, C., Johansson, A.-K., Alvan, G., Bergman, K., & Kühler, T. (2006). Are pharmaceuticals potent environmental pollutants? Part I: environmental risk assessments of selected active pharmaceuticals ingredients. Science of the Total Environment, 364, 67–87.
Cayman Chemical (2012). Product information, Indomethacin 70270.
Chen, H.-C., Wang, P.-L., & Ding, W.-H. (2008). Using liquid chromatography-ion trap mass spectrometry to determine pharmaceuticals residues in Taiwanese rivers and wastewaters. Chemosphere, 72, 863–869.
Chen, Y., Xi, X., Yu, G., Cao, Q., Wang, B., Vince, F., & Hong, Y. (2014). Pharmaceutical compounds in aquatic environment in China: locally screening and environmental risk assessment. Frontiers of Environmental Science & Engineering, 9(3), 1–7.
Christen, V., Hickmann, S., Rechenberg, B., & Fent, K. (2010). Highly active human pharmaceuticals in aquatic systems: a concept for their identification based on their mode of action. Aquatic Toxicology, 96, 167–181.
EU Directive, (2013). Directive 2013/39/EU of the European Parliament and of the Council of 12 August 2013 amending Directives 200/60/EC and 2008/105/EC as regards priority substances in the field of water policy (OJ L 226/1, 24.8.2013, p. 9).
EaSI-Pro ® View 14.0 Data base for dangerous chemicals, 2005 Haskoning B.V. http://www.ekotox.eu/component/content/article/118-EASI-pro-view
Edge, T. A., & Hill, S. (2005). Occurrence of antibiotic resistance in Escherichia coli from surface waters and fecal pollution sources near Hamilton, Ontario. Canadian Journal of Microbiology, 51, 501–505.
EMEA, (2006). Guideline on the environmental risk assessment of medicinal products for human use; The European Agency for the Evaluation of Medicinal Products, London, England, Doc. Ref. EMEA/CHMP/SWP/4447/00, http://www.emea.eu.int/pdfs/human/swp/444700en.pdf.
Enick, O. V., & Moore, M. M. (2007). Assessing the assessments: pharmaceuticals in the environment. Environmental Impact Assessment Review, 27, 707–729.
ESAC, (2005). Peer Review of European Commission, Proposal for a new testing strategy (Step-down approach) to reduce the use of fish in acute aquatic toxicity testing, Joint Research Centre.
Feitosa-Felizzola, J., & Chiron, S. (2009). Occurrence and distribution of selected antibiotics in a small Mediterranean stream (Arc River, Southern France). Journal of Hydrology, 364(1–2), 50–57.
Fent, K., Weston, A. A., & Caminada, D. (2006). Ecotoxicology of human pharmaceuticals. Aquatic Toxicology, 76, 122–159.
Fernández, C., Beltrán, E.M., Tarazona, J.V. (2014). Pharmaceuticals effects in the environment, Encyclopedia of Toxicology (Third Edition), 844–848.
Ferrari, B., Paxe’us, N., Lo Giudice, R., Pollio, A., & Garrica, J. (2003). Ecotoxicological impact of pharmaceuticals found in treated wastewaters: study of carbamazepine, clofibric acid, and diclofenac. Ecotoxicology and Environmental Safety, 55, 359–370.
Gartiser, S., Urich, E., Alexy, R., & Kümmerer, K. (2007). Ultimate biodegradation and elimination of antibiotics in inherent tests. Chemosphere, 67, 604–613.
Gheorghe, S., Lucaciu, I., Grumaz, R., (2010). Microbiotests versus conventional toxicity tests. In: Proc. of Inter. Conf. SGEM, Albena, Bulgary, vol. 2, 669–677.
Gheorghe, S., Lucaciu, I., Stanescu, E., & Stoica, C. (2013). Romanian aquatic toxicity testing strategy under REACH. Journal of Environmental Protection and Ecology, 14(2), 601–611.
Gheorghe, S., Lucaciu, I., Paun, I., Stoica, C., & Stanescu, E. (2014). Environmental exposure and effects of some micropollutants found in Romanian surface waters. Journal of Environmental Protection and Ecology, 15(3), 878–889.
Goni-Urriza, M., Capdepuz, M., Arpin, C., Raymond, N., Caumette, P., & Quetin, C. (2000). Impact of an urban effluent on antibiotic resistance of riverine Enterobacteriaceae and Aeromonas spp. Applied and Environmental Microbiology, 66(1), 125–132.
Granberg, R. A., & Rasmuson, A. C. (1999). Solubility of paracetamol in pure solvents. Journal and Chemical Engineering Data, 44(6), 1391–95.
Grung, M., Kallqvist, T., Sakshaug, S., Skurtveit, S., & Thomas, S. K. V. (2008). Environmental assessment of Norwegian priority pharmaceuticals based on the EMEA guideline. Ecotoxicology and Environmental Safety, 71(2), 328–340.
Hamre, H.T., (2006). Initial assessment of eleven pharmaceuticals using EMEA guideline in Norway, TA-2216.
Homem, V., & Santos, L. (2011). Degradation and removal methods of antibiotics from aqueous matrices—A review. Journal of Environmental Management, 92, 2304–2347.
Jux, U., Baginski, R. M., Arnold, H. G., Krönke, M., & Peter, N. (2002). Detection of pharmaceuticals contaminations of river, pond, and tap water from Cologne (Germany) and surroundings. International Journal of Hygiene and Environmental Health, 205(5), 393–398.
Kim, S., & Aga, D. S. (2007). Potential ecological and human health impacts of antibiotics and antibiotic-resistant bacteria from wastewater treatment plants. Journal of Toxicology and Environmental Health, 10, 559–573.
Kim, S. D., Cho, J., In: Kim, S., Vanderford, B. J., & Snyder, S. A. (2007a). Occurrence and removal of pharmaceuticals and endocrine disruptors in South Korean surface, drinking, and waste waters. Water Research, 41, 1013–1021.
Kim, Y., Choi, K., Jung, J. Y., Park, S., Kim, P. G., & Park, J. (2007b). Aquatic toxicity of acetaminophen, carbamazepine, cimetidine, diltiazem and six major sulfonamides, and their potential ecological risks in Korea. Environmental International, 33, 370–375.
Kimiko, A. H. T., Hiroshi, A., & Yasunobu, A. (2000). Transgenic zebrafish for detecting mutations caused by compounds in aquatic environments. Nature Biotechnology, 18, 62–65.
Koreje, K., Demeestere, K., De Wispelaere, P., Vergeynst, L., Dewulf, J., & Van Langenhove, H. (2012). From multi-residue screening to target analysis of pharmaceuticals in water: Development of a new approach based on magnetic sector mass spectrometry and application in the Nairobi River basin, Kenya. Science of the Total Environment, 437, 153–164.
Kosjek, T., (2006). Pharmaceuticals residues removal in a pilot wastewater treatment plant, NORMAN workshop, Menorca, Spain, November 27–28.
Kümmerer, K., (2008). Pharmaceuticals in the environment: sources, fate, effects and risks, 3rd Edition, Springer-Verlag, Berlin Heidelberg, 4–6.
Kümmerer, K. (2009a). Antibiotics in the aquatic environment—a review—part II. Chemosphere, 75, 435–441.
Kümmerer, K. (2009b). The presence of pharmaceuticals in the environment due to human use—present knowledge and future challenges. Journal of Environmental Management, 90(8), 2354–2366.
Li, Z. H., & Randak, T. (2009). Residual pharmaceutically active compounds (PhAcs) in aquatic environment—status, toxicity and kinetics: a review. Veterinary Medicine - Czech, 52(7), 295–314.
Lin, W. C., Chen, H. C., & Ding, W. H. (2005). Determination of pharmaceuticals residues in waters by solid-phase extraction and large-volume on-line derivatization with gas chromatography–mass spectrometry. Journal of Chromatography. A, 1065, 279–285.
Madureira, T., Barreiro, J., Rocha, M., Cass, Q., & Tiritan, M. (2010). Spatiotemporal distribution of pharmaceuticals in the Douro River estuary (Portugal). Science of the Total Environment, 408(22), 5513–5520.
Martinez, J. L. (2009). Environmental pollution by antibiotics and by antibiotic resistance determinants. Environmental Pollution, 157, 2893–2902.
Mohannad, Q., Mustafa, K. F. M., Shlomo, N., Sabino, A. B. A., Laura, S., & Rafik, K. (2013). Stability and removal of naproxen and its metabolite by advanced membrane wastewater treatment plant and micelle–clay complex, Clean – Soil, Air, Water, 41(9999), 1–7.
Moldovan, Z. (2006). Occurrence of pharmaceuticals and personal care products as micro pollutants in rivers from Romania. Chemosphere, 64, 1808–1817.
Moldovan, Z., Schmutzer, G., Tusa, F., Calin, R., & Alder, A. C. (2007). An overview of pharmaceuticals and personal care products contamination along the river Somes watershed, Romania. Journal of Environmental Monitoring, 9, 986–993.
Moldovan, Z., Chira, R., & Alder, A. C. (2009). Environmental exposure of pharmaceuticals and musk fragrances in the Somes River before and after upgrading the municipal waste water treatment plant Cluj-Napoca, Romania. Environmental Science and Pollution Research, 16(Suppl 1), S46–S54.
Muhammad, S. U. R., Ameena, S., Audil, R., Raza, A., Muhammad, F. M., & Tariq, M. (2013). Chemometric classification of advanced oxidation processes for the degradation of pharmaceuticals and personal care products. Environmental Engineering and Management Journal, 12(3), 475–481.
Nita-Lazar, M., Galaon, T., Banciu, A., Paun, I., Stoica, C., & Lucaciu, I. (2016). Screening of various harmful compounds in a new bacterial biological model. Journal of Environmental Protection and Ecology, 17(1), 237–247.
Nowara, A., Burhenne, J., & Spitelle, M. (1997). Binding of fluoroquinolone carboxylic acid derivates to clay minerals. Journal of Agriculture and Food Chemistry, 45(4), 1459–1463.
Peak, N., Knapp, C. W., Yang, R. K., Hanfelt, M. M., Smith, M. S., Aga, D. S., & Graham, D. W. (2007). Abundance of six tetracycline resistance genes in wastewater lagoons at cattle feedlots with different antibiotic use strategies. Environmental Microbiology, 9, 143–151.
Peng, X., Yu, Y., Tang, C., Tan, J., Huang, Q., & Wang, Z. (2008). Occurrence of steroid estrogens, endocrine-disrupting phenols, and acid pharmaceuticals residues in urban riverine water of the Pearl River Delta, South China. Science of the Total Environment, 397, 158–166.
Petrović M., (2007). Analysis, Fate and Removal of pharmaceuticals in the Water Cycle. Publisher: Amsterdam; Boston: Elsevier, 543.
Pop, C.-E. (2010). The Romanian population health in the European context, an approach in terms of quality of life. Quality of life, 21(3–4), 274–305.
Roberts, P. H., & Thomas, K. V. (2006). The occurrence of selected pharmaceuticals in wastewater effluent and surface waters of the lower Tyne catchment. Science of the Total Environment, 356(1–3), 143–153.
Roepke, T. A., Snyder, M. J., & Cherr, G. N. (2005). Estradiol and endocrine disrupting compounds adversely affect the normal development of the sea urchin embryo at environmentally relevant concentrations. Aquatic Toxicology, 71(2), 155–173.
Romanian pharmacopoeia, Edition 10 (2015). Editura Medicala, ISBN: 9789733906629.
Santos, J. L., Aparicio, I., Alonso, E., & Callejón, M. (2005). Simultaneous determination of pharmaceuticals active compounds in wastewater samples by solid phase extraction and high-performance liquid chromatography with diode array and fluorescence detectors. Analytica Chimica Acta, 550, 116–122.
Snyder, S. A., Westerhoff, P., Yoon, Y., & Sedlak, D. L. (2003). Pharmaceuticals, personal care products and endocrine disruptors in water: implications for the water industry. Environmental Engineering Science, 20(5), 449–469.
Straub, J. O. (2001). Environmental risk assessment for new human pharmaceuticals in the European Union according to the draft guideline/discussion paper of January 2001. Toxicology Letter, 131, 137–143.
Stuer-Lauridsen, F., Birkved, M., Hansen, L. P., Holten Lutzhùft, H. C., & Halling-Sùrensen, B. (2000). Environmental risk assessment of human pharmaceuticals in Denmark after normal therapeutic use. Chemosphere, 40, 783–793.
Syracuse Science Centre, (2002). Database of experimental octanol-water partition coefficients (Log P). Homepage: http://esc-plaza.syrres.com/interkow/kowdemo.htm.
Takacs-Novak, K., Josan, M., Hermecz, I., & Szasz, G. (1992). Lipophilicity of antibacterial fluoroquinolones. International Journal of Pharmaceutics, 79, 89–96.
TDG, (2003). Technical Guidance Document on Risk Assessment, Commission Directive 93/67/EEC on Risk Assessment for new notified substances, European Commission.
Thaker, A. (2005). Pharmaceuticals data elude researchers. Environmental Science and Technology, 139, 193–194A.
Triebskorn, R., Casper, H., Scheil, V., & Schwaiger, J. (2007). Ultrastructural effects of pharmaceuticals (carbamazepine, clofibric acid, metoprolol, diclofenac) in rainbow trout (Oncorhynchus mykiss) and common carp (Cyprinus carpio). Analytical and Bioanalitycal Chemistry, 387, 1405–1416.
Tsiaka, P., Tsarpali, V., Ntaikou, I., Kostopoulou, M. N., Lyberatos, G., & Dailianis, S. (2013). Carbamazepine-mediated pro-oxidant effects on the unicellular marine algal species Dunaliella tertiolecta and the hemocytes of mussel Mytilus galloprovincialis. Ecotoxicology, 22, 1208–1220.
Tsung, H. Y., Angela, Y.-C. L., Sri Chandana, P., Pui-Kwan, A. H., Ping, Y. Y., & Cheng, F. L. (2011). Biodegradation and bio-sorption of antibiotics and non-steroidal anti-inflammatory drugs using immobilized cell process. Chemosphere, 84(9), 1216–1222.
USEPA, 2007. Method 1694: Pharmaceuticals and personal care products in water, soil, sediment and biosolids by HPLC-MS/MS, «http://www.caslab.com/EPA-Methods/PDF/1694.pdf».
Valcárcel, Y., Alonso, S. G., Rodríguez-Gil, J. L., Maroto, R. R., Gil, A., & Catalá, M. (2011). Analysis of the presence of cardiovascular and analgesic/anti-inflammatory/antipyretic pharmaceuticals in river—and drinking-water of the Madrid Region in Spain. Chemosphere, 82(7), 1062–1071.
Valcárcel, S. Y., Alonso, G., Rodríguez-Gil, J. L., Castaño, A., Montero, J. C., Criado-Alvarez, J. J., Mirón, I. J., & Catalá, M. (2013). Seasonal variation of pharmaceuticals active compounds in surface (Tagus River) and tap water (Central Spain). Environmental Science and Pollution Research, 20, 1396–1412.
Vieno, N. M., Harkki, H., Tuhkanen, T., & Kronberg, L. (2007). Occurrence of pharmaceuticals in river water and their elimination in a pilot-scale drinking water treatment plant. Environmental Science and Technology, 41, 5077–5084.
Wiegel, S., Aulinger, A., Brockmezer, R., Harms, H., Loffler, J., Reincke, H., Schmidt, R., Stachel, B., Von Tumpling, W., & Wanke, A. (2004). Pharmaceuticals in the river Elbe and its tributaries. Chemosphere, 57, 107–126.
Wollenberger, L., Halling-Sorensen, B., & Kusk, K. O. (2000). Acute and chronic toxicity of veterinary antibiotics to Daphnia magna. Chemosphere, 40, 723–730.
Ying, G. G., Kookanab, R. S., & Kolpinc, D. W. (2009). Occurrence and removal of pharmaceutically active compounds in sewage treatment plants with different technologies. Journal of Environmental Monitoring, 11, 1498–1505.
Zhang, Y., Geißen, S.-U., & Gal, C. (2008). Carbamazepine and diclofenac: removal in wastewater treatment plants and occurrence in water bodies. Chemosphere, 73, 1151–1161.
Zhao, J. L., Ying, G. G., Wang, L., Yang, J. F., Yang, X. B., Yang, L. H., & Li, X. (2009). Determination of phenolic endocrine disrupting chemicals and acidic pharmaceuticals in surface water of the Pearl Rivers in South China by gas chromatography–negative chemical ionization–mass spectrometry. Science of the Total Environment, 407(2), 962–974.
Acknowledgments
The authors thank the National Research Program (CORE)—PN no. 13 N/2009 for the financial support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Gheorghe, S., Petre, J., Lucaciu, I. et al. Risk screening of pharmaceutical compounds in Romanian aquatic environment. Environ Monit Assess 188, 379 (2016). https://doi.org/10.1007/s10661-016-5375-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-016-5375-3