
Abstract
Low hemoglobin concentration is associated with increased mortality, but there is disagreement with regard to the clinical definition of anemia. We aimed to evaluate the prevalence, clinical correlates and association with total and cause-specific long-term mortality across the hemoglobin distribution and for previously proposed definitions of anemia. Blood hemoglobin concentration and mean corpuscular volume was measured in participants of the Malmö diet and cancer study—a prospective cohort study, and related to baseline characteristics and outcomes during follow-up. Primary endpoints were all-cause mortality, cardiovascular mortality and cancer-related mortality. A U-shaped association of hemoglobin with total mortality was observed in spline regression analyses, with nadir at hemoglobin 150 g/L among men and 130 g/L among women. Mortality increased steeply with more strict definitions of anemia, hazard ratio: 1.36, 1.94 and 2.16 for hemoglobin <140/130 (men/women), 132/122 and 130/120 g/L, respectively. Similar trends were seen for both cancer- and cardiovascular mortality. The incidence of coronary disease and cancer did not differ across groups. Erythrocyte volume was an independent predictor of mortality, with the highest mortality observed for macrocytic anemia, which was less prevalent than microcytic and normocytic anemia. Dietary intake of iron and vitamin B12 were significantly lower and use of antithrombotic medications was significantly higher in subjects with anemia. The World Health Organisation definition of anemia was associated with increased mortality (hazard ratio 2.16) but excess mortality was also observed at higher hemoglobin levels. Of morphological subtypes, anemia with macrocytosis was rare but associated with the highest mortality.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anemia, defined as a low blood concentration of hemoglobin, is a major determinant of morbidity globally. Anemia is associated with impaired oxygen delivery, decreased exercise tolerance and a reduced quality of life in older adults [1, 2]. It can also result in impaired tolerance for ischemia and has been associated with worsened outcomes in several diseases including renal failure, heart failure, myocardial infarction, and cancer [3–8].
Although many studies have described reference intervals for hemoglobin in healthy individuals, there is significant variability in the definition of anemia among clinical laboratories and few studies have described the distribution, clinical correlates and prognostic impact of hemoglobin concentration in the general population.
The most commonly used definition of anemia is the World Health Organization’s definition of a hemoglobin concentration below 130 g/L for men and 120 g/L for women [9, 10]. However, this definition has been criticized for largely being based on expert opinion and studies with potentially flawed measurement techniques. It was derived from a small study sample of healthy, young individuals which cannot be extrapolated to middle-aged or elderly individuals [11]. Furthermore, a recent study observed an adverse prognosis with a definition of anemia as high as a hemoglobin below 140 g/L for men and 130 g/L for women [12]. On the other hand, one study showed that the WHO definition might be clinically relevant [13]. Two surveys of large American databases suggested that a hemoglobin concentration below 132 g/L for men and 122 for women might be more clinically relevant with a prevalence of about 5 % in the general population [11].
Given the conflicting data of previous studies, we aimed to evaluate the prevalence, clinical correlates and impact of anemia on total and cause-specific mortality, using previously proposed definitions and across the range of the hemoglobin distribution in a middle-aged Swedish population (the Malmö Diet and Cancer Study, MDCS). We also studied the distribution and prognostic importance of the major clinical subclassifications of anemia, based on mean corpuscular volumes; micro-, normo-, and macrocytic anemia.
Methods
Study sample
The population-based Malmö Diet and Cancer Study (MDCS) [14, 15] included 30,447 men and women from a middle-aged Swedish population (age at inclusion 44–73 years, mean 58.0 years). In brief, all men born between 1923 and 1945 and women between 1923 and 1950 in the city of Malmö in southern Sweden were invited to participate, and the participation rate was approximately 40 %. All participants underwent a baseline examination between 1991 and 1996. Participants filled out a questionnaire including questions on smoking habits, physical activity, medical history and use of medications. Blood samples, anthropometrics and blood pressure measurements were collected at baseline. Hypertension was defined as either a systolic blood pressure of ≥140 mmHg, a diastolic blood pressure ≥90 mmHg, or the use of antihypertensive medication. The dietary intake of folate, vitamin B12 and iron was assessed in an interview-based, modified diet history method that combined (1) a 7 day menu-book for registration of lunch and dinner meals, cold beverages including alcohol, drugs and nutrient supplements (including iron, folate and vitamin B12 supplements); (2) a 168-item questionnaire for assessment of meal pattern, consumption frequencies, and portion sizes of regularly eaten foods; and (3) a 45-min complementary interview. Physical activity was measured as a score, incorporating different physical activities. The methods and validity of the methods have been described elsewhere [16–18]. Blood samples were analyzed with a Sysmex K-1000 using electric resistance detection for counting blood cells and the cyanmethemoglobin method for hemoglobin measurement. Analyses were performed consecutively at screening using fresh, heparinized blood samples. The representativity of MDCS for the general population of Malmö has previously been studied [19]. Participants in MDCS were on average slightly healthier, with a lower mortality than non-participants with a similar socio-demographic structure as the general population.
All individuals provided written, informed consent. The regional ethics committee approved the study.
Ascertainment of clinical end-points
Information on clinical endpoints was obtained by linkage of national healthcare registers to the unique personal identification number that every Swedish citizen receives upon birth or immigration [20]. Information on time and cause of death was obtained from the Swedish Cause of Death Register (CDR) [21] and information on coronary artery disease and cancer was obtained from the Swedish Hospital Discharge Register (HDR) [22]. These nation-wide registers include data on primary and contributory diagnoses from all hospitals in Sweden. The CDR includes diagnoses from death certificates since 1952, regardless if death occurred outside of Sweden. Diagnoses in the CDR are coded as primary or contributory to cause of death. Reporting of data to the HDR has been compulsory since 1987 but the Malmö University hospital, which is the only hospital serving the city, has been reporting since 1969. Diagnoses in both registers are based upon the International Classification of Disease (ICD), and the 8th edition (ICD-8) was used until the end of 1986, the 9th edition (ICD-9) between 1987 and 1996 and the 10th edition (ICD-10) from 1997 until present. The CDR includes information about the cause of death in >99 % of the total deaths in Sweden [23]. The diagnostic validity has been reported to be high, with positive predictive values of 90 % for neoplasms and 87 % for ischemic heart disease [24]. The HDR includes diagnoses for >99 % of discharged patients [25]. The HDR has been validated with a positive predictive value of 85–95 % for most diagnoses. Validity is higher for more severe conditions [e.g. myocardial infarction (>98 %) and malignancies] [22]. There is a high level of agreement (>90 %) between cause of death in the CDR and primary diagnosis in the HDR in myocardial infarction and neoplasms [21].
The predominant specific causes of death were defined from ICD codes in the CDR: death from cardiovascular causes (ICD-9: 390-459, ICD-10: I00-I99) and cancer-related death (ICD-9: 140-239, ICD-10: C00-C99). Other specific causes of death studied included hematologic causes (ICD-9: 280-289, ICD-10: D50-D77), digestive causes (ICD-9: 520-579, ICD-10: K), respiratory causes (ICD-9: 460-519, ICD-10: J), infectious disease (ICD-9: 001-139, ICD-10: A,B), and trauma (ICD-9: 800-999, ICD-10: V,W,X,Y). Incident coronary event was defined as myocardial infarction (ICD-9: 410, ICD-10: I21) or death due to ischemic heart disease (ICD-9: 412 or 414, ICD-10: I22-23 or I25). Cancer was defined as diagnosis codes 140-239 (ICD-9) and C00-C99 (ICD-10) in the HDR or CDR.
Statistical methods
The prevalence, clinical characteristics, and prognosis associated with anemia were evaluated across four previously proposed cut-off values for hemoglobin: 140/130 g/L (in men/women), 132/122, 130/120 and <110 [5, 9–11, 13]. Each anemia group was compared with the part of the population not included in the specific definition of anemia.
Erythrocyte volume and hemoglobin content were evaluated as independent predictors of mortality. The impact of subclassification into morphological subtypes (microcytic, normocytic and macrocytic anemia) and subtypes based on erythrocyte hemoglobin content (hypochromic, normochromic, hyperchromic) was evaluated. Microcytic anemia was defined as mean corpuscular volume (MCV) below 80 femtoliters (fL), normocytic anemia as MCV between 80 and 100 fL, and macrocytic anemia as MCV >100 fL. Hypochromic anemia was defined as mean corpuscular hemoglobin concentration (MCHC) below 320 g/L, normochromic anemia as MCHC between 320 and 360 g/L and hyperchromic anemia as MCHC above 360 g/L. In both subclassification analyses the group without anemia by any definition (above hemoglobin 140/130 g/L) was used as control group.
Baseline characteristics were compared between study participants with and without anemia according to each definition, using Fisher’s exact test, Student’s t test or Mann–Whitney’s U test, as appropriate.
The association of each definition of anemia with total mortality during 10 years of follow-up was evaluated using sex-stratified Cox proportional hazards regression analyses. Follow-up was defined as time from baseline examination to the time of an event or end of follow-up, with censoring after 10 years. Cox models were adjusted for potential confounders (determined a priori) including age, body mass index, hypertension, smoking, alcohol consumption, and physical activity. The association of anemia, according to each definition, with the predominant causes of mortality (coronary artery disease, cancer) and with case fatality in these diseases was also tested. Models with and without inclusion of pre-menopausal women were studied, to evaluate the impact of this healthier group, which could potentially bias mortality analyses because of lower hemoglobin levels.
The association of hemoglobin concentration with total mortality was also evaluated using a restricted cubic spline with knots at the 10th, 25th, 50th, 75th and 90th percentiles of hemoglobin.
P values below 0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics (version 20.0 IBM Corp., Armonk, NY, USA) or SAS version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Prevalence of anemia
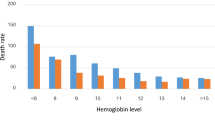
Hemoglobin measurements were available for 30,330 participants. The distribution of hemoglobin in male and female participants of the MDCS are shown in Online Resource 1, and the prevalence of anemia according to previously proposed definitions are shown in Table 1. A hemoglobin cut-off of 140 g/L for men and 130 g/L for women resulted in 6,713 subjects with anemia (prevalence 22.0 %). Restricting the cut-off to 132 and 122 g/L in men and women, respectively, resulted in a decline in prevalence to 1,719 subjects (5.6 %). Further restriction to 130 and 120 g/L in men and women, respectively, yielded a prevalence of 1,167 subjects (3.8 %). Finally, restriction to <110 g/L resulted in a prevalence of 171 subjects (0.6 %). The 5th percentile for male and female hemoglobin concentration was 134 and 121 g/L, respectively.
The distributions of major morphological subclasses of anemia across definitions are shown in Table 1. The proportion of patients with microcytosis or macrocytosis was significantly higher for each group of anemic patients compared to non-anemic patients. Further, the proportion of anemic individuals with microcytic anemia increased markedly with the more strict definitions of anemia, from 4.0 % (hemoglobin <140/130 g/L) to 57.9 % (<110 g/L). The proportion of macrocytic anemia also increased with more strict definitions, but remained low, from 1.0 % (<140/130 g/L) to 2.9 % (<110 g/L).
Baseline characteristics
The clinical characteristics at study baseline are presented in Table 2. We observed significant differences between the groups with lower age, larger proportion of females and large proportions of pre- and perimenopausal women for the more strict definitions of anemia. Subjects with anemia also had significantly lower BMI, consumed less alcohol, were less likely to report smoking and less often hypertensive. The dietary intake of iron and vitamin B12 were significantly lower in subjects with anemia, and in the groups with the lowest and highest Hb cut-off (<140/130 and <110) no significant differences in use of antithrombotic medications were noted. Pre-menopausal women had significantly lower hemoglobin (mean 133.2 g/L) than post-menopausal women (mean 137.5 g/L, P < 0.01).
Prognosis of anemia
During up to 10 years of follow-up, a total of 2,651 (8.7 %) participants died, 912 (3.1 %) died from cardiovascular disease and 1,218 (4.1 %) from cancer-related causes. 1,473 subjects (5.0 %) were diagnosed with coronary artery disease and 1,426 (4.8 %) were diagnosed with cancer during follow-up. Other important causes of death were less common, as shown in Online Resource 2.
The adjusted relative risk of total mortality across the range of hemoglobin is illustrated in Fig. 1. An inverse U shaped association with mortality was observed in both men and women. Mortality risk was lowest for hemoglobin 150 in men and 130 in women and increased as hemoglobin deviated from around 145–165 g/L for men and 120–145 g/L for women. This relative risk increase was particularly marked for a hemoglobin concentration below 130 g/L for men and 120 g/L for women. The results of the unadjusted cubic spline were similar, as shown in Online Resource 3.

Cubic splines describing the adjusted hazard ratios for 10-year all-cause mortality as a function of hemoglobin concentration. P for non-linear association <0.0001 for both men and women. Knots placed at 10th, 25th, 50th, 75th and 90th percentiles. Adjusted for age, BMI, hypertension, smoking, physical activity and alcohol consumption
All diagnostic definitions of anemia were associated with a higher total mortality compared to no anemia as shown in Table 3. All diagnostic definitions were also associated with an increased risk of cardiovascular mortality and the risk increased proportionally with increasingly strict definition. All definitions were also significantly associated with increased risk of cancer mortality, except for subjects with hemoglobin <110 in whom confidence intervals were wide. An expanded model with inclusion of prevalent heart failure to the model yielded similar results (Online Resource 4). Other important causes of death were too rare for statistical analyses, but rates of death from non-malignant gastrointestinal diseases and infectious diseases were numerically higher in subjects with anemia, as shown in Online Resource 2. Inclusion of premenopausal women did not significantly change the results (data not shown).
Anemia was associated with an increased risk of mortality related to renal disease for two of the definitions of anemia (132/122 and 130/120, with HR 8.08 and HR 13.22 respectively, both P < 0.01) but was not significant for the most lenient definition (140/130, HR 2.34, P = 0.13) as shown in Online resource 6. However, renal mortality was rare (n = 4 for the 132/122 and 130/120 groups, n = 6 for the 140/130 group) and no cases of renal mortality were noticed in the group with the lowest Hb.
A total of 1,473 participants were diagnosed with an incident coronary event (4.8 %). The incidence of coronary events and incident cancer were similar in all groups, and no significant risk increase was seen with anemia by any definition. The distribution of major organ-specific cancers associated with anemia is illustrated in Online Resource 5.
Subclassification by erythrocyte volume and hemoglobin content
Hemoglobin concentration and MCV were independently associated with all-cause mortality in the MDCS, while a multiplicative interaction term was not significant.
Mortality risks of patients with anemia subclassified by erythrocyte volume are shown in Table 4. Risk of total mortality was increased in all groups compared to subjects without anemia and was highest in subjects with macrocytosis for all definitions of anemia, except for the group with the lowest hemoglobin, which was not statistically significant. The risk of cancer mortality was also highest in subjects with macrocytosis, and a similar non-significant trend was observed for cardiovascular mortality although confidence intervals were wide. Risk of cardiovascular mortality and cancer mortality was higher in subjects with normocytosis compared to subjects without anemia, but was not significantly higher in the smaller group with microcytosis. The group with hemoglobin <110 was too small to observe any significant increase in mortality.
Compared to subjects with anemia and normocytosis, risk of total mortality and cancer mortality was higher in subjects with macrocytosis, as shown in Online Resources 7. In contrast, mortality was not significantly different with microcytosis as compared to subjects with normocytosis for any definition of anemia.
Hemoglobin concentration and MCHC were also independently associated with all-cause mortality in the MDCS, while a multiplicative interaction term was not significant. The distributions of MCHC in the non-anemic population and in participants with anemia across definitions are shown in Online Resource 8. The proportion of anemic subjects with hypochromic anemia increased with a more strict definition of anemia while the proportion with hyperchromic anemia declined. Associations of MCHC subgroups with mortality are shown in Online Resource 9. Increased cardiovascular mortality was observed when the anemia was hypochromic (HR 1.97, 2.61, 3.77 and 0.71 for 140/130, 132/122, 130/120 and <110 respectively) as compared to normochromic anemia. No case of hyperchromic anemia was noticed in the group with the most strict definition of anemia (<110).
Discussion
The present study evaluated the prevalence, clinical correlates and prognostic impact of anemia across the entire range of the hemoglobin distribution and using previously proposed definitions in a middle-aged population. Our results provide several important insights on the epidemiology of anemia in middle-aged subjects.
First, we observed a U-shaped association of hemoglobin with total mortality over 10 years, with the lowest risk for hemoglobin 150 g/L for men and 130 g/L for women. Anemia as defined according to the WHO was associated with a hazard ratio of 2.16 (95 % confidence interval 1.80–2.60), but excess mortality was observed at even higher hemoglobin (as high as 140 g/L for men and 130 g/L for women). However, the relative hazard ratio increased the lower cutoff points that were used. The lowest proposed hemoglobin cut-off of 110 g/L resulted in a very small group, smaller than in some previous studies, likely reflecting the population-based study design. Prevalence estimates were otherwise similar to the few previous studies in middle-aged subjects, ranging from 4 % for the WHO definition to 22 % for the least strict definition (Hb <140/130 g/L), and consistent with observations in elderly subjects [5]. Thus, anemia definitions that include individuals with a slightly increased mortality risk come at the price of a markedly higher prevalence of over one fifth of the middle-aged population. However, our findings indicate that hemoglobin concentrations <140 g/L in men and <130 g/L in women merit some degree of monitoring and evaluation. These findings were consistent when including premenopausal women.
Second, anemia by all definitions was associated with excess risk of both cancer-related and cardiovascular mortality—the two major causes of death in the western population. The risk of incident cancer was not significantly different between groups. The incidence of coronary disease was also not increased compared to individuals without anemia. This observation indicates an effect on case fatality rate in myocardial infarction rather than disease incidence per se, possibly due to effects of reduced oxygen transport to ischemic tissues. Another possibility is that anemia, despite not being directly related to the pathophysiology of coronary artery disease per se, might be associated with other factors such as inflammation, which could influence case-fatality. Several studies have reported increased mortality in patients hospitalized for coronary artery disease with anemia and in heart failure patients with anemia [3–5, 26], and there is ongoing debate about the benefits and risks of blood transfusion in such patient groups. Our study observed substantially increased case fatality and is the first, as far as we are aware, to provide prospective data on case fatality rate in coronary disease in the general population with information on both hospitalized subjects and subjects who died before reaching the hospital. Mortality related to renal disease was also greatly increased for two of the definitions of anemia (132/122 and 130/120). This likely reflects the close relationship between kidney disease and anemia. However, renal mortality was rare and confidence intervals were wide.
Third, erythrocyte volume predicted mortality independently of hemoglobin, with the highest mortality observed for macrocytic anemia, which was less prevalent than microcytic and normocytic anemia. This unexpected observation has not previously been reported. The principal causes of macrocytic anemia are considered to be deficiency of folic acid or vitamin B12, hypothyroidism, alcohol abuse, and hematologic malignancies [27]. Particularly the latter would be expected to also substantially impact survival, which is also further corroborated by the considerably increased risk of cancer-related mortality in subjects with anemia. Our findings therefore highlight the importance of careful evaluation of subjects with macrocytic anemia. Total mortality was similarly increased with microcytic and normocytic anemia as compared to subjects without anemia. The most common cause of microcytic anemia in this population is likely to be iron-deficiency anemia, often resulting from gastrointestinal bleeding/cancer, and perhaps anemia on the basis of chronic disease, as the prevalence of thalassemia is low in Sweden. Normocytic anemia most likely reflects inflammation, chronic disease or renal failure [28]. No significant differences were noted between mortality risk for microcytic anemia and normocytic anemia.
Finally, our results confirm a substantial role for menopause on the population distribution of hemoglobin in middle-aged subjects. Female sex, lower age, and pre- or perimenopause were strongly associated with anemia. No significant association was observed with use of antithrombotic medications in the groups with the highest and lowest hemoglobin, which might indicate a modest contribution to anemia in the middle-aged population. Alcohol consumption was lower in participants with anemia. This association was independent of age, only significant in male participants and remained significant after exclusion of participants reporting no alcohol consumption. This observation could potentially reflect male anemic participants being less healthy, treated as outpatients and less inclined to consume alcohol. Other important factors associated with increased risk of anemia included low dietary intake of vitamin B12 and iron—underscoring benefits with improved population interventions to provide dietary recommendations. However, our study provides no direct information with regard to the benefits and risks of correcting anemia. Studies have also shown an association between blood transfusion and adverse outcomes [29, 30], which have motivated careful and conservative treatment strategy, with blood transfusions withheld for very low hemoglobin concentrations in critically ill patients. This treatment strategy is therefore unlikely to be appropriate for these individuals who seem to be at a high risk even though they lack other comorbidities. Other treatment options for anemia have been developed, including erythropoietin therapy and iron infusions that might be beneficial for patients with less severe anemia [31, 32] although these treatments might have other drawbacks that need to be taken into consideration [33]. Improved diagnostics and attempts to correct nutritional deficiencies, alcohol overconsumption and optimized therapy for any chronic diseases associated with anemia would therefore likely be the most effective ways to reduce the disease burden of anemia in the population. Indeed, it has previously been shown that clinical anemia is one of the last manifestations of iron deficiency and one of the first to get corrected when adequate supplementation and treatment is initiated. It may however be important to continue treatment even after the hemoglobin concentration has normalized, to replenish body stores of iron [34, 35].
Our study was a large, contemporary, population-based cohort study of middle-aged subjects. However, our study also has limitations which merit consideration. First, this study was based on a single laboratory hemoglobin value, why we are unable to further characterize measurement errors and transient anemia, which has previously been shown to have a small impact on outcomes [26]. However, the assay used for measurement was used clinically at the time and has been shown to have low intra-reader variability, and the impact of transient anemia, if any, is expected to bias our results to the null and unlikely to positively confound our results. Further, even though several potential confounding factors were included in the multivariate models, we did not have data on to what extent smoking, alcohol intake and other confounding factors changed during the 10-year follow-up period. Finally, measures of renal function, inflammation, bleeding disorders and hematologic disorders were not available in this study, and adjustment for these important determinants of anemia was therefore not possible. However, a random subgroup of MDCS participants (n = 5,413) underwent further testing including high-sensitive C-reactive protein (CRP) and creatinine measurements from which estimated glomerular filtration rate (eGFR) could be calculated using the Cockcroft-Gault formula. In that subcohort, only 5 (<0.1 %) participants had severely reduced renal function (eGFR below 30), and 695 participants (13 %) had moderately reduced renal function (eGFR between 30 and 60). Increasing prevalence of moderately reduced eGFR with stricter definitions of anemia was noticed (17, 20, 21 and 39 % for 140/130, 132/122, 130/120 and <110 respectively). CRP was not significantly different between the different definitions of anemia compared to the non-anemic subjects except in the most lenient anemic definition (140/130 g/L), which had lower CRP than non-anemic participants.
In conclusion, the present study found that the prevalence of anemia in a general, middle-aged Swedish population was common, ranging from between 0.6 and 22 % depending on the definition. Anemia by all definitions was associated with an increased risk of all-cause, cardiovascular and cancer-related mortality, particularly with the less prevalent macrocytic anemia. The upper diagnostic cut-off below which excess mortality was evident was 140 g/L in men and 130 g/L in women. Our results provide novel information on the epidemiology of anemia and highlight the importance of careful evaluation and follow-up of middle-aged individuals with anemia even with a lenient definition, particularly in the context of macrocytic anemia.
References
Penninx BW, Pahor M, Cesari M, et al. Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J Am Geriatr Soc. 2004;52(5):719–24.
Thomas DR. Anemia and quality of life: unrecognized and undertreated. J Gerontol A Biol Sci Med Sci. 2004;59(3):238–41.
Hamm CW, Bassand J-P, Agewall S, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2011;32(23):2999–3054.
Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12065 patients with new-onset heart failure. Circulation. 2003;107(2):223–5.
Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005;111(16):2042–9.
Bolińska S, Sobkowicz B, Zaniewska J, et al. The significance of anaemia in patients with acute ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Kardiologia Polska. 2011;69(1):33–9.
Caro JJ, Salas M, Ward A, Goss G. Anemia as an independent prognostic factor for survival in patients with cancer: a systemic, quantitative review. Cancer. 2001;91(12):2214–21.
Winther SA, Finer N, Sharma AM, Torp-Pedersen C, Andersson C. Association of anemia with the risk of cardiovascular adverse events in overweight/obese patients. Int J Obes (Lond). Prepublished on Jun 18 2013. doi:10.1038/ijo.2013.111.
World Health Organisation. Hemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva: World Health Organization; 2011.
World Health Organisation. Nutritional anaemias. Report of a WHO Scientific Group. Geneva: World Health Organisation; 1968.
Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006;107(5):1747–50.
Culleton BF, Manns BJ, Zhang J, Tonelli M, Klarenbach S, Hemmelgarn BR. Impact of anemia on hospitalization and mortality in older adults. Blood. 2006;107(10):3841–6.
Izaks GJ, Westendorp RGJ, Knook DL. The definition of anemia in older persons. JAMA. 1999;281(18):1714–7.
Berglund G, Elmstähl S, Janzon L, Larsson SA. The Malmo diet and cancer study. Design and feasibility. J Intern Med. 1993;233(1):45–51.
Smith JG, Platonov PG, Hedblad B, Engström G, Melander O. Atrial fibrillation in the Malmö diet and cancer study: a study of occurrence, risk factors and diagnostic validity. Eur J Epidemiol. 2010;25(2):95–102.
Riboli E, Elmstahl S, Saracci R, Gullberg B, Lindgarde F. The Malmo food study: validity of two dietary assessment methods for measuring nutrient intake. Int J Epidemiol. 1997;26(Suppl 1):161–73.
Wirfalt E, Mattisson I, Johansson U, Gullberg B, Wallstrom P, Berglund G. A methodological report from the Malmo diet and cancer study: development and evaluation of altered routines in dietary data processing. Nutr J. 2002;1:3.
Ericson UC, Ivarsson MI, Sonestedt E, et al. Increased breast cancer risk at high plasma folate concentrations among women with the MTHFR 677T allele. Am J Clin Nutr. 2009;90(5):1380–9.
Manjer J, Carlsson S, Elmståhl S, Gullberg B, Janzon L, Lindström M, Mattisson I, Berglund G. The Malmö diet and cancer study: representativity, cancer incidence and mortality in participants and non-participants. Eur J Cancer Prev. 2001;10(6):489–99.
Ludvidgsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24(11):659–67.
Johansson LA, Westerling R. Comparing Swedish hospital discharge records with death certificates: implications for mortality statistics. Int J Epidemiol. 2000;29(3):495–502.
Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450.
Dödsorsakstatistik—Historik, metoder och tillförlitlighet. Socialstyrelsen. http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/18019/2010-4-33.pdf (14 May 2014).
Johansson LA, Björkenstam C, Westerlin R. Unexplained differences between hospital and mortality data indicated mistakes in death certification: an investigation of 1,094 deaths in Sweden during 1995. J Clin Epidemiol. 2009;62(11):1202–9.
Kvalitet och innehåll i patientregistret: Utskrivningar från 1964–2007 och besök i specialiserad öppenvård (exklusive primärvårdsbesök) 1997-2007. Socialstyrelsen. http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/8306/2009-125-15_200912515_rev2.pdf (14 May 2014).
Valente S, Lazzeri C, Chiostri M, Sori A, Giglioli C, Gensini GF. Prior and new onset anemia in ST-elevation myocardial infarction: a different prognostic role? Intern Emerg Med. 2011;6(4):329–36.
Aslina F, Mazza JJ, Yale SH. Megaloblastic anemia and other causes of macrocytosis. Clin Med Res. 2006;4(3):236–41.
Beyer I, Compté N, Busuioc A, Cappelle S, Lanoy C, Cytryn E. Anemia and transfusions in geriatric patients: a time for evaluation. Hematology. 2010;15(2):116–21.
Wu W-C, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarctions. N Engl J Med. 2001;345(17):1230–6.
Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667–74.
Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation. 2003;107(2):294–9.
Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol. 2000;35(7):1737–44.
Skali H, Parving H-E, Parfrey PS, et al. Stroke in patients with type 2 diabetes mellitus, chronic kidney disease, and anemia treated with Darbepoetin Alfa. Circulation. 2011;124(25):2903–8.
Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut. 2000;46(Suppl IV):iv1–iv5.
Mahoney DH Jr. Anemia in at-risk populations—what should be our focus? Am J Clin Nutr. 2008;88(6):1457–8.
Acknowledgments
The Malmö Diet and Cancer study was made possible by grants from the Swedish Cancer Society, the Swedish Medical Research Council, the Swedish Dairy Association, the Albert Påhlsson and Gunnar Nilsson Foundations and the Malmö city council. J.G.S. was supported by the Swedish Heart–Lung Foundation, governmental funding of clinical research within the Swedish National Health Service, the Ulla Ekdahl foundation, the Thorsten Westerström foundation and Skåne University Hospital in Lund.
Conflict of interest
The authors declare no competing interests. All individuals provided written, informed consent. The regional ethics committee approved of the study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Martinsson, A., Andersson, C., Andell, P. et al. Anemia in the general population: prevalence, clinical correlates and prognostic impact. Eur J Epidemiol 29, 489–498 (2014). https://doi.org/10.1007/s10654-014-9929-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-014-9929-9