
Abstract
Evolution of the industrialized society had led to a risk management policy in many domains. Assessment of health care risk in the case of infectious diseases often includes mathematical models. Results of modelling were used in France to design emergency plans against flu pandemic. We believe that models cannot predict the features of the future outbreaks because the intrinsic properties of an emergent pathogen and the ecosystem in which it is developing are very complex. Of course, prediction of future outbreaks is not possible without using models, but we think that it is an illusion to presently believe that an emerging phenomenon can be anticipated by using only prediction from models. The recent pandemic caused by the novel A/H1N1 virus has confirmed the unpredictability of infectious diseases. The rapid evolution in several domains such as antimicrobial therapeutics, vaccine and hygiene conditions make comparison with past pandemics hard. The adherence of populations to prevention measures and immunisation campaigns are unpredictable. In addition, the presentation of pessimistic models is deleterious. They impress governments and provoke fears. There is a striking necessity to develop the number and the capacities of sentinel centres to take and adapt decisions based on timely available scientific information.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
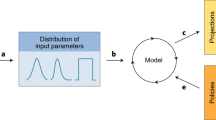
Evolution of society had led to a risk management policy in many domains. The assessment of health care risk in infectious diseases, especially concerning future epidemics, often includes mathematical models which tentatively predict in silico the burden of the future outbreaks such as attack rate, dissemination, morbidity or mortality. Currently, models are designed to run with different scenarios, and probabilistic methods allow testing their performance in a number of situation. But the question asked by physicians, scientists and in fact everyone is “how many people will die, how many will be hospitalized?”. Such predictions from models were used in France to design the emergency plan against flu pandemic [1]. We believe that models cannot predict with acceptable accuracy the features of the future outbreaks because the intrinsic properties of an emergent pathogen and the ecosystem in which it is developing are very complex and unstable. Of course, prediction of future outbreaks is not possible without using models, but we think that it is an illusion to presently believe that an emerging phenomenon can be anticipated by using only prediction from models. The recent pandemic caused by the novel A/H1N1 virus has confirmed the unpredictability of infectious diseases.
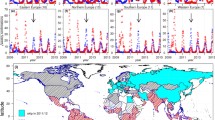
Seasonality of respiratory infections is a well-known phenomenon in temperate regions. Flu has long been associated with cold season, and the word “Influenza” comes from “influenza di freddo” in Italian that means “cold influenced”. A marked peak of respiratory infections occurs during cold winter months. Several mechanisms have been proposed to explain it, such as seasonal environmental changes (temperature humidity), seasonal host-behaviour changes and seasonal changes in host physiology (melatonin, vitamin D) [2–4]. However, there is still no clear understanding of this phenomenon. In contrast, disease seasonality is less defined in tropical regions where a background of influenza cases is observed throughout the year on top of which epidemics occur at intermediate months between the influenza season in temperate countries of the Northern and Southern hemispheres [4]. On the top, none of yet proposed determinants can explain why the four last pandemics of influenza (1918, 1957, 1968, and 2009) did not initiate during the cold season.
Interference between several respiratory viruses affecting the spread of influenza was recently described in Europe and drastically modified the dynamics of the outbreak [5, 6]. In France and in Sweden, an epidemic of rhinovirus infections occurred after the start of school year, and delayed the onset of the A/H1N1 pandemic. We also observed in Marseille that the epidemic of Respiratory Syncytial Virus bronchiolitis, which happens usually just before the seasonal flu epidemic, occurred later in the season, just after that the A/H1N1 pandemic started to decline. In addition interference between several Influenza viruses remains not properly known: at the beginning of the A/H1N1 pandemic, nobody was able to predict whether seasonal influenza strains (H3N2 and H1N1) would still provoke an epidemic wave or not.
In certain groups of population, the presence of cross-reactive antibodies against a new pandemic strain of influenza can heavily affect viral dissemination and therefore impact on the epidemiologic characteristics of the pandemic (total number of cases, age of the cases, number of severe cases, number of deaths, death rate, length of the phenomenon…) and seems unpredictable. The fact that the elderly were partially protected against the novel A/H1N1 [7–9] explains that the novel A/H1N1 virus infected mostly young people. In addition, at-risk groups may not be the same as for seasonal flu. For example, obesity was an undisputable independent risk factor of severity and lethality during the A/H1N1 pandemic [10, 11].
The inherent variability of new variants makes predictions difficult. Each pandemic virus has its own intrinsic properties which can evolve during the pandemic period. Then, intrinsic pathogenicity of new pandemic variants appears to be unpredictable. Experimental data derived from animal models must not be directly extrapolated to humans: in the A/H1N1 case, experiences with ferrets predicted a severity of pneumonia intermediate between that due to seasonal virus and the highly pathogenic avian H5N1 virus [12]. But in fact, the fatality rate of the novel A/H1N1 virus was relatively mild.
The novel 2009 H1N1 virus reminded the 1918 pandemic, also caused by a H1N1 virus, despite totally distinct, which was associated with a large number of secondary bacterial co-infection which could explain partially the huge number of deaths [13]. Because of drastically different sanitary conditions nowadays, it is awkward to use the 1918 data as a basis for anticipating the spread, severity, and health consequences of present and future H1N1 pandemics. Currently, the use of antibiotics and anti-pneumococcal vaccines allow to efficiently combat the historically lethal bacterial co-infections. The availability of adapted vaccine and the rapid evolution on several domains such as antiviral therapeutics and hygiene conditions are likely to play a critical role in the burden of these new pandemic variants as well as the increase of air traffic in their spread. Some models take into account the impact of human interventions such as vaccine/antiviral delivery, isolation of infected patients, school closure, halting air traffic and non-pharmaceutical interventions. Moreover, it remains often difficult to evaluate their real impact even without applying any model. For example, it was only in the late 90s that hand washing indisputably demonstrated, through randomized trials, its efficacy to prevent inter-human transmission in developed countries [14, 15]. In 2005, a randomized-trial in Pakistan confirmed it in low-income countries [16]. Furthermore, the efficacy of mask use, largely recommended during A/H1N1 pandemic, to prevent respiratory infections is still to be clearly established by randomized trials [17–19]. Thereby, their introduction into models seems very tricky.
The vast majority of studies showed that immunization against influenza has a true impact in terms of hospitalization rate, global morbidity, influenza associated mortality as well as global mortality [20–26]. Intriguingly, during the immunisation campaign against the A/H1N1 pandemic virus, a large proportion of the population was reluctant to accept vaccination in some countries such as France and Germany. Human behaviours often are unpredictable and could vary among countries and vary with time. In France, the negative image provided by the mass media could have contributed to the low uptake of the A/H1N1 vaccine. We observed and reported that in public hospitals of Marseille, the nurses were less immunised against the new A/H1N1 pandemic virus than against seasonal flu [27]. Fears of vaccination promoted by anti-immunization lobbies are largely relayed by the media and the doubts induced and amplified by mediatisation persists for a long time, even when scientists have demonstrated that there is no scientific evidence for suspicion. The association between multiple sclerosis and hepatitis B vaccine on one hand [28], and between autism and measles vaccine on the other hand [29] will be standing for many years to come, and any model is able to predict these events. One model can predict the willingness to accept a vaccine only for one specific situation. External factors cannot be included into models because they are often unknown until they appear. In France, the fact that medical information about the A/H1N1 vaccine was delivered and promoted primarily by politicians could have a counterproductive effect. Medical recommendations bypassing the medical system arouse suspicion in the population [27].
With hindsight, the recent pandemic reinforces the idea that presentation of pessimistic models mostly based on extrapolated hypotheses is deleterious. They impress governments and provoke fears. In another hand, it has been previously observed that pessimistic hypothesis about bioterrorism based only on speculations led governments to elaborate countermeasure plans with disproportionate measures. The Dark Winter operation, a bio-terrorist attack simulation, resembles movie script more than reality. Fears of a putative H5N1 avian flu pandemic amplified by pessimistic figures based on unsupported prediction constrained governments to implement emergency flu plans. Later on, these plans postulated that the fatality rate will be close to that observed in cases of A/H5N1 infection. For example, In France the 2009 emergency plan against pandemic flu predicted 91,000–212,000 deaths [1]. But A/H5N1 virus is still an almost pure zoonotic agent with transmission properties drastically distinct from those of the human adapted H1N1, H2N2 or H3N2 viruses. During the A/H1N1 pandemic in Marseille, no intermediate measure had been planified between (i) maintaining the organisation and logistics of the public hospital system as it was before the crisis, and (ii) the emergency opening of a 700 bed-hospital exclusively dedicated for A/H1N1 infected patients. In the real-life situation, along 10 months pandemic period, more than 2,500 clinical specimens were laboratory-documented: of these patients, around 11% were hospitalized and used simultaneously less than 50 beds at the peak of the pandemic.
In conclusion, infectious diseases remain unpredictable with mathematical models because pathogens and their ecosystem evolve continuously in a very unstable manner. Of course, some models which take into consideration the antiviral/antimicrobial therapies, the vaccines, the sanitary condition and the non-pharmaceutical interventions are useful to anticipate some logistic problems (quantity–purchase) and can help to prepare the response to the future pandemics but they cannot predict with acceptable accuracy the major features of a future pandemic (number of cases, hospitalization, deaths). The pessimistic predictions resulting from bioterrorism and the putative avian flu outbreak were published in highly-rated scientific journals. However, they were neither supported by indisputable scientific evidence nor confirmed in real-time up to now. They fuelled fears in the population through amplification by the media, causing great concern amongst the public and the politicians. In order to fight future outbreaks and as a complementary approach of modelling methods, we need to reinforce the network of sentinel centres by increasing their timely detection/diagnostics capacities and by implementing a large variety of technological tools detecting abnormal events. The data from these sentinel centres should not be necessarily exhaustive but they require to produce sufficient amount of data to investigate emergence and epidemic tendencies. Coupled with the fact that data from hospital-based surveillance systems and Google searching tools are easily and timely available, such surveillance method system will not be very costly. Our capacity for analysis and laboratory documentation needs to be increased and better integrated; during a crisis all data must be rapidly shared using communication media such as internet [30]. Rapid communication of research using specific free media such as Promed and ‘PloS Currents: Influenza’ can also improve the information dissemination. In addition, very early data about a new variant could be incorporate in some models and then produce more accurate predictions. Furthermore, decision process should be based on timely available scientific data to allow decision makers to take real time decision. Precautionary principle should be advantageously replaced by alertness principle.
References
Secrétariat général de la défense nationale (république française). Plan national de prévention et de lutte « pandémie grippale » n° 150/sgdn/pse/pps du 20 février 2009. Available:http://www.Pandemie-grippale.Gouv.Fr/img/pdf/plan_pg_2009.Pdf. Accessed on 4 Nov 2007.
Dowell SF. Seasonal variation in host susceptibility and cycles of certain infectious diseases. Emerg Infect Dis. 2001;7:369–74.
Lipsitch M, Viboud C. Influenza seasonality: lifting the fog. Proc Natl Acad Sci USA. 2009;106:3645–6.
Lofgren E, Fefferman NH, Naumov YN, Gorski J, Naumova EN. Influenza seasonality: underlying causes and modeling theories. J Virol. 2007;81:5429–36.
Casalegno JS, Ottmann M, Duchamp MB, Escuret V, Billaud G, Frobert E, Morfin F, Lina B. Rhinoviruses delayed the circulation of the pandemic influenza a (h1n1) 2009 virus in france. Clin Microbiol Infect. 2010;16:326–9.
Linde A, Rotzen-Ostlund M, Zweygberg-Wirgart B, Rubinova S, Brytting M. Does viral interference affect spread of influenza? Euro Surveill. 2009;14:19354.
Hancock K, Veguilla V, Lu X, Zhong W, Butler EN, Sun H, Liu F, Dong L, DeVos JR, Gargiullo PM, Brammer TL, Cox NJ, Tumpey TM, Katz JM. Cross-reactive antibody responses to the 2009 pandemic h1n1 influenza virus. N Engl J Med. 2009;361:1945–52.
Miller E, Hoschler K, Hardelid P, Stanford E, Andrews N, Zambon M. Incidence of 2009 pandemic influenza a h1n1 infection in england: a cross-sectional serological study. Lancet. 2010;375:1100–8.
Nougairede A, Ninove L, Zandotti C, Salez N, Mantey K, Resseguier N, et al. Novel virus influenza a (h1n1sw) in South-Eastern France, April–August 2009. PLoS One. 2010;5:e9214.
Intensive-care patients with severe novel influenza a (h1n1) virus infection-michigan, June 2009. MMWR Morb Mortal Wkly Rep 2009;58:749–752.
Vaillant L, La Ruche G, Tarantola A, Barboza P. Epidemiology of fatal cases associated with pandemic h1n1 influenza 2009. Euro Surveill. 2009;14:19309.
van den Brand JM, Stittelaar KJ, van Amerongen G, Rimmelzwaan GF, Simon J, de Wit E, Munster V, Bestebroer T, Fouchier RA, Kuiken T, Osterhaus AD. Severity of pneumonia due to new h1n1 influenza virus in ferrets is intermediate between that due to seasonal h1n1 virus and highly pathogenic avian influenza h5n1 virus. J Infect Dis. 2010;201:993–9.
Morens DM, Taubenberger JK, Fauci AS. Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. J Infect Dis. 2008;198:962–70.
Niffenegger JP. Proper handwashing promotes wellness in child care. J Pediatr Health Care. 1997;11:26–31.
Roberts L, Smith W, Jorm L, Patel M, Douglas RM, McGilchrist C. Effect of infection control measures on the frequency of upper respiratory infection in child care: a randomized, controlled trial. Pediatrics. 2000;105:738–42.
Luby SP, Agboatwalla M, Feikin DR, Painter J, Billhimer W, Altaf A, Hoekstra RM. Effect of handwashing on child health: a randomised controlled trial. Lancet. 2005;366:225–33.
MacIntyre CR, Cauchemez S, Dwyer DE, Seale H, Cheung P, Browne G, Fasher M, Wood J, Gao Z, Booy R, Ferguson N. Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis. 2009;15:233–41.
Aiello AE, Murray GF, Perez V, Coulborn RM, Davis BM, Uddin M, Shay DK, Waterman SH, Monto AS. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. 2010;201:491–8.
Cowling BJ, Fung RO, Cheng CK, Fang VJ, Chan KH, Seto WH, Yung R, Chiu B, Lee P, Uyeki TM, Houck PM, Peiris JS, Leung GM. Preliminary findings of a randomized trial of non-pharmaceutical interventions to prevent influenza transmission in households. PLoS One. 2008;3:e2101.
Christenson B, Lundbergh P, Hedlund J, Ortqvist A. Effects of a large-scale intervention with influenza and 23-valent pneumococcal vaccines in adults aged 65 years or older: a prospective study. Lancet. 2001;357:1008–11.
Kwong JC, Stukel TA, Lim J, McGeer AJ, Upshur RE, Johansen H, Sambell C, Thompson WW, Thiruchelvam D, Marra F, Svenson LW, Manuel DG. The effect of universal influenza immunization on mortality and health care use. PLoS Med. 2008;5:e211.
Nichol KL, Lind A, Margolis KL, Murdoch M, McFadden R, Hauge M, Magnan S, Drake M. The effectiveness of vaccination against influenza in healthy, working adults. N Engl J Med. 1995;333:889–93.
Nichol KL, Margolis KL, Wuorenma J, Von Sternberg T. The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 1994;331:778–84.
Nichol KL, Nordin J, Mullooly J, Lask R, Fillbrandt K, Iwane M. Influenza vaccination and reduction in hospitalizations for cardiac disease and stroke among the elderly. N Engl J Med. 2003;348:1322–32.
Nichol KL, Nordin JD, Nelson DB, Mullooly JP, Hak E. Effectiveness of influenza vaccine in the community-dwelling elderly. N Engl J Med. 2007;357:1373–81.
Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M. The japanese experience with vaccinating schoolchildren against influenza. N Engl J Med. 2001;344:889–96.
Nougairede A, Lagier JC, Ninove L, Sartor C, Badiaga S, Botelho E, Brouqui P, Zandotti C, De Lamballerie X, La Scola B, Drancourt M, Gould EA, Charrel RN, Raoult D. Likely correlation between sources of information and acceptability of a/h1n1 swine-origin influenza virus vaccine in marseille, france. PLoS One. 2010;5:e11292.
Herroelen L, de Keyser J, Ebinger G. Central-nervous-system demyelination after immunisation with recombinant hepatitis b vaccine. Lancet. 1991;338:1174–5.
Lee JW, Melgaard B, Clements CJ, Kane M, Mulholland EK, Olive JM. Autism, inflammatory bowel disease, and mmr vaccine. Lancet. 1998;351:905.
Raoult D. Rapport sur le bioterrorisme. France: Ministère de la santé de la famille et des personnes handicapées; 2003.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nougairède, A., Charrel, R.N. & Raoult, D. Models cannot predict future outbreaks: A/H1N1 virus, the paradigm. Eur J Epidemiol 26, 183–186 (2011). https://doi.org/10.1007/s10654-010-9533-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-010-9533-6