
Abstract
New therapeutic targets are needed to fight cancer. Aurora kinases (AK) were recently identified as vital key regulators of cell mitosis and have consequently been investigated as therapeutic targets in preclinical and clinical studies. Aurora kinase inhibitors (AKI) have been studied in many cancer types, but their potential capacity to limit or delay metastases has rarely been considered, and never in adrenal tissue. Given the lack of an effective pharmacological therapy for adrenal metastasis and adrenocortical carcinoma, we assessed AKI (VX-680, SNS314, ZM447439) in 2 cell lines (H295R and SW13 cells), 3 cell cultures of primary adrenocortical metastases (from lung cancer), and 4 primary adrenocortical tumor cell cultures. We also tested reversan, which is a P-gp inhibitor (a fundamental efflux pump that can extrude drugs), and we measured AK expression levels in 66 adrenocortical tumor tissue samples. Biomolecular and cellular tests were performed (such as MTT, thymidine assay, Wright’s staining, cell cycle and apoptosis analysis, Western blot, qRT-PCR, and mutation analysis). Our results are the first to document AK overexpression in adrenocortical carcinoma as well as in H295R and SW13 cell lines, thus proving the efficacy of AKI against adrenal metastases and in the SW13 cancer cell model. We also demonstrated that reversan and AKI Vx-680 are useless in the H295R cell model, and therefore should not be considered as potential treatments for ACC. Serine/threonine AK inhibition, essentially with VX-680, could be a promising, specific therapeutic tool for eradicating metastases in adrenocortical tissue.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aurora kinases (AK) are serine/threonine kinases fundamental to mitosis and cell division. The Aurora kinase family comprises 3 members, Aurora A, B and C, which have 67–76 % of their amino acid sequence in the catalytic domain in common [1]. AK are frequently found overexpressed in a variety of human tumors. In particular, Aurora kinase A is aberrantly expressed in renal, ovarian, and hepatic carcinoma, and many others. As Aurora family members have been shown to interact with crucial tumor suppressor proteins and oncogenic proteins, they are also considered an important target for antitumor therapy [2]. Their importance in cancer has led to many compounds being designed to inhibit AK. Among them, VX-680 (also called MK-0457) has been shown to block cell cycle progression and induce apoptosis in many tumors, fostering growth inhibition in in vivo xenograft models [3]. SNS314, another AK inhibitor (AKI), has also exhibited a promising reduction in cell growth and tumorigenicity in in vitro experiments. ZM447439 is a selective, ATP-competitive inhibitor of Aurora kinases A and B [3] that was recently assessed in a primary cell culture obtained from a pediatric adrenocortical carcinoma, producing interesting results [4]. Reversan is a small molecule that selectively and non-toxically targets P-glycoprotein (P-gp), a member of the superfamily of human ATP-binding cassette (ABC) proteins, which are fundamental efflux pumps in many tissues and have a protective role against xenobiotics [5]. P-gp is also implicated in multidrug resistance (MDR), a phenomenon that confers tumor cell resistance against a wide variety of anti-cancer drugs (such as vinca alkaloids, doxorubicin, etoposide) [6]. H295R and SW13 cells, and the majority of adrenocortical carcinomas (ACC) were recently found to express P-gp [7].
Virtually all types of tumor can develop metastases, which may spread to different tissues and organs via organ-specific colonization processes [8]. Metastases to the adrenal glands are rare, but may derive from various primary cancers, non-small-cell lung cancer (NSCLC) being considered the most likely [9]. The American Association of Endocrine Surgeons strongly recommends treating metastases as soon as possible with chemotherapy or surgical resection (adrenalectomy) to avoid exacerbating the patient’s condition and symptoms [10].
Primary adrenocortical tumors (ACT), on the other hand, can be roughly divided into aldosterone-producing adenomas (APA), non-aldosterone-secreting cortical adenomas (NACA), and adrenocortical carcinomas (ACC). ACC are rare malignancies with an estimated incidence of 0.7–2.0 cases per million population a year [11]. They carry a poor prognosis, with a 5-year survival rate of less than 35 %, and metastases are common [12]. Surgery remains the mainstay of treatment, while pharmacological therapy is mainly based on the adrenotoxic drug, mitotane (o,p’-DDD), despite its low response rate and significant toxicity [13] – hence the need to develop new treatment options.
This study analyzed the expression of Aurora kinases A, B and C in 70 adrenal samples, 2 cell lines (SW13 and H295R, the 2 most frequent cancer cell models considered in the setting of adrenocortical diseases), 3 cell cultures from primary adrenocortical metastases (from NSCLC), and 4 primary adrenocortical tumor cell cultures. Three different AKI were assessed and the origins of their cytostatic and cytotoxic effects on the cell models were investigated.
Materials and methods
Materials
VX-680, SNS314 mesylate, ZM447439, and mitotane were purchased from Selleckchem Europe. Fetal bovine serum (FBS), 3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyl tetrazolium bromide (MTT), trichloracetic acid (TCA), reversan and propidium iodide were purchased from Sigma Aldrich, Italy. DMEM-F12, 0.05 % trypsin-EDTA, insulin, transferrin, selenium and antibiotics were obtained from Life Technologies, Italy. The primary antibodies were: Akt (code 9272), phospho-Akt (Ser473) (code 9271), Erk1/2 (code 4695), phospho-Erk1/2 (Thr202/Tyr204) (code 4370), phospho-Aurora A (Thr288) (code 3079), phospho-Aurora A (Thr288) / phospho-Aurora B (Thr232) / phospho-Aurora C (Thr198) (code 2914), Aurora A (code 4718), Aurora B (code 3094), all from Cell Signaling Technology; caspase 3 (code 110,543) and 9 (code 112,888) from GeneTex; and anti-β-actin antibody (code A5441) from Sigma-Aldrich. The secondary antibodies were: horseradish peroxidase-labeled goat anti-mouse or anti-rabbit (Jackson ImmunoResearch).
Patients
Adrenocortical tissues were obtained from 23 patients with ACC, 26 with NACA, 17 with APA, and 9 individuals with normal adrenals (NA). The tissues were used for mRNA (RT-PCR) and DNA (PCR and sequencing) extraction. The etiology, clinical diagnosis and staging of each adrenocortical mass were established as explained elsewhere [14]. All clinical data are summarized in Table 1. All patients gave their written informed consent to the collection and use of their adrenal tissue for research purposes. The study was approved by the local ethics committee “Azienda Ospedaliera di Padova Prot. n.2989P/13”. It was conducted in accordance with the Declaration of Helsinki, and no children (under 18 years old) were involved in the study.
Cell cultures
The H295R and SW13 tumor cell lines were obtained from the American Type Culture Collection (ATCC, Rockville, MD). The H295R cells came from a female patient diagnosed with an adrenocortical carcinoma. This strain secretes mineralocorticoids, glucocorticoids and adrenal androgens. The SW13 cells came from a metastatic deposit in the adrenal cortex derived from a lung carcinoma in a 55-year-old female [15]. Seven primary cell cultures were also studied: 3 cell cultures from primary adrenocortical metastases (derived from NSCLC) and 1 ACC, 1 APA, 2 NACA cell cultures. All experiments involving cell manipulation were conducted after incubating the cell lines with 0.1 % FBS as previously reported [16].
MTT assay and drug combination strategy
SW13 and H295R cells were plated in 96-well plates at a density of 5x103 cells/well in supplemented medium, with or without drugs. VX-680 was used at 1, 10, 50, 100, 200, 500 nM for 24 h, 48 h and 72 h (and also 120 h and 144 h for the H295R cells). SNS314 was used at 1, 10, 100 nM for 24 h and 72 h. ZM447439 was used at 0.1, 1, 10 μM for 24 h and 72 h. Mitotane was used at 10 μM for 24 h and 72 h. Methods and cell survival percentages were as previously reported [16]. Each analysis was run in quadruplicate and repeated 3 times. The half maximal inhibitory concentration (IC50) was calculated in dose-response curves using CalcuSyn software (Biosoft, Ferguson, MO). MTT assay was also performed on 4 primary adrenocortical tumor (1 ACC, 1 APA, 2 NACA) and 3 metastatic cell cultures. The concentrations of VX-680 were 10 and 200 nM for 24 h.
Interaction between VX-680 and mitotane was analyzed using the combination index (CI) values calculated with the CompuSyn 3.0.1 analysis software. CI values were generated over a range of fraction-affected levels from 5 %–95 % of growth inhibition, relying on the dose-response curves by MTT assay, as previously described [17]. Antagonism is defined as CI > 1.15, synergism as CI < 0.85 and additivity when the values lie between 0.85 and 1.15. Reversan was dissolved in DMSO (10 mg/ml) at 60 °C according to the manufacturer’s instructions, and diluted to obtain a concentration of 1 mM.
[3H] thymidine assay
H295R and SW13 cells were seeded in 24-well plates and incubated with varying concentrations of VX-680 (10 and 200 nM) for 24 h and 72 h according to the method already described [18]. Experiments were performed in quadruplicate and repeated 3 times. [3H] thymidine assay was also performed on 2 primary adrenocortical tumor cell cultures (NACA-1 and APA). The concentrations of VX-680 used were 10 and 200 nM for 24 h; and the experiments were performed in triplicate.
Cell morphology assessment with Wright’s staining
H295R and SW13 cells were cultured on coverslips for 48 h, incubated overnight in 0.1 % FBS, and then treated with VX-680 at 200 nM, SNS314 at 100 nM, ZM447439 at 10 μM for 72 h and 144 h. Lower concentrations of the above-mentioned drugs were used too (data not shown). Then SW13 and H295R cells were treated as previously described [19]. Cell morphology was assessed by light microscopy at ×400 magnification. The experiments were repeated twice.
Cell cycle distribution and apoptosis analysis
For the cell cycle analysis, the H295R cells were incubated for 24 h, 72 h and 144 h, and the SW13 cells for 24 h and 72 h. Briefly, H295R and SW13 cells were plated at a density of 1x106 cells/well and treated with VX-680 (10 and 200 nM) as previously described [17].
Apoptosis was assessed with the Annexin V-FITC kit (BD Biosciences, San Diego, CA, USA) as previously described [17]. Briefly, the H295R and SW13 cells were plated at a density of 1x106 cells/well for two days, then treated with VX-680 (10 and 200 nM) for 24 h and 72 h (and also 144 h for the H295R cells). The experiments were performed in triplicate and data were assessed with the CXP analytical software.
Western blot analysis
The SW13 and H295R cells were treated with different concentrations of VX-680 (10 and 200 nM) for 72 h as previously described [20, 21]. Briefly, the proteins were extracted, loaded onto SDS/PAGE, electroblotted and incubated overnight with different primary antibodies. After adding secondary antibodies, immunoreactivity was detected with LiteAblot Extend Long-Lasting Chemiluminescent Substrate (EuroClone). Films were scanned and band intensity was quantified with ImageJ software 1.44p. The experiments were performed in triplicate.
Aurora kinases A, B and C mutation analysis and real-time PCR assay
AURKA and AURKB DNA were extracted from H295R and SW13 cells using genomic DNA isolation (QIAamp DNA micro Kit, Qiagen) according to the manufacturer’s protocol. DNA was amplified using appropriate primers for AURKA [22] and AURKB [23], then assessed by direct sequencing (bidirectionally), as described elsewhere [24]. No AURKC mutation analysis was performed because its role in the mitotic process needs to be unambiguously clarified [25].
The real-time PCR (RT-PCR) method was used as in a previous work [14]. Briefly, total RNA was extracted from H295R and SW13 cells and from 66 ACT and 9 NA samples with an RNeasy Mini Kit (SABioscience) according to the manufacturer’s protocol, and stored at −80 °C. The concentration and integrity of the RNA and cDNA synthesis were checked. AURKA, AURKB, AURKC and GAPDH primer sequences were obtained from previous works [22, 23, 26]. Data were obtained as Ct values according to the guidelines and used to determine ΔCt values (ΔCt = Ct of the target gene minus Ct of the housekeeping gene). The 2-ΔΔCt equation was used to calculate the fold changes in gene expression between two categories of samples (e.g. ACC vs NA).
Statistical analysis
Statistical analyses were performed using GraphPad Prism 5 software (GraphPad Software, Inc., San Diego, CA) and Microsoft Excel software. Cell line data were analyzed using a two-tailed paired Student’s t-test and RT-PCR data with the Kruskal-Wallis analysis and Dunn’s posttest. The Mann-Whitney test was used for band quantification. Survival analyses were done using a Kaplan-Meier survival plot and two-sided log-rank tests (using a two-fold increase in the median values of normal adrenal tissue gene expression as a cut-off). A p < 0.05 was considered statistically significant. Data are presented as medians and quartiles.
Results
AK inhibitors affect cell viability
MTT assay was performed to examine cell viability in SW13, H295R, primary and metastatic tumor cells. As shown in Fig. 1a, VX-680 induced a concentration- and time-dependent inhibition of mitochondrial activity in the SW13 cells with an IC50 of 84 ± 7 nM at 72 h. Treatment of the H295R cells indicated that no IC50 was reached (Fig. 1b). The data in Fig. 1c–d show that SNS314 and ZM447439 may reduce SW13 cell viability, especially at 72 h, whereas H295R cells do not respond to the drug treatments (Supplementary Fig. 1A-B). Among the primary adrenocortical tumor cell samples, only APA revealed a slight decrease in cell viability when VX-680 was used at 200 nM (Fig. 1e). In metastatic cell cultures, VX-680 induced a reduction in cell viability, particularly at 200 nM (Fig. 1f).

Cell viability of adrenocortical tumor cells on MTT assay. a and b: cell viability in SW13 and H295R cells after different times and concentrations treatments. c and d: cell viability in SW13 cells after 24 h and 72 h of treatment with ZM447439 and SNS314. E: 4 primary adrenocortical tumor cell lines (1 ACC, 1 APA and 2 NACA) treated with VX-680 for 24 h. F: 3 metastatic tumor cell lines (from lung cancer) treated with VX-680 for 24 h. Treatment vs control: * p < 0.05. Experiments performed in quadruplicate and repeated 3 times
The VX-680 + mitotane combination was applied to see if the selective pharmacological adrenocortical therapy (mitotane) could enhance the effect of the AKI. VX-680 + mitotane did not induce any marked reduction in cell viability (Supplementary Fig. 1C-D): the CI for VX-680 (200 nM) + mitotane (10 μM) in the SW13 cells at 72 h was 2.1 (the CI could not be calculated at 24 h and for the H295R cells because the IC50 could not be reached).
Reversan alone induced a reduction in mitochondrial activity in SW13 cells, particularly at 72 h and at higher concentrations, while no significant changes were seen in the H295R cells (Fig. 2a–b). A combination of reversan 5 μM with VX-680 (at 10 and 200 nM) induced a marked decrease in SW13 cell viability, especially at 72 h, while the H295R cells did not respond to this combination (Fig. 2c–d). Reversan 5 μM was used (in combination with VX-680) to resemble its possible administration in humans, while reversan alone reached an IC50 of 95 ± 7 μM at 48 h and 24 ± 6 μM at 72 h.

Cell viability of cell models on MTT assay. a and b: cell viability in SW13 and H295R cells after different times and concentrations of reversan treatment. C and D: cell viability in SW13 and H295R cells after 24, 48 and 72 h of treatment with VX-680 (indicated as V) and reversan (indicated as R). Treatment vs control: * p < 0.05. Experiments performed in triplicate and repeated 3 times
Proliferation rate modulated by VX-680
[3H] thymidine incorporation assays were performed to assess the SW13 and H295R cell proliferation rate. VX-680 reduced the proliferation of SW13 cells, especially at 72 h and 200 nM (Fig. 3a–b). No substantial differences were seen for the H295R cells (Supplementary Fig. 1E-F). Only 1 APA sample showed an evident reduction in proliferation rate at 200 nM (Fig. 3c).

Adrenocortical cell proliferation and morphological changes. a, b, c, d: Proliferation rate of adrenocortical cells treated with VX-680 and assessed by [3H] thymidine incorporation assay. The results are expressed as a percentage of control (100 %). (a and b: SW13 cells at 24 h and 72 h. c and d: NACA-1 and NACA-2 cells at 24 h. Treatment vs control: * p < 0.05; ** p < 0.01. Experiments performed in quadruplicate and repeated 3 times). E, F, G, H: SW13 cell morphology at 72 h and H295R at 144 h, assessed with Wright’s staining (E: SW13 control cells. F: SW13 cells treated with VX-680 at 200 nM. G: H295R control cells. H: H295R cells treated with VX-680 at 200 nM. Experiments performed twice)
Cell morphology changes after VX-680 treatment
Wright’s staining method emphasized sharp morphological changes in the SW13 cells. VX-680 enables the cells to enter mitosis, but prevents their complete cytokinesis. The cells consequently tend to remain aggregated, forming clusters. Our data showed that the SW13 cells treated with VX-680 at 200 nM were larger than the control and multinucleated (Fig. 3e–f). Similar results were obtained with higher concentrations of SNS314 and ZM447439 (data not shown). No appreciable changes occurred in the H295R cells (Fig. 3g–h).
Flow cytometry analysis after VX-680 treatment
Based on the role of AK in cell cycle progression, we examined the effect of VX-680 on SW13 and H295R cells. As expected, the drug induced a G2/M phase increase after treatment at 100, 200 and 500 nM in SW13 cells, and a concomitant G1 phase reduction (Fig. 4a). The same could not be said for H295R cells, in which no cell cycle modulation was detected even after prolonged treatment times (Fig. 4b).

Cell cycle distribution and protein alteration in SW13 and H295R cells. A and B: Representative cell cycle analysis for cell lines treated with VX-680 at different concentrations (a: SW13 cells at 72 h. b: H295R cells at 144 h. Experiments performed in triplicate). c: Representative Western blot at 72 h analyzed for AKA, p-AKA, AKB, p-AKA/AKB/AKC, Akt, p-Akt, Erk1/2, p-Erk1/2, β-actin; C, control (10 = treatment with VX-680 at 10 nM. 200 = treatment with VX-680 at 200 nM; experiments performed in triplicate)
To see whether AKI could lead to apoptosis, we analyzed the effect of VX-680 on the fate of apoptotic or necrotic cells. Annexin V-FITC flow cytometry analysis revealed no increase in the cell death process in either SW13 or H295R cell lines (Supplementary Fig. 2A–D).
AK are expressed in SW13 and H295R cells
Western blot analysis confirmed the presence of all antigens tested, and of AK in particular (Fig. 4c). Aurora kinase A was not modulated by the drug treatment, unlike Aurora kinase B and p- Aurora kinases A, B, C (Fig. 4c). Both cell lines showed a decrease in the signal for Aurora kinase B and p- Aurora kinase B (Supplementary Fig. 3A–D).
We also analyzed the MAPK and PI3K/Akt pathways in SW13 and H295R cells because there are reports in the literature of these pathways being modulated by AKI [27, 28]. No substantial change was seen using VX-680, however. Only p-Akt increased slightly in the SW13 cells after treating them with VX-680 at 10 and 200 nM (p < 0.05, Supplementary Fig. 3E). We analyzed an initiator caspase (CASP9) and an effector caspase (CASP3) too, but no clear reactivity modulation emerged in either of the cell lines (Fig. 4c).
Mutation analysis and gene expression profile
AURKA and AURKB gene mutation analysis revealed a similar pattern for the SW13 and H295R cells (Table 2), with one novel alteration (c.42 + 1_42 + 61dup).
Our RT-PCR data confirmed the presence of AURKA, AURKB, AURKC mRNA in both cell lines and in human tissues. AURKA and AURKB expression was significantly higher in ACC patients (p < 0.001) and NACA patients (p < 0.05) than in NA, while the difference for APA patients did not reach statistical significance, though there seemed to be the same trend (Fig. 5). No differences in expression were apparent between ACC, NACA and APA for either AURKA or AURKB (Fig. 5).

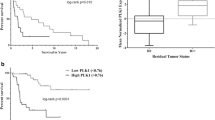
Aurora kinase A (AURKA) and Aurora kinase B (AURKB) expression in 66 ACT patients. The graph shows Y-value median-quartile boxplots with decile error bars. NA = normal adrenals, ACC = adrenocortical carcinomas, APA = aldosterone-producing adenomas, NACA = non-aldosterone-secreting cortical adenomas. * p < 0.05; *** p < 0.001
As expected, AURKA and AURKB expression was correlated in ACT patients too (p < 0.001), while no such association was found between AURKA and AURKC, or between AURKB and AURKC. Due to the small numbers involved in our sample, AURKC expression could not be considered as amplified in statistical terms, but a similar trend emerged for this set too (data not shown). H295R and SW13 cells expressed high levels of AURKA (2-ΔΔCt = 2.5 and 2.3, respectively) and AURKB (2-ΔΔCt = 16.5 and 15.4, respectively), but not of AURKC (2-ΔΔCt = 0.5 and 0.2, respectively). Kaplan-Meier survival curve analysis showed no statistical significant difference in ACC event-free survival as far as AURKA or AURKB gene expression were concerned, though a trend could be hypothesized (log-rank Mantel-Cox test p = 0.18, see Supplementary Fig. 4).
Discussion
Our work demonstrates the efficacy of AKI in adrenocortical tumor in vitro models, confirming the expression of Aurora kinases A, B and C in adult adrenocortical tumor tissues, and in SW13 and H295R cell lines, and showing that AKI are especially effective on primary adrenocortical metastases from NSCLC, and on SW13 cells. The latter are an interesting model of metastasis, the only one available for studying metastatic potential in the adrenal glands. It is worth emphasizing that chemotherapy regimens for treating adrenal metastases (that cannot be resected) could be another fundamental aim in the fight against cancer. A compound such as VX-680, which actively terminates the cells’ ability to duplicate may have a second-line role in the treatment of metastases and play an active part in a pharmacological cocktail [29]. VX-680 has never been tested in adrenocortical models. It was recently included in a phase 2 study on different subtypes of leukemia, which goes to show the progress made with AKI in clinical research [30]. Our study is the first in which adrenocortical tumor cells derived from adrenal metastases (of NSCLC) have been treated with VX-680, demonstrating its antiproliferative effect. In this regard, VX-680 could have potential as a drug with remarkable effects on metastases from NSCLC, though more samples and more research are naturally needed to support this impression.
MTT analysis emphasized the efficacy of the 3 AKI on SW13 cell viability at different times and in various concentrations, with a prevalent effect of VX-680 (Fig. 1a), which convinced us to focus our efforts on this compound. More specifically, VX-680 induced a concentration- and time-dependent inhibition of mitochondrial activity in SW13 cells, while H295R cells seemed to respond differently to AKI, giving the impression of a more cytostatic effect (Fig. 1b and Supplementary Fig. 1A-B). Among the primary adrenocortical tumor cell samples, only APA revealed a slight decrease in cell viability (Fig. 1e). In metastatic cells (Fig. 1f), the effects of VX-680 seemed intense and constant: we surmise that the compound might be very effective on actively proliferating cells (such as metastatic cells), which have a high capacity for replication [31].
Given the paucity of results in H295R cells, we tested the P-gp inhibitor reversan, partly because a recent work suggested P-gp activation in SW13 and H295R cells, and also because AKI could be a P-gp substrate [7]. The compound was not effective in reversing P-gp-mediated resistance, however, and it had no effect on cell proliferation up to a concentration of 100 μM in H295R cells and 72 h of incubation (Fig. 2b–d). There could be several reasons for the lack of reversan activity in H295R cells: a) P-gp gene (ABCB1) mutations; b) P-gp may be so overexpressed that higher amounts (>100 μM) are needed to inhibit its activity; c) other ABC superfamily genes may be involved in MDR; d) other MDR proteins may participate in H295R cell resistance; or e) VX-680 might not be recognized as a substrate by ABCB1, even though this had already been demonstrated elsewhere [32]. Nonetheless, we can exclude AURKA and AURKB alterations as potential sources of H295R cell resistance, but more efforts are needed to clarify this complex picture. In SW13 cells, on the other hand, we saw a substantial effect of reversan, alone or in combination with VX-680 (Fig. 2a–c). In particular, using VX-680 at 200 nM and reversan at 5 μM may have an additive effect, as demonstrated by MTT assay (Fig. 2c).
[3H] thymidine assay generated similar cell proliferation results to MTT analysis, again showing a different behavior of the 2 cell lines (Fig. 3a-b and Supplementary Fig. 1E-F). We undertook a cell morphology analysis in an effort to clarify the effects of AKI in SW13 and H295R cells. We found that SW13 cells treated with VX-680 were aberrantly large, with multiple nuclei, while H295R cells were not (Fig. 3e–h). This may be attributable partly to drug effects (which prevent the completion of cytokinesis), and partly to a different genetic background. In fact, H295R cells carry diverse mutations, such as p.S45P in CTNNB1 and a homozygous deletion of exons 8–9 of TP53, whereas SW13 cells carry no mutations in CTNNB1 and a homozygous point mutation in exon 6 of TP53. A novel alteration was identified as well, i.e. 42 + 1_42 + 61dup (homozygous in SW13 cells and heterozygous in H295R cells) in the 5′-UTR region of the AURKA gene. Other known homozygous polymorphisms were found (Table 2) that might contribute to cell diversity [22, 30]. The meaning of these alterations remains unknown.
One of the main effects of AKI is to generate polyploid cells as a result of multiple rounds of DNA synthesis in the absence of cytokinesis [33]. Cell cycle analysis revealed that the G2/M phase increased in SW13 cells, especially at higher VX-680 concentrations. This finding suggests the presence of endoreduplication, a hallmark of Aurora kinase B inhibition [34, 35], as seen on cell morphology analysis (Fig. 2e-f), and Western blot quantification (Fig. 4c and Supplementary Fig. 4A-D). G2/M arrest may lead to cell death, and an increase in the subG1 cell population in SW13 cells was clearly evident, which might be related to necrosis and apoptosis (Fig. 4a). Flow cytometry analysis with Annexin V-FITC was performed to distinguish between these two different cell fates. This method revealed no substantial changes in either cell line (Supplementary Fig. 2A-B), as confirmed by Western blot, and caspase 3 and 9 were not modulated by VX-680 treatments either (Fig. 4c). We consequently surmise that the cell death observed in SW13 cells on cell cycle analysis (subG1 increased at high drug concentrations) is more likely to be attributable to necrotic processes (toxic effects) than to apoptosis [36]. H295R cells seemed to behave differently: no endoreduplication or polyploid cells emerged on morphological (Fig. 3g-h) or cell cycle analysis (Fig. 4b). This may be because H295R cells are associated with a specific genetic background or already occasionally multinucleated (with the consequences that this implies) [15]. Alternatively, it could be that the integrity of the p53-p21Waf1/Cip1 pathway in the G1 postmitotic checkpoint, which seems to govern response to VX-680, may already be impaired [37]. More data are needed to elucidate these results.
Western blot analysis showed that VX-680 inhibited AK expression, particular affecting Aurora kinase B – in fact, the drug is known to have a predilection for targeting Aurora kinase B (Fig. 4c) [35]. This result may be associated with the stronger Aurora kinase B expression emerging from qRT-PCR (Fig. 5), and the more Aurora kinase B is expressed, the more it is inhibited by VX-680. As expected, p-Aurora kinase A, B and C were found decreased, suggesting that VX-680 could take effect on appropriate biochemical targets. In addition, p-Akt was increased in SW13 cells treated with VX-680 at 200 nM, while total Akt expression was normal (Fig. 4c). This finding was unexpected, and no clear link seemed to exist between Akt phosphorylation and AK inhibition. Only one previous work supported this result, and the authors suggested that Aurora kinase A might activate Akt and induce chemoresistance in ovarian cancer cells [38]. Akt activation might be understood in the light of the fact that a blockade on other main signaling pathways (induced by AKI) could reverberate on the Akt pathway, inducing a slight Akt activation. We also analyzed the MAPK and PI3K/Akt pathways in SW13 and H295R cells because other publications have demonstrated a modulation of these pathways by AKI [27], but no substantial changes came to light using VX-680.
In addition to our Western blot results, qRT-PCR demonstrated AURKA, AURKB, AURKC expression in ACT samples and in 2 cell lines. As expected, AURKA and AURKB were found overexpressed in ACC and NACA, as happens in other cancer types. These results demonstrate that AK are present in high concentrations in adrenocortical tumors, suggesting an important role for AK in adrenocortical tumorigenesis (even though AK inhibition seemed to have no beneficial effect in a H295R cell model). AURKA and AURKB overexpression in ACC patients might be related to a worse event-free survival (Supplementary Fig. 4), but it is hard to deduce a trend so it is only by studying a large sample of patients that this hypothesis might be confirmed or rejected.
In conclusion, our novel contribution to clarifying the biomolecular features of ACT may pave the way to AKI being used to treat metastatic processes involving adrenal tissue. In particular, VX-680 could be a novel compound for use in association with others in chemotherapies for metastases from NSCLC, or as a second-line clinical approach to metastatic ACC, because this drug acts specifically on the SW13 cell model and metastatic cells. We also demonstrated that the P-gp inhibitor reversan and AKI Vx-680 are of no use in the H295R cell model, and therefore should not be considered when planning primary ACC treatments. Our research on the anti-metastatic potential of AKI is ongoing to extend our human biological series, also to other tumor types.
Abbreviations
- AK:
-
Aurora kinase
- AKI:
-
Aurora kinase inhibitors
- ACT:
-
Adrenocortical tumors
- ACC:
-
adrenocortical carcinomas
- NACA:
-
non-aldosterone-secreting cortical adenomas
- APA:
-
aldosterone-producing adenomas
- NSCLC:
-
non-small-cell lung cancer
- AURK :
-
AK gene
References
Carmena M, Earnshaw WC (2003) The cellular geography of aurora kinases. Nat Rev Mol Cell Biol 4:842–854
Gautschi O, Heighway J, Mack PC, Purnell PR, Lara PN Jr, Gandara DR (2008) Aurora kinases as anticancer drug targets. Clin Cancer Res 14:1639–1648
Fu J, Bian M, Jiang Q, Zhang C (2007) Roles of aurora kinases in mitosis and tumorigenesis. Mol Cancer Res 5:1–10
Borges KS, Moreno DA, Martinelli CE Jr, Antonini SR, de Castro M, Tucci S Jr, Neder L, Ramalho LN, Seidinger AL, Cardinalli I, Mastellaro MJ, Yunes JA, Brandalise SR, Tone LG, Scrideli CA (2013) Spindle assembly checkpoint gene expression in childhood adrenocortical tumors (ACT): overexpression of aurora kinases a and B is associated with a poor prognosis. Pediatr Blood Cancer 60:1809–1816
Obreque-Balboa JE, Sun Q, Bernhardt G, Konig B, Buschauer A (2016) Flavonoid derivatives as selective ABCC1 modulators: synthesis and functional characterization. Eur J Med Chem 109:124–133
Kathawala RJ, Gupta P, Ashby CR Jr, Chen ZS (2015) The modulation of ABC transporter-mediated multidrug resistance in cancer: a review of the past decade. Drug Resist Updat 18:1–17
Gagliano T, Gentilin E, Benfini K, Di Pasquale C, Tassinari M, Falletta S, Feo C, Tagliati F, Uberti ED, Zatelli MC (2014) Mitotane enhances doxorubicin cytotoxic activity by inhibiting P-gp in human adrenocortical carcinoma cells. Endocrine 47:943–951
Nguyen DX, Bos PD, Massague J (2009) Metastasis: from dissemination to organ-specific colonization. Nat Rev Cancer 9:274–284
Moreno P, de la Quintana BA, Musholt TJ, Paunovic I, Puccini M, Vidal O, Ortega J, Kraimps JL, Bollo Arocena E, Rodriguez JM, Gonzalez Lopez O, Del Pozo CD, Iacobone M, Veloso E, Del Pino JM, Garcia Sanz I, Scott-Coombes D, Villar-Del-Moral J, Rodriguez JI, Vazquez Echarri J, Gonzalez Sanchez C, Gutierrez Rodriguez MT, EscoreSsca I, Nuno Vazquez-Garza J, Tobalina Aguirrezabal E, Martin J, Candel Arenas MF, Lorenz K, Martos JM, Ramia JM (2013) Adrenalectomy for solid tumor metastases: results of a multicenter European study. Surgery 154:1215–1222 discussion 1222-1213
Libe R (2015) Adrenocortical carcinoma (ACC): diagnosis, prognosis, and treatment. Front Cell Dev Biol 3:45
Dy BM, Wise KB, Richards ML, Young WF Jr, Grant CS, Bible KC, Rosedahl J, Harmsen WS, Farley DR, Thompson GB (2013) Operative intervention for recurrent adrenocortical cancer. Surgery 154:1292–1299 discussion 1299
Gaujoux S, Brennan MF (2012) Recommendation for standardized surgical management of primary adrenocortical carcinoma. Surgery 152:123–132
Mariniello B, Rosato A, Zuccolotto G, Rubin B, Cicala MV, Finco I, Iacobone M, Frigo AC, Fassina A, Pezzani R, Mantero F (2012) Combination of sorafenib and everolimus impacts therapeutically on adrenocortical tumor models. Endocr Relat Cancer 19:527–539
Wang T, Rainey WE (2012) Human adrenocortical carcinoma cell lines. Mol Cell Endocrinol 351:58–65
Bertazza L, Barollo S, Radu CM, Cavedon E, Simioni P, Faggian D, Plebani M, Pelizzo MR, Rubin B, Boscaro M, Pezzani R, Mian C (2015) Synergistic antitumour activity of RAF265 and ZSTK474 on human TT medullary thyroid cancer cells. J Cell Mol Med 19:2244–2252
Barollo S, Bertazza L, Baldini E, Ulisse S, Cavedon E, Boscaro M, Pezzani R, Mian C (2014) The combination of RAF265, SB590885, ZSTK474 on thyroid cancer cell lines deeply impact on proliferation and MAPK and PI3K/Akt signaling pathways. Investig New Drugs 32:626–635
Pezzani R, Rubin B, Redaelli M, Radu C, Barollo S, Cicala MV, Salva M, Mian C, Mucignat-Caretta C, Simioni P, Iacobone M, Mantero F (2014) The antiproliferative effects of ouabain and everolimus on adrenocortical tumor cells. Endocr J 61:41–53
Redaelli M, Mucignat-Caretta C, Isse AA, Gennaro A, Pezzani R, Pasquale R, Pavan V, Crisma M, Ribaudo G, Zagotto G (2015) New naphthoquinone derivatives against glioma cells. Eur J Med Chem 96:458–466
Barollo S, Pezzani R, Cristiani A, Redaelli M, Zambonin L, Rubin B, Bertazza L, Zane M, Mucignat-Caretta C, Bulfone A, Pennelli G, Casal Ide E, Pelizzo MR, Mantero F, Moro S, Mian C (2014) Prevalence, tumorigenic role, and biochemical implications of rare BRAF alterations. Thyroid 24:809–819
Rubin B, Monticelli H, Redaelli M, Mucignat C, Barollo S, Bertazza L, Mian C, Betterle C, Iacobone M, Fassina A, Boscaro M, Pezzani R, Mantero F (2015) Mitogen-activated protein kinase pathway: genetic analysis of 95 adrenocortical tumors. Cancer Investig 33:526–531
Hienonen T, Salovaara R, Mecklin JP, Jarvinen H, Karhu A, Aaltonen LA (2006) Preferential amplification of AURKA 91 a (Ile31) in familial colorectal cancers. Int J Cancer 118:505–508
Failes TW, Mitic G, Abdel-Halim H, Po’uha ST, Liu M, Hibbs DE, Kavallaris M (2012) Evolution of resistance to aurora kinase B inhibitors in leukaemia cells. PLoS One 7:e30734
Barollo S, Pezzani R, Cristiani A, Bertazza L, Rubin B, Bulfone A, Pelizzo MR, Torresan F, Mantero F, Pennelli G, Moro S, Mian C (2013) Functional significance of the novel H-RAS gene mutation M72I in a patient with medullary thyroid cancer. Exp Clin Endocrinol Diabetes 121:546–550
Quartuccio SM, Schindler K (2015) Functions of aurora kinase C in meiosis and cancer. Front Cell Dev Biol 3:50
Zekri A, Lesan V, Ghaffari SH, Tabrizi MH, Modarressi MH (2012) Gene amplification and overexpression of aurora-C in breast and prostate cancer cell lines. Oncol Res 20:241–250
Wan XB, Long ZJ, Yan M, Xu J, Xia LP, Liu L, Zhao Y, Huang XF, Wang XR, Zhu XF, Hong MH, Liu Q (2008) Inhibition of aurora-a suppresses epithelial-mesenchymal transition and invasion by downregulating MAPK in nasopharyngeal carcinoma cells. Carcinogenesis 29:1930–1937
Huang XF, Luo SK, Xu J, Li J, Xu DR, Wang LH, Yan M, Wang XR, Wan XB, Zheng FM, Zeng YX, Liu Q (2008) Aurora kinase inhibitory VX-680 increases Bax/Bcl-2 ratio and induces apoptosis in aurora-A-high acute myeloid leukemia. Blood 111:2854–2865
Leong L, Madame Curie Bioscience Database, Landes Bioscience, Austin (TX)
Seymour JF, Kim DW, Rubin E, Haregewoin A, Clark J, Watson P, Hughes T, Dufva I, Jimenez JL, Mahon FX, Rousselot P, Cortes J, Martinelli G, Papayannidis C, Nagler A, Giles FJ (2014) A phase 2 study of MK-0457 in patients with BCR-ABL T315I mutant chronic myelogenous leukemia and Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood Cancer J 4:e238
Wagnerova H, Lazurova I, Felsoci M (2013) Adrenal metastases. Bratisl Lek Listy 114:237–240
Tavanti E, Sero V, Vella S, Fanelli M, Michelacci F, Landuzzi L, Magagnoli G, Versteeg R, Picci P, Hattinger CM, Serra M (2013) Preclinical validation of aurora kinase-targeting drugs in osteosarcoma. Br J Cancer 109:2607–2618
Baldini E, Arlot-Bonnemains Y, Sorrenti S, Mian C, Pelizzo MR, De Antoni E, Palermo S, Morrone S, Barollo S, Nesca A, Moretti CG, D’Armiento M, Ulisse S (2011) Aurora kinases are expressed in medullary thyroid carcinoma (MTC) and their inhibition suppresses in vitro growth and tumorigenicity of the MTC-derived cell line TT. BMC Cancer 11:411
Nair JS, Ho AL, Tse AN, Coward J, Cheema H, Ambrosini G, Keen N, Schwartz GK (2009) Aurora B kinase regulates the postmitotic endoreduplication checkpoint via phosphorylation of the retinoblastoma protein at serine 780. Mol Biol Cell 20:2218–2228
Keen N, Taylor S (2004) Aurora-kinase inhibitors as anticancer agents. Nat Rev Cancer 4:927–936
Samadi A, Loo P, Mukerji R, O’Donnell G, Tong X, Timmermann BN, Cohen MS (2009) A novel HSP90 modulator with selective activity against thyroid cancers in vitro. Surgery 146:1196–1207
Gizatullin F, Yao Y, Kung V, Harding MW, Loda M, Shapiro GI (2006) The aurora kinase inhibitor VX-680 induces endoreduplication and apoptosis preferentially in cells with compromised p53-dependent postmitotic checkpoint function. Cancer Res 66:7668–7677
Yang H, He L, Kruk P, Nicosia SV, Cheng JQ (2006) Aurora-a induces cell survival and chemoresistance by activation of Akt through a p53-dependent manner in ovarian cancer cells. Int J Cancer 119:2304–2312
Acknowledgments
We thank Dr. Frances Coburn and Jillian Walton for text editing. This work was partially supported by the ENS@T-CANCER (European Network for the Study of Adrenal Tumors - grant agreement no. 259735), and the Associazione Italiana per la Ricerca Oncologica di Base (AIROB, Padova, Italy). All authors have read the journal’s authorship agreement and the manuscript has been read and approved by all named authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
All authors have read the journal’s policy on conflicts of interest and have none to disclose.
Electronic supplementary material
ESM 1
Supplementary Fig. 1 Cell viability and cell proliferation analyzed by MTT and [3H] thymidine assay. A and B, cell viability in H295R cells at different times and concentrations for ZM447439 and SNS314. Experiments were performed in triplicate. C and D, cell viability in SW13 and H295R cells at 24 h and 72 h treated with mitotane alone or the combination of mitotane + VX-680: V1 = 10 μM(mitotane) + 200 nM(VX-680), V2 = 10 μM(mitotane) + 10 nM(VX-680). E and F, [3H] thymidine incorporation for H295R cells at 24 h and 72 h treated with VX-680. Experiments were performed in triplicate. The standard deviation bars are present for each point-analysis, but they are not easily perceived due to small values. (GIF 75 kb)
ESM 2
Supplementary Fig. 2 Representative histograms of SW13 and H295R cells at 24 h and 72 h by flow cytometric analysis with Annexin V-FITC and propidium iodide. A and B, SW13 cells. C and D, H295R cells. Experiments were performed in triplicate. (GIF 69 kb)
ESM 3
Supplementary Fig. 3 Western blot analysis of SW13 and H295R cells treated and untreated with VX-680. Histograms represent band quantification by ImageJ analysis, normalized to control (arbitrary units). A and B, band quantification of AKB and p-AKB for H295R cells. C, D, E, band quantification of AKB, p-AKB, p-Akt for SW13 cells. * p < 0.05. Experiments were performed in triplicate. (GIF 48 kb)
ESM 4
Supplementary Fig. 4 Kaplan-Meier survival curves of AURKA or AURKB gene expression in ACC patients (n = 23). Comparison between ACC patients not overexpressing AK genes and ACC patients overexpressing AURKA or AURKB. Log-rank Mantel-Cox Test p = 0.18. (GIF 16 kb)
Rights and permissions
About this article

Cite this article
Pezzani, R., Rubin, B., Bertazza, L. et al. The aurora kinase inhibitor VX-680 shows anti-cancer effects in primary metastatic cells and the SW13 cell line. Invest New Drugs 34, 531–540 (2016). https://doi.org/10.1007/s10637-016-0358-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-016-0358-3