
Abstract
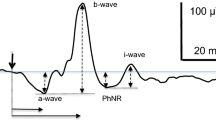
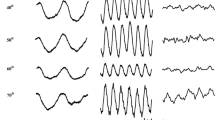
Our purpose was to explore S-cone ERG protocols for a commercial full-field hand-held stimulator that contains colored LEDs, and to see whether the test would be useful as a part of routine ERG testing. S-cone responses were elicited by blue flashes over a longer-wavelength background. With the standard stimulator containing blue (461 nm), green (513 nm) and red (652 nm) LEDs, we were unable to obtain satisfactory responses. Reproducible S-cone ERGs were obtained with a stimulator that had been custom-fitted with shorter-wavelength blue (440 nm) LEDs for stimulation, and orange (590 nm) LEDs for background adaptation. S-cone responses took only a few minutes to record, and the typical waveform showed a slow peak at 45–50 ms with amplitude 3–9 μV, but ranging from 0 μV to more than 10 μV. Larger waves appeared in a patient with enhanced S-cone syndrome. S-cone responses could also be obtained with an alternating blue-orange flicker protocol. We added the S-cone response to our regular ERG protocol for a number of months. Although most normal subjects and patients showed recognizable S-cone responses with this stimulator, the amplitudes were small and there was too much variability to make the technique effective for routine clinical testing. In general, the S-cone responses followed the standard cone ERG responses in disease.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Greenstein VC, Hood DC, Ritch R, Steinberger D, Carr RE. S (blue)cone pathway vulnerability in retinitis pig-mentosa, diabetes and glaucoma. Invest Ophthalmol Vis Sci 1989; 30: 1732–1737.
Simonsen SE, Rosenberg T. Reappraisal of a short-wavelength-sensitive (S-cone)recording technique in rou-tine clinical electroretinography. Doc Ophthalmol 1996; 91: 323–332.
Gouras P, Eggers HM, MacKay CJ. Cone dystrophy, nyctalopia, and supernormal rod responses. Arch Oph-thalmol 1983; 101: 718–724.
Sawusch M, Pokorny J, Smith VC. Clinical Electroreti-nography for short wavelength sensitive cones. Invest Ophthalmol Vis Sci 1987; 28: 966–974.
Gouras P, MacKay J. Electroretinographic responses of the short-wavelength-sensitive cones. Invest Ophthalmol Vis Sci 1990; 31: 1203–1209.
Swanson WH, Birch DG, Anderson JL. S-cone function in patients with retinitis pigmentosa. Invest Ophthalmol Vis Sci 1993; 33: 3045–3055.
Gouras P, MacKay CJ, Yamamoto S. The human S-cone electroretinogram and its variation among subjects with and without L and M-cone function. Invest Oph-thalmol Vis Sci 1993; 34: 2437–2442.
Horiguchi M, Miyake Y, Kondo M, Suzuki S, Tanikawa A, Mo Koo H. Blue light-emitting diode built-in contact lens electrode can record human S-cone electroretino-gram. Invest Ophthalmol Vis Sci 1995; 36: 1730–1732.
Arden G, Wolf J, Berninger T, Hogg CR, Tzekov R, Holder GE. S-cone ERGs elicited by a simple technique in normals and in tritanopes. Vis Res 1999; 39: 641–650.
Kuniyoshi K, Uno N, Irifune M, Shimomura Y. Electro-retinography of short-wavelength-sensitive cones with a LED built-in electrode and its normal values. Doc Oph-Thalmol 2003; 106(3): 311–318.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Marmor, M.F., Cabael, L., Shukla, S. et al. Clinical S-cone ERG recording with a commercial hand-held full-field stimulator. Doc Ophthalmol 109, 101–107 (2004). https://doi.org/10.1007/s10633-004-3299-7
Issue Date:
DOI: https://doi.org/10.1007/s10633-004-3299-7