
Abstract
With the increasing incidence of hepatocellular carcinoma (HCC) and its high mortality rates, effective treatment options are of urgent need, preferably in a multidisciplinary setting. In the management of those patients, interventional radiologists play a key role. In this article, we reviewed the current literature for regional, intraarterial treatment strategies of advanced-stage HCC including conventional transarterial chemoembolization, transarterial embolization, transarterial embolization with drug-eluting beads, and selective internal radiation therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.

Thomas J. Vogl

Tatjana Gruber-Rouh
Key Messages
-
Intraarterial therapies in patients with intermediate-stage hepatocellular carcinoma (HCC) show improved treatment response and disease control with acceptable safety profiles.
-
Conventional transarterial chemoembolization (cTACE), bland transarterial embolization (TAE), transarterial embolization with drug-eluting beads (DEB-TACE), and selective internal radiation therapy (SIRT) are interventional intraarterial therapy options in HCC treatment.
-
Patients with HCC should be treated in hospitals with multidisciplinary team with expertise in liver tumors.
Introduction
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related death worldwide due to its complexity of tumor pathogenesis, disease reccurrence after curative treatment, and metastases [1]. The major risk factor for HCC is liver cirrhosis, usually related to chronic hepatitis B (HBV) or C virus (HCV) infection, or overconsumption of alcohol [2]. Obesity, metabolic syndrome, nonalcoholic steatohepatitis (NASH), and hemochromatosis are also significant risk factors [3,4,5,6].
Patients with HCC have a poor prognosis. At the time of first diagnosis, many patients have already an advanced stage of disease that precludes curative options such as liver transplantation, surgical excision, and percutaneous ablation methods including radiofrequency ablation and microwave ablation [7].
Recently developed and improved interventional treatment techniques lead to an increasing importance of interventional radiologists in the management of patients with advanced-stage HCC. In advanced-stage HCC, multiple locoregional intraarterial treatment options have been established to slow down disease progression. Those treatment options may improve the outcome of potentially curative therapies of HCC in Barcelona Clinic Liver Cancer (BCLC) A stage as well as a bridging treatment before tumor resection or ablation therapies [7,8,9].
For each individual patient, the optimum interventional, liver-directed intraarterial treatment option needs to be carefully selected. Treatment options include bland transarterial embolization (TAE), conventional transarterial chemoembolization (cTACE), TACE with chemotherapeutically loaded beads (DEB-TACE), or selective internal radiation therapy (SIRT) [7,8,9,10,11,12]. This article provides an overview of intraarterial therapies in the treatment of HCC based on a review of the current literature.
Conventional Transarterial Chemoembolization (cTACE)
Conventional transarterial chemoembolization (cTACE) is one of the leading treatment options for HCC with nearly half of all HCC patients undergoing this procedure at some point during their clinical history [13, 14].
In accordance with the BCLC guidelines, cTACE is currently the standard of care for patients with HCC in the intermediate stage (BCLC stage B) [15,16,17]. In patients eligible for curative treatment (BCLC stage A), cTACE can be performed as bridging treatment option.
TACE is also a locoregional catheter-based intraarterial therapy for the treatment of HCC and liver metastases from different primaries including colorectal cancer (CRC), breast cancer (BC), and neuroendocrine tumors (NET) [18,19,20,21,22,23,24].
Transarterial chemoembolization (TACE) is based on the effect of simultaneous application of chemotherapeutic drugs and embolic agents such as degradable starch microspheres (DSM), collagen and gelatine sponge (Gelofam), polyvinyl alcohol, or lipiodol. All embolic agents have in common that they increase the time range of the chemotherapeutic effect on tumor lesions. Commonly used chemotherapeutic agents are doxorubicin, epirubicin, mitomycin, cisplatin, and miriplanin. A previous study has shown that HCC cells are highly sensitive to various chemotherapy drugs: irinotecan in 44% of HCC patients, gemcitabine in 36%, mitomycin in 14%, cisplatin in 8%, and 5-fluorouracil oxalate (5-FU) in 4% [25]. While doxorubicin, mitomycin, and cisplatin are commonly used in the USA and Europe, doxorubicin is the most commonly used chemotherapeutic agent in Asia [26]. The selection of chemotherapeutic agents, embolic agents and application method vary from center to center. A further standardization of TACE protocols is needed.
From the technical perspective, chemoembolization should be as selective as possible. Selective or superselective administration of the mixture of chemotherapeutic agent and occluding particles results in a high local concentration of the chemotherapeutic agent within the tumor with low systemic distribution. Due to the occlusion of the vessel by the embolic particles, the chemotherapeutic agent remains in the tumor, and the resulting hypoxia further improves the effect of the chemotherapeutic agent. Most commonly, a mixture of chemotherapeutic and embolic agents is injected first, followed by the injection of embolizing particles until stagnation of blood flow in the tumor branch is observed [27].
Lipiodol as the most commonly used embolic agent in cTACE has an average pharmacological half-life time of 4–12 weeks, while DSM have an average pharmacological half-life time of 90–120 min. The total embolization time of DSM leads to only moderately increased VEGF levels after the embolization compared to cTACE and most likely to less neoangiogenesis [28].
Prerequisite for successful TACE is the presence of a hypervascularized tumor. cTACE is either performed as “on demand” (repeated in case of persistent vascularization) or as “continuous” (repeated every 4–6 weeks until devascularization) schedule.
TACE Procedure
After disinfection, sterile covering of the access point (inguinal region), and local anesthesia, a 5F-sheath is inserted into the femoral common artery using the Seldinger technique. After that, a 5F pigtail catheter is used for the aortography to gain an exploratory view of the abdominal arteries including the celiac trunk and the superior mesenteric artery. In a next step, selective catheterization of the celiac trunk using a 5F sidewinder catheter is performed. The angiography depicts the anatomy of the hepatic artery, tumor blush, feeding arteries, and arteriovenous shunts. In addition to the pre-interventional, contrast-enhanced CT or MRI, an indirect portography should be performed during angiography to ensure a stable flow in the portal vein. During the initial TACE, cone beam CT can be performed to evaluate the tumor-feeding artery and detection of small HCC lesions. A 2.8F coaxial microcatheter system is inserted through the celiac trunk and past the branches of the gastroduodenal artery. The microcatheter for the injection of chemotherapeutic drugs and embolic agents should be placed selectively or superselectively in the segment arteries which feed HCC lesions. After confirming the correct position of the catheter tip, the chemotherapeutic and embolic agents are infused under radiographic guidance. To control the correct administration of drugs and the occlusion of tumor vessels with flow stasis, a final angiography should be performed. After completing the procedure, the punctured location of the femoral artery must be occluded by using a percutaneous closure device or compression bandage.
After the interventional treatment, patients should be transferred to an interventional ward for subsequent clinical observation. Patients can be discharged on the day of the procedure if no complications occur.
Most patients are either treated as outpatients or stay one night at the hospital; prolonged hospital stay is necessary in case of complications.
Before discharge, patients should be informed about possible post-embolization side effects. Post-embolization syndrome is one of the most common side effects of chemoembolization and includes abdominal pain, slight elevation of temperature, nausea, vomiting, and sometimes fatigue. Intravenous analgesics during and oral analgesics after the procedure provide sufficient pain control. The incidence of major complications after TACE has been reported with 5.6% including necrosis of liver parenchyma, decompensation of liver cirrhosis and abscess, and mortality rates of 0–10% [29].
Benefits and risk of treatment-induced liver failure need to be carefully balanced before TACE. Contraindications of TACE are Child–Pugh class C, uncorrectable coagulopathie, total portal vein thrombosis, poor residual liver function, total bilirubin > 3 mg/dL, extrahepatic metastases, or the presence of high-flow arterioportal or arteriovenous shunts.
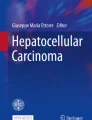
TACE treatment usually requires multiple procedures in intervals of 4–6 weeks. MRI and CT are performed to evaluate results of the chemoembolization (Fig. 1).

A 78-year-old female patient with recurrent HCC after first curative atypical resection of HCC in liver segments 7 and 8. Partial response achieved after three sessions of TACE. a Pre-treatment transverse contrast-enhanced T1-weighted MR image shows a 3.6 × 3.9 cm HCC lesion (arrow) in liver segment 4a. b Post-embolization DSA image shows the presence of lipiodol deposition in HCC lesion (arrow). A microcatheter was inserted in the right liver artery. c CT after 3. TACE. Documentation of lipiodol deposition in HCC lesions in liver segment 4 (arrow). d Post-treatment transverse contrast-enhanced T1-weighted MR image after three sessions of TACE shows partial response with devascularization and necrosis of intrahepatic lesion (arrow)
In conclusion, TACE is a moderately invasive, intraarterial method for the treatment of HCC. Treatment of intermediate-stage HCC aims at a palliative treatment rather than curative. cTACE in patients with BCLC stage B has level I evidence [15, 30,31,32,33].
In a meta-analysis including 545 patients, Llovet et al. showed a survival benefit for patients with TACE compared with the best supportive care in well-selected cases. TACE improved the 2-year survival rate with an odds ratio of 0.53 (p < 0.017) in comparison with an untreated control group. TACE has been reported to achieve partial response in 15–62% of HCC patients. Patients in TACE group had a median survival of 16–20 months [30]. A summary of the previous studies is shown in Table 1.
Transarterial Embolization (TAE)
Bland transarterial embolization (TAE) aims at achieving total arterial occlusion of the tumor vessels in the absence of chemotherapeutic agents. The result of TAE is tumor necrosis [34]. Favorable embolic agents used for tumor vessel occlusion are lipiodol and polyvinyl alcohol particles. Technical methods of TAE are similar to those for conventional chemoembolization.
In combination with ablation therapy, TAE achieves survival rates similar to surgical resection [35]. In addition to the treatment effect of TAE, HCC lesions are well visualized by lipiodol for ablation therapy planning.
TACE with Chemotherapeutically Loaded Beads (DEB-TACE)
In recent years, chemotherapeutically loaded beads (DEB) have been introduced in the clinical practice, including doxorubicin-loaded beads for treatment of HCC. DEB-TACE is defined as the infusion of microspheres which are loaded with chemotherapeutic agents to achieve sustained, in vivo drug release. Indications for DEB-TACE are similar to those for cTACE.
Chemotherapeutically loaded beads are produced from biocompatible polyvinyl alcohol (PVA) hydrogel that has been modified with sulfonate groups for the controlled loading and delivery of chemotherapeutic drugs. The beads are available in different sizes (100–300 μm until 500–700 μm) and can be loaded with doxorubicin or irinotecan. The advantage of DEB-TACE in comparison with cTACE is the favorable pharmacokinetic profile. The use of chemotherapeutically loaded beads results in a lower peak plasma concentration of the chemotherapeutic agents and longer exposure to the tumor compared to other therapeutic agents. Chemoembolization using DEBs results in significantly fewer drug-related side effects compared with cTACE [36, 37]. Doxorubicin is gradually sequestered inside the tumor as the drug dissociates from the beads only under specific ionic circumstances such as those found in tumor cells [36,37,38,39].
A randomized phase II study which compared DEB-TACE and cTACE showed that DEB-TACE was associated with a significant reduction in liver toxicity and drug-related adverse effects. Patients with Child–Pugh B, recurrence of HCC, or bilobar HCC disease had a significant increase in objective response [40].
Several trials studying the effect of DEB-TACE with doxorubicin have been performed in patients with HCC and are summarized in Table 1. Overall, these studies reported that DEB-TACE proved to be effective in patients with advanced-stage disease with improved treatment response and disease control while safety profile was described as acceptable. These results may provide a niche for those patients with poor conditions such as patients with Child–Pugh B and ECOG 1 disease.
In comparison with DEBs with smaller diameters, DEBs with larger diameters induced limited necrosis because occlusion of proximal vessel. DEBs with smaller diameters can be delivered to distal vessels where they obstruct collateral channels [38, 39, 41].
Han et al. [42] performed a meta-analysis comparing DEB-TACE and cTACE with 217 and 237 patients, respectively. The results showed that DEB-TACE tends to have better results for disease control, although differences were not significant.
Selective Internal Radiation Therapy (SIRT)
Another treatment option for HCC in BCLC stage B is 90Y radioembolization, which delivers high-dose ß-emitting radiolabeled microspheres through a microcatheter to the HCC lesions via its arterial supply [33, 43, 44]. This technique is a combination of brachytherapy and embolization. Radioembolization uses the same technical principle as cTACE.
A randomized phase II study statistically observed a significantly longer time to progression for patients treated with SIRT when compared to those treated with cTACE [45]. Indications for SIRT are diffuse HCC, diffuse non-hypervascularized HCC, and HCC without response to TACE [46].
Yttrium-90 is the most common isotope for radioembolization. It is a ß-emitter which has a penetration of 2.5 mm and a half-life time of 64.2 h. Radioembolization using resin or glass microspheres has shown promising initial results.
Preparatory arteriography is required before radioemolization. The purpose of this arteriography is to determine where to inject the 90Y labeled microspheres by identifying the main artery which supplies the tumor and by confirming that there are no arteries arising close to the injection location which could lead to an extrahepatic spread of particles, primarily into the gastrointestinal tract. During preparatory arteriography, those arteries can be preventively occluded with coils [47]. After preparatory arteriography is finished, albumin particles labeled with 99mTc (99mTc-MAA) are injected, and subsequent scintigraphy ensures that there are no sites of extrahepatic gastrointestinal hyperactivity and that the hepato-pulmonary shunt remains low with the objective that the dose delivered to the lungs should be less than 30 Gy per treatment session, with a maximum cumulative dose of 50 Gy [47].
In the time of SIRT, selective injection of microspheres is achieved through closed circuit delivery using a proprietary delivery system specific to that particular device [27, 48]. Close monitoring using angiography during microsphere delivery is recommended to ensure that there is no significant inadvertent reflux into normal hepatic tissue or elsewhere, which may lead to inadvertent tissue damage. Due to the low tissue penetration, SIRT does not require isolation of the patient and requires only limited radioprotection measurements after the treatment.
Following SIRT, the HCC lesions are monitored using either contrast-enhanced CT or MRI to ensure that the lesions have undergone total necrosis and ruling out residual tumor, which would otherwise continue to grow (Fig. 2).

A 66-year-old patient with NASH-related HCC underwent selective internal radiation therapy (SIRT) of multiple HCC liver lesions. The patient had recurrence of HCC after the initial curative left hemihepatectomy and was in BCLC B stage. Eight weeks after SIRT, complete response according to mRECIST was documented. a Pre-treatment transverse contrast-enhanced T1-weighted MR image shows multiple HCC liver lesions. b Digital subtraction angiogram image during SIRT procedure shows the presence of arterial hypervascularity of multiple HCC lesions. c Post-treatment transverse contrast-enhanced T1-weighted MR image obtained 8 weeks after radioembolization (SIRT) shows the elimination of tumor vascularity and completely necrosis of intrahepatic lesions
SIRT has only few risks of complications. It can cause unspecific symptoms such as fever, nausea, pain, fatigue, and anorexia. If the microspheres accidentally enter the gastrointestinal system, they can cause local inflammation including pancreatitis, cholecystitis, ulcerations, and radiation-induced pneumonia [27, 49].
The safety of Y90 radioembolization has been documented in phase I and phase II clinical investigation [50]. In several retrospective studies, the efficacy of SIRT in the treatment of HCC has been reported (Table 1).
Salem et al. [51, 52] documented in a large prospective study that there was no significant difference regarding median survival between TACE group versus radioembolization group with 20.5 and 17.5 months, respectively [51]. A meta-analysis including 14 studies about radioembolization showed response rates of HCC ranging from 78 to 89% [53].
The relevant costs and effort associated with SIRT may limit a wider use of this technique.
Transarterial Therapies as Part of a Sequential Treatment of HCC
A combination of locoregional transarterial therapies might offer a good tool for the treatment of HCC, especially in a neoadjuvant setting. Neoadjuvant treatment is defined as a clinical situation in which the previous treatment with transarterial locoregional therapy caused a significant decrease in the size and number of HCC lesions so that a possible curative local treatment, such as hepatic resection or ablation with curative intent, could be performed.
Conclusion
The findings in the recent literature indicate that intraarterial therapies play an important role in the treatment of HCC and include multiple treatment options such as cTACE, TAE, DEB-TACE, and SIRT. Management of HCC requires a multidisciplinary approach for optimum, patient-tailored treatment in centers with excellent expertise in liver tumor treatment.
References
Cabibbo G, Latteri F, Antonucci M, Craxì A. Multimodal approaches to the treatment of hepatocellular carcinoma. Nat Clin Pract Gastroenterol Hepatol. 2009;6:159–169.
Ganne-Carrié N, Chaffaut C, Bourcier V, et al. Estimate of hepatocellular carcinoma’s incidence in patients with alcoholic cirrhosis. J Hepatol. 2018;69:1274–1283.
Streba LA, Vere CC, Rogoveanu I, Streba CT. Nonalcoholic fatty liver disease, metabolic risk factors, and hepatocellular carcinoma: an open question. World J Gastroenterol. 2015;21:4103–4110.
Kanda T, Matsuoka S, Yamazaki M, et al. Apoptosis and non-alcoholic fatty liver diseases. World J Gastroenterol. 2018;24:2661–2672.
El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011;365:1118–1127.
Singal AG, El-Serag HB. Hepatocellular carcinoma from epidemiology to prevention: translating knowledge into practice. Clin Gastroenterol Hepatol. 2015;13:2140–2151.
Thomas MB, Jaffe D, Choti MM, et al. Hepatocellular carcinoma: consensus recommendations of the National Cancer Institute clinical trials planning meeting. J Clin Oncol. 2010;28:3994–4005.
Rougier P, Mitry E, Barbare JC, Taieb J. Hepatocellular carcinoma (HCC): an update. Semin Oncol. 2007;34:S12–S20.
Lencioni R. Loco-regional treatment of hepatocellular carcinoma in the era of molecular targeted therapies. Oncology. 2010;78:107–112.
Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255.
Pesapane F, Nezami N, Patella F, et al. New concepts in embolotherapy of HCC. Med Oncol. 2017;34:58.
Molvar C, Lewandowski RJ. Intra-arterial therapies for liver masses: data distilled. Radiol Clin North Am. 2015;53:973–984.
Geschwind JF, Kudo M, Marrero JA, et al. TACE treatment in patients with sorafenibtreated unresectable hepatocellular carcinoma in clinical practice: final analysis of GIDEON. Radiology. 2016;8:150667.
Trevisani F, Golfieri R. Lipiodol transarterial chemoembolization for hepatocellular carcinoma: Where are we now? Hepatology. 2016;64:23–25.
European Association for the Study of the Liver1; European Organisation for Research and Treatment of Cancer. EASL–EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943.
Ramsey DE, Kernagis LY, Soulen MC, et al. Chemoembolization of hepatocellular carcinoma. J Vasc Interv Radiol. 2002;13:S211–S221.
Ahrar K, Gupta S. Hepatic artery embolization for hepatocellular carcinoma: technique, patient selection, and outcomes. Surg Oncol Clin N Am. 2003;12:105–126.
Massmann A, Rodt T, Marquardt S, et al. Transarterial chemoembolization (TACE) for colorectal liver metastases–current status and critical review. Langenbecks Arch Surg. 2015;400:641–659.
Gruber-Rouh T, Naguib NN, Eichler K, et al. Transarterial chemoembolization of unresectable systemic chemotherapy-refractory liver metastases from colorectal cancer: long-term results over a 10-year period. Int J Cancer. 2014;134:1225–1231.
Chang J, Charalel R, Noda C, et al. Liver-dominant breast cancer metastasis: a comparative outcomes study of chemoembolization versus radioembolization. Anticancer Res. 2018;38:3063–3068.
Wang M, Zhang J, Ji S, Shao G, et al. Transarterial chemoembolisation for breast cancer with liver metastasis: a systematic review. Breast. 2017;36:25–30.
Alexander ES, Soulen MC. Liver metastases from noncolorectal malignancies (neuroendocrine tumor, sarcoma, melanoma, breast). Cancer J. 2016;22:381–386.
Topaloglu S, Ozturk MH. Chemoembolization for neuroendocrine liver metastasis. Hepatogastroenterology. 2014;61:398–404.
Grozinsky-Glasberg S, Kaltsas G, et al. Hepatic intra-arterial therapies in metastatic neuroendocrine tumors: lessons from clinical practice. Endocrine. 2018;60:499–509.
Chen T, Chu ZH, Liu JP, et al. Application of adenosine triphosphate tumor chemosensitive assay system to individual chemotherapy for hepatocellular carcinoma. Aizheng. 2005;24:1018–1022. (Abstract).
Wu J, Song L, Zhao DY, Guo B, Liu J. Chemotherapy for transarterial chemoembolization in patients with unresectable hepatocellular carcinoma. World J Gastroenterol. 2014;20:10960–10968.
Gruber-Rouh T, Marko C, Thalhammer A, et al. Current strategies in interventional oncology of colorectal liver metastases. Br J Radiol. 2016;26:20151060.
Schicho A, Hellerbrand C, Krüger K, et al. Impact of different embolic agents for transarterial chemoembolization (TACE) procedures on systemic vascular endothelial growth factor (VEGF) levels. J Clin Transl Hepatol. 2016;4:288–292.
Raoul JL, Sangro B, Forner A, et al. Evolving strategies for the managementof intermediate-stage hepatocellular carcinoma: available evidence and expert opinion on the use of transarterial chemoembolization. Cancer Treat Rev. 2011;37:212–220.
Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37:429–442.
Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlledtrial. Lancet. 2002;359:1734–1739.
Cammà C, Schepis F, Orlando A, et al. Transarterial chemoembolization for unresectable hepatocellular carcinoma:meta-analysis of randomized controlled trials. Radiology. 2002;224:47–54.
Vande Lune P, Abdel Aal AK, Klimkowski S, et al. Hepatocellular carcinoma: diagnosis, treatment algorithms, and imaging appearance after transarterial chemoembolization. J Clin Transl Hepatol. 2018;6:175–188.
Takeba Y, Kumai T, Matsumoto N, et al. Irinotecan activates p53 with its active metabolite, resulting in human hepatocellular carcinoma apoptosis. J Pharmacol Sci. 2007;104:232–242.
Maluccio M, Covey AM, Gandhi R, et al. Comparison of survival rates after bland arterial embolization and ablation versus surgical resection for treating solitary hepatocellular carcinoma up to 7 cm. J Vasc Interv Radiol. 2005;16:955–961.
Varela M, Real MI, Burrel M, et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol. 2007;46:474–481.
Poon RT, Tso WK, Pang RW, et al. A phase I/II trial of chemoembolization for hepatocellular carcinoma using a novel intra-arterial drug-eluting bead. Clin Gastroenterol Hepatol. 2007;5:1100–1108.
Nam HC, Jang B, Song MJ. Transarterial chemoembolization with drug-eluting beads in hepatocellular carcinoma. World J Gastroenterol. 2016;22:8853–8861.
Lencioni R, de Baere T, Burrel M, et al. Transcatheter treatment of hepatocellular carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): technical recommendations. Cardiovasc Intervent Radiol. 2012;35:980–985.
Lammer J, Malagari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010;33:41–52.
Malagari K. Drug-eluting particles in the treatment of HCC: chemoembolization with doxorubicin-loaded DC Bead. Expert Rev Anticancer Ther. 2008;8:1643–1650.
Han S, Zhang X, Zou L, et al. Does drugeluting bead transcatheter arterial chemoembolization improve the management of patients with hepatocellular carcinoma? A metaanalysis. PLoS One. 2014;9:e102686.
Molvar C, Lewandowski RJ. Intra-arterial therapies for liver masses: data distilled. Radiol Clin North Am. 2015;53:973–984.
Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology. 2010;52:762–773.
Salem R, Gordon AC, Mouli S, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151:1155–1163.
Dezarn WA, Cessna JT, DeWerd LA, et al. Recommendations of the American Association of Physicists in Medicine on dosimetry, imaging, and quality assurance procedures for 90Y microsphere brachytherapy in the treatment of hepatic malignancies. Med Phys. 2011;38:4824–4845.
Aubé C, Bouvier A, Lebigot J, et al. Radiological treatment of HCC: interventional radiology at the heart of management. Diagn Interv Imaging. 2015;96:625–636.
Vente MA, Wondergem M, van der Tweel I, et al. Yttrium-90 microsphere radioembolization for the treatment of liver malignancies: a structured meta-analysis. Eur Radiol. 2009;19:951–959.
Fiorentini G, Aliberti C, Tilli M, et al. Intra-arterial infusion of irinotecan-loaded drug-eluting beads (DEBIRI) versus intravenous therapy (FOLFIRI) for hepatic metastases from colorectal cancer: final results of a phase III study. Anticancer Res. 2012;32:1387–1395.
Mazzaferro V, Sposito C, Bhoori S, et al. Yttrium-90 radioembolization for intermediate-advanced hepatocellular carcinoma: a phase 2 study. Hepatology. 2013;57:1826–1837.
Salem R, Lewandowski RJ, Kulik L, et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011;140:497–507.
Sangro B, Iñarrairaegui M, Bilbao JI. Radioembolization for hepatocellular carcinoma. J Hepatol. 2012;56:464–473.
Golfieri R, Bilbao JI, Carpanese L, et al. Comparison of the survival and tolerability of radioembolization in elderly vs. younger patients with unresectable hepatocellular carcinoma. J Hepatol. 2013;59:753–761.
Hatanaka T, Arai H, Shibasaki M, et al. Factors predicting overall response and overall survival in hepatocellular carcinoma patients undergoing balloon-occluded transcatheter arterial chemoembolization: a retrospective cohort study. Hepatol Res. 2018;48:165–175.
Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35:1164–1171.
Gruber-Rouh T, Kamal A, Eichler K, et al. Transarterial chemoembolization (TACE) using mitomycin with or without irinotecan for hepatocellular carcinoma in european patients. Oncol Res Treat. 2018;41:438–442.
Yamakado K, Miyayama S, Hirota S, et al. Hepatic arterial embolization for unresectable hepatocellular carcinomas: Do technical factors affect prognosis? Jpn J Radiol. 2012;30:560–566.
Takaki S, Sakaguchi H, Anai H, et al. Long-term outcome of transcatheter subsegmental and segmental arterial chemoemobolization using lipiodol for hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2012;35:544–554.
Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111:255–264.
Facciorusso A, Di Maso M, Muscatiello N. Drug-eluting beads versus conventional chemoembolization for the treatment of unresectable hepatocellular carcinoma: a meta-analysis. Dig Liver Dis. 2016;48:571–577.
Mantry PS, Mehta A, Madani B, et al. Selective internal radiation therapy using yttrium-90 resin microspheres in patients with unresectable hepatocellular carcinoma: a retrospective study. J Gastrointest Oncol. 2017;8:799–807.
Kim DY, Park BJ, Kim YH, et al. Radioembolization with Yttrium-90 resin microspheres in hepatocellular carcinoma: a multicenter prospective study. Am J Clin Oncol. 2015;38:495–501.
Kolligs FT, Bilbao JI, Jakobs T, et al. Pilot randomized trial of selective internal radiation therapy vs. chemoembolization in unresectable hepatocellular carcinoma. Liver Int.. 2015;35:1715–1721.
Gramenzi A, Pettinato C, Cappelli A, et al. Reply to: “Sorafenib or (90) Y loaded resin microsphere radioembolization for locally-advanced hepatocellular carcinoma, what should we trust?”. Liver Int. 2015;35:1780–1781.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vogl, T.J., Gruber-Rouh, T. HCC: Transarterial Therapies—What the Interventional Radiologist Can Offer. Dig Dis Sci 64, 959–967 (2019). https://doi.org/10.1007/s10620-019-05542-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05542-5