
Abstract
Background
Children with active inflammatory bowel disease (IBD) are frequently underweight. Anti-tumor necrosis factor (anti-TNF) agents may induce remission and restore growth. However, its use in other autoimmune diseases has been associated with excess weight gain. Our aim was to examine whether children with IBD could experience excess weight gain.
Methods
A centralized diagnostic index identified pediatric IBD patients evaluated at our institution who received anti-TNF therapy for at least 1 year between August 1998 and December 2013. Anthropometric data were collected at time of anti-TNF initiation and annually. Excess weight gain was defined as ΔBMI SDS (standard deviation score) where patients were (1) reclassified from “normal” to “overweight/obese,” (2) “overweight” to “obese,” or (2) a final BMI SDS >0 and ΔSDS >0.5.
Results
During the study period, 268 children received anti-TNF therapy. Of these, 69 had sufficient follow-up for a median of 29.3 months. Median age at first anti-TNF dose was 12.8 years. At baseline, mean weight SDS was −0.7 (SD 1.4), while mean BMI SDS was −0.6 (1.3). Using baseline BMI SDS, 11.6% were overweight/obese. At last follow-up (LFU), however, the mean ΔBMI SDS was 0.50 (p < 0.0001). However, 10 (17%) patients had excess weight gain at LFU; 3 patients were reclassified from “normal” to “obese,” and 7 had a final BMI SDS >0 and ΔSDS >0.5.
Conclusions
Pediatric patients with IBD may experience excess weight gain when treated with anti-TNF agents. Monitoring for this side effect is warranted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Patients with inflammatory bowel disease (IBD) frequently experience weight loss due to chronic diarrhea and malabsorption. Patients may avoid eating to lessen these symptoms, exacerbating weight loss [1]. Children subsequently may develop growth failure [2]. Treatment with anti-tumor necrosis factor agents (anti-TNF) has been shown to lead to weight gain and a reversal of growth failure in children [3, 4]. It is unclear, however, if patients may gain excessive weight as a result of anti-TNF therapy. An average of 5.2 kg weight gain was reported in a retrospective survey of adult Crohn’s patients, and similar findings have been reported in rheumatoid arthritis, psoriasis, and psoriatic arthritis [5,6,7].
Due to reports of weight gain in adults and anecdotal experience in children, we sought to determine if pediatric patients with IBD experienced excessive weight gain when exposed to anti-TNF therapy.
Methods
Study Design and Population
This retrospective study was approved by the Mayo Clinic Institutional Review Board. The medical records of all patients seen in the Division of Pediatric Gastroenterology and Hepatology were electronically searched to identify patients with IBD who received anti-TNF therapy between August 1998 and December 2013. Clinical notes were searched for the words “ulcerative colitis” or “pancolitis,” “Crohn’s disease,” “indeterminate colitis,” “infliximab” or “Remicade,” “adalimumab” or “Humira,” and “certolizumab” or “Cimzia.” Pediatric patients were defined as those who were less than 18 years of age at the time of first anti-TNF therapy.
Records were reviewed for demographic information, duration and extent of disease, length of follow-up, and dates and dosing of anti-TNF therapy. Prior and concomitant medications were recorded. We collected anthropomorphic data at time of anti-TNF initiation, 2, 6, and 12 months, annually, as well as last follow-up (LFU). Last follow-up was defined as the end of the study period, discontinuation of anti-TNF therapy, or intestinal surgery. Patients were excluded if they had insufficient data or follow-up (<12 months after anti-TNF initiation). If patients switched anti-TNF agents, we continued to collect anthropometric data if the time interval between agents did not exceed 3 months. The physician global assessment (PGA) was used to assess the patient’s disease activity at each time point.
Anthropometric Data
Weight, height, and body mass index (BMI) were calculated at each time point, and converted to standard deviation scores (SDS) for analyses, based on Centers for Disease Control 2000 published data [8]. These SDS scores account for differences in the rate of change in weight and BMI based on age and gender. For instance, an appropriate weight gain over 1 year at the 50‰ would be 5.4 kg for a 13-year-old boy and 3.5 kg for a 13-year-old girl, but only 3.6 kg for a 16-year-old boy and 1.3 kg for a 16-year-old girl. Weight and BMI SDS at each time point are reported as mean with standard deviation. Using Centers for Disease Control data, underweight was defined as BMI SDS <−1.645 (corresponding to the 5‰), overweight between 1.036 (85‰) and 1.645 (95‰), and obese SDS >1.645 (95‰), respectively. Although an increase in weight or BMI SDS would be considered a statistically significant change in weight gain, the definition of excess weight gain is lacking in the literature. Further, patients who are underweight and/or growth stunted due to active Crohn’s disease may start with negative SDS scores and have appropriately large gains in weight, height, and BMI after achieving remission. In the absence of an existing definition for excess weight gain, we chose to describe the number of patients who by BMI SDS (1) changed from “normal” (between −1.645 and 1.036) to “overweight/obese” (>1.036), (2) changed from “overweight” (>1.036) to “obese” (>1.645), and (3) had both a final BMI SDS >0 and ΔSDS >0.5 during the study period.
Statistical Analysis
Descriptive statistics were used, including percentages for discrete variables, and mean, median, and range for continuous variables. Differences between baseline and last follow-up SDS were analyzed using a paired t test. Linear mixed effects models were used to analyze weight and BMI SDS over time by gender, IBD type, Paris age classification at baseline, baseline weight and BMI categories with random effects for subject. Each univariate model included time, the covariate, and the interaction between time and the covariate. JMP version 10.0 and SAS version 9.3 (Sas Institute Inc. Cary, NC) was used for all analyses, and p < 0.05 was considered statistically significant. All statistical tests were two-sided.
Results
Demographics and Medication Use
Between August 1998 and December 2013, 268 pediatric patients with IBD evaluated at our institution received anti-TNF therapy, of whom 69 had at least 1 year of anti-TNF therapy and follow-up (Supplement 1). The baseline characteristics of the cohort are summarized in Table 1. The median age at time of diagnosis was 12.8 years (range 4.2–17.4), with a median of 7.3 months (range 0–133) from IBD diagnosis to start of anti-TNF therapy. Median follow-up of our cohort was 29.3 months (range 12.0–109.2), with data available beyond 24 months in 43 patients (62.3%). The majority of patients had Crohn’s disease (85.5%), with a predominantly ileocolonic (83.1%) distribution and inflammatory phenotype. However, 12 patients (20.3%) had penetrating disease. Of the 8 patients with ulcerative colitis, 5 (62.5%) had pancolitis at initiation of anti-TNF therapy.
The type of anti-TNF used, concomitant medications, and baseline serology are shown in Table 2. Infliximab (IFX) was the most common anti-TNF therapy used for 63 (92.6%) of patients, while 32 (46.4%) received adalimumab, and 8 (11.6%) received certolizumab. During the study period, 26 (37.7%) switched to a second drug, while 4 (5.8%) received all three anti-TNF agents. Escalation of therapy (dose or frequency) was instituted for 39 (61.9%) patients, with an average of 1.8 changes (range 0–4). Concomitant immunomodulation was used in 25 (36.2%) patients. Use of corticosteroids at baseline, 24 months, and LFU was 68.1, 6.3, and 5.8%, respectively. Within 2 months of anti-TNF initiation, 21 (31%) achieved and sustained clinical remission through the remaining study period. Twenty-three (33.3%) patients discontinued all anti-TNF therapy during the study period; 11 (16.1%) due to side effects, 5 (7.2%) switched to an immunomodulator, and 6 (5.9%) required surgery.
Weight and BMI SDS of Overall Cohort
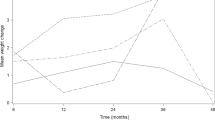
Figure 1 shows box plots of weight and BMI SDS over time of the overall cohort. (SDS scores of weight and BMI at baseline, 12, 24 months, and LFU are shown in Supplement 2.). At 24 months, weight and BMI data were available for 32 and 30 patients, respectively. At initiation of anti-TNF therapy, the mean weight SDS was −0.65 (SD 1.4), while the mean BMI SDS was −0.59 (SD 1.3). At baseline, 15 (21.7%) patients were underweight (weight SDS < −1.645), while 6 (8.7%) were overweight with a weight SDS >1.036. Using baseline BMI SDS, the percentages for underweight and overweight/obese patients were 15.9 and 11.6%, respectively. At 24 months after anti-TNF initiation, the mean weight SDS and BMI SDS at 24 months was −0.09 (1.1), and −0.09 (0.9), respectively. At LFU, the mean weight SDS and BMI SDS was −0.10 (1.4) and −0.09 (1.3), respectively. After 24 months of biologic therapy, the average Δweight SDS and ΔBMI SDS were not significant compared to baseline. At LFU, however, the mean Δweight SDS was 0.56 (p < 0.0001), while ΔBMI SDS was 0.50 (p < 0.0001).

Weight and BMI SDS over time in pediatric patients treated with anti-TNF therapy. o and + indicate outliers and the mean of the weight and BMI SDS scores, respectively
Change in Weight Categories Over Time
Table 3 outlines the weight categories using BMI SDS from baseline to LFU. Patients who were “underweight” at baseline either remained underweight or normalized. Of the 58 patients who were of “normal,” “overweight,” or “obese” at baseline, 10 (17%) gained excess weight using our criteria. Of the 50 patients who were initially “normal” weight at baseline, 3 were “overweight/obese” at follow-up. An additional 5 had a final SDS >0.5 and ΔSDS >0.5. Of the 4 patients who were “obese” at baseline, 2 had a ΔSDS >0.5. The 8 patients with a baseline BMI SDS >1.036 (“obese”) remained so at LFU. The median follow-up time in this subset of patients was 31.5 months (range 13.6–108). We examined the potential contribution of corticosteroids to excess weight gain. Nine children had no exposure to corticosteroids for at least 12 months prior to LFU, while 1 child had no exposure for at least 6 months. Patients who were underweight at baseline gained weight faster than patients who were of normal weight or obese (p = 0.02), likely reflecting improvements in disease activity (Supplement 3).
A larger percentage of patients with ulcerative colitis were overweight by weight SDS (25 vs. 5.1%) and BMI SDS (25 vs. 8.5%) than Crohn’s disease at baseline. At LFU, patients with Crohn’s disease had statistically significant weight gain, with a mean weight ΔSDS of 0.57 (SD 0.8) and ΔBMI SDS of 0.52 (SD 0.8) (p < 0.0001) (Supplement 2). Although no difference in weight gain over time was observed by IBD type at 24 months (p = 0.18), slower gains in weight SDS were observed in patients with Crohn’s disease compared to ulcerative colitis (−0.01, 95% CI −0.02, −0.006, p = 0.0002) (Supplement 3).
At baseline, more females were overweight by both weight (12.5 vs. 4.5%) and BMI SDS (15.6 vs. 8.1%) than males. While both genders experienced significant increases in both weight and BMI SDS at LFU (Supplement 2), we did not observe a difference between genders over time. However, younger patients (<10 years) experienced faster weight gain than older patients at 24 months (p = 0.02) and LFU (p < 0.001).
We did not detect differences in need for dose increases based on baseline weight categories. Disease activity during the course of the study period (sustained remission within 2 months of starting anti-TNF agent or flares during the study period) was not associated with significant changes in weight or BMI gain.
Discussion
To our knowledge, this is the first study to investigate whether anti-TNF therapy is associated with excessive weight gain in children with IBD. In our cohort of 69 patients, 10 patients gained excess weight by BMI SDS, including 3 patients who were of “normal” weight at baseline but were “obese” at LFU. Those who were overweight at baseline remained in this category. We did not detect differences in weight gain by gender or IBD type.
The prevalence of overweight/obese pediatric patients with IBD varies across studies. In our study, 11.6% were overweight/obese at baseline using BMI SDS. Data from the ImproveCareNow registry reported that 20% of CD patients were overweight or obese at time of study entry, while inception data from the Pediatric IBD collaborative and the Wisconsin cohort reported 9 and 10%, respectively. These inception cohorts reported 20 and 34% overweight/obese prevalence in their UC patients [4, 6].
Studies of anti-TNF weight gain in patients with IBD are scant. Although Issa et al. reported an average weight gain of 5.3 kg over 24 months in adults with IBD treated with infliximab, the ImproveCareNow IBD registry observed a small but nonsignificant association in pediatric patients who were overweight/obese and concomitant infliximab use [5, 9]. Studies in the adult rheumatology and dermatology literature suggest significant weight gains ranging from 2.2 to 4.8 kg. Brown et al.’s retrospective study of patients with rheumatoid arthritis treated with anti-TNF agents found that although 64.8% gained an average of 4.6 kg over 24 months, 32.1% lost an average of 4.36 kg. In contrast to our findings, higher BMI at baseline was negatively associated with weight gain [6]. In a large open-label study of 106 patients with spondyloarthropathy treated with infliximab or etanercept, an average weight gains of 2.2 kg occurred within 24 months [10]. Renzo et al. [7] reported similar findings in their study of infliximab and etanercept in adult patients with psoriasis (2.2 kg) and psoriatic arthritis (1.63 kg) in only 24 weeks. Florin et al. reported incremental weight gain over time in 35 patients with psoriasis treated with infliximab—2.5 kg at 12 months and 4.8 kg at 24 months. As in our cohort, changes were greater in patients who were of normal weight at baseline than those who were overweight/obese [11]. Only one study has examined other autoimmune conditions treated with anti-TNF therapy in the pediatric population; Shafferman et al. [12] reported a statistically significant increase of BMI SDS score of 0.15 in pediatric patients with juvenile idiopathic arthritis, although this was not statistically different from increases in a cohort not exposed to anti-TNF therapy.
The mechanism of excess weight gain (beyond normalization of weight and/or growth) caused by anti-TNF therapy is not fully understood. TNF-alpha is known to cause cachexia, which in addition to weight loss, is associated with muscle and adipose wasting and anorexia. Anti-TNF therapy may not only reverse anorexia, but contribute to an ongoing increase in appetite through effects on ghrelin, leptin, and adiponectin [13]. Ghrelin is an orexigenic hormone produced by the stomach and intestine in response to hunger, leading to increased food intake [14]. Studies in patients with active rheumatoid arthritis have demonstrated low levels in active disease and increased serum levels after anti-TNF treatment [13, 15]. In contrast, leptin is an anorexic peptide hormone produced by adipocytes, which can alter food intake and subsequently body weight and fat stores through its action on the hypothalamus [16]. Leptin levels have been shown to be decreased in children with IBD, but the effect of anti-TNF therapy on levels has been variable [17,18,19,20].
This excess weight gain seen with anti-TNF therapy may have clinical consequences. First, it is our anecdotal experience that patients and their families brought up their concerns about the weight gain and appearance. Secondly, there may be subsequent failure to achieve or maintain clinical response to anti-TNF therapy. Obesity has been associated with increased levels of the pro-inflammatory adipokines leptin, resistin, and visfatin, as well as decreased levels of the anti-inflammatory adiponectin [21]. A recent meta-analysis of anti-TNF therapy in adults with autoimmune diseases showed an OR 2.16 risk of failing to achieve clinical response or remission in obese patients, regardless of fixed or weight-based dosing [22]. The ImproveCareNow registry observed higher rates of IBD-related surgery in children who were overweight or obese [9]. While we did not observe a correlation between overweight/obesity and disease activity, our sample size may be too small to observe a difference, and this was not a primary aim of our study.
In our cohort, patients <10 years of age had the most weight gain during our study period. This may reflect the faster growth velocity seen in early puberty and/or greater impact of anti-TNF agents seen in this population. We did not observe a difference in the proportion of patients with excess weight gain between patients <10 vs. ≥10 years of age, but this is likely due to sample size. Walters et al. [23] observed that infliximab only improved the height velocity in pediatric Crohn’s when used in children in early puberty compared to late puberty. Children <10 years of age would be Tanner 1-II, while 10–15 years of age may span the spectrum of pubertal staging. At our center, we do not routinely record pubertal staging; thus, our analysis was confined to Paris age classification. Additional studies with a larger cohort may help clarify whether anti-TNF effects on weight would also vary by pubertal staging.
There are several limitations to our study. Although 268 patients received anti-TNF therapy during our study period, we analyzed 69 patients with at least 1 year of follow-up anthropometric data. As a tertiary care center, some patients who switched care to our center had already initiated anti-TNF therapy without baseline anthropometric data available. In addition, it is our practice to coordinate infliximab infusions with local institutions or home infusions when feasible for the convenience of our patients. Although monitoring serology is obtained and results faxed to us at the time of infusions, we typically do not receive anthropometric data. Patients who received adalimumab therapy at home may not have been seen close to the timepoints we set for our study protocol. The majority of our patients used corticosteroids at some point during the study period, and the retrospective nature of the study precluded adjusting for duration and dosing. While these could have confounded our study, the minority of patients were using corticosteroids at 24 months (6.3%) and LFU (5.8%). Further, those who gained excess weight by our criteria had not been exposed to corticosteroids for at least 6 months. Lastly, our cohort was largely Caucasian and centered in the Midwest United States, so our results may not be generalizable to other ethnicities and regions.
Our study demonstrates that some pediatric patients with IBD may experience excessive weight gain when treated with anti-TNF agents. Those who are of “normal” or “overweight” by BMI SDS seem to be at greater risk. Additional larger studies are needed to verify this association. Monitoring for this side effect and appropriate counseling regarding lifestyle modifications are warranted.
Abbreviations
- IBD:
-
Inflammatory bowel disease
- Anti-TNF:
-
Anti-tumor necrosis factor
- BMI:
-
Body mass index
- LFU:
-
Last follow-up
- SDS:
-
Standard deviation score
References
Gerasimidis K, McGrogan P, Edwards CA. The aetiology and impact of malnutrition in paediatric inflammatory bowel disease. J Hum Nutr Diet. 2011;24:313–326.
Vadan R, Gheorghe LS, Constantinescu A, et al. The prevalence of malnutrition and the evolution of nutritional status in patients with moderate to severe forms of Crohn’s disease treated with Infliximab. Clin Nutr. 2011;30:86–91.
Borrelli O, Bascietto C, Viola F, et al. Infliximab heals intestinal inflammatory lesions and restores growth in children with Crohn’s disease. Dig Liver Dis. 2004;36:342–347.
Hyams J, Crandall W, Kugathasan S, et al. Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology. 2007;132:863–873.
Issa M, Weber L, Shidham S, et al. Infliximab significantly increases proportion of overweight/obese Crohn’s disease patients receiving longterm maintenance therapy. Gastroenterology. 2006;130:A209.
Brown RA, Spina D, Butt S, et al. Long-term effects of anti-tumour necrosis factor therapy on weight in patients with rheumatoid arthritis. Clin Rheumatol. 2012;31:455–461.
Renzo LD, Saraceno R, Schipani C, et al. Prospective assessment of body weight and body composition changes in patients with psoriasis receiving anti-TNF-alpha treatment. Dermatol Ther. 2011;24:446–451.
Kuczmarski RJ, Ogden CL, Guo SS, et al. CDC growth charts for the United States: methods and development. Vital Health Stat. 2000;11:1–190.
Long MD, Crandall WV, Leibowitz IH, et al. Prevalence and epidemiology of overweight and obesity in children with inflammatory bowel disease. Inflamm Bowel Dis. 2011;17:2162–2168.
Briot K, Gossec L, Kolta S, et al. Prospective assessment of body weight, body composition, and bone density changes in patients with spondyloarthropathy receiving anti-tumor necrosis factor-alpha treatment. J Rheumatol. 2008;35:855–861.
Florin V, Cottencin AC, Delaporte E, et al. Body weight increment in patients treated with infliximab for plaque psoriasis. J Eur Acad Dermatol Venereol. 2013;27:e186–e190.
Shafferman A, Fontaine KR, Cron RQ, et al. Changes in body mass index in children with juvenile idiopathic arthritis treated with tumor necrosis factor inhibitors. J Rheumatol. 2014;41:113–118.
Gonzalez-Gay MA, Garcia-Unzueta MT, Berja A, et al. Anti-tumour necrosis factor alpha therapy modulates ghrelin in patients with severe rheumatoid arthritis. Ann Rheum Dis. 2008;67:1644–1646.
Kalra SP, Bagnasco M, Otukonyong EE, et al. Rhythmic, reciprocal ghrelin and leptin signaling: new insight in the development of obesity. Regul Pept. 2003;111:1–11.
Otero M, Nogueiras R, Lago F, et al. Chronic inflammation modulates ghrelin levels in humans and rats. Rheumatology. 2004;43:306–310.
Roubos EW, Dahmen M, Kozicz T, et al. Leptin and the hypothalamo-pituitary-adrenal stress axis. Gen Comp Endocrinol. 2012;177:28–36.
Aurangzeb B, Leach ST, Lemberg DA, et al. Assessment of nutritional status and serum leptin in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2011;52:536–541.
Fawcett RL, Waechter AS, Williams LB, et al. Tumor necrosis factor-alpha inhibits leptin production in subcutaneous and omental adipocytes from morbidly obese humans. J Clin Endocrinol Metab. 2000;85:530–535.
Franchimont D, Roland S, Gustot T, et al. Impact of infliximab on serum leptin levels in patients with Crohn’s disease. J Clin Endocrinol Metab. 2005;90:3510–3516.
Karmiris K, Koutroubakis IE, Xidakis C, et al. The effect of infliximab on circulating levels of leptin, adiponectin and resistin in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2007;19:789–794.
Versini M, Jeandel PY, Rosenthal E, et al. Obesity in autoimmune diseases: not a passive bystander. Autoimmun Rev. 2014;13:981–1000.
Singh S, Facciorusso A, Singh AG, et al. Obesity is associated with inferior response to anti-TNF therapy in immune-mediated inflammatory diseases: a systematic review and meta-analysis. Gastroenterology. 2017;152:S154.
Walters TD, Gilman AR, Griffiths AM. Linear growth improves during infliximab therapy in children with chronically active severe Crohn’s disease. Inflamm Bowel Dis. 2007;13:424–430.
Acknowledgments
The authors thank Kevin Chevalier for assisting in statistical analysis.
Author’s contribution
LH contributed to the acquisition and analysis of data, and writing of the manuscript. RC contributed to the design, data acquisition, and writing of the manuscript. BM contributed to the statistical analysis and interpretation of data. FE contributed to the design, analysis, and interpretation of data. SK contributed to the conception and design, interpretation of data, and writing of the manuscript. JT contributed to the conception and design, analysis and interpretation of data, and writing of the manuscript. All the authors have approved the final version for publication and agree to be accountable for this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Haas, L., Chevalier, R., Major, B.T. et al. Biologic Agents Are Associated with Excessive Weight Gain in Children with Inflammatory Bowel Disease. Dig Dis Sci 62, 3110–3116 (2017). https://doi.org/10.1007/s10620-017-4745-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-017-4745-1