
Abstract
Background
There are limited data on the effect of curry on gastroesophageal reflux disease (GERD). Our objective was to study the effects of curry on GERD.
Methods
Symptomatic non-erosive gastroesophageal reflux disease (NERD) patients and healthy volunteers underwent ambulatory 24-h esophageal pH monitoring before consumption of either 400 or 800 ml of curry; they were monitored for 3 h thereafter for changes in esophageal pH and upper abdominal symptoms. Selected volunteers were monitored similarly after water ingestion.
Results
In total, 25 NERD patients (23 males; mean age, 45 years) and 19 volunteers (13 males; mean age, 22 years) participated. In both patients and volunteers, curry ingestion induced more esophageal acid exposure than did ingestion of a similar volume of water. Curry induced significantly more esophageal acid exposure in NERD patients than in volunteers. Upper abdominal symptoms and esophageal acid exposure were more severe and persisted longer in patients than in volunteers.
Conclusion
Curry induced more acid reflux and caused worse symptoms in patients with NERD than in healthy individuals. Patients with NERD should be advised to avoid curry ingestion.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ingestion of chilli, a common ingredient in curry, causes various gastrointestinal symptoms, including heartburn, chest discomfort, nausea, belching, abdominal discomfort and distension in up to 42% of patients presenting with chronic abdominal pain [1]. Although the pathogenesis of these symptoms is unknown, it seems possible that some, for example heartburn and chest discomfort, might have arisen as a result of increased esophageal acid exposure, because chilli is known not to affect esophageal motility [2]. As stated in a review article, although some patients experience heartburn after eating spicy food, limited data have been published regarding the effects of ingestion of spicy food on esophageal pH [3]. Gastroesophageal reflux disease (GERD) is an increasingly common disease in Asia [4]. In multi-ethnic Asia, it has been noted that reflux-type symptoms are more common among Indians than Chinese or Malays [5]. Curry is a common component of the Asian diet. Whether curry induces acid reflux and produces reflux-type symptoms is not known. The objective of this study was to investigate the effects of curry on gastroesophageal reflux.
Materials and Methods
Study Population
Consecutive patients attending the gastroenterology department at a tertiary hospital in Singapore were invited to participate in the study if they had non-erosive reflux disease (NERD), defined as the presence of a dominant complaint of heartburn on two or more days per week over a period of at least three months with normal upper GI endoscopy. A patient was excluded from the study if he or she:
-
1.
was unable to consume curry for any reason;
-
2.
was suffering from current or previous organic gastrointestinal problems including peptic ulcer disease;
-
3.
was younger than 18 or older than 70 years of age;
-
4.
in the case of female, was pregnant; or
-
5.
had used prescribed drugs, for example proton-pump inhibitors or H2-receptor antagonists, for at least a week before recruitment.
In addition, a separate group of healthy, asymptomatic men and non-pregnant women volunteers aged between 18 and 35 years with no previous history of GERD or any of its related symptoms were recruited as controls.
Investigational Material
The material investigated was a 25% (w/v) suspension of a commercial curry powder (Baba Products (M) Sdn. Bhd, Kuala Lumpur, Malaysia) which comprises a mixture of coriander, chilli, cumin, fennel, turmeric, chickpeas, pepper, cinnamon, cardamom, star anise, cloves, and other spices. The curry suspension was boiled for 30 min and cooled to room temperature before consumption. In this study, 400 or 800 ml (with twice the curry content) of the cooked curry suspension was tested. The pH of the curry suspension used was measured to be 7.
Study Procedures
This study was approved by the hospital Institutional Review Board before subject recruitment. All participants gave informed consent before enrolment into the study. On enrolment, all patients were questioned for characteristics of their symptoms using a standard questionnaire which principally assessed six upper abdominal symptoms: fullness, bloating, discomfort, pain, nausea, and heartburn. The severity of these symptoms were scored using an analog scale of 0–10 where 0 = absent and 10 = unbearable, and a total symptom score was computed. The patients had to have normal findings on esophagogastroduodenoscopy performed within 6 months before study entry. Although the volunteers were not required to undergo esophagogastroduodenoscopy for the study, they were carefully interviewed and examined to exclude medical illness.
Standard manometry was performed as previously described [6] on all the subjects after an overnight fast. This was followed by ambulatory 24-h esophageal pH monitoring [6], for which the subject was intubated transnasally with a monocrystalline antimony pH electrode (Synectics Medical, Stockholm, Sweden) such that the electrode was located 5 cm above the upper border of the lower esophageal sphincter. A separate silver/silver-chloride reference electrode was attached to the skin of the non-dominant shoulder. Both electrodes were connected to a digital data recorder (Digitrapper Mark 11 Gold, Synectics Medical, Stockholm, Sweden) which sampled esophageal pH data at a rate of 4 Hz. Subjects were allowed to return to their home or working place with the apparatus on. They could assume their normal activities and eat their usual meals but not take drinks and foods of pH less than 4. Values obtained during the daytime (“upright”) period during 24-h pH monitoring were taken as baseline reading.
Subjects returned to the hospital the following day. After a 1-h stabilization period, subjects were asked to consume either 400 or 800 ml of the cooked curry suspension over a 5-min period. The presence and severity of various upper abdominal symptoms were assessed as described above just before the meal, and at fixed time intervals (15, 30, 60, 90, 120, 150, and 180 min) after ingestion of curry. After each time interval, the sum of the scores of all the symptoms was computed to give the total symptom score. Ambulatory esophageal pH monitoring was left on until 180 min post-ingestion of curry. During the assessment time period, subjects were allowed to move about or sit upright but were prohibited from reclining.
At the end of the 3 h monitoring period, esophageal pH data were transferred from the recorder to a personal computer and analyzed using dedicated commercial software (EsopHogram version 5.60; Gastrosoft, USA). The number of refluxes, duration of refluxes, and esophageal acid exposure time were computed on the basis of the following criteria:
-
1.
a drop of the esophageal pH to less than 4 for at least 4 s would indicate the onset of a reflux episode;
-
2.
a subsequent rise of pH to above 4 would indicate the end of the reflux episode; and
-
3.
in the event of a successive fall of pH below 4 within a 5-s period, the consecutive reflux episodes would be taken as one single complex.
The esophageal acid exposure time, defined as the total percentage of time the pH was below 4 (over the daytime period during the 24-h pH monitoring for the baseline studies, or over 3 h for the post-ingestion studies), was computed for each subject.
In addition, the volunteers who ingested 800 ml curry were also asked to undergo a 3-h water drink test a week later. The test was conducted in exactly the same manner as the curry stress test, except that each volunteer ingested 800 ml water instead of the curry.
Measures of Outcome
The primary measure of outcome was the change in esophageal pH after ingestion of curry. It was expressed as total percentage of time the pH remained below 4. The secondary measure of outcome was the concurrent change of the symptom scores. All measures of outcome were compared with the respective baseline levels taken before ingestion of the curry.
Statistical Analysis
All statistical analysis was performed with the Statistical Package for the Social Sciences (Version 13.0; SPSS, Chicago, Illinois, USA). Group symptom scores were computed by summing individual scores and expressed as mean ± SE. A repeated measurement analysis was performed to compare the symptom scores between the patients and volunteers. The Wilcoxon signed rank test was performed to compare the percentage of time the pH was below 4 in subjects before and after ingestion of curry. The Mann–Whitney U test was performed to compare the number of refluxes, duration of long refluxes, and mean percentage of time the pH was below 4 after ingestion of curry among the patients and volunteers. Sub-group analysis by volume of ingested curry was also performed for the above-mentioned analyses. Statistical significance was assumed at P ≤ 0.05.
Results
Demographic Characteristics of Subjects
In total, 25 patients with NERD and 19 healthy volunteers participated in this study. The subjects were predominantly Chinese (patients, 64%; volunteers, 89.5%) and mostly males (patients, 92%; volunteers, 73.7%). The mean age of patients was 44.8 ± 2.4 years (range, 19–68 years) whereas that of volunteers was 21.5 ± 0.9 years (range, 18–35 years). At baseline, more than half of the NERD patients had upper abdominal symptoms including heartburn. Fried, spicy, or sour foods were felt by most of these patients to be a likely cause of an aggravation of their heartburn. None of the volunteers and NERD patients was using aspirin or non-steroidal anti-inflammatory drugs.
Effect of Curry Ingestion on Healthy Volunteers
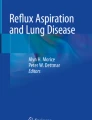
None of the healthy volunteers had abnormal reflux during the 24 h pH monitoring before curry ingestion. Of the 19 healthy volunteers, eight ingested 400 ml curry and 11 ingested 800 ml. Post-ingestion, both groups experienced statistically similar number of refluxes, number of long refluxes, duration of long refluxes, and percentage of time esophageal pH remained below 4. One of the eight who ingested 400 ml curry and five of the 11 who ingested 800 ml had a time esophageal pH was below 4 exceeding four percent post-ingestion, but the difference is not statistically significant (P = 0.153). Overall, the 19 volunteers had significantly higher mean total symptom scores 15 min (9.6 ± 2.1, P = 0.005) and 30 min (6.8 ± 1.7, P = 0.015) post-ingestion compared with their own baseline mean total symptom scores (2.9 ± 1.1) (Fig. 1). Total symptom scores at 60-min (4.3 ± 1.5), 90-min (2.8 ± 1.1), 120-min (2.3 ± 1.0), 150-min (1.8 ± 0.9), and 180-min (0.7 ± 0.6) did not differ from baseline levels. There were also no differences among total symptom scores for fullness, bloating, discomfort, pain, nausea, and heartburn throughout the monitored post-ingestion period.

Mean total symptom scores for patients and volunteers at different times post-ingestion of curry
Effect of Curry Ingestion on NERD Patients
All patients with NERD had abnormal pH data supporting abnormal reflux during the 24 h pH monitoring before curry ingestion. Of the 25 NERD patients, 15 ingested 400 ml curry and 10 ingested 800 ml. Just as with healthy volunteers, there was no significant difference in the number of refluxes, number of long refluxes, duration of longest reflux, and percentage of time esophageal pH remained less than 4 between patients who ingested 400 and 800 ml curry, whether at the baseline or after curry ingestion. For the patients who ingested 400 ml curry, mean (±SE) percentage of time the pH was below 4 increased from 5.4 ± 1.2 to 11.8 ± 2.2 (P = 0.007) post-curry ingestion; for patients who ingested 800 ml curry, mean percentage of time the pH was below 4 increased from 6.4 ± 3.3 to 20.5 ± 6.8 (P = 0.007) post-ingestion. Overall, the mean (±SE) percentage of time the esophageal pH remained below 4 increased from the baseline level of 5.8 ± 1.4 to 15.3 ± 3.1 after ingestion of curry in all NERD patients (P < 0.001).
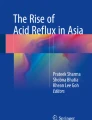
At baseline, the mean total symptom scores were similar in both 400 and 800 ml groups. However, after curry ingestion, the mean (±SE) total symptom scores were consistently higher in patients who ingested 800 ml curry compared with those who ingested 400 ml (23.9 ± 4.1 vs. 8.3 ± 1.3 at 15 min after curry ingestion; 22.5 ± 3.7 vs. 9.7 ± 1.1 at 30 min; 22.0 ± 3.9 vs. 8.5 ± 1.0 at 60 min; 20.8 ± 4.8 vs. 7.5 ± 1.1 at 90 min; 16.7 ± 3.8 vs. 6.2 ± 1.3 at 120 min; 16.7 ± 4.0 vs. 4.5 ± 1.1 at 150 min; 14.1 ± 3.7 vs. 3.3 ± 1.0 at 180 min; P < 0.05). By combining the 400 and 800 ml groups, the mean total symptom scores taken 15, 30, 60, 90, 120 and 150 min after ingestion of curry were significantly higher than that at baseline (P ≤ 0.005) but the score at 180-min returned to baseline level (P = 0.136)(Fig. 1). Figure 2 depicts a typical pH monitoring strip from a patient after ingestion of curry. Note that the post-curry ingestion drop of esophageal pH to less than 4 persisted until the end of the 3-h monitoring period. The pH drop occurred in conjunction with the appearance of upper abdominal symptoms.

pH monitoring strip from a patient before and after ingestion of 400 ml curry (yellow box)
Difference in Response After Curry Ingestion between Healthy Volunteers and Patients
Comparison of differences in responses between the healthy volunteers and NERD patients was determined by combining the 400 and 800 ml ingestion groups. Post-ingestion of curry, the NERD patients experienced a significantly greater number of refluxes (30.4 ± 4.5 vs. 15.7 ± 4.8; P = 0.006), number of long refluxes (1.1 ± 0.4 vs. 0.3 ± 0.2; P = 0.047), duration of longest reflux (6.6 ± 1.3 vs. 3.3 ± 1.3; P = 0.005) and percentage of time pH remained below 4 (15.3 ± 3.1 vs. 4.7 ± 1.8; P = 0.001) in the 3-h monitoring period, compared with volunteers. At baseline, there was no significant difference between symptoms of patients and volunteers. At 15-min post-ingestion of curry, patients experienced significantly more heartburn (1.3 ± 0.4 vs. 0.2 ± 0.1; P = 0.014) than volunteers. At all time points that followed, patients experienced significantly more fullness, bloating, discomfort, pain, nausea, and heartburn than healthy volunteers. The mean total symptom scores were significantly higher in patients than volunteers 30, 60, 90, 120, 150, and 180 min after ingesting curry but symptoms peaked at the same time (15-min) in both patients and volunteers (Fig. 1).
Difference in Responses Between Curry and Water Ingestion Among Volunteers
For the 11 volunteers who were tested for both curry (800 ml) and water (800 ml) ingestion, the mean (±SE) percentage of time esophageal pH remained below 4 was significantly higher after ingesting curry (7.2 ± 2.9 vs. 1.2 ± 0.42 for water; P = 0.044). The mean total symptom score was significantly higher 30 min after ingesting curry compared with water ingestion (6.6 vs. 0.3 for water, P = 0.028).
Discussion
Our study showed that in healthy volunteers, curry ingestion induced significantly more esophageal acid exposure than did ingestion of a similar volume of water, suggesting that the curry and not the volume worsened gastroesophageal reflux. We also showed that curry resulted in significantly higher esophageal acid exposure in patients with a history of GERD than in healthy volunteers. Upper abdominal symptoms post-curry ingestion were also more severe and persisted longer in patients than in volunteers, with symptoms peaking in 15 min and returning to baseline only after 3 h. These results suggest that curry is a powerful aggravator of gastroesophageal reflux, particularly among patients with a history of gastroesophageal reflux. We monitored for a total of 180 min after curry ingestion to enable observation of the trend over time.
Chilli, a constituent spice in curry has been shown to induce increased gastroesophageal reflux [7]. The exact mechanism by which curry induces reflux is still unknown, but the caloric content of curry could partly explain induction of reflux. Although highly specific and sensitive for the diagnosis of GERD, the 24-h pH monitoring is limited in its applications because of the dynamic nature of the disease. Studies have shown that its results are normal in 25% of patients with erosive esophagitis and in approximately 33% of patients with NERD [8]. Patients who report reflux symptoms may thus not test positive during pH monitoring. It seems likely that such patients might test positive during pH monitoring if stressed with factors such as curry. Patients with a definite history of heartburn, who tested negative during 24-h pH monitoring, could be subjected to the curry stress test. With this approach, those patients who, on the basis of 24-h pH monitoring, would otherwise be mislabeled as having functional heartburn could be correctly diagnosed.
It will be interesting to study the effects on symptom relief and improvement in esophageal pH for patients with GERD after abstinence from spicy food. However, before such results become available, patients with GERD should be informed that curry ingestion worsens symptoms and acid reflux in GERD. Therefore, curry ingestion should be avoided in GERD.
Conclusion
Curry induced more reflux and caused more severe symptoms in patients with GERD than in healthy individuals. Patients suffering from GERD and who have symptoms aggravated by curry ingestion should be advised to avoid curry.
References
Kang JY, Tay HH, Guan R. Chronic upper abdominal pain: site and radiation in various structural and functional disorders and the effect of various foods. Gut. 1992;33:743–748.
Yeoh KG, Ho KY, Guan R, Kang JY. How does chili cause upper gastrointestinal symptoms? A correlation study with esophageal mucosal sensitivity and esophageal motility. J Clin Gastroenterol. 1995;21:87–90.
Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med. 2006;166:965–971.
Lim LG, Ho KY. Gastroesophageal reflux disease at the turn of the millennium. World J Gastroenterol. 2003;9:2135–2136.
Ho KY, Kang JY, Seow A. Prevalence of gastrointestinal symptoms in a multiracial Asian population, with particular reference to reflux-type symptoms. Am J Gastroenterol. 1998;93:1816–1822.
Ho KY, Kang JY. Prolonged ambulatory oesophageal pH and pressure recording in healthy adults in Singapore. Singapore Med J. 1998;39:295–299.
Milke P, Diaz A, Valdovinos MA, Moran S. Gastroesophageal reflux in healthy subjects induced by two different species of chilli (Capsicum annum). Dig Dis. 2006;24:184–188.
Ho KY, Kang JY. Esophageal mucosal acid sensitivity can coexist with normal pH recording in healthy adult volunteers. J Gastroenterol. 2000;35:261–264.
Acknowledgments
We wish to thank Dr Jennie Wong for her editorial assistance.
Conflict of interest
The authors declare no competing interest. This study was not funded by any grant.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lim, L.G., Tay, H. & Ho, K.Y. Curry Induces Acid Reflux and Symptoms in Gastroesophageal Reflux Disease. Dig Dis Sci 56, 3546–3550 (2011). https://doi.org/10.1007/s10620-011-1799-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1799-3