
Abstract
Background
Small intestinal bacterial overgrowth (SIBO) has been observed in several disorders of the gastrointestinal tract. Studies have shown abnormalities of motor function in obese patients, and there is indirect evidence suggesting that SIBO is present in them.
Aims
To study small intestinal motility and the prevalence of SIBO in obese patients and to determine whether there was any relationship between both parameters.
Methods
Thirty-nine patients scheduled for bariatric surgery were subjected to hydrogen breath test with lactulose and to a stationary small intestinal motility study with perfused catheters.
Results
SIBO was observed in 41% of obese patients and was not related to body mass index. Small intestinal manometry showed a marked increase of clustered contractions in obese patients with SIBO compared to obese subjects without SIBO, whereas all the other parameters of fasting cyclic activity were not different.
Conclusions
SIBO was a frequent finding in obese patients and was associated with an increased pattern of clustered contractions, which was not observed in absence of SIBO.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Small intestinal bacterial overgrowth (SIBO) is defined as the presence of an abnormal number of bacteria in the small intestine. It has been associated with anatomical abnormalities of the small bowel, such as blind loops and diverticula [1–3]. SIBO has also been a frequent finding being associated with alterations in fasting small intestinal motor activity [4–6] and other pathological conditions such as advanced chronic liver disease [7, 8].
In the past, the development of SIBO was commonly observed in obese patients after jejune-ileal bypass operations for morbid obesity [9, 10]. The spontaneous appearance of SIBO in obese female patients was suggested by observation of an increased endogenous production of ethanol. Since the most probable source of ethanol was bacterial fermentation, this provides indirect evidence of the presence of SIBO [11]. However, SIBO was not directly investigated in that study. The finding of endogenous ethanol production was also observed in the obese ob/ob mice model and was decreased by treatment with neomycin [12].
Since an abnormal profile of peptides with potential effects on gastrointestinal motility, such as leptin [13] and ghrelin [14, 15] has been observed in obese patients, changes of motor activity have been investigated in this condition. Several studies have been performed in order to establish the presence of functional abnormalities of the gastrointestinal tract in obese patients [16]. Most of these studies have been focused on the motor function of the stomach [17, 18].
Very few studies have addressed small intestinal motor function abnormalities in obese patients. In one study, an increase in orocecal transit time (OCTT) was found [19], however this observation was not confirmed by subsequent studies [20, 21].
Pieramico et al. [22] studied small intestinal motility in 14 severely obese patients: while the intestinal migrating motor complex (MMC) was essentially normal, the gastric component of phase III of the MMC occurred less frequently than in a control group.
Therefore, according to the indirect evidence discussed previously, the possibility to find a higher incidence of SIBO in obese patients exists. Also, since the unique study of small intestinal motility in obese patients was performed in a small number of patients, disorders of motility might be observed in a greater series of patients.
The aims of the present study were firstly, to determine the prevalence of SIBO in a group of obese patients before bariatric surgery. Secondly, to assess their OCTT and thirdly, to study in this group of patients the relationship between the presence of SIBO and small intestinal motility.
Methods
Thirty-nine patients entered the study, and their average age was 37.5 years (range 25–61 years); 35 were female. Body mass index (BMI) was 44.9 ± 7 kg/m2; all were scheduled for bariatric surgery. All obese patients were submitted to a lactulose hydrogen breath test and a stationary study of small intestinal motility. All subjects signed an informed consent. This study was approved by the Ethical Committee of the University Hospital of the University of Chile.
Lactulose Hydrogen Breath Test
SIBO and OCTT were investigated by means of the H2 breath test with lactulose. The test was performed after a 12-h fasting; subjects consumed a low carbohydrate diet on the day before.
After a mouthwash with 1% hexetidine (Duranil®, Warner-Lambert Company), basal values of H2 concentration were measured. After the administration of 25 ml of 66.7% lactulose (Duphalac® Grünenthal Lab. Santiago, Chile) dissolved in 200 ml of distilled water, H2 concentration (expressed as parts per million (PPM) in end-expiratory air) was measured by means of an automatic analyzer (Quintron MicroLyzer Model CM2, Milwaukee, Wisconsin, USA). The following criteria was used to define the presence of SIBO: an increase over basal values of H2 concentration of 10 PPM or more during the first 60 min, with an associated second peak caused by colonic fermentation of lactulose. Orocecal transit time expressed in minutes was defined as the time elapsed between lactulose ingestion and the initiation of a sustained increase in H2 concentration. In the presence of SIBO, we used the time from the onset of the second H2 concentration peak, corresponding to colonic fermentation of lactulose.
Small Intestinal Motility
Duodenal motor activity was studied by means of a multi-lumen, perfused catheter assembly, which incorporated four polyvinyl tubes (internal diameter, 0.9 mm) glued together with tetrahydrofuran and with side holes spaced 3 cm apart. They were continuously infused with bubble-free distilled water by a pneumo-hydraulic capillary infusion system (Arndorfer Medical Specialities, Greendale, Wisconsin, USA) at a rate of 0.4 ml/min. The manometric catheters were attached to external TP-400t pressure transducers and connected to a Nihon Kohden polygraph (Nihon Kohden, Tokyo, Japan).
The outputs of the amplifiers were, in turn, connected to an analog–digital converter in a personal computer, and signals were analyzed by a computer program developed in our laboratory.
After an overnight fast, the catheter assembly was passed into the mouth to the stomach and was placed under fluoroscopic control until the tip of the assembly had reached the angle of Treitz, therefore, the recording sites were located in the third and fourth part of the duodenum. Studies were performed in the fasting state only.
Analysis of Motor Activity
The different phases of the MMC and clustered contractions were identified by direct visual inspection of the chart-recording paper using the following criteria: phase I was characterized by the complete absence of contractions; phase II consisted of irregular phasic contractions, which culminated in a burst of rhythmic phasic contractions at a frequency of 12 cpm (phase III). To define MMC activity, the presence of at least one phase III, preceded by phase II and followed by phase I, was required. Clustered contractions were defined as a sequence of three to ten rhythmic contractions, preceded and followed by a quiescent period of 1–5 min in duration (Fig. 1).

Clusters of contractions followed by phase III of the MMC, defined as a sequence of three to ten rhythmic contractions, preceded and followed by a quiescent period of 1–5 min in duration
The frequency and amplitude of contractions were calculated by means of the computer program.
Statistical Analysis
Comparison within obese patients with and without SIBO for age, BMI, OCTT, and motility parameters were made using Student’s t test for un-paired observations.
The presence of cyclic activity of the MMC in both groups was compared using Fisher’s exact test and the two sample proportion tests for the percentage of the MMC of the total recording time occupied by phase II. All results are expressed as the mean ± standard error (SE) and a p value of <0.05 was considered to be statistically significant.
Results
Lactulose H2 Breath Test
SIBO was observed in 16 obese patients. This group of patients had a significant lower mean age compared to the group in which SIBO was not present. No differences in BMI were observed between obese subjects with SIBO and obese subjects with a normal H2 breath test (Table 1).
Fifteen patients were asymptomatic; occurrence of symptoms possibly associated to SIBO is shown in Table 1. None of the patients had diabetes or liver cirrhosis. Elevated transaminase levels were observed in seven patients, six of them without SIBO. Liver biopsy was performed in 26 patients, their findings are shown in Table 2.
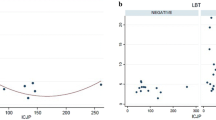
Among the obese subjects, no differences were observed in OCTT between subjects with (109 ± 16 min) and without SIBO (108 ± 22 min) (p = 0.4).
Small Intestinal Motility
The duration of the manometric recordings was not different between obese patients with or without SIBO (Table 3). Cyclic activity of the MMC was present in all obese subjects without SIBO, but was absent in two obese patients with SIBO. The MMC cycles and phase I durations were not different comparing both groups (Table 3). Manometric characteristics of phase II are shown (Table 4): several parameters, such as duration, the percentage of the MMC cycle of the total recording time occupied by phase II, or the amplitude or frequency of contractions during phase II were no different in obese patients, with or without SIBO. In contrast, a marked increase in the occurrence of clustered contractions (p < 0.001) was observed in all obese patients with SIBO (including those with or without cyclic activity) compared to obese subjects without SIBO. The absolute and relative number of phase III duration and the amplitude of contractions were not different between both groups (Table 5).
Discussion
In the present study we have observed 41% of prevalence of SIBO in obese patients. While parameters of small intestinal fasting cyclic motility were not essentially different comparing normal obese subjects to those with an abnormal lactulose breath test. A marked increase in the occurrence of clustered contractions among obese patients with SIBO was observed.
The presence of SIBO has been defined by different methods, such as the direct culture of jejunal aspirates, currently considered the gold standard, or by indirect tests such as H2 breath test using glucose or lactulose as substrate. The relative accuracy of these tests remains controversial, as being the optimal criteria for the diagnosis of SIBO based on the pattern of breath hydrogen excretion [23]. Because of its relatively non-invasive nature, we chose to use the lactulose breath hydrogen test and diagnostic criteria that have been extensively used by others.
The reason why some obese patients may develop SIBO is unclear, but does not appear to be related to a more advanced age; in fact, obese subjects with SIBO were on average, younger than those who did not have SIBO. Also, the presence of SIBO was independent of gender and OCTT. An underlying motor abnormality seems to be a more likely explanation given the prominence of clustered contractions among obese subjects with SIBO and the absence of fasting cyclic activity in two patients with SIBO. In all the other obese subjects, the duration of cyclic activity and the manometric characteristics of the different phases were not different. Our results are in accordance with a previous study [22] in obese patients, in which the duration of the intestinal MMC and their respective phases were normal. The same authors observed, however, that the gastric component of phase III and plasma motilin levels were decreased in obese subjects. These parameters were not studied here.
The small intestinal motor response to food ingestion was not investigated in this study; however, it is unlikely, given our understanding of relationships between motor patterns and SIBO, that any post-prandial alteration in motor activity might contribute significantly to the development of SIBO as an isolated disorder.
Another factor not investigated in our study was gastric emptying. Several studies have reported an accelerated rate of gastric emptying of solids in obese subjects [17, 18]. It is possible to speculate that the rapid delivery of an excessive amount of food to the duodenum could serve as a substrate for bacteria.
Clustered contractions (CC) represent a motor pattern described in several pathological conditions, such as partial small intestinal obstruction and pseudo-intestinal obstruction [24], and it has also been described in liver cirrhosis [7, 8]. It is interesting to note that SIBO has also been observed in all of the previously mentioned disorders. This motor disorder has been recorded, as in the present series in presence of cyclic activity of the MMC, or in association with a complete suppression of normal fasting activity of the small bowel, as has been observed in advanced stages of liver cirrhosis [8]. In this last condition, prolonged administration of either prokinetics, antibiotics, or orthotopic liver transplantation [25, 26], has resulted in motility improvement, including the reappearance of cyclic activity of the MMC and the suppression of CC activity. These changes in small intestinal motility were also coincident with an improvement in the lactulose H2 breath test. If CC is associated with an impairment of small bowel, propulsive motility is unclear.
An alternative and possible conclusion of the present study is, of course, that an increased density of bacteria in the upper small intestine may result in (rather than be a consequence of) the altered motility pattern characterized by an increase in CC activity.
Irritable bowel syndrome is a common disorder in which dysmotility of the small intestine and SIBO have both been implicated. Earlier manometric observations [27] revealed an increase in CC activity in these patients; on the other hand, Pimentel et al. [28, 29] have reported SIBO in 78–84% of patients with IBS. However, this finding has not been confirmed by other studies, and this observation is a matter of controversy. In a recent study [30] with a large number of IBS patients, SIBO established by culture of jejunal aspirate was only observed in 4% of patients. Dysmotility was recorded in the presence of SIBO but CC was not increased.
The appearance of CC in the presence of SIBO could, alternatively, be the result of the overgrowth of some specific strains of bacteria or perhaps of the presence of some additional factors such as liver disease; it was not possible to establish the relevance of these and other factors in this study.
Another interesting and potentially related observation is that ethanol has been shown to induce a pattern of predominant CC’s in normal volunteers [31]. Enhanced endogenous ethanol production has been documented in obese patients [11] and it might explain the appearance of CC.
The relationship between SIBO and fatty liver disease may be speculated by pulling together findings of two published papers. The first describes an experimental model of NAFLD in the ob/ob mice in which SIBO and over-expression of TNF-α were both reported in the obese animals. Treatment with a probiotic cocktail reduced total fat content of the liver, lowered transaminase levels, and improved liver histology [32]. The second study compared germ-free animals with conventionally raised (gut colonized by bacteria) mice [33]. While the conventionally raised mice consumed 29% less chow, these animals contained 42% more body fat than the germ-free animals. When gut bacteria were introduced to germ-free mice, there was a 57% increase in total body fat content. This increase in body fat was accompanied by a rise of fasting glucose and insulin levels, 2.3-fold increase in total liver triglycerides, and increased expression of two enzymes involved in hepatic synthesis of fatty acids: acetyl-CoA carboxylase (Acc1) and fatty acid synthase (Fas).
In conclusion, using the lactulose H2 breath test with restricted diagnostic criteria (60 min and a double peak), the finding of SIBO in asymptomatic population has been estimated in 20% by other studies [34], therefore it seems that SIBO was more frequent in obese patients. However, the absence of a control group of normal subjects with similar age and female/male ratio with LBT and recording of small intestinal motility, our results must be analyzed with caution. Also, the relative small number of patients with SIBO might explain why we have failed to identify risk factors for the presence of SIBO in this patient population. The most striking motility pattern associated with SIBO among obese subjects may be a consequence of SIBO. The possible role of other factors in the development of this altered motility and SIBO deserves additional investigation.
References
Bishop R, Anderson CM. The bacterial flora of the stomach and small intestine in children with intestinal obstruction. Arch Dis Child. 1960;35:487–491.
Di Stefano M, Miceli E, Missanelli A, Mazzocchi S, Corazza GR. Absorbable vs. non-absorbable antibiotics in the treatment of small intestine bacterial overgrowth in patients with blind-loop syndrome. Aliment Pharmacol Ther. 2005;21:985–992.
Skar V, Skar AG, Osnes M. The duodenal bacterial flora in the region of papilla of Vater in patients with and without duodenal diverticula. Scand J Gastroenterol. 1989;24:649–656.
Vantrappen C, Janssens J, Hellemans J, Ghoos Y. The interdigestive motor complex of normal subjects and patients with bacterial overgrowth of the small intestine. Interdigestive motor complex and small intestinal bacterial overgrowth. J Clin Invest. 1997;59:1158–1166.
Stotzer PO, Björnsson ES, Abrahamsson H. Interdigestive and postprandial motility in small intestinal bacterial overgrowth. Scand J Gastroenterol. 1996;31:875–880.
Vincent B, Nieuwenhuijs MD, Verheem A, et al. The role of interdigestive small bowel motility in the regulation of gut microflora, bacterial overgrowth, and bacterial translocation in rats. Ann Surg. 1998;228:188–193.
Chesta J, Defilippi Cl, Defilippi C. Abnormalities in proximal small bowel motility in patients with cirrhosis. Hepatology. 1993;17:828–832.
Madrid AM, Cumsille F, Defilippi C. Altered small bowel motility in patients with liver cirrhosis depends on severity of liver disease. Dig Dis Sci. 1997;42:738–742.
Paerregaard A, Justesen T, Prytz H, Anderson B, Gudmand-Höyer E. Metronidazole treatment of bypass-enteropathy after jejunoileal shunt-operation for obesity. Acta Chir Scand. 1982;148:153–156.
Passaro E Jr, Drenick E, Wilson SE. Bypass enteritis. A new complication of jejunoileal bypass for obesity. Am J Surg. 1976;131:169–174.
Nair S, Cope K, Terence RH, Mae A. Obesity and female gender increase breath ethanol concentration: potential implications for the pathogenesis of nonalcoholic steatohepatitis. Am J Gastroenterol. 2001;96:1200–1204.
Cope K, Risby T, Diehl AM. Increased gastrointestinal ethanol production in obese mice: implications for fatty liver disease pathogenesis. Gastroenterology. 2000;119:1340–1347.
Konturek PC, Konturek JW, Czesnikiewicz-Guzik M, Brzozowski T, Sito E, Konturek SJ. Neuro-hormonal control of food intake; basic mechanisms and clinical implications. J Physiol Pharmacol. 2005;56:5–25.
Tack J, Depoortere I, Bisschops R, et al. Influence of ghrelin on interdigestive gastrointestinal motility in humans. Gut. 2006;55:327–333.
Suematsu M, Katsuki A, Sumida Y, et al. Decreased circulating levels of active ghrelin are associated with increased oxidative stress in obese subjects. Eur J Endocrinol. 2005;153:403–407.
Xing J, Chen JDZ. Alterations of gastrointestinal motility in obesity. Obes Res. 2004;12:1723–1732.
Tosetti C, Corinaldesi R, Stanghellini V, et al. Gastric emptying of solids in morbid obesity. Int J Obes Relat Metab Disord. 1996;20:200–205.
McCallum RW, Jones TF, Lin Z, Sarosiek I, Moncure M. Assessment of gastric emptying, myoelectric activity in the morbidly obese patient. Gastroenterology. 2001;120:A-290.
Basilisco G, Camboni G, Bozzani A, Vita P, Doldi S, Bianchi PA. Orocecal transit delay in obese patients. Dig Dis Sci. 1989;34:509–512.
Wisen O, Johansson C. Gastrointestinal function in obesity: motility, secretion, and absorption following a liquid test meal. Metabolism. 1992;41:390–395.
French SJ, Murray B, Rumsey RD, Sepple CP, Read NW. Preliminary studies on the gastrointestinal responses to fatty meals in obese people. Int J Obes Relat Metab Disord. 1993;17:295–300.
Pieramico O, Malfertheiner P, Nelson DK, Glasbrenner B, Ditschuneit H. Interdigestive gastroduodenal motility and cycling of putative regulatory hormones in severe obesity. Scand J Gastroenterol. 1992;27:538–544.
Simrén M, Stotzer P-O. Use and abuse of hydrogen breath test. Gut. 2006;55:291–303.
Summers RW, Anuras S, Green J. Jejunal manometry patterns in health, partial intestinal obstruction, and pseudoobstruction. Gastroenterology. 1983;85:1290–1300.
Madrid AM, Hurtado C, Venegas M, Cumsille F, Defilippi C. Long-term treatment with cisapride and antibiotics in liver cirrhosis: effect on small intestinal motility, bacterial overgrowth, and liver function. Am J Gastroenterol. 2001;96:1251–1255.
Madrid AM, Brahm J, Buckel E, Silva G, Defilippi C. Orthotopic liver transplantation improves small bowel motility disorders in cirrhotic patients. Am J Gastroenterol. 1997;92:1044–1045.
Kellow JE, Phillips SF. Altered small bowel motility in irritable bowel syndrome is correlated with symptoms. Gastroenterology. 1987;92:1885–1893.
Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal overgrowth reduces symptoms of irritable bowel syndrome. Am J Gastroenterol. 2000;95:3503–3506.
Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates with symptom improvement in irritable bowel syndrome, a double-blind, randomized, placebo-controlled study. Am J Gastroenterol. 2003;98:412–419.
Posserud I, Stotzer P-O, Björnosson ES, Abrahamsson H, Simrén M. Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gut. 2007;56:802–808.
Schmidt T, Eberle R, Pfeiffer A, Kaess H. Effect of ethanol on postprandial duodenojejunal motility in humans. Dig Dis Sci. 1997;42:1628–1633.
Bäckhned F, Ding H, Wang T, et al. The gut microbiota as an environmental factor that regulates fat storage. PNAS. 2004;101:15718–15723.
Bäckhned F, Manchester JK, Semenkovich CF, Gordon JI. Mechanisms underlying the resistance to diet-induced obesity in germ-free mice. PNAS. 2007;104:979–984.
Vanner S. The small intestinal bacterial overgrowth. Irritable bowel syndrome hypothesis: implications for treatment. Gut. 2008;57:1315–1321.
Acknowledgments
The authors are grateful to Dr. Eamonn M. Quigley, for his careful review of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Madrid, A.M., Poniachik, J., Quera, R. et al. Small Intestinal Clustered Contractions and Bacterial Overgrowth: A Frequent Finding in Obese Patients. Dig Dis Sci 56, 155–160 (2011). https://doi.org/10.1007/s10620-010-1239-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1239-9