
Abstract
We sought to assess the significance of an incidental finding of colorectal wall thickening (CRWT) on computed tomography (CT) scan in African-American and Hispanic patients. We retrospectively reviewed charts of African-American and Hispanic patients from January 1994 to December 2005. Those patients were included in whom the colonoscopy was performed due to incidental CRWT on CT scan. Patients with a history or a family history of colorectal malignancy, inflammatory bowel disease, or colorectal surgery, with an incomplete colonoscopic examination, or <18 years of age were excluded. Endoscopic and pathological findings were abstracted. Thirty-two patients met the criteria. Endoscopic examination was abnormal in 21 (65.6%). The positive predictive value of CRWT for abnormal endoscopic examination was 65.6%. Abnormal endoscopic examination revealed diverticulosis in 9 (43%), erythematous mucosa in 8 (38%), polyps in 6 (29%), mass in 2 (9%), thickened folds in 1 (5%), and diverticulitis in 1 (5%). Histopathological findings revealed colitis in 7 (33%), adenoma in 4 (19%), hyperplastic polyps in 4 (19%), adenocarcinoma in 2 (9%), lymphoid aggregates in 2 (9%), melanosis coli in 1 (5%), and normal in 1 (5%) in the abnormal examination group. Abnormal endoscopic examination was found in 65.6% of patients. The prevalence of colitis, adenomas, and malignancy was high, therefore abnormal CRWT warrants further endoscopic evaluation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Computed tomography (CT) scanning is a frequently used modality in diagnostic investigation for numerous clinical problems. Colorectal wall thickening (CRWT) on CT scan of the abdomen and pelvis is a familiar finding. This finding may be due to inflammatory bowel disease, neoplasia, ischemia, celiac disease, or edema [1–6]. CRWT may be a sign of early pathological changes of an unidentified disease. This finding may also be due to inadequate distention of the colon and rectum or thick tenacious material adherent to the wall, or it may be a mere artifact. CT scan has limited ability to differentiate between pathological and nonpathological findings. There are no existing guidelines about the management of patients with incidental CRWT on CT scan. The findings were considered to be incidental if the patients did not have any known gastrointestinal (GI) disease and they underwent CT scan examination for a non-GI-related problem or if they had a known GI disease but the CRWT finding was not directly related to their disease.
CRWT on CT scan can be due to changes in the luminal, intramural, or extramural portions of the wall. Most pathological changes in the colon and rectum also cause mucosal surface abnormality. Luminal examination of the colon and rectum offers the opportunity to detect such abnormalities. Although virtual colonoscopy has a higher sensitivity and specificity than CT scan, endoscopic examination provides a direct view of the luminal mucosa and the opportunity to perform biopsies or other needed interventions simultaneously [7].
Previous studies have shown that CRWT on CT scan warrants colonoscopic examination, but data in African-American and Hispanic patients is lacking [8–10]. The incidence and prevalence of inflammatory bowel disease, celiac disease, and colorectal cancer are different in African-American and Hispanic patients compared to Caucasians [11–14]. Furthermore, there are racial differences in family history, disease location, and extraintestinal manifestations in African-American and Hispanic patients with inflammatory bowel disease [15]. Even colorectal cancer is diagnosed at advanced stages (TNM Stage III or IV) in this minority population compared to Caucasians [16]. Incidental CRWT on CT scan can be an early sign of an undiagnosed disease in this minority population. Early diagnosis of the disease will help to decrease the morbidity and mortality and hence will improve the outcome in African-American and Hispanic patients.
In our clinical experience, we have repeatedly seen the incidental finding of CRWT in patients who undergo CT scan. To our knowledge, there is no published report describing the frequency and clinical significance of incidental CRWT on CT scan in African-American and Hispanic patients. Therefore, we did this study to evaluate the clinical significance of the incidental finding of CRWT on CT scan in African-American and Hispanic patients. The finding of CRWT was correlated with colonoscopic and histopathological findings.
Methods
We performed a retrospective review of the medical charts of patients seen at our inner-city hospital who underwent colonoscopic examination only due to the finding of CRWT on CT scan. These patients were selected from the procedure logbook and computerized procedure notes of the Division of Gastroenterology. The available data from January 1994 to December 2005 were reviewed. This was followed by a detailed review of the medical charts of these patients. In our study, the colorectal wall was considered thickened when it measured more than 3 mm in the colon and 5 mm in the rectum on CT scan [17]. The finding of CRWT was confirmed by a certified staff radiologist. CT scan examinations were performed on a Picker PQ 6000 scanner. All CT scans were performed with intravenous and oral contrasts. Gastrograffin (Bracco Diagnostics, Princeton, NJ) was used for oral contrast and Omnipaque 300 (Amersham Health, Princeton, NJ) or Visipaque 320 (Amersham Health) was used for intravenous contrast, depending on the renal function. Abdominal images were obtained at 8-mm increments. Most of the colonoscopies were performed with direct-view Olympus colonoscopes (CF-Q160 AL; Olympus Optical Co, Ltd., Tokyo). A few colonoscopies were performed with direct-view Pentax colonoscopes (EC-3872 K; Habashi-Ku, Tokyo).
Patients who had a colonoscopic exam after good or fair bowel preparation and were older than 18 years of age were included in the study. One gallon of Golytely (Braintree Laboratories Inc., Braintree, MA) was utilized for all patients for bowel preparation for colonoscopy. Patients were excluded from the study for the following reasons: any history of known inflammatory bowel disease, surgery of the colon or rectum, not being African American or Hispanic, a positive family history for colon cancer, and incomplete colonoscopic examination. Since the finding of colonic wall thickening is known in patients with liver cirrhosis, these patients were excluded from the study [3, 18]. Data regarding age, gender, ethnicity, family history of colon cancer, indication for colonoscopy, CT findings, and histopathology (if available) were abstracted. Biopsies were performed on all patients with abnormal colonoscopic examination. The Institutional Review Board of the university approved the study.
Statistical analysis
The data were analyzed by independent sample t test and Fisher's exact test. For all tests, a two-sided P value <0.025 was considered statistically significant. The analysis was performed on SPSS software v. 13.3 (SPSS Inc., Chicago, IL).
Results
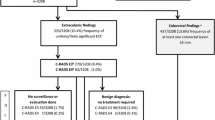
We found 37 patients in whom colonoscopy was performed due to the incidental finding of CRWT on CT scan. Three patients with an incomplete colonoscopic examination and two non-Hispanics and non-African-Americans were excluded from the study. The 32 patients who met the criteria for the study were analyzed. The mean age of the patients was 48.3 ± 9.7 years (range, 32–70 years). The majority of the patients were Hispanics (59.4%). We found the same proportion for females (59.4%). All of the patients denied any family history of colon cancer, except one who gave a history of unidentified cancer in father diagnosed at an unknown age.
Colonoscopic examination was abnormal in 21 (65.6%) and normal in 11 (34.4%) of the patients. Hence, the positive predictive value of CRWT on CT scan for an abnormal colonoscopic examination was 65.6% (Table 1). The mean age of the patients in the group with an abnormal examination was higher (50.1 ± 9.9 years) than that of the group with a normal examination (44.9 ± 8.7 years), but this was not statistically significant (two-sided P = 0.15). The number of Hispanic patients was higher in the abnormal colonoscopic examination group compared to the normal one (Hispanics, 14 vs 5; African Americans, 7 vs 6). Hispanic patients had 2.4 times higher odds for the presence of an abnormal colonoscopic examination, but this was not statistically significant (95% CI, 0.43–14.08; two-sided P = 0.28) (Fig. 1). We also found that colonoscopic examination was abnormal more often in females compared to males (females, 15 vs 4; males, 6 vs 7). Odds of abnormal colonoscopic examination were 4.38 times higher in females compared to males, but the difference was not statistically significant (95% CI, 0.74–28.34; two-sided P = 0.07) (Fig. 2).

Histogram showing the colonoscopy examinations in African-American and Hispanic patients. *NS=Non-significant
The indication for CT scan in the majority of the patients was nonspecific abdominal pain. The abdominal pain was described as vague and nonlocalized in most of the patients. In a few patients the pain was referred to the lower abdomen. A few patients underwent CT scan examination for flank pain, anemia of unknown etiology, and hematuria.
The abnormal colonoscopic examinations revealed diverticuli (43%; N = 9) and erythematous mucosa (38%; N = 8) in the majority of the cases. The prevalence of polyps (29%; N = 6) and mass (9%; N = 2) was high and striking. The prevalence of diverticulitis and thickened folds was low (5%; N = 1) (Fig. 3). In our study biopsies were performed only in patients with an abnormal colonoscopic examination. In this group, the histopathological findings were significant in 20 (95%) cases. The prevalence of colitis (33%; N = 7), tubular adenoma (19%; N = 4), and hyperplastic polyps (19%; N = 4) was very high. Interestingly, two patients (9%) were diagnosed with adenocarcinoma of the colon. The histology was consistent with poorly differentiated adenocarcinoma, and both of them were females. One patient underwent colonic resection, but the second patient refused any surgery. The cancer was found to invade through the muscular propria up to the subserosal fat, but there was no evidence of lymph node involvement (TNM Stage T3 N0 M0). In a few patients the biopsies were positive only for lymphoid aggregate (9%; N = 2) and melanosis coli (5%; N = 1). In only one patient (5%) with an abnormal colonoscopic examination did the histology reveal normal colonic mucosa (Fig. 4). Therefore, 95% of the biopsies done in patients with an abnormal colonoscopic examination were positive for significant pathology. The summation of the colonoscopic and histopathological findings is >100%, because a few patients had more than one abnormal finding.

Histogram showing the colonoscopy findings in males and females. *NS=Non-significant

Colonoscopy findings in patients with an abnormal examination

Histopathological findings in patients with an abnormal colonoscopic examination
Discussion
CRWT is a nonspecific CT scan finding. It is measured as the distance from the outer colorectal wall edge, which is defined by identification of the mesenteric fat-bowel wall interface, to the inner bowel wall edge, as demarcated by noting the interface between the bowel wall and intestinal feces, gas, or diluted contrast material [17, 19]. CRWT may be an early pathological finding in the colorectal wall. This may be due to high expression of interleukin-1β and nitric oxide in colonic tissue as demonstrated by previous studies done in the presence of colitis [20, 21]. CRWT may occur at a stage where the disease, if diagnosed early, may be curable. This will help to reduce the morbidity and mortality related to the disease and hence will improve the outcome.
The sensitivity of abdominal CT scan for detecting bowel wall thickening has increased and previous studies have shown a 69% correlation between bowel wall thickening on CT scan and colonoscopic findings [10]. The CT scan finding of CRWT is a clinically significant finding, which correlates highly with abnormal endoscopic examination. Our study demonstrated that the positive predictive value of CRWT on CT scan for abnormal colonoscopic examination is 65.6% in African-American and Hispanic patients. We found higher number of females and Hispanics showing an abnormal colonoscopic examination, although the results were not statistically significant due to the small sample size.
Although the majority of the findings in abnormal colonoscopic examinations were benign, a significant proportion of the population had tubular adenoma, colitis, and colon cancer. Colorectal cancer is found to be more aggressive and less responsive to therapeutic interventions in African-American and Hispanic patients [22, 23]. Interestingly, the colon cancer diagnosed in two patients was poorly differentiated. Both of these patients were above the recommended age for colorectal cancer screening. This reflects the general practice in the community, where a significant proportion of the eligible African-American and Hispanic patients do not undergo screening examination for colorectal cancer or are not referred to gastroenterologists at the appropriate age [24–26]. This finding reemphasizes the significance of performing screening colonoscopy at the recommended age in African-American and Hispanic patients.
A retrospective study done by Cai et al. showed that 96% (N = 23) of patients with the incidental finding of thickening of the sigmoid or rectum and 13% (N = 2) of patients with cecum wall thickening had significant abnormalities on further evaluation [9]. Another prospective study, performed by Rockey et al., showed the likelihood of finding endoscopic abnormalities in 66% (N = 22) of patients with colonic wall thickening, but their sample included a significant number of patients with human immunodeficiency virus (HIV) [10]. In this study, due to the inclusion of HIV patients, a significant number of them were diagnosed with cytomegalovirus infection, lymphoma, or granuloma. We found a similar positive predictive value (65.6%) of CRWT for abnormal colon examination, despite the absence of HIV patients in our population. This may be due to the different prevalence of inflammatory bowel disease, colorectal cancer, and diverticulosis in African-American and Hispanic patients [15, 22, 27]. The retrospective study done by Zeddun et al., presented at Digestive Disease Week in 2005, demonstrated significant findings in 59% (N = 22) of patients with ileocolonic wall thickening on CT scan. The prevalence of colitis was 43% (N = 16) in their studied patients [28]. We found a lower prevalence of colitis in our population, but this may be due to the analysis of patients with only CRWT, and not with ileal wall thickening.
Although inflammatory and neoplastic diseases involving intra- and extramural portions of the colonic wall cause abnormalities on the mucosal surface, this phenomenon may not be present in every case. This may have led to the lower positive predictive value of CRWT on CT scan for abnormal colonoscopic findings. In such cases diagnosis of the real pathology may be missed even with colonoscopic examination. Unfortunately, we did not have biopsies from those patients in whom the colonoscopic examination was found to be normal, despite the presence of CRWT on CT scan. The approach to the patients with incidental CRWT identified on CT scan, but no gross abnormality on endoscopic evaluation, is controversial. The workup of such patients should be custom tailored depending on the clinical condition of the patient. If the pretest probability of finding significant pathology is high, then the CT scan findings should be confirmed by repeated CT scan or air contrast barium enema. In the absence of a higher degree of suspicion for significant pathology, further workup should not be performed.
The majority of the patients had the CT scan investigation due to nonspecific abdominal pain. It is very unusual for a CT scan to be performed on patients who are truly asymptomatic. Therefore, the indications for CT scan mimick the way clinical medicine is practiced in the general population. The indication for CT scan was verified in the medical charts of the patients, but there is still the chance of subjective bias by the patient's examining physician.
Limitations of our study include the patient selection and direct verification bias. Because the patient selection was based on reports in the procedure logbook and computerized notes of the Gastroenterology Department, some patients with the incidental finding of CRWT on CT scan may have been omitted. A few patients who did not have a complete evaluation at our hospital were excluded from the study, which may have affected the results of the study. There were patients who had the incidental finding of CRWT but did not undergo colonoscopic examination due to comorbidities. It would be interesting to know the disease course and the outcomes in this group of patients. Since this was a retrospective study, it was very difficult to obtain such information. The small sample size may have affected the results of the study, along with the failure to show statistical significance. Further studies with larger sample sizes may help to evaluate the role of endoscopic evaluation in such patients.
In conclusion, the incidental finding of CRWT on CT scan had a high correlation with abnormal colonoscopic findings. Although the majority of the findings were benign, the prevalence of tubular adenoma and cancer was high. Patients with such findings warrant further evaluation by endoscopic examination. Further studies with larger sample sizes are needed to prove the cost-effectiveness of colonoscopy in patients with the incidental finding of CRWT on CT scan.
References
Byun JH, Ha HK, Kim AY, Kim TK, Ko EY, Lee JK, Yu ES, Myung SJ, Yang SK, Jung HY, Kim JH (2003) CT findings in peripheral T-cell lymphoma involving the gastrointestinal tract. Radiology 227:59–67
Choi D, Jin Lee S, Ah Cho Y, Lim HK, Hoon Kim S, Jae Lee W, Hoon Lim J, Park H, Rae Lee Y (2003) Bowel wall thickening in patients with Crohn's disease: CT patterns and correlation with inflammatory activity. Clin Radiol 58:68–74
Hwang JC, Ha HK, Yoon KH, Lee M, Kim PN, Lee YS, Chung YH, Jung HY, Suh DJ, Auh YH (1999) Colonic wall thickening in cirrhotic patients: CT features and its clinical significance. Abdom Imaging 24:125–128
Morson BC (1979) Diverticular disease of the colon. Acta Chir Belg 78:369–376
Xiong L, Chintapalli KN, Dodd GD 3rd, Chopra S, Pastrano JA, Hill C, Leyendecker JR, Abbott RM, Grayson D, Feig J (2004) Frequency and CT patterns of bowel wall thickening proximal to cancer of the colon. AJR Am J Roentgenol 182:905–909
Tomei E, Diacinti D, Marini M, Mastropasqua M, Di Tola M, Sabbatella L, Picarelli A (2005) Abdominal CT findings may suggest coeliac disease. Dig Liver Dis 37:402–406
O’Hare A, Fenlon H (2006) Virtual colonoscopy in the detection of colonic polyps and neoplasms. Best Pract Res Clin Gastroenterol 20:79–92
Moraitis D, Singh P, Jayadevan R, Cayten CG (2006) Colonic wall thickening on computed tomography scan and clinical correlation. Does it suggest the presence of an underlying neoplasia? Am Surg 72:269–271
Cai Q, Baumgarten DA, Affronti JP, Waring JP (2003) Incidental findings of thickening luminal gastrointestinal organs on computed tomography: an absolute indication for endoscopy. Am J Gastroenterol 98:1734–1737
Rockey DC, Halvorsen RA Jr Higgins JL, Cello JP (1995) Prospective evaluation of patients with bowel wall thickening. Am J Gastroenterol 90:99–103
Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ (2005) Cancer statistics, 2005. CA Cancer J Clin 55:10–30
Polite BN, Dignam JJ, Olopade OI (2005) Colorectal cancer and race: understanding the differences in outcomes between African Americans and whites. Med Clin North Am 89:771–793
Mostafa G, Matthews BD, Norton HJ, Kercher KW, Sing RF, Heniford BT (2004) Influence of demographics on colorectal cancer. Am Surg 70:259–264
Simsek H, Schuman BM (1989) Inflammatory bowel disease in 64 black patients: analysis of course, complications, and surgery. J Clin Gastroenterol 11:294–298
Nguyen GC, Torres EA, Regueiro M, Bromfield G, Bitton A, Stempak J, Dassopoulos T, Schumm P, Gregory FJ, Griffiths AM, Hanauer SB, Hanson J, Harris ML, Kane SV, Orkwis HK, Lahaie R, Oliva-Hemker M, Pare P, Wild GE, Rioux JD, Yang H, Duerr RH, Cho JH, Steinhart AH, Brant SR, Silverberg MS (2006) Inflammatory bowel disease characteristics among African Americans, Hispanics, and non-Hispanic Whites: characterization of a large North American cohort. Am J Gastroenterol 101:1012–1023
Chien C, Morimoto LM, Tom J, Li CI (2005) Differences in colorectal carcinoma stage and survival by race and ethnicity. Cancer 104:629–639
Fisher JK (1983) Abnormal colonic wall thickening on computed tomography. J Comput Assist Tomogr 7:90–97
Quilez C, Palazon JM, Arenas J, Alonso S, Sanchez J, Belda G, Perez-Mateo M (2003) Colonic wall thickening in patients with cirrhosis and portal hypertension. Rev Esp Enferm Dig 95:269–272, 265–268
Macari M, Balthazar EJ, Megibow AJ (1999) The accordion sign at CT: a nonspecific finding in patients with colonic edema. Radiology 211:743–746
Yamada T, Takahashi S, Masuda K, Ohara H, Nakazawa T, Sano H, Ando T, Nakamura S, Kobayashi S, Kuno A, Aoki S, Nomura T, Joh T, Itoh M (2003) Kupffer-cell depletion attenuates colonic and extracolonic granulomatous inflammation in chronic colitis. J Lab Clin Med 142:268–277
Daddaoua A, Puerta V, Requena P, Martinez-Ferez A, Guadix E, de Medina FS, Zarzuelo A, Suarez MD, Boza JJ, Martinez-Augustin O (2006) Goat milk oligosaccharides are anti-inflammatory in rats with hapten-induced colitis. J Nutr 136:672–676
Stefanidis D, Pollock BH, Miranda J, Wong A, Sharkey FE, Rousseau DL, Thomas CR Jr, Kahlenberg MS (2006) Colorectal cancer in Hispanics: a population at risk for earlier onset, advanced disease, and decreased survival. Am J Clin Oncol 29:123–126
Polite BN, Dignam JJ, Olopade OI (2006) Colorectal cancer model of health disparities: understanding mortality differences in minority populations. J Clin Oncol 24:2179–2187
Ata A, Elzey JD, Insaf TZ, Grau AM, Stain SC, Ahmed NU (2006) Colorectal cancer prevention: adherence patterns and correlates of tests done for screening purposes within United States populations. Cancer Detect Prev 30:134–143
James TM, Greiner KA, Ellerbeck EF, Feng C, Ahluwalia JS (2006) Disparities in colorectal cancer screening: a guideline-based analysis of adherence. Ethn Dis 16:228–233
Pollack LA, Blackman DK, Wilson KM, Seeff LC, Nadel MR (2006) Colorectal cancer test use among Hispanic and non-Hispanic U.S. populations. Prev Chronic Dis 3:A50
Basu D, Lopez I, Kulkarni A, Sellin JH (2005) Impact of race and ethnicity on inflammatory bowel disease. Am J Gastroenterol 100:2254–2261
Zeddun S AM, Nsien E, Ehrlich L (2005) Endoscopic findings in patients with evidence of ileocolonic thickening on computed tomography. Gastroenterology 128:A–405
Acknowledgments
This study was funded by NIH Grant 5R25RR019488-04. Part of this paper was presented at the American College of Gastroenterology Meeting, Las Vegas, Nevada, October 2006. We are thankful to Dr. Yoshikawa and Dr. Anyadike for their valuable suggestions during the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Padda, M., Vadgama, J., Sandhu, P. et al. Clinical Significance of Incidental Colorectal Wall Thickening on Computed Tomography Scan in African-American and Hispanic Patients. Dig Dis Sci 52, 3159–3164 (2007). https://doi.org/10.1007/s10620-006-9639-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-006-9639-6