
Abstract
Hypertension (HT) is a common and life threating health problem worldwide leading to stroke, heart attack and renal failure. It is characterized by elevated blood pressure forced heart load. Human interleukin-6 (IL-6) and C- reactive protein (CRP) are known to be involved in inflammatory processes. IL-6 gene is a polymorphic gene which −174 G/C is a common and −572 G/C is a rare polymorphisms identified in promoter region. Publications on IL-6 gene polymorphisms raised the question whether this gene polymorphisms lead to susceptibility to HT or not. To investigate the effects of IL-6 gene −174 G/C (rs 1800795) and −572 G/C (rs1800796) polymorphisms on plasma IL-6 and CRP levels and their associations with hypertension disease in Turkish population we analyzed −174 G/C and −572 G/C polymorphisms and plasma IL-6 and CRP levels in 111 healthy controls and 108 hypertension patients from Adıyaman, Turkey. We determined the genotypes using polymerase chain reaction-restriction fragment length polymorphism and analyzed plasma levels of IL-6 by ELISA and CRP by automated standard biochemical methods. We have found no statistically significant differences between IL-6 gene −174 G/C and −572 G/C genotypes and allelic frequencies and IL-6 and CRP plasma levels and HT (p > 0.05). No CC genotype was found in control subjects for −572 G/C polymorphism. In conclusion, we found relation to −174 G/C and −572 G/C gene variants between neither IL-6 and CRP levels nor hypertension. The −572 G allele and GG genotype are predominant in Turkish population in Adıyaman, Turkey whereas the CC genotype is very rare.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hypertension (HT) is one of the most common chronic, complex genetic disease world-wide. Its occurrence is influenced by both genetic and environmental factors (Li et al. 2005; Kearneya et al.2004; Conen et al. 2009; Wang et al. 2011). It is characterized by high blood pressure forced heart load. It is known as an important risk factor for cardiovascular, renal disease and stroke but the underlying mechanisms of how high blood pressure cause to cardiovascular disease (CVD) are still uncertain. It leads to poor life quality and increases morbidity and mortality (Li et al. 2005, Chae et al. 2001; Nakajima et al. 1999; Johansson 1999). However molecular mechanisms of hypertension are not fully understood, the inflammation is known to be playing an essential role in pathogenesis of hypertension and cardiovascular diseases. Inflammation is an independent risk factor that may act on initiation and development of HT disease (Li et al. 2005; Bautista et al. 2005; Sesso et al. 2006). Recent studies show increased baseline plasma inflammatory marker levels such as IL-6 and C-reactive protein (CRP) in HT and CVD (Wang et al. 2011; Sesso et al. 2006; Humphries et al. 2001; Gao et al. 2011; Bermudez et al. 2002; Ridker et al. 2000).
Interleukin-6 is a cytokine that plays an essential role in cellular and humoral immune response and is related to inflammation, host defense, and tissue injury (Gao et al. 2011; Ridker et al.2000). It is one of the most important acute-phase response mediators and regulates CRP production in hepatocytes (Gao et al. 2011; Ridker et al. 2000; Jenny et al. 2002; Berg et al. 2009; Baumann and Gauldie 1994). It has been found that both IL-6 and CRP are associated with HT and coronary heart disease in the manner of endothelial dysfunction and impaired fibrinolysis (Humphries et al. 2001; Boos and Lip 2006). However plasma IL-6 levels are very low in healthy individuals they increased rapidly in infection, trauma or stress conditions (Jenny et al. 2002). Plasma IL-6 levels show great differences even among healthy individuals, related to both genetic and environmental factors (Gao et al. 2011; Jenny et al. 2002). These differences may be explained by IL-6 gene variations (Sesso et al. 2006; Gao et al. 2011; Fishman et al. 1998). The IL-6 gene is located at p21 of chromosome 7, contains a 1.3 kb coding sequence with five exons and encodes a 23.7 kd protein. It is a polymorphic gene which −634 C/G, −598 A/G, −597 G/A, −572 G/C, −174 G/C polymorphisms were identified in its promoter region (Wang et al. 2011; Nakajima et al. 1999; Sesso et al. 2006; Gao et al. 2011; Jenny et al. 2002; Baumann and Gauldie 1994; Wypasek et al. 2010; Tanaka et al. 2005; Sanders et al. 2009; Timasheva et al. 2008; Kitamura et al. 2002; Illig et al. 2004). Therefore most of the studies on IL-6 gene focus on promoter region polymorphism analyses. Three single nucleotide polymorphisms (SNPs) in the gene promoter region (−597 G/A; −572 C/G and −174 G/C) have been found to be related to increased gene expression and elevated plasma levels of IL-6 (Humphries et al. 2001; Gao et al. 2011; Rivera-Chavez et al. 2003; Tonet et al. 2008).
In light of the foregoing; the aim of our this study was to investigate the effects of IL-6 gene −174 G/C (rs 1800795), −572 G/C (rs1800796) polymorphisms on plasma IL-6 and CRP levels and their associations with hypertension disease.
Materials and methods
Study population
This study enrolled 108 healthy control subjects and 111 patients with essential hypertension who were admitted to the Cardiology Department of Adıyaman 82th Year State Hospital between February 2010 and January 2011. The study complies with the Declaration of Helsinki and the approval from the Ethic Committee of the Adıyaman University and written informed consent from each individual have been obtained.
Patients who have valve stenosis greater than mild degree or regurgitation, aortic coarctation, previous cardiac surgery, chronic kidney disease, hepatic dysfunction, respiratory illness, acute infection, chronic inflammatory disease or complex congenital heart disease were excluded from the study.
The blood pressure was measured three times after 5-min rest in the sitting position on both upper limbs with the use of automatic manometer (Omron M4 Plus, Omron Healthcare Europe, Hoofddorp, Holland). The mean value of the second and the third measurements were calculated. The measurements taken on the dominant limb were used. The blood pressure values above 140 mmHg for systolic blood pressure (SBP) and above 90 mmHg for diastolic blood pressure (DBP) are considered as hypertension (Chobanian et al. 2003).
Blood assays
EDTA blood samples were centrifuged immediately and two plasma samples were separated for each subject. One of these samples was stored at −20 °C until IL-6 analyses was performed and the second sample was used immediately for analyzing CRP, lipids including total cholesterol, low-density lipoprotein (LDL), high density lipoprotein (HDL) and triglyceride levels (Commercial kit-Roche Diagnostics, Mannheim, Germany, auto analyzer-Roche/Hitachi Cobas c Systems, Basel, Switzerland). The plasma samples were tested for IL-6 levels using an ELISA kit (DIAsource IL-6 EASIA, ELISA reader -Epoc)
Genotype determination
Genomic DNA was extracted from EDTA blood samples by standard salting out method (Miller et al. 1988). Genotyping was performed using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) technique.
IL6 gene −174 G/C and −572 G/C polymorphisms at promoter region were analyzed according to Karahan et al. (2005) and Humpries et al. (2001) with minor modifications as follows.
For −174 G/C, a 431-bp region was amplified by PCR using IL-6 Pro-F 5′CAGAAGAACTCAGATGACTG3′ and IL-6 Pro-R 5′GTGGGGCTGATTGGAAACC3′ primer pair (Karahan et al. 2005). For −572 G/C polymorphism a 163-bp region was amplified by PCR using forward primer F:5′-GGAGACGCCTTGAAGTAACTGC-3′, and reverse primer R: 5′-GAGTTTCCTCTGAC TCCATCGCAG-3′ (Humpries et al. 2001). PCR conditions were provided as 50 ng genomic DNA, 1XPCR buffer, 1.5 mM MgCl2, 100 mol dNTP mixture, 50 pmol of each primer and 0.5 U Taq polymerase in a total volume of 25 l. Cycling conditions were performed as 1 min at 95 °C pre denaturation step, 35 cycles of 1 min at 94 °C denaturation, 1 min at 59 °C (and 55 °C for −572 G/C) annealing and 1 min at 72 °C extension steps following by 5 min at 72 °C single cycle final extension step using thermal cycler (Applied Biosystems Veriti).
RFLP analysis
Interleukin-6 −174 G/C PCR products (431-bp) were digested with 5 Units of NlaIII (Fermentas, St. Leon-Rot, Germany) restriction endonuclease at 37 °C overnight. Digested restriction fragments were electrophoresed on 1 % (wt/vol) agarose gel and bands were visualized under UV after ethidium bromide staining (Vilber Lourmat Marne La Vallee, France). Three different genotypes were determined including G/G with 229, 173, 29 bp and G/C with 229, 173, 122, 51, 29 bp and C/C with 229, 122, 51, 29 bp fragments.
For the IL6 −572 G/C PCR products (163 bp) the same procedure as above was used with Mbl (Fermantas) restriction endonuclease and the genotypes were determined as G/G with 163 bp (undigested), G/C with 163, 101, 62 bp and C/C with 101, 62 fragments.
Statistical analysis
Statistical analysis was performed by running a packaged program of IBM SPSS Statistics 20 software. Comparison of the categorical variables (such as: gender, genotype, allele…) between groups were performed with Pearson Chi Square Test, Yates’ Chi Square Test, Fisher’s Exact Test, One Proportion Exact p Value and Chi Square Goodness of Fit Test analyses. On the other hand, continuous variables (such as: age, height, weight…) were compared between groups with Mann–Whitney U Test for the non-normal variables and Student’s t Test for the normally distributed variables. We compared parameter values between two groups by means of two independent sample t test and Mann–Whitney U test. Furthermore we used Shapiro–Wilk Test for the normality. The p values less than 0.05 were accepted as significant.
Results
Basic characteristics of the HT patients selected for this study are listed in Table 1. There were statistically significant differences between the control group and patients group with respect to gender distribution (p = 0,00), smoking (p = 0,02), diabetes mellitus (DM) (p = 0,00), myocardial infarction (MI) (p = 0,00), body mass index (BMI) (p = 0,00), HDL (p = 0,04), SBP (p = 0,00), DBP (p = 0,00). On the other hand, no significant statistical differences were found in terms of age (p = 0,579), alcohol consumption (p = 0,674), stroke (p = 0,077), total cholesterol (p = 0,335), low density lipoproteins (LDL) (p = 0,561), triglyceride (p = 0,158). In comparison to IL-6 and CRP levels between control and HT groups no significant statistical differences were found (Table 1).
IL-6 gene −174 G/C and −572 G/C genotype distribution and allelic frequencies of controls and patients with HT are listed in Table 2. No statistically significant differences were found between control and patient groups in terms of genotype distribution and allelic frequencies of IL-6 gene −174 G/C (p = 0,215, p = 0,573) and −572 G/C polymorphisms (p = 0,508, p = 0,698). Genotype frequencies of −174 G/C polymorphism were determined as 63.9 % GG, 31.5 % GC and 4.6 % CC in control subjects whereas they were 52.3 % GG, 42.3 % GC and 5.4 % CC in patients group. For −572 G/C polymorphism 76.6 % GG, 20.4 % GC and 0 % CC were found in control subjects whereas 77.5 % GG, 21.6 % GC and 0.9 % CC in patients group. No CC genotype was found in control subjects for −572 G/C polymorphism (Table 2). Genotype distributions were in Hardy–Weinberg equilibrium for both −174 G/C (p = 0.758 for control subjects and p = 0.370 patients group) and −572 G/C (p = 0.238 for control subjects and p = 0.261 for patients group) polymorphisms.
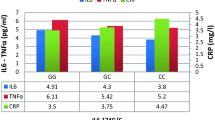
In comparison to plasma IL-6 and CRP levels between two groups according to genotype distributions of −174 G/C and −572 G/C polymorphisms no statistically significant differences were found (p > 0.05) (Table 3).
Discussion
In the present study we have investigated the effects of IL-6 gene −174 G/C and −572 G/C polymorphisms on plasma IL-6 and CRP levels and their possible effects on hypertension etiopathogenesis. Hypertension is a complex genetic disease influenced by both genetic and environmental factors and characterized by high blood pressure (Yamada et al. 2006; Tabassum and Ahmad 2011). Age, gender, life style (sedative life, obesity, excessive alcohol consumption, salty diet and stress), metabolic diseases such as diabetes mellitus are important factors influencing HT development (Grundy et al. 1999). We have found associations between HT and some individual properties such as gender (more in women than men), smoking, and diabetes, MI, BMI, and low HDL (p < 0.05). The summarized results are shown in Table 1. In concordance with our results HT prevalence has been found to be increased in men than women in early adulthood whereas it has been found to be increased in women than man in late adulthood and older age (Özcan 1995). SBP shows a sharper increase with age more in women than man. This means increase in blood pressure and HT prevalence in elderly women (Mancia et al. 2007; Mosca et al. 2011). Acute increase in blood pressure just 15–30 min after cigarette smoking shows that smoking is an important risk factor for hypertension (Öksüz 2004; Suheil 2007). Suheil showed that the influence of BMI on HT. They have suggested that hypertension rate was 3 % in normal weight, 15.9 % in overweight, 33.3 % in obese individuals (Suheil 2007).
Interleukin-6 gene is a polymorphic gene whose −174 G/C and −572 G/C are the common and the rare polymorphisms identified in its promoter region respectively. Some studies showed association between −174 G/C or −572 G/C or both polymorphisms and HT whereas some other studies showed no relationship (Wang et al. 2011; Humphries et al. 2001; Jenny et al. 2002; Timasheva et al. 2008; Losito et al. 2003; Pola et al. 2002).
In our study we found no relationship between genotype distributions and allelic frequencies of IL-6 gene −174 G/C and −572 G/C polymorphisms and HT in comparison to controls and HT patients group. While we found only one case with CC genotype in HT group we found no CC genotype in control subjects for −572 G/C polymorphism (Table 2). This shows that CC genotype of −572 G/C polymorphism is very rare in the Turkish population in the Adıyaman region consistent with results of Humphries et al. (2011) who studied 2589 healthy and 163 CVD men of UK origin and found very rarely −572 CC genotype (GG/GC/CC 2224/225/9 in controls and 135/19/0 in CVD group) (Humphries et al. 2001).
In accordance to our findings, no significant differences were found between IL-6 −174 G/C and −572 G/C polymorphisms and HT whereas some other studies showed relations between IL-6 −174 G/C polymorphism and HT and also cardiovascular diseases (CVD) (Humphries et al. 2001; Timasheva et al. 2008; Losito et al. 2003; Pola et al. 2002; Wong et al. 2007).
Polymorphisms −174 G/C and −572 G/C were shown to be associated with plasma IL-6 (Humphries et al. 2001; Fishman et al. 1998; Losito et al. 2003) and CRP levels (Humphries et al. 2001; Losito et al. 2003; Wong et al. 2007).
Increased IL-6 levels lead to vascular resistance and hypertension in consequence of endothelial dysfunction (Boos and Lip 2006). IL-6 stimulates release of acute phase reactants such as CRP, fibrinogen, amyloid A, TNF-a and IL-ip. It is known that elevated CRP blood levels enhanced hypertension development by inflammation (Wong et al. 2007; Savoia and Schiffrin 2006).
In this study, in order to investigate the relationship between IL-6 gene −174 G/C and −572 G/C variants and IL- 6 and CRP plasma levels and HT we analyzed and compared both IL-6 gene variants and IL6 and CRP levels in healthy control group and HT patients. We have found no statistically significant differences between IL-6 and CRP levels and −174 G/C and −572 G/C IL-6 gene variants and HT (p > 0.05) (Tables 1, 3).
Some studies showed elevated plasma levels of IL-6 associated to −174 G/C polymorphism in patients group (Fishman et al. 1998; Losito et al. 2003) whereas both −174 G/C and −572 G/C polymorphisms were associated with elevated plasma CRP levels (Humphries et al. 2001; Losito et al. 2003; Savoia and Schiffrin 2006). Elevated IL-6 or CRP levels or both were found to be associated with HT. However in some studies no association was found between IL-6 or CRP and HT (Bautista et al. 2005; Sesso et al. 2006; Humphries et al. 2001; Losito et al. 2003).
As it seems, the studies in this area produced contradictory results and discussions. Therefore we investigated in this study the effects of −174 G/C and −572 G/C polymorphisms in the promoter region of the IL-6 gene on plasma IL-6 and CRP levels and their associations with hypertension disease. In our study neither IL-6 and CRP levels nor HT were found significantly associated with −174 G/C and −572 G/C gene variants. This may be because such gene polymorphisms and their effects show broad changes between different populations (Gao et al. 2011) and geographic regions.
In conclusion we found relation to −174 G/C and −572 G/C gene variants between neither IL-6 and CRP levels nor hypertension and −572 G allele and the GG genotype is predominant in the Turkish population in the Adıyaman region whereas the CC genotype is very rare.
References
Baumann H, Gauldie J (1994) The acute phase response. Immunol Today 15:74–80
Bautista LE, Vera LM, Arenas IA, Gamarra G (2005) Independent association between inflammatory markers (C-reactive protein, interleukin-6, and TNF-a) and essential hypertension. J Hum Hypertens 19:49–154
Berg KK, Madsen HO, Garred P, Wiseth R, Gunnes S, Videm V (2009) The additive contribution from inflammatory genetic markers on the severity of cardiovascular disease. Scand J Immunol 69:36–42
Bermudez EA, Rifai N, Buring J, Manson JAE, Ridker PM (2002) Interrelationships among circulating interleukin-6, C-reactive protein, and traditional cardiovascular risk factors in women. Arterioscler Thromb Vasc Biol 22:1668–1673
Boos CJ, Lip GYH (2006) Is hypertension an inflammatory process? Curr Pharm Des 12:1623–1635
Chae CU, Lee RT, Rifai N, Ridker PM (2001) Blood pressure and inflammation in apparently healthy men. Hypertension 38:399–403
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee (2003) The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 289:2560–2572
Conen D, Cheng S, Steiner LL, Buring JE, Ridker PM, Zee RYL (2009) Association of 77 polymorphisms in 52 candidate genes with blood pressure progression and incident hypertension: the women’s genome health study. J Hypertens 27:476–483
Fishman D, Faulds G, Jeffery R, Mohamed-Ali V, Yudkin JS, Humphries S, Woo P (1998) The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J Clin Invest 102:1369–1376
Gao SP, Pan M, Chen C, Ge LJ, Jiang MH, Luan H, Zheng JG, Deng XT, Pan HY, Zhu JH (2011) The G to A polymorphism at -597 of the interleukin-6 gene is extremely rare in southern Han Chinese. Cytokine 55:1–3
Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith SC, Sowers JR (1999) Diabetes and cardiovascular disease a statement for healthcare professionals from the American Heart Association. Circulation 100:1134–1146
Humphries SE, Luong LA, Ogg MS, Hawe E, Miller GJ (2001) The interleukin-6 -174 G/C promoter polymorphism is associated with risk of coronary heart disease and systolic blood pressure in healthy men. Eur Heart J 22:2243–2252
Illig T, Bongardt F, Schöpfer A, Müller-Scholze S, Rathmann W, Koenig W, Thorand B, Vollmert C, Holle R, Kolb H, Herder C; Kooperative Gesundheitsforschung im Raum Augsburg/Cooperative Research in the Region of Augsburg (2004) Significant association of the interleukin-6 gene polymorphisms C-174G and A-598G with type 2 diabetes. J Clin Endocrinol Metab 89:5053–5058
Jenny NC, Tracy RP, Ogg MS, Luong LA, Kuller LH, Arnold AM, Sharrett AR, Humphries SE (2002) Interleukin-6 plasma levels and the -174G>C polymorphism are associated with the development of cardiovascular disease. Arterioscler Thromb Vasc Biol 22:2066–2071
Johansson BB (1999) Hypertension mechanisms causing strok. Clin Exp Pharmacol Physiol 26:563–565
Karahan ZC, Deda G, Sipahi T, Elhan AH, Akar N (2005) TNF-A-308G/A and IL-6 -174 G/C polymorphisms in the Turkish pediatric stroke patients. Thromb Res 115:393–398
Kearneya PM, Whelton M, Reynolds K, Whelton PK, He J (2004) Worldwide prevalence of hypertension: a systematic review. J Hypertens 22:11–19
Kitamura A, Hasegawa G, Obayashi H, Kamiuchi K, Ishii M, Yano M, Tanaka T, Yamaguchi M, Shigeta H, Ogata M, Nakamura N, Yoshikawa T (2002) Interleukin-6 polymorphism (-634C/G) in the promotor region and the progression of diabetic nephropathy in type 2 diabetes. Diabet Med 19:1000–1005
Li JJ, Fang CH, Hui RT (2005) Is hypertension an inflammatory disease? Med Hypotheses 64:236–240
Losito A, Kalıdas K, Santoni S, Jeffery S (2003) Association of interleukin-6 -174 G/C promoter polymorphism with hypertension and left ventricular hypertrophy in dialysis patients. Kidney Int 64:616–622
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Struijker Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Kjeldsen SE, Erdine S, Narkiewicz K, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Cifkova R, Dominiczak A, Fagard R, Heagerty AM, Laurent S, Lindholm LH, Mancia G, Manolis A, Nilsson PM, Redon J, Schmieder RE, Struijker-Boudier HA, Viigimaa M, Filippatos G, Adamopoulos S, Agabiti-Rosei E, Ambrosioni E, Bertomeu V, Clement D, Erdine S, Farsang C, Gaita D, Kiowski W, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O'Brien E, Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P, Viigimaa M, Waeber B, Williams B, Zamorano JL, The task force for the management of arterial hypertension of the European Society of Hypertension, The task force for the management of arterial hypertension of the European Society of Cardiology (2007) 2007 Guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 28:1462–1536
Miller SA, Dykes DD, Polesky HF (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16:1215
Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, Newby LK, Piña IL, Roger VL, Shaw LJ, Zhao D, Beckie TM, Bushnell C, D'Armiento J, Kris-Etherton PM, Fang J, Ganiats TG, Gomes AS, Gracia CR, Haan CK, Jackson EA, Judelson DR, Kelepouris E, Lavie CJ, Moore A, Nussmeier NA, Ofili E, Oparil S, Ouyang P, Pinn VW, Sherif K, Smith SC Jr, Sopko G, Chandra-Strobos N, Urbina EM, Vaccarino V, Wenger NK; American Heart Association (2011) Effectiveness-based guidelines for the prevention of cardiovascular disease in women: 2011 update: a guideline from the American Heart Association. J Am Coll Cardiol 57:1404–1423
Nakajima T, Ota N, Yoshida H, Watanabe T, Emi M (1999) Allelic variants in the interleukin-6 gene and essential hypertension in Japanese women. Genes Immun 1:115–119
Öksüz E (2004) Hipertansiyonda klinik değerlendirme ve ilaç dışı tedavi. Sted 13:103s
Özcan N (1995) Hipertansiyon İdeal Matbaacılık, Ankara
Pola R, Flex A, Gaetani E, Pola P, Bernabei R (2002) 174 G/C polymorphism of the interleukin-6 gene promoter and essential hypertension in an elderly Italian population. J Hum Hypertens 16:637–640
Ridker PM, Rifai N, Stampfer MJ, Hennekens CH (2000) Plasma concentration of IL-6 and the risk of future myocardial infarction among apparently healthy men. Circulation 101:1767–1772
Rivera-Chavez FA, Peters-Hybki DL, Barber RC, O’Keefe GE (2003) Interleukın-6 promoter haplotypes and interleukın-6 cytokine responses. Shock 20:218–223
Sanders J, Hawe E, Brull DJ, Hubbart C, Lowe GDO, Rumley A, Humphries SE, Montgomery HE (2009) Higher IL-6 levels but not IL6 -174G>C or -572G>C genotype areassociated with post-operative complication following coronary artery bypass graft (CABG) surgery. Atherosclerosis 204:196–201
Savoia C, Schiffrin EL (2006) Inflammation in hypertension. Curr Opin Nephrol Hypertens 15:152–158
Sesso HD, Wang L, Buring JE, Ridker PM, Gaziano JM (2006) Comparison of interleukin-6 and c-reactive protein for the risk of developing hypertension in women. Hypertension 49:304–310
Suheil SJ (2007) Risk factors for hypertension among urban males in Mombasa Kenya. Official Publication of the Tanzania Medical Students’ Association 8:13–16
Tabassum N, Ahmad F (2011) Role of natural herbs in the treatment of hypertension. Pharmacogn Rev 5:30–40
Tanaka C, Mannamı T, Kamıde K, Takıuchı S, Kokubo Y, Katsuya T, Kawano Y, Mıyata T, Ogıhara T, Tomoıke H (2005) Single nucleotide polymorphisms in the interleukin gene associated with blood pressure and atherosclerosis in a Japanese general population. Hypertens Res 28:35–41
Timasheva YR, Nasibullin TR, Zakirova AN, Mustafina OE (2008) Association of interleukin-6, interleukin- 12, and interleukin-10 gene polymorphisms with essential hypertension in Tatars from Russia. Biochem Genet 46:64–74
Tonet AC, Karnikowski M, Moraes CF, Gomes L, Karnikowski MGO, Cordova C, Nobrega OT (2008) Association between the -174 G/C promoter polymorphism of the interleukin-6 gene and cardiovascular disease risk factors in Brazilian older women. Braz J Med Biol Res 41:47–53
Wang L, Manson JE, Gaziano JM, Liu S, Cochrane B, Cook NR, Ridker PM, Rifai N, Sesso HD (2011) Circulating inflammatory and endothelial markers and risk of hypertension in white and black postmenopausal women. Clin Chem 57:729–736
Wong LYF, Leung RYH, Ong KL, Cheung BMY (2007) Plasma levels of fibrinogen and C-reactive protein are related to interleukin-6 gene -572 C4G polymorphism in subjects with and without hypertension. J Hum Hypertens 21:875–882
Wypasek E, Undas A, Maciejewska MS, Kapelak B, Plicner D, Stepien E, Sadowski J (2010) The increased plasma C-reactive protein and interleukin-6 levels in patients undergoing coronary artery bypass grafting surgery are associated with the interleukin-6 -174G>C gene polymorphism. Ann Clin Biochem 47:343–349
Yamada Y, Matsuo H, Segawa T, Watanabe S, Kato K, Hibino T, Yokoi K, Ichihara S, Metoki N, Yoshida H, Satoh K, Nozawa Y (2006) Assessment of the genetic component of hypertension. Am J Hypertens 19:1158–1165
Acknowledgments
This study was supported by a grant of the Research Foundation of Adıyaman University (FEFYL/2012-0002), Turkey.
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Karaman, E., Urhan Kucuk, M., Bayramoglu, A. et al. Investigation of relationship between IL-6 gene variants and hypertension in Turkish population. Cytotechnology 67, 947–954 (2015). https://doi.org/10.1007/s10616-014-9732-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10616-014-9732-1