
Abstract
One way of attempting to improve the efficacy and effectiveness of Cognitive Behavioral Therapy (CBT) for depression is to identify the processes of change that contribute towards its positive outcome. In addition to well-researched cognitive processes, another possible change process is affect experiencing (AE); i.e., a patient’s affective experience in-session. Theorists, clinicians and researchers have emphasized the role of affective traits, tendencies and symptoms in the development, maintenance, and treatment of depression. We make the case that it may be important to also consider patients’ full range of affect experiencing (AE), as a changeable in-session process that may relate to CBT treatment outcome. This systematic review aimed to clarify what is already empirically known regarding in-session AE in CBT for depression and which gaps in empirical research need to be filled by future studies. The reviewed studies on AE in CBT for depression suggest that it is possible to identify and measure AE. In-session experiencing of positive and negative affect (when it includes cognitive processes) relates to and may predict a reduction of symptoms. We encourage researchers to develop and refine multifaceted process measures and analyses to explore when, how and how much AE can be effectively experienced by patients, and how optimal levels of AE may be facilitated by the therapist.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since Beck’s (1979) introduction of the cognitive model for depression 50 years ago, numerous studies have demonstrated the efficacy and effectiveness of Cognitive Behavioral Therapy (CBT) for depression (for a review of meta-analyses, see Butler et al. 2006). However, a significant proportion of depressed patients do not benefit from CBT (Cuijpers et al. 2014). The average improvement among CBT responders in routine clinical practice may only be 20–50% (Westbrook and Kirk 2005). Furthermore, the limited access to CBT services (White 2008) and high drop-out rates (e.g. Bados et al. 2007), mean that there is a need to optimize the effectiveness of treatment for each individual patient, at the earliest opportunity.
One way of attempting to improve CBT for depression is to identify the precise processes of change that contribute towards positive treatment outcome. CBT processes which have been investigated include, cognitive change, behavioral change, and the therapeutic alliance (e.g. Llewelyn et al. 2016). Our understanding of how CBT achieves its effects is currently incomplete (Strunk et al. 2017), and the potential change processes in CBT for depression have not been adequately tested (Crits-Christoph et al. 2013). In addition to further analysis relating to the role of changing cognitions (e.g. modification of beliefs) and learning compensatory skills (e.g. problem solving techniques such as generating alternative explanations for negative events) in CBT for depression (e.g. Lorenzo-Luaces et al. 2015, 2016), research on possible additional processes beyond cognitive and behavioral change could be worthwhile.
We attempt to complement the existing process-outcome research by putting forward the possibility of an additional, often ignored, change process; the patient’s in-session experience of affect, called affect experiencing (AE). We propose that the process of facilitating patients’ deepening of their affective experience in-session possibly offers an additional avenue by which CBT treatments for depression may succeed. We will start with a brief description of the theoretical, empirical, and clinical rationale for the importance of AE, followed by a systematic review of the existing empirical evidence on the role of AE in CBT for depression.
AE in CBT: Theories of Change
In this section, we briefly describe the concept of AE, its role in the development of pathology and theories of change that may be considered relevant to the CBT treatment of depression. At the broadest level, AE refers to all the tacit and explicit (non-) verbal processes involved in the patient’s generation, experience, regulation and the cognitive elaboration of a felt sense of a specific emotion (Whelton 2004). From this perspective, AE is viewed as the means whereby patient’s emotions can be brought into conscious awareness, evaluated, understood, and used to guide planning, decision-making, and behavior (Greenberg 2008). Different theoretical and neuro-scientifically informed models of affect emphasize its importance as a primary motivational system (e.g. Ekman and Davidson 1994) to facilitate implicit knowledge learning and to activate and modify emotional memory (Samoilov and Goldfriend 2000). AE has been hypothesized to be effective in activating basic emotion- related brain systems theorized to have evolved prior to the development of language-based representations (Holmes and Mathews 2010). The capacity to identify and act upon affective information is considered necessary to function adaptively.
Affective Science
With its long tradition of extrapolating from basic research, CBT for depression can readily benefit from developments in affective science (Gross 2015). By definition, depression is an affective disorder; a mental disorder in which a major disturbance of feelings or emotions is predominant. People who suffer from an affective disorder, such as anxiety, PTSD (Berking and Wupperman 2012) and depression (Boumparis et al. 2017) experience dysfunction in the identification, experience, expression and/or regulation of affects (Aldao 2016). Depression, specifically, has been linked with alexithymia (e.g. Honkalampi et al. 2001), mood-congruent processing biases (e.g. Kaiser et al. 2015), affective interference, (e.g. Gotlib and Joormann 2010) and high dysregulated negative affect in addition to diminished positive affect (e.g. Boumparis et al. 2017; Hofmann et al. 2012). Also, depression may be associated with a lack of flexibility to resort to different emotion regulation strategies (Bonanno et al. 2004). In line with this, affective change is a common secondary outcome of CBT for depression as reported by patients (e.g. Baker et al. 2012), and observed in the neuronal networks sub-serving emotional processes (e.g. Goldapple et al. 2004).
However, the exact role of these affective processes in depression is rather complex. First, affective symptomatology might not only be a consequence of depression but also play a role in the development and maintenance of depressive symptoms themselves. Research suggests that low levels of positive affect and high levels of negative affect are not necessary equivalent to depression but increase the likelihood of developing a depressive disorder (e.g. Bos et al. 2013). Moreover, in their emotion dysregulation model, Hofmann et al. (2012) describe how a positive feedback loop can become established between the depressive disorder, dysregulation, negative affect, and affective styles (tendencies to prefer certain emotion regulation strategies over others), which leads to a chronic condition that becomes difficult to change. More specifically, Hofmann and colleagues posit that affective disorders are the result of maladaptive regulation of negative emotions, coupled with deficiencies in the experience of positive affect. In line with this model, it has, for example, been reported that depressed individuals choose to use emotion-regulation strategies to maintain or increase their level of sadness more than non-depressed individuals (Millgram et al. 2015), which might make them more likely to stay depressed. In contrast, positive affect might operate as a source of resilience in buffering stress levels (Fredrickson 2001), might play a protective role in the development of depression (Lindahl and Archer 2013), and seems to mediate recovery in depressive patients (Hart et al. 2008).
The role of affect in depression is further complicated by the close connections between cognitive and affective processes. Most everyday emotional processes in the brain are complex mixtures of primary (feeling), secondary (learning and thinking), and tertiary (thoughts about thought) processes that make it hard to identify the affects that contribute to psychopathology (Panksepp 2007). And even if patients would be exactly clear on their underlying affects in treatment, it remains unclear whether to emphasize emotion generation or emotion regulation (Gross 2015). All in all, this complex role of affective processes in the development and maintenance of depression, underlines the importance of affective processes, besides cognitive processes, in the treatment of depression.
AE in Psychotherapy
Traditional CBT theory often maintains that cognitive change precedes affective change and that correcting negative automatic thoughts, maladaptive information processing (that cause and maintain symptoms of depression) and improving compensatory/coping skills may lead to a reduction of symptoms (e.g. Barber and DeRubeis 1989). This means that, traditionally, CBT therapists, especially cognitive therapists have often prioritized cognitive over affective processes (Samoilov and Goldfried 2000); putting more emphasis on managing and containing affective arousal; viewing negative affect in-session as troublesome and symptomatic, something to be tamed and brought back to rational control (Driessen and Hollon 2010). Despite this early emphasis on the role of cognitive processes in CBT, the current theoretical consensus is that affective processes may be more than the product of cognition (for a review of empirical evidence on the complexity of this relationship in relation to depression, see Scott and Ingram 1998).
Several theories of emotional processing postulate that moderate levels of inhibitory affect (i.e. some level of anxious apprehension, destabilization, incongruence, discomfort, guilt, shame or pain) are necessary for emotional activation to occur; to help patients develop motivation to experience affect that was previously avoided (McCullough et al. 2011) and establish change in neural growth, new learning and effective functioning (e.g., Doidge 2007; Ogden et al. 2006). These theories suggest that change occurs when emotional memories are activated (i.e. emotionally experienced) and updated by new emotional experiences in the “here and now” (Lane et al. 2015). Similarly, enhancing patient’s emotional processing in-session, is seen as a necessary and natural process of change in several cognitive behavioral frameworks (e.g., Cognitive Experiential self-theory by Epstein 1994; Dynamic Systems theory by; Hayes and Harris 2000; Interactive Cognitive Subsystems by; Barnard and Teasdale 1991). These theoretical frameworks underline the importance of dual processing of rational knowledge that is consciously known (head-level, cold, intellectual & logical) as well as experiential, implicit knowledge that is experienced in the body. In other words, the rational information needs to become meaningful experientially for it to be incorporated into patients’ existing cognitive structures (Burum and Goldfried 2007). These theoretical frameworks have been applied to numerous pathologies including depression (e.g., Hayes and Harris 2000; Teasdale 1999), have received empirical support (e.g., Hayes et al. 2015; Gillanders & Flaming, 2006), and have informed the development of novel CBT treatments (e.g., Hayes 2015; Segal et al. 2012).
AE in CBT: Practice
A chorus of clinical voices have started recommending that CBT, including CBT for depression, would benefit from a more integrated, complex and differentiated view of the relation between cognition and affect (e.g., Burum and Goldfried 2007; Grosse Holtforth et al. 2012; Hauke and Dall’Occhio 2013; Safran 1998; Samoilov and Goldfried 2000; Whelton 2004). The early focus on “cold” cognitions (i.e. knowledge, insight) has lost its heuristic value and the next phase of CBT development lies in the construct of “hot” cognitions (i.e., affective-laden appraisals or evaluations) that are processed on an emotional level (David and Szentagotai 2006).
However, clinicians would not have to develop new interventions to accommodate this new focus on affect experiencing, some therapists already focus on affect in the conduct of the standard CBT protocol for depression (Thoma and McKay 2015). Arguably, typical CBT techniques for depression, such as, exposure to feared situations in behavioral experiments (Bennett-Levy et al. 2004), or imagery techniques (e.g. modification and re-scripting) used to transform maladaptive schemas (e.g. Hackmann et al. 2011; Young et al. 2003), the procedure of Socratic dialogue (Greenberger and Padesky 1995) to “guide discovery”, and challenging hot thoughts (i.e., affect-laden appraisals or evaluations), might also aim to capture and enhance previously avoided affect in-session (Teasdale 1996). So, in other words, even within a mainly cognitive approach, to achieve most and quickest change, CBT therapists might already focus on the hot cognitions that the patient experiences as most emotionally-laden and therefore most triggering of maladaptive coping strategies (Greenberger and Padesky 1995). This implicit focus on AE in standard CBT practices implies that, in addition to cognitive insight, AE may be viewed as a vehicle for change rather than solely as a target for change.
AE in CBT: Research
Empirical research has already begun to support the proposition that AE might be an important change process. In-session AE has been found to predict symptom improvement across theoretical orientations, including humanistic, experiential (Greenberg 2008; Pascual-Leone and Greenberg 2007) and psychodynamic therapy (the meta-analysis by Diener et al. 2007 reports an effect size of r = .30, very similar to the well established effect size of the impact of the therapeutic alliance on outcome).
Also, within CBT there is increased evidence that in-session AE is an important process of change in the treatment of anxiety disorders, such as PTSD (Prolonged Exposure to fear experiences activated by trauma; e.g. Foa et al. 1995), social anxiety disorder (e.g. Hayes et al. 2008), panic disorder (e.g. Sassaroli et al. 2015), and specific phobia (e.g. Schumacher et al. 2015), as well as cluster C personality disorders (e.g. Ulvenes et al. 2014) and chronic fatigue (e.g. Godfrey et al. 2007). Admittedly, the role of AE in relation to techniques or change mechanisms in treatment of anxiety disorders may be different in the treatment of depression.
Moreover, CBT designed for anxiety disorders has considerable positive effects on comorbid depressive symptoms (effect size g = 0.81), with treatment effects comparable to those of CBT for primary depression (Cuijpers et al. 2016). This suggests the possibility that the facilitation of AE in-session, specific to exposure/experiential interventions for anxiety disorders, may also function as a mechanism of change in CBT for depression (as also argued by Hayes 2015).
Furthermore, the growing evidence-base for experiential affect-focused interventions that have been developed as add-on to traditional CBT (e.g. Exposure-based Cognitive Therapy for depression; Hayes et al. 2015) and efficacious third-wave CBT approaches, further underline the importance of AE and the associated cognitive processing of these experiences in CBT treatment.
In sum, affective processes are important in the development of psychopathology, including depression, as well as its treatments. AE has been emphasized in several theories of change and identified as an important in-session process in a range of psychotherapies for depression, third-wave CBT treatments, as well as CBT treatments for other disorders. This literature suggests that AE might be a potential change process, in addition to cognitive processes and alliance, that is currently under-researched in CBT for depression and that deserves further exploration.
Systematic Review
Now that we have set up a general hypothesis regarding the potential importance of AE in CBT for depression, we conducted a systematic review to examine the role, definition and empirical investigation of AE as change process in CBT for depression. Building on previous research on the role of affect as a trait, tendency, symptom or pre-post outcome in depression, we focus on AE as the patient’s affective state, in-session process, that is amenable to change in the moment. Also, rather than solely focusing on those affects related to the diagnosis of depression (e.g., sadness, irritability, guilt, & low sense of pleasure), AE captures affects in the full range of basic emotional systems (Panksepp 2007). Thus, depressive feeling is only one possibility of AE; patients could also experience other affects such as anger, anxiety, jealousy, shame, pride or closeness. In other words, depressive feeling can be an AE, but depression itself is a diagnostic entity, i.e. an affective disorder.
By reviewing the available empirical findings, we aim to generate tentative hypotheses and stimulate further research on AE in CBT for depression. Raising awareness of AE as an integral part of CBT may ultimately contribute to the development of clinical practice guidelines around these affective in-session processes that may be implemented in the training and practice of everyday CBT clinicians and may lead to more effective and efficient therapies for our patients.
Methods
Systematic Search
Several steps were taken to ensure the search was systematic. Firstly, we followed published guidance for systematic reviews of evaluations of health care interventions (Liberati et al. 2009), including the five PICOS components (population, intervention, comparators, outcome and study design) identified as preferred reporting items for systematic reviews and meta-analyses (PRISMA). Secondly, we used operational definitions to identify and clarify constructs of interest. “Affect experiencing” was defined broadly as the level of emotional arousal currently in focus in the session. The intensity of arousal may be indicated by a verbal exploration of the patient’s current affect, the patients’ vocal tone, arousal, facial expression, nonverbal or charged verbal statements during a session, and subsequent expressions of relief or anxiety following the in-session experience.
The literature review was conducted using the following databases: ScienceDirect, ERIC, SocINDEX, MEDLINE, PsychInfo, Academic Search Complete, ProQuest Central, PsycArticles and Scopus. Search terms included variations on the terms for: (a) in-session affective experiencing (emotion*, affect*, feeling, experien*, process*, in-session, within-session), (b) cognitive behavioral therapy (cognitive therapy, cognitive behavio* therapy, CBT), and (c) depress*. The search was conducted on abstracts of peer-reviewed journals with ‘AND’ entered in the database search to link the different categories (a, b and c) of search terms. For a more detailed description of the database searches, see Appendix A. For clarity, we will use the term CBT, and AE throughout the paper, to reflect the different search terms.
Seven inclusion criteria were used: (i) the study was reported in the English language and published in a peer-reviewed journal before January 2017; (ii) the study reported on adult patients (18–65 years-old), in line with a focus on the implications of the review for adult mental health services, as well as with the majority of existing psychotherapy research (Stewart and Chambless 2007); (iii) the patients suffered from depression, identified by a Diagnostic and Statistical Manual of Mental Disorders diagnosis (DSM), by validated symptom measures; (iv) the treatment was explicitly labeled as CBT intervention or was reported as an unspecified treatment conducted by CBT therapists specifically, to the exclusion of other potentially related integrative interventions or third-wave CBT approaches that incorporate CBT techniques, such as Dialectical Behavior Therapy (Linehan 2015) or Cognitive Analytic Therapy (Ryle and Kerr 2003); (v) the study reported on a CBT treatment that was conducted in an individual format, rather than group, family or couples therapy; (vi) AE was conceptualized as an affect-laden emotional experience by the patient in-session, rather than reported emotionally intensive experiences outside the therapy in between sessions; (vii) AE was measured at least once during treatment, as therapy process, rather than (solely) as therapy outcome or as patient personality trait (potential moderator).
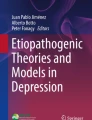
The literature search was conducted twice by the first author, and all steps of the systematic search were repeated by a research assistant to double check the accuracy of the search findings. These three systematic searches identified the same set of 13 empirical studies to be included in this review. Figure 1 shows a PRISMA diagram of the flow of sources through the literature search. A total of 223 published articles were identified during the systematic search of the databases that included all search terms in their abstract, of which 45 were duplicate studies and 7 were unpublished dissertations. The abstracts of the remaining 171 articles were screened. Of these, 103 articles reported on clinical or theoretical models, rather than original empirical studies, and were therefore excluded. A total of 68 empirical articles were skimmed in full to determine eligibility for this review. Of these empirical articles, 31 studies failed to meet the criteria because they either reported on youth (n = 11), a group treatment (n = 6), or integrative therapy (n = 14). From the studies that reported on patients’ affective processes in individual CBT treatment for depressed adults, most measured affect awareness outside the session as secondary treatment outcome (n = 19) rather than affect experiencing in-session. For example, Porter et al. (2016) measured facial emotional processing before and after CBT treatment for depression and Hayes et al. (2015) rated emotional intensity in essays that depressed patients had written in between CBT sessions. Other studies were excluded because they focused on affective patient traits at baseline (n = 4) as predictor or moderator of change rather than the therapy process (e.g. Ritchey et al. 2011). A total of 14 studies examined the relationship between AE in-session and outcome of individual CBT treatment for adults with depression. One of these studies was a publication of a study protocol, and did not report results (Babl et al. 2016) and therefore was not included in this review. The final review consists of 13 treatment studies (marked with * in the reference list; described in Tables 1, 2), of which 9 were process-outcome studies and 4 were process studies of predetermined effective treatment sessions.

PRISMA flow chart
Characteristics of the Reviewed Studies
Design
From the 13 reviewed studies (see Table 1 for an overview of the characteristics of the reviewed studies), 12 reported on secondary analyses of 8 different existing datasets and one study collected data specifically for this process research. 10 of the 12 studies reported on data from clinical trials comparing CBT with another type of treatment. Stringer et al. (2010) also drew from a larger dataset, but in the naturalistic setting of a university counseling service. The only study that did not analyze pre-existing treatment outcome data (Wiser and Goldfried 1993) compared CBT and psychodynamic therapy sessions that were identified by expert therapists as the session with the most significant change for the patient. However, unlike the large sample sizes of the original treatment trials (e.g. N = 469 in Abel et al. 2016) the secondary process analyses reflected relatively small subsamples, ranging from a case (Basto et al. 2016) to 50 patients Abel et al. (2016).
The fact that most studies included in this review report on secondary analyses from larger treatment trials enhanced the comparability of the findings. First, most studies reported on controlled study protocols, clear diagnostic criteria for Major Depressive Disorder (DSM-IV), manualized CBT treatments (e.g. Beck 1979), and treatment adherence checks as well as well-validated and commonly used outcome measures. The comparability of the results in this review was further enhanced by the fact that most (n = 8) process-outcome studies used the Beck Depression Inventory (BDI; Beck et al. 1996) and (n = 5) the Hamilton Rating Scale for Depression (HRSD; Hamilton 1960) to report levels of depression at baseline and end of treatment.
AE Measures
The comparability of the study findings was, however, complicated by the varying nature and quality of the measurements of AE and the associated coding procedures. For a more detailed description of the measures that were used to operationalize AE, including their reported psychometric properties, see Appendix B.
First, most of the process measures that were used to operationalize AE were not explicitly developed to measure AE and appeared not to have been validated with a comparative normative sample. Moreover, many process measures of AE reported in the studies did not distinguish between different affects; however, the function of one affect is not the same as the other. For example, Negative Patient Affect (Jones and Pulos 1993) collapsed observations of anger, sadness (expressive affects) and anxiety, guilt, shame and pain (inhibitory affects, see McCullough et al. 2003) into one single rating, which means it may not adequately differentiate important affective phenomena. More specifically, research suggests that experiencing of anxiety, for example, can be distinguished in two distinct anxiety types, that activate different regions in the brain (Engels et al. 2007); anxious apprehension (involves more left- than right-hemisphere activity) and anxious arousal (associated with the opposite pattern). We argue that anxious arousal is a vulnerability factor for the development of depressive symptoms (Gay et al. 2017), whereas some level of anxious apprehension is likely to be a necessary aspect of emotional processing in treatment of affective disorders, including depression (e.g. Hayes 2015).
Comparability of the studies was further complicated by the fact that each process measure captured different aspects of AE, such as positive or negative valence, inhibition or expression of affect either over a whole session or in speaking turns within a session. Some conceptualized AE as a mixed cognitive-affective process (e.g. affective exploration) others as a sole affective process (expressed bodily arousal or inhibition). Most studies focused on negative AE, whereas five studies also measured affects with a positive valence (e.g. Ablon and Jones 1999).
Moreover, all reviewed studies based their AE ratings on patients’ verbally expressed AE in-session, either via self-report or observer-ratings of transcripts with or without audio-recordings, or solely on audio-recordings of sessions (Abel et al. 2016). This means that none of the AE measurements captured in-session affective processes that occurred outside of patient’s conscious awareness. This is problematic given that people might be unaware of affective changes in their autonomic nervous system, and that depressed patients have a tendency towards over-reporting negative affect (e.g. Disner et al. 2011).
Furthermore, only one study used a self-report measure (Stringer et al. 2010). Although arguably the patient’s view of their own AE is more clinically relevant than an observer’s view of AE in-session, the positive correlations found by Stringer and colleagues could have been artificially inflated due to shared method variance. In other words, it is possible that the same affective symptoms of depression were reported twice; by the process measure and by the symptom measures (BDI, OQ-45 & SCL-5), that were all self-reported after session. The other 12 reviewed studies used observer-rated coding systems, and established sufficient reliability across multiple raters, with intra-class correlations of 0.70 and higher (defined as ‘good’ by Shrout and Fleiss 1979). However, the construct and criterion validity of these AE coding systems as well as the exact training procedures were often insufficiently reported.
Finally, the reviewed studies reported on the association of in-session AE and treatment outcome. None of the studies compared AE to other processes postulated by CBT theory, e.g. cognitive change and behavioral change. Furthermore, no studies examined the role of AE as a potential mediator. No studies considered the temporal assessment of AE and change in symptoms and therefore no studies examined whether AE is a potential cause of change in symptoms. In more general terms, the poor methodological quality of most studies, and small sample sizes resulted in low statistical power and therefore impeded the pooling of results for meta-analysis.
Results
AE in CBT for Depression: Empirical Studies
Table 2 shows an overview of the findings of the reviewed studies. All thirteen studies that empirically measured AE in CBT for depression, identified some level of AE (intensity). This suggests that it is worthwhile exploring the process of AE in more detail; the change of AE over treatment as well as within session, and in relation to treatment outcome.
Comparison of Study Findings that Used the Same AE Measure
Some researchers applied the same scale to measure AE and thus would be expected to report similar results. For example, scores on the Experiencing Scale (EXP; Klein et al. 1986) were reported in five studies. In contrast to expectation, the five studies that used the well-established EXP to measure AE, reported mixed findings regarding the relationship between EXP ratings and outcome. Three studies linked higher EXP ratings with good treatment outcomes (Castonguay et al. 1996; Watson and Bedard 2006; Watson et al. 2011), whereas the other two small sample studies reported no connection between moments of high EXP and effective treatment (Rudkin et al. 2007; Wiser and Goldfried 1993).
Besides the EXP, the Psychotherapy Process Q-sort (PQS; Jones 2000) was also used to operationalize AE in multiple studies. However, the three studies that used the PQS, all created different subscales from the PQS items, therefore the results from these studies are not as easily comparable. Nevertheless, these studies indicated that higher ratings on the four differently constructed negative affect subscales were related to poorer outcome. In summary, these studies using the PQS support a negative affect-negative outcome link.
AE Changes Throughout Treatment
Overall, the studies that measured change of AE throughout treatment found no significant differences over time, with intensity levels staying about the same between early and late sessions (Basto et al. 2016; Ablon and Jones 1999), seemingly suggesting that AE is a relatively stable patient characteristic. However, looking more closely at the change in AE during treatment, intensity first appears to increase and then levels-off during the termination phase, resembling an inversed U shape over treatment (Abel et al. 2016; Rudkin et al. 2007; Watson and Bedard 2006). In addition, valence was lower in the initial sessions and higher in the final phase of treatment, which indicates that AE changes over time from predominantly negative affect to more positive affect (Basto et al. 2016). Generally, these results are in line with recent findings on the reduced negative affect and increased positive affect in the recovery of depression (Boumparis et al. 2017; Hart et al. 2008). Also, these results are compatible with Hayes and Strauss’s (1998) suggestion that resolving depressive symptoms requires an immersion in negative feelings— feeling worse before feeling better.
AE Changes Within Session
The only study that measured change of AE intensity (affective arousal) within sessions (Mackay et al. 2002) found a significant decrease of AE during the session followed by an increase at the end of the session. Within CBT session, the time course of arousal tended to be U-shaped whereas it was inverted-U-shaped in the Psychodynamic Interpersonal therapy (PI) sessions. This difference between the treatments during the middle of the sessions (Mackay et al. 2002) may be consistent with the view that reported expert PI therapists viewed portions containing higher AE as more critical to the change process, whereas CBT therapists viewed lower levels of AE as being therapeutically more significant (Wiser and Goldfried 1993).
AE in Good and Bad Outcome Cases
The three studies that compared good and bad outcome cases, although all using the EXP measure for AE, gave contradictory results. Rudkin et al. (2007) reported lower AE in the improved two cases (clinical significant and reliable change on the BDI), then in the two cases that showed no improvement. Wiser and Goldfried (1993) found no difference between AE in segments that were identified as significant or non-significant to the improvement in that session. Watson and Bedard (2006) found the opposite results, concluding that the 10 good outcome cases (highest reliable change on the BDI) showed significantly higher AE than the 10 bad outcome cases (lowest reliable change on the BDI) in CBT. These contradictory findings might suggest that good outcome does not require AE levels to change within-session per se, but for in-session AE to slowly increase over the course of several sessions. This pattern of AE change over treatment in good outcome cases, is consistent with the inversed U pattern found in other psychotherapies (Ulvenes et al. 2014).
AE in CBT Compared to Other Therapies
Compared to other treatment modalities, CBT patients experienced either similar levels of AE intensity (Coombs et al. 2002; Mackay et al. 2002; Wiser and Goldfried 1993), or slightly lower AE intensity (Coombs et al. 2002; Jones and Pulos 1993; Rudkin et al. 2007; Watson and Bedard 2006), when measuring the cognitive exploration and expression of affect with a negative valence (Mackay et al. 2002). CBT patients, for example, expressed less anger, less ambivalent or negative feelings to the therapist, and less struggles to control feelings than patients in Psychodynamic Therapy (PT) (Jones and Pulos 1993). The levels of inhibition (arguably a type of negative affect) in CBT appeared also to be lower than in Interpersonal Psychotherapy (IPT) (Coombs et al. 2002) but higher than in PT (Jones and Pulos 1993). When CBT patients expressed negative affect, it was with relatively higher valence ratings (more pleasant) than in PI (Mackay et al. 2002).
AE and Treatment Outcome
In line with research on other therapy models (Hendricks 2007), most of the studies reported that “deeper” process (i.e., higher scores on the EXP) lead to improved symptoms. Higher AE predicted better treatment outcomes at the end of treatment and follow-up in the five studies that reported regression analyses. One of these studies (Hayes and Strauss 1998) also reported a non-significant relation between a second measure of AE and outcome. The effect of AE on outcome seems to depend on the nature of the AE intensity (whether it included a cognitive element) and AE valence (whether it was negative or positive).
Higher AE levels were related to lower symptom levels when the measured AE construct included an aspect of cognitive processing (e.g. emotional processing in Abel et al. 2016; EXP in; Castonguay et al. 1996; collaboration of emotional exploration in; Coombs et al. 2002; destabilization in; Hayes and Strauss 1998; affect regulation in; Watson et al. 2011) or when it measured AE with a positive valence specifically (e.g. having a cathartic experience & feeling animated or excited) (Ablon and Jones 1999).
In contrast, it appears that when AE was measured as a purely negative affective experience (expressed or inhibited affect without cognitive processing), higher AE had no impact (client affective intensity in Hayes and Strauss 1998) or even a negative impact on the treatment outcome (Ablon and Jones 1999). It must be noted, however, that this negative relation only appeared to be true for post treatment outcome. When process and outcome were measured in the same early sessions, higher AE intensity was unrelated to symptom ratings (Basto et al. 2016) but was related to increased hope (Abel et al. 2016). This suggests that AE might bring some immediate relief but it may take a few sessions before AE contributes towards symptom improvement.
The only exception to this was Stringer et al. (2010), who measured self-reported arousal levels of negative affect without cognitive processing. Like the measures of AE that include cognitive processing, their AE scores at the third session, appeared to be related to improved outcomes at this same session as well as the final session. As this was the only self-report measure of AE, it could be argued that some level of cognitive processing had already taken place for the patients to be able to identify these negative emotions.
Discussion
There is a growing evidence-base for the relationship between affective traits and the development, maintenance and treatment of depression. This review makes the case that it may be important to consider patients’ affect experiencing (AE), as a changeable in-session state beyond the typical depressive affects, as it may relate to CBT treatment outcome. This is consistent with the increasing number of theorists and clinicians, who suggest that, in addition to cognitive processes, AE might be a vehicle for change in CBT treatment for depression and thus an important avenue to explore (e.g., Grosse Holtforth et al. 2012; Hauke and Dall’Occhio 2013; Hayes 2015).
This systematic review of the empirical evidence aimed to clarify what is already known regarding AE in CBT for depression and which gaps in empirical research need to be filled by future studies. The systematic search highlights that AE has been poorly defined within the CBT literature for depression and has received relatively little empirical exploration. The scarcity of empirical process-outcome research in this area might be explained in part by the complexity of measuring in-session AE, with regards to its intensity, optimal level, valence (positive or negative), inhibitory and expressive function, cohesion with cognitive processing, immediate changes within session, between sessions, within different therapy models and different patients.
This review illustrates that it is possible to identify and measure AE in CBT for depression. However, AE reported by patients and AE reported by trained observers might not be the same. The only study that used a self-report measure instead of observer ratings (Stringer et al. 2010) found contradictory results. This either raises questions regarding the validity of the measure, suggests a difference in opinion between observers and patients, or indicates the complexity of measuring a construct that is not always conscious or expressed verbally.
Overall within-session AE changed in a specific U shaped pattern, different from more emotion-focused treatments such as Experiential Dynamic Therapy, which show an inversed U shape pattern of AE change within session (e.g. Aafjes-van Doorn et al. 2017). However, when considering the entire treatment, the pattern of AE change in CBT showed an increase over time, indicating highest in-session AE in the middle phase of treatment, leveling off at the end of treatment. This pattern is consistent with the AE change found in other psychotherapies (e.g. Ulvenes et al. 2014).
AE predicted symptom improvement (Abel et al. 2016; Castonguay et al. 1996; Hayes and Strauss 1998; Stringer et al. 2010), measured at the end of treatment and follow-up, suggesting that AE might lead to change in CBT for depression. These findings are consistent with the frameworks proposed by the Cognitive Experiential self-theory (Epstein 1994), Interactive Cognitive Subsystems (Barnard and Teasdale 1991) and the Dynamic Systems Theory (Hayes and Harris 2000) that forms the foundation for the Exposure-Based Cognitive Therapy model for depression (Hayes 2015).
Limitations of the Systematic Review
This systematic review was limited in several ways. First, the poor methodological quality of most studies, and small sample sizes impeded the pooling of results for meta-analysis. Second, the clinical implications of the findings are limited because they only support the association of AE and treatment outcome and cannot clarify the exact role of AE in CBT for depression. The small number of empirical papers identified in this review merely emphasize the lack of research into the role of AE in CBT for depression and the need for further empirical research in this area. Third, we are aware that the narrow scope of the inclusion criteria in this review, of treatments explicitly identified as CBT, might have resulted in an arbitrary selection of studies. It is likely that recently developed CBT-based integrative approaches, such as Mindfulness Based Cognitive Therapy (Segal et al. 2012) or Emotional Schema Therapy (Leahy 2015), that are mostly based on cognitive behavioral principles and have been the focus of empirical research on AE, were not included in this review because they were labeled as integrative treatments by the authors. The opposite might also be true. For example, we included a study in this review on Exposure-Based Cognitive Therapy (EBCT; Hayes and Strauss 1998), because it was described by the authors as a CBT model (originally developed for PTSD). However, if the authors had emphasized the integrative nature of EBCT, as done in other publications from the same research group (Hayes et al. 2005), this empirical study would not have been included in this review. Notably, our findings on in-session AE in traditional CBT for depression, are consistent with the Dynamic Systems Theory, that is the foundation for EBCT (Hayes et al. 2015). Given these narrow selection criteria, it will be important to consider the findings of this review not in isolation but in the context of the growing empirical evidence on the role of AE in other CBT-based integrative treatments for depression.
Thus, the limited literature available does not enable us to derive strong conclusions regarding the role of AE in the treatment of depression. However, the review enables us to ask important questions about where the field should be headed.
Future Directions
We hope that this review will encourage researchers to consider the role of AE in CBT. Applying multifaceted process measures and analyses, might help to explore when, how and how much AE can be effectively experienced by patients and may lead to future research on how optimal levels of AE may be facilitated by the therapist. Given the relative infancy of affect-related research in CBT for depression, three important areas for further investigation are apparent. First, given the lack of adequate tools to assess the cognitive, inhibitory and expressive aspects of in-session AE as well as its positive and negative valence, it will be important to develop and improve measurement tools that cover the different aspect of AE. Also, process coding of video-recordings, rather than transcripts or audio-recordings, could be a more valid source for coding AE because it captures non-verbal affect expressions, such as subtle hands or eye-movements, trembling or blushing. Besides observer-ratings, AE should also be measured by other means, including patient self-report, therapist ratings, computer based text analyses and physiological measures (e.g. Fleury et al. 2016). Using multiple source of data will elucidate whether they converge into one or more underlying mechanisms of this potential change process.
Secondly, micro-analyses of AE within moments during sessions (e.g. Aafjes-van Doorn et al. 2017) could help elucidate whether change in cognition precedes AE or AE precedes cognitive change, and ratify whether experiential work is an effective augmentation to current cognitive behavioral practice. Most likely this is a complex process over time. Detailed micro-analyses could also clarify if and how AE in-session is connected to a specific intervention, peak activation, or average activation that predicts treatment outcome (e.g. as done for short term dynamic therapy in Town et al. 2012). It might be possible to identify the optimal level of patients’ affective arousal in-session above and below which patients will have a worse outcome (see Carryer and Greenberg 2010 for an example of an empirical investigation into the optimal level of AE in experiential therapy for depression), alongside the cognitive modes of processing. Because AE is a dynamic and not a static process, it is likely that the same level of AE might be appropriate in one moment and very un-therapeutic another moment. The required intensity of arousal in a certain moment may need much more fine-grained process measurement of (a) the patients’ vocal tone, facial expression, nonverbal or charged verbal statements during a session, (b) the duration of the affective arousal, (c) the levels of cognitive insight before and after the AE, and (d) subsequent expressions of relief.
Finally, research should seek to elucidate the mechanisms of action underlying cognitive behavioral experiential work by investigating possible causal pathways through which AE may achieve therapeutic effects in CBT. Although theorists have proposed several ideas (e.g., destabilization, emotion regulation, implicit knowledge learning, or modified emotional memory), these possible underlying mechanisms of change still need to be examined. Future mediation analyses of AE, could also include other process-related variables, such as the alliance (e.g. Fisher et al. 2016), the attunement to the patient’s AE (e.g. Ulvenes et al. 2014), the therapist’s tolerance of emotions (e.g. Schumacher et al. 2015), and the memorability of interventions (e.g. Greenberg 2007). Other moderating factors such as the patient’s emotional flexibility (Bonanno et al. 2004), patient’s positive and negative affect levels (e.g. Boumparis et al. 2017), attachment style (e.g. Garrison et al. 2012), gender, culture, learning style (e.g. van Doorn et al. 2012) and preference for different levels of affect in-session (e.g. Cooper and Norcross 2016), may also interact with in-session AE to predict outcome. Such research would not only benefit clinical practice by refining techniques for the facilitation of in-session AE but also help inform best practice guidance for their implementation.
Clinical Implications
Once future empirical research has further clarified the role of AE in CBT for depression, effectiveness of treatments may be further enhanced by research on how an optimal level of patients’ AE in-session could potentially be facilitated. Although it is beyond the scope of this review to give a comprehensive overview of all possible therapist techniques that have been proposed to facilitate AE, we briefly illustrate some possible clinical strategies that might aid the patient’s AE in-session and might be considered in future research on AE in CBT treatment for depression.
First, the therapist should consider starting with addressing the patient’s reluctance to engage in experiential exercises and accept feelings of distress (Clark 2013). Rather than omitting in-session exposures from the treatment because of patient refusal, Clark (2013) suggests that CBT therapists could apply the ‘Collaborative Empiricism’ approach Kazantzis et al. (2013) to identify, normalize and change maladaptive beliefs about emotions that undermine engagement in the therapy process, and develop gradual exposures that can test the patients’ negative assumptions. The use of motivational interviewing techniques to address those same issues is likely to be helpful.
The next step would be to actively engage with affect in-session rather than focusing exclusively on reducing it. Therapists could deliberately enhance patient’s awareness of in-session emotional disturbance, by noticing, tolerating (i.e. covert modeling; Goldfried 2013; overt role playing; Vyskocilova and Prasko 2012) and normalizing the experienced ‘destabilization’, explaining that ‘sometimes things need to be become worse before they get better’ (Hayes et al. 2015).
To further facilitate and amplify patients’ AE, therapists could apply strategies as adjunct to the conventional CBT protocol, barrowing from evidence-based third-wave CBT and integrative therapies, such as Acceptance and Commitment Therapy (Hayes et al. 2011), Compassion-Focused Therapy (Gilbert 2009), Affect Phobia Therapy (McCullough et al. 2003), Emotion-Focused Therapy (Greenberg 2008), Mindfulness-Based Cognitive Therapy (Segal et al. 2012) and Emotional Schema Therapy (Leahy 2015).
However, as mentioned previously, therapists do not have to borrow from other treatment protocols; they may also capture and enhance AE by applying standard CBT practices (i.e. exposure, imagery and challenging hot cognitions). Additional procedures that may be used to facilitate AE in CBT sessions for depression include: (i) “two-chair work” to alternate perspectives from both chairs, and increase self-compassion (see Goldfried 2013); (ii) “empty chair work”, to help the patient to express their wishes and needs, and change emotional schemas concerning the other (see Babl et al. 2016); (iii) brief “meditative” or “mindfulness” practices, to help patients learn to intentionally control their attention (e.g., Hayes and Harris 2000; Lau and Grabovac 2009; Teasdale and Chaskalson 2011); (vi) “tracking” of patients’ bodily sensations during the session (see Hauke and Dall’Occhio 2013); (v) “audio- and proprioception” to invite patients to experiment with changes in vocal tone, body positions and gestures (Barnard and Teasdale 1991); (vi) “focusing” on the here-and now inner experience by symbolizing feelings in words or pictures; and (vii) offering “evocative empathic responses” by extending the patient’s narrative with vivid examples and metaphors (Kennedy-Moore and Watson 2001) and elaborating on their catastrophic scenarios (Vyskocilova and Prasko 2012).
Conclusion
Considering the theorized models of psychopathology development (e.g. Hofmann et al. 2012), pathways of change (e.g., Hayes et al. 2015; Lane et al. 2015), and the recent findings in psychotherapy research and the affective neurosciences, AE might play an important role in CBT for depression. The details around when, how and how much AE can be effectively manipulated in CBT still must be empirically determined. Further research is needed to ratify the efficacy of different affect-facilitating interventions in CBT and further inform best guidance for its implementation.
For now, we may conclude that, regardless of the specific technique, therapists may want to be mindful not to avoid difficult affect experiences and exposure exercises in CBT (Clark 2013). We realize that this is easier said than done (Schumacher et al. 2014). Although some therapists might pull for more than the patient is ready to experience (Gelso and Kanninen 2017), others might find it difficult to focus on salient emotions, and to maintain the level of emotional arousal that might be most conducive to change (Subic-Wrana et al. 2016). Attending emotionally-focused training (e.g. Montagno et al. 2011) or participating in regular process coding of treatment sessions, (Schanche et al. 2010), might help therapists to hone their awareness of patients’ AE, to reflect on its meaning and function, and to build competence in facilitating positive and negative AE in-session.
References
Aafjes-van Doorn, K., Lilliengren, P., Cooper, A., Macdonald, J., & Falkenström, F. (2017). Patients’ affective processes within initial experiential dynamic therapy sessions. Psychotherapy, 54(2), 175–183.
*Abel, A., Hayes, A. M., Henley, W., & Kuyken, W. (2016). Sudden gains in cognitive–behavior therapy for treatment-resistant depression: Processes of change. Journal of Consulting and Clinical Psychology, 84(8), 726–737. doi:10.1037/ccp0000101.
*Ablon, J. S., & Jones, E. E. (1999). Psychotherapy process in the NIMH treatment of depression collaborative research program. Journal of Consulting and Clinical Psychology, 67(1), 64–75. doi:10.1037/0022-006X.67.1.64.
Adler, J. M., Harmeling, L. H., & Walder-Biesanz, I. (2013). Narrative meaning making is associated with sudden gains in psychotherapy clients’ mental health under routine clinical conditions. Journal of Consulting and Clinical Psychology, 81(5), 839–845. doi:10.1037/a0033774.
Aldao, A. (2016). Introduction to the special issue: Emotion regulation as a transdiagnostic process. Cognitive Therapy and Research, 40(3), 257–261. doi:10.1007/s10608-016-9764-2.
Babl, A., Holtforth, M. G., Heer, S., Lin, M., Stähli, A., Holstein, D., … Ramseyer, F. (2016). Psychotherapy integration under scrutiny: Investigating the impact of integrating emotion-focused components into a CBT-based approach: A study protocol of a randomized controlled trial. BioMedCentral Psychiatry, 16(1), 423–443. doi:10.1186/s12888-016-1136-7.
Bados, A., Balaguer, G., & Saldaña, C. (2007). The efficacy of cognitive–behavioral therapy and the problem of drop-out. Journal of Clinical Psychology, 63(6), 585–592. doi:10.1002/jclp.2036.
Baker, R., Owens, M., Thomas, S., Whittlesea, A., Abbey, G., Gower, P., … Thomas, P. W. (2012). Does CBT facilitate emotional processing? Behavioural and Cognitive Psychotherapy, 40(1), 19–37. doi:10.1016/j.jad.2011.08.004.
Barber, J. P., & DeRubeis, R. J. (1989). On second thought: Where the action is in cognitive therapy for depression. Cognitive Therapy and Research, 13(5), 441–457. doi:10.1007/BF01173905.
Barkham, M., Shapiro, D. A., Hardy, G. E., & Rees, A. (1999). Psychotherapy in two-plus-one sessions: Outcomes of a randomized controlled trial of cognitive–behavioral and psychodynamic–interpersonal therapy for subsyndromal depression. Journal of Consulting and Clinical Psychology, 67(2), 201–211.
Barnard, P. J., & Teasdale, J. D. (1991). Interacting cognitive subsystems: A systemic approach to cognitive-affective interaction and change. Cognition & Emotion, 5(1), 1–39. doi:10.1080/02699939108411021.
*Basto, I., Pinheiro, P., Stiles, W. B., Rijo, D., & Salgado, J. (2016). Changes in symptom intensity and emotion valence during the process of assimilation of a problematic experience: A quantitative study of a good outcome case of cognitive-behavioral therapy. Psychotherapy Research, 1–13. doi:10.1080/10503307.2015.1119325.
Beck, A. T. (1979). Cognitive therapy of depression. New York: Guilford Press.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation.
Bennett-Levy, J., Westbrook, D., Fennell, M., Cooper, M., Rouf, K., & Hackmann, A. (2004). Behavioural experiments: Historical and conceptual underpinnings. In Oxford guide to behavioural experiments in cognitive therapy (Vol. 2, pp. 1–20). Oxford: Oxford University Press. doi:10.1093/med:psych/9780198529163.003.0001.
Berking, M., & Wupperman, P. (2012). Emotion regulation and mental health: Recent findings, current challenges, and future directions. Current Opinion in Psychiatry, 25(2), 128–134. doi:10.1097/YCO.0b013e3283503669.
Bonanno, G. A., Papa, A., Lalande, K., Westphal, M., & Coifman, K. (2004). The importance of being flexible: The ability to both enhance and suppress emotional expression predicts long-term adjustment. Psychological Science, 15(7), 482–487. doi:10.1111/j.0956-7976.2004.00705.x.
Bos, S. C., Macedo, A., Marques, M., Pereira, A. T., Maia, B. R., Soares, M. J., … Azevedo, M. H. (2013). Is positive affect in pregnancy protective of postpartum depression? Revista Brasileira de Psiquiatria, 35(1), 5–12. doi:10.1016/j.rbp.2011.11.002.
Boumparis, N., Karyotaki, E., Kleiboer, A., Hofmann, S. G., & Cuijpers, P. (2017). The effect of psychotherapeutic interventions on positive and negative affect in depression: A systematic review and meta-analysis. Journal of Affective Disorders, 202, 153–162. doi:10.1016/j.jad.2016.05.019.
Burum, B. A., & Goldfried, M. R. (2007). The centrality of emotion to psychological change. Clinical Psychology: Science and Practice, 14(4), 407–413. doi:10.1111/j.1468-2850.2007.00100.x.
Butler, A. C., Chapman, J. E., Forman, E. M., & Beck, A. T. (2006). The empirical status of cognitive-behavioral therapy: A review of meta-analyses. Clinical Psychology Review, 26(1), 17–31. doi:10.1016/j.cpr.2005.07.003.
Carryer, J. R., & Greenberg, L. S. (2010). Optimal levels of emotional arousal in experiential therapy of depression. Journal of Consulting and Clinical Psychology, 78(2), 190–199. doi:10.1037/a0018401.
*Castonguay, L. G., Goldfried, M. R., Wiser, S., Raue, P. J., & Hayes, A. M. (1996). Predicting the effect of cognitive therapy for depression: A study of unique and common factors. Journal of Consulting and Clinical Psychology, 64(3), 497–504. doi:10.1037/0022-006X.64.3.497.
Clark, D. A. (2013). Collaborative empiricism: A cognitive response to exposure reluctance and low distress tolerance. Cognitive and Behavioral Practice, 20(4), 445–454. doi:10.1016/j.cbpra.2012.06.001.
*Coombs, M. M., Coleman, D., & Jones, E. E. (2002). Working with feelings: The importance of emotion in both cognitive-behavioral and interpersonal therapy in the NIMH Treatment of Depression Collaborative Research Program. Psychotherapy: Theory, Research, Practice, Training, 39(3), 233–244. doi:10.1037/0033-3204.39.3.233.
Cooper, M., & Norcross, J. C. (2016). A brief, multidimensional measure of clients’ therapy preferences: The Cooper-Norcross Inventory of Preferences (C-NIP). International Journal of Clinical and Health Psychology, 16(1), 87–98. doi:10.1016/j.ijchp.2015.08.003.
Crits-Christoph, P., Gibbons, M. C., & Mukherjee, D. (2013). Psychotherapy process-outcome research. In M.J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (6th Ed), (pp 298–340). Hoboken, NJ: Wiley.
Cuijpers, P., Cristea, I. A., Weitz, E., Gentili, C., & Berking, M. (2016). The effects of cognitive and behavioural therapies for anxiety disorders on depression: A meta-analysis. Psychological Medicine, 46(16), 3451–3462. doi:10.1017/S0033291716002348.
Cuijpers, P., Karyotaki, E., Weitz, E., Andersson, G., Hollon, S. D., & van Straten, A. (2014). The effects of psychotherapies for major depression in adults on remission, recovery and improvement: A meta-analysis. Journal of Affective Disorders, 159, 118–126. doi:10.1016/j.jad.2014.02.026.
David, D., & Szentagotai, A. (2006). Cognitions in cognitive-behavioral psychotherapies; toward an integrative model. Clinical Psychology Review, 26(3), 284–298. doi:10.1016/j.cpr.2005.09.003.
Diener, M. J., Hilsenroth, M. J., & Weinberger, J. (2007). Therapist affect focus and patient outcomes in psychodynamic psychotherapy: A meta-analysis. American Journal of Psychiatry, 164(6), 936–941. doi:10.1007/BF01172968.
Disner, S. G., Beevers, C. G., Haigh E.A.P., & Beck, A. T. (2011). Neural mechanisms of the cognitive model of depression. Nature Reviews Neuroscience, 12, 467–477. doi:10.1038/nrn3027.
Doidge, N. (2007). The brain that changes itself: Stories of personal triumph from the frontiers of brain science. London: Penguin Books.
Driessen, E., & Hollon, S. D. (2010). Cognitive behavioral therapy for mood disorders: Efficacy, moderators and mediators. Psychiatric Clinics of North America, 33(3), 537–555. doi:10.1016/j.psc.2010.04.005.
Ekman, P. E., & Davidson, R. J. (1994). The nature of emotion: Fundamental questions. Oxford: Oxford University Press.
Elkin, I., Parloff, M. B., Hadley, S. W., & Autry, J. H. (1985). NIMH treatment of Depression Collaborative Research Program: Background and research plan. Archives of General Psychiatry, 42(3), 305–316.
Endicott, J., Spitzer, R. L., Fleiss, J. L., & Cohen, J. (1976). The Global Assessment Scale: A procedure for measuring overall severity of psychiatric disturbance. Archives of General Psychiatry, 33(6), 766–771.
Engels, A. S., Heller, W., Mohanty, A., Herrington, J. D., Banich, M. T., Webb, A. G., & Miller, G. A. (2007). Specificity of regional brain activity in anxiety types during emotion processing. Psychophysiology, 44(3), 352–363. doi:10.1111/j.1469-8986.2007.00518.x.
Epstein, S. (1994). Integration of the cognitive and the psychodynamic unconscious. American Psychologist, 49(8), 709–724. doi:10.1037/0003-066X.49.8.709.
Fisher, H., Atzil-Slonim, D., Bar-Kalifa, E., Rafaeli, E., & Peri, T. (2016). Emotional experience and alliance contribute to therapeutic change in psychodynamic therapy. Psychotherapy, 53(1), 105–116. doi:10.1037/pst0000041.
Fleury, G., Fortin-Langelier, B., & Ben-Cheikh, I. (2016). The cardiac rhythm of the unconscious in a case of panic disorder. American Journal of Psychotherapy, 70(3), 277–300.
Foa, E. B., Riggs, D. S., Massie, E. D., & Yarczower, M. (1995). The impact of fear activation and anger on the efficacy of exposure treatment for posttraumatic stress disorder. Behavior Therapy, 26(3), 487–499. doi:10.1016/S0005-7894(05)80096-6.
Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: the broaden- and -build theory of positive emotions. American. Psychologist, 56, 218–226. doi:10.1037/0003-066X.56.3.218.
Garrison, A. M., Kahn, J. H., Sauer, E. M., & Florczak, M. A. (2012). Disentangling the effects of depression symptoms and adult attachment on emotional disclosure. Journal of Counseling Psychology, 59(2), 230–239. doi:10.1037/a0026132.
Gay, M. C., Bungener, C., Thomas, S., Vrignaud, P., Thomas, P. W., Baker, R., … Montreuil, M. (2017). Anxiety, emotional processing and depression in people with multiple sclerosis. BMC Neurology, 17(1), 43. doi:10.1186/s12883-017-0803-8.
Gelso, C. J., & Kanninen, K. M. (2017). Neutrality revisited: On the value of being neutral within an empathic atmosphere. Journal of Psychotherapy Integration. doi:10.1037/int0000072.
Gilbert, P. (2009). Developing a compassion-focused approach in cognitive behavioural therapy. In G. Simos (Ed.), Cognitive behaviour therapy: A guide for the practising clinician (Vol. 2, pp. 205–220). London: Routledge.
Gillanders, D., & Fleming, P. F. (2006). A test of the interacting cognitive subsystems model using a laboratory analogue of depressive interlock. Clinical Psychology & Psychotherapy, 13(5), 297–305. doi:10.1002/cpp.499.
Godfrey, E., Chalder, T., Ridsdale, L., Seed, P., & Ogden, J. (2007). Investigating the active ingredients of cognitive behaviour therapy and counselling for patients with chronic fatigue in primary care: developing a new process measure to assess treatment fidelity and predict outcome. British Journal of Clinical Psychology, 46(3), 253–272. doi:10.1348/014466506X147420.
Goldapple, K., Segal, Z., Garson, C., Lau, M., Bieling, P., Kennedy, S., & Mayberg, H. (2004). Modulation of cortical-limbic pathways in major depression: Treatment-specific effects of cognitive behavior therapy. Archives of General Psychiatry, 61(1), 34–41. doi:10.1001/archpsyc.61.1.34.
Goldfried, M. R. (2013). Evidence-based treatment and cognitive-affective-relational-behavior-therapy. Psychotherapy, 50(3), 376–380. doi:10.1037/a0032158.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: current status and future directions. Annual Review of Clinical Psychology, 6, 285–312. doi:10.1146/annurev.clinpsy.121208.131305.
Greenberg, L. (2008). Emotion and cognition in psychotherapy: The transforming power of affect. Canadian Psychology, 49(1), 49–59. doi:10.1037/0708-5591.49.1.49.
Greenberg, L. S. (2007). A guide to conducting a task analysis of psychotherapeutic change. Psychotherapy Research, 17(1), 15–30.
Greenberger, D., & Padesky, C. A. (1995). Mind over mood: Change how you feel by changing the way you think. New York: The Guilford Press.
Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. doi:10.1080/1047840X.2014.940781.
Grosse Holtforth, M., Hayes, A. M., Sutter, M., Wilm, K., Schmied, E., Laurenceau, J., & Caspar, F. (2012). Fostering cognitive-emotional processing in the treatment of depression: A preliminary investigation in exposure-based cognitive therapy. Psychotherapy and Psychosomatics; Basel, 81(4), 259–260. doi:10.1159/000336813.
Hackmann, A., Bennett-Levy, J., & Holmes, E. A. (2011). Oxford guide to imagery in cognitive therapy. Oxford: Oxford University Press. doi:10.1093/med:psych/9780199234028.001.0001.
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery & Psychiatry, 23(1), 56–62. doi:10.1136/jnnp.23.1.56.
Hart, S. L., Vella, L., & Mohr, D. C. (2008). Relationships among depressive symptoms, benefit-finding, optimism, and positive affect in multiple sclerosis patients after psychotherapy for depression. Health Psychology, 27, 230–238. doi:10.1037/0278-6133.27.2.230.
Hathaway, S. R., & McKinley, J. C. (1983). Minnesota Multiphasic Personality Inventory: Manual for administration and scoring. Minneapolis: University of Minnesoata Press.
Hauke, G., & Dall’Occhio, M. (2013). Emotional Activation Therapy (EAT): Intense work with different emotions in a cognitive behavioral setting. European Psychotherapy, 11(1), 5–29.
Hayes, A. M. (2015). Facilitating emotional processing in depression: The application of exposure principles. Current Opinion in Psychology, 4, 61–66. doi:10.1016/j.copsyc.2015.03.032.
Hayes, A. M., & Goldfried, M. R. (1996). Rating scale of therapy change processes. Unpublished Manuscript, University of Miami.
Hayes, A. M., Feldman, G. C., & Goldfried, M. R. (2006). The Change and Growth Experiences Scale: A measure of insight and emotional processing. In L. G. Castonguay & C. Hill (Eds.), Insight in psychotherapy (pp. 231–253). Washington, DC: American Psychological Association.
Hayes, A. M., Beevers, C. G., Feldman, G. C., Laurenceau, J.-P., & Perlman, C. (2005). Avoidance and processing as predictors of symptom change and positive growth in an integrative therapy for depression. International Journal of Behavioral Medicine, 12(2), 111–122. doi:10.1207/s15327558ijbm1202_9.
Hayes, A. M., & Harris, M. S. (2000). The development of an integrative treatment for depression. In S. Johnson, A. M. Hayes, T. Field, N. Schneiderman & P. McCabe (Eds.), Stress, coping, and depression (pp. 291–306). Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
*Hayes, A. M., & Strauss, J. L. (1998). Dynamic systems theory as a paradigm for the study of change in psychotherapy: An application to cognitive therapy for depression. Journal of Consulting and Clinical Psychology, 66(6), 939–947. doi:10.1037/0022-006X.66.6.939.
Hayes, A. M., Yasinski, C., Barnes, J. B., & Bockting, C. L. (2015). Network destabilization and transition in depression: New methods for studying the dynamics of therapeutic change. Clinical Psychology Review, 41, 27–39. doi:10.1016/j.cpr.2015.06.007.
Hayes, S. A., Hope, D. A., & Heimberg, R. G. (2008). The pattern of subjective anxiety during in-session exposures over the course of cognitive-behavioral therapy for clients with social anxiety disorder. Behavior Therapy, 39(3), 286–299. doi:10.1016/j.beth.2007.09.001.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2011). Acceptance and commitment therapy: The process and practice of mindful change. New York: The Guilford Press.
Hendricks, M. N. (2007). The role of experiencing in psychotherapy: Attending to the “bodily felt sense” of a problem makes any orientation more effective. Journal of Contemporary Psychotherapy, 37(1), 41–46. doi:10.1007/s10879-006-9033-x.
Hofmann, S. G., Sawyer, A. T., Fang, A., & Asnaani, A. (2012). Emotion dysregulation model of mood and anxiety disorders. Depression and Anxiety, 29(5), 409–416. doi:10.1002/da.21888.
Hollon, S. D., DeRubeis, R. J., Evans, M. D., Wiemer, M. J., Garvey, M. J., Grove, W. M., & Tuason, V. B. (1992). Cognitive therapy, pharmacotherapy and combined cognitive-pharmacotherapy in the treatment of depression. Archives of General Psychiatry, 49, 774–781.
Holmes, E. A., & Mathews, A. (2010). Mental imagery in emotion and emotional disorders. Clinical Psychology Review, 30(3), 349–362. doi:10.1016/j.cpr.2010.01.001.
Honkalampi, K., Hintikka, J., Laukkanen, E., & Viinamäki, J. L. H. (2001). Alexithymia and depression: A prospective study of patients with major depressive disorder. Psychosomatics, 42(3), 229–234. doi:10.1176/appi.psy.42.3.229.
Horvath, A. O., & Greenberg, L. (1986). The development of the Working Alliance Inventory: A research handbook. New York: Guildford Press.
Jones, E. E. (2000). Psychotherapy process Q-set (PQS). Therapeutique Action. Northvale, NJ: Jason Aronson Inc.
*Jones, E. E., & Pulos, S. M. (1993). Comparing the process in psychodynamic and cognitive-behavioral therapies. Journal of Consulting and Clinical Psychology, 61(2), 306–316. doi:10.1037/0022-006X.61.2.306.
Kaiser, R. H., Andrews-Hanna, J. R., Spielberg, J. M., Warren, S. L., Sutton, B. P., Miller, G. A., … Banich, M. T. (2015). Distracted and down: Neural mechanisms of affective interference in subclinical depression. Social Cognitive and Affective Neuroscience, 10(5), 654–663. doi:10.1093/scan/nsu100.
Kazantzis, N., Tee, J. M., Dattilio, F. M., & Dobson, K. S. (2013). How to develop collaborative empiricism in cognitive behavior therapy: Conclusions from the C&BP special series. Cognitive and Behavioral Practice, 20(4), 455–460. doi:10.1016/j.cbpra.2013.03.005.
Kennedy-Moore, E., & Watson, J. C. (2001). How and when does emotional expression help? Review of General Psychology, 5(3), 187–212. doi:10.1037/1089-2680.5.3.187.
Klein, M. (1969). The Experiencing Scale: A research and training manual. Madison: Wisconsin Psychiatric Institute.
Klein, M. H., Coughlan, P. M., & Kiesler, D. J. (1986). The psychotherapeutic process: a research handbook. New York: Guildford Press.
Lambert, M. J., Burlingame, G. M., Umphress, V., Hansen, N. B., Vermeersch, D. A., Clouse, G. C., & Yanchar, S. C. (1996). The reliability and validity of the Outcome Questionnaire. Clinical Psychology & Psychotherapy, 3(4), 249–258. doi:10.1002/(SICI)1099-0879(199612)3:4<249::AID-CPP106>3.3.CO;2-J.
Lane, R. D., Ryan, L., Nadel, L., & Greenberg, L. (2015). Memory reconsolidation, emotional arousal, and the process of change in psychotherapy: New insights from brain science. Behavioral and Brain Sciences, 38, 1–64. doi:10.1017/S0140525X14000041.
Lau, M. A., & Grabovac, A. D. (2009). Mindfulness-based interventions: Effective for depression and anxiety: Evidence supports adjunctive role for the combination of meditative practices and CBT. Current Psychiatry, 8(12), 39–55.
Leahy, R. L. (2015). Emotional schema therapy. New York: The Guilford Press.
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gotzsche, P. C., Ioannidis, J., … Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Annals of Internal Medicine, 151(4), 1–18. doi:10.7326/0003-4819-151-4-200908180-00136.
Lindahl, M., & Archer, T. (2013). Depressive expression and anti-depressive protection in adolescence: stress, positive affect, motivation and self-efficacy. Psychology, 4, 495–505. doi:10.4236/psych.2013.46070.
Linehan, M. M. (2015). DBT skills training manual. New York: Guilford Publications.
Llewelyn, S., Macdonald, J., & Aafjes-van Doorn, K. (2016). Process–outcome studies. In J. Norcross (Ed.), Handbook of clinical psychology (pp. 451–463). Worcester: American Psychological Association. doi:10.1037/14773-020.
Lorenzo-Luaces, L., German, R. E., & DeRubeis, R. J. (2015). It’s complicated: The relation between cognitive change procedures, cognitive change, and symptom change in cognitive therapy for depression. Clinical Psychology Review, 41, 3–15. doi:10.1016/j.cpr.2014.12.003.
Lorenzo-Luaces, L., Keefe, J. R., & DeRubeis, R. J. (2016). Cognitive-behavioral therapy: Nature and relation to non-cognitive behavioral therapy. Behavior Therapy, 47(6), 785–803. doi:10.1016/j.beth.2016.02.012.
Mackay, H. C., Barkham, M., & Stiles, W. B. (1998). Staying with the feeling: An anger event in psychodynamic–interpersonal therapy. Journal of Counseling Psychology, 45(3), 279–289.
*Mackay, H. C., Barkham, M., Stiles, W. B., & Goldfried, M. R. (2002). Patterns of client emotion in helpful sessions of cognitive-behavioral and psychodynamic-interpersonal therapy. Journal of Counseling Psychology, 49(3), 376–380. doi:10.1037/0022-0167.49.3.376.
McCullough, L., Bhatia, M., Ulvenes, P., Berggraf, L., & Osborn, K. (2011). Learning how to rate video-recorded therapy sessions: A practical guide for trainees and advanced clinicians. Psychotherapy, 48(2), 127–137.
McCullough, L., Kuhn, N., Andrews, S., Kaplan, A., Wolf, J., & Lanza Hurley, C. (2003). Treating affect phobia: A manual for short-term dynamic psychotherapy. New York: The Guilford Press.
Millgram, Y., Joormann, J., Huppert, J. D., & Tamir, M. (2015). Sad as a matter of choice? Emotion-regulation goals in depression. Psychological Science, 26(8), 1216–1228. doi:10.1177/0956797615583295.
Montagno, M., Svatovic, M., & Levenson, H. (2011). Short-term and long-term effects of training in emotionally focused couple therapy: Professional and personal aspects. Journal of Marital and Family Therapy, 37(4), 380–392. doi:10.1111/j.1752-0606.2011.00250.x.
Ogden, P., Minton, K., & Pain, C. (2006). Hierarchical information processing: Cognitive, emotional and sensorimotor dimensions. In P. Ogden, K. Minton & C. Pain (Eds.), Trauma and the body: A sensorimotor approach to psychotherapy (pp. 1–50). New York: Norton & Company.
Panksepp, J. (2007). Neurologizing the psychology of affects: How appraisal-based constructivism and basic emotion theory can coexist. Perspectives on Psychological Science, 2(3), 281–296. doi:10.1111/j.1745-6916.2007.00045.x.
Pascual-Leone, A., & Greenberg, L. S. (2007). Emotional processing in experiential therapy: Why “the only way out is through.” Journal of Consulting and Clinical Psychology, 75(6), 875–887. doi:10.1037/0022-006X.75.6.875.
Porter, R. J., Bourke, C., Carter, J. D., Douglas, K. M., McIntosh, V. V. W., Jordan, J., … Frampton, C. M. A. (2016). No change in neuropsychological dysfunction or emotional processing during treatment of major depression with cognitive–behaviour therapy or schema therapy. Psychological Medicine, 46(2), 393–404. doi:10.1017/S0033291715001907.
Prosser, M., & Watson, J. C. (2007). The relationship of affect regulation to outcome in the treatment of depression. In 22nd annual conference of the Society for the Exploration of Psychotherapy Integration. Lisbon, Portugal.
Ritchey, M., Dolcos, F., Eddington, K. M., Strauman, T. J., & Cabeza, R. (2011). Neural correlates of emotional processing in depression: Changes with cognitive behavioral therapy and predictors of treatment response. Journal of Psychiatric Research, 45(5), 577–587. doi:10.1016/j.jpsychires.2010.09.007.
*Rudkin, A., Llewelyn, S., Hardy, G., Stiles, W. B., & Barkham, M. (2007). Therapist and client processes affecting assimilation and outcome in brief psychotherapy. Psychotherapy Research, 17(5), 613–621. doi:10.1080/10503300701216298.
Ryle, A., & Kerr, I. B. (2003). Introducing cognitive analytic therapy: Principles and practice. Chichester: Wiley.
Safran, J. D. (1998). Widening the scope of cognitive therapy: The therapeutic relationship, emotion, and the process of change. Northvale. Lanham, NJ: Jason Aronson Incorporated.
Salgado, J., Meira, L., Santos, A., Cunha, C., Bento, T., Almeida, C., … Pinheiro, P. (2010). Protocolo clínico para investigação: adaptação do manual de terapia cognitivo-comportamental para a depressão. Unpublished manuscript.
Samoilov, A., & Goldfried, M. R. (2000). Role of emotion in cognitive-behavior therapy. Clinical Psychology: Science and Practice, 7(4), 373–385. doi:10.1093/clipsy.7.4.373.
Sassaroli, S., Brambilla, R., Cislaghi, E., Colombo, R., Centorame, F., Veronese, G., … Ruggiero, G. M. (2015). Emotion-abstraction patterns and cognitive interventions in a single case of standard cognitive-behavioral therapy. Research in Psychotherapy: Psychopathology, Process and Outcome, 17(2), 65–72. doi:10.4081/ripppo.2014.146.
Schanche, E., Høstmark Nielsen, G., McCullough, L., Valen, J., & Mykletun, A. (2010). Training graduate students as raters in psychotherapy process research: Reliability of ratings with the achievement of therapeutic objectives scale (ATOS). Nordic Psychology, 62(3), 4–20. doi:10.1027/1901-2276/a000013.
Schumacher, S., Gaudlitz, K., Plag, J., Miller, R., Kirschbaum, C., Fehm, L., … Ströhle, A. (2014). Who is stressed? A pilot study of salivary cortisol and alpha-amylase concentrations in agoraphobic patients and their novice therapists undergoing in vivo exposure. Psychoneuroendocrinology, 49, 280–289. doi:10.1016/j.psyneuen.2014.07.016.
Schumacher, S., Miller, R., Fehm, L., Kirschbaum, C., Fydrich, T., & Ströhle, A. (2015). Therapists’ and patients’ stress responses during graduated versus flooding in vivo exposure in the treatment of specific phobia: A preliminary observational study. Psychiatry Research, 230(2), 668–675. doi:10.1016/j.psychres.2015.10.020.
Scott, W. D., & Ingram, R. E. (1998). Affective influences in depression: Conceptual issues, cognitive consequences, and multiple mechanisms. In W. F. Flack & J. D. Laird (Eds.), Emotions in psychopathology: Theory and research (pp. 200–215). New York: Oxford University Press.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2012). Mindfulness-based cognitive therapy for depression. New York: Guilford Press.
Shapiro, D. A., Barkham, M., Rees, A., Hardy, G. E., Reynolds, S., & Startup, M. (1994). Effects of treatment duration and severity of depression on the effectiveness of cognitive-behavioral and psychodynamic-interpersonal psychotherapy. Journal of Consulting and Clinical Psychology, 62(3), 522.
Shrout, P. E., & Fleiss, J. L. (1979). Intraclass correlations: uses in assessing rater reliability. Psychological Bulletin, 86(2), 420–428. doi:10.1037/0033-2909.86.2.420.
Stewart, R. E., & Chambless, D. L. (2007). Does psychotherapy research inform treatment decisions in private practice? Journal of Clinical Psychology, 63(3), 267–281. doi:10.1002/jclp.20347.
Stiles, W. B. (2002). Session Evaluation Questionnaire: Structure and use. Oxford: Miami University.
Stiles, W. B., Elliott, R., Llewelyn, S. P., Firth-Cozens, J. A., Margison, F. R., Shapiro, D. A., & Hardy, G. (1990). Assimilation of problematic experiences by clients in psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 27(3), 411–420.
Stiles, W. B., Morrison, L. A., Haw, S. K., Harper, H., Shapiro, D. A., & Firth-Cozens, J. (1991). Longitudinal study of assimilation in exploratory psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 28(2), 195–206. doi:10.1037/0033-3204.28.2.195.
*Stringer, J. V., Levitt, H. M., Berman, J. S., & Mathews, S. S. (2010). A study of silent disengagement and distressing emotion in psychotherapy. Psychotherapy Research, 20(5), 495–510. doi:10.1080/10503301003754515.
Strunk, D. R., Adler, A. D., & Hollon, S. D. (2017). Cognitive therapy of depression. In R. J. DeRubeis & D. R. Strunk (Eds.), The Oxford handbook of mood disorders (pp. 411–422). Oxford: Oxford University Press.
Subic-Wrana, C., Greenberg, L. S., Lane, R. D., Michal, M., Wiltink, J., & Beutel, M. E. (2016). Affective change in psychodynamic psychotherapy: Theoretical models and clinical approaches to changing emotions. Zeitschrift Für Psychosomatische Medizin Und Psychotherapie, 62(3), 207–223.
Tambs, K., & Moum, T. (1993). How well can a few questionnaire items indicate anxiety and depression? Acta Psychiatrica Scandinavica, 87(5), 364–367.
Teasdale, J. D. (1996). Clinically relevant theory: Integrating clinical insight with cognitive science. In P. M. Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 26–47). New York: The Guilford Press.
Teasdale, J. D. (1999). Emotional processing, three modes of mind and the prevention of relapse in depression. Behaviour Research and Therapy, 37, S53–S77. doi:10.1016/S0005-7967(99)00050-9.
Teasdale, J. D., & Chaskalson, M. (2011). How does mindfulness transform suffering? II: the transformation of dukkha. Contemporary Buddhism, 12(1), 103–124. doi:10.1080/14639947.2011.564826.
Thoma, N. C., & McKay, D. (2015). Working with emotion in cognitive-behavioral therapy: Techniques for clinical practice. New York: The Guilford Press.
Town, J. M., Hardy, G. E., McCullough, L., & Stride, C. (2012). Patient affect experiencing following therapist interventions in short-term dynamic psychotherapy. Psychotherapy Research, 22(2), 208–219. doi:10.1080/10503307.2011.637243.
Ulvenes, P. G., Berggraf, L., Wampold, B. E., Hoffart, A., Stiles, T., & McCullough, L. (2014). Orienting patient to affect, sense of self, and the activation of affect over the course of psychotherapy with cluster C patients. Journal of Counseling Psychology, 61(3), 315–324. doi:10.1037/cou0000028.
van Doorn, K., McManus, F., & Yiend, J. (2012). An analysis of matching cognitive-behavior therapy techniques to learning styles. Journal of Behavior Therapy and Experimental Psychiatry, 43(4), 1039–1044. doi:10.1016/j.jbtep.2012.05.001.
Vyskocilova, J., & Prasko, J. (2012). Emotional processing strategies in cognitive behavioral therapy. Activitas Nervosa Superior Rediviva, 54(4), 150–158.
Warwar, S., & Greenberg, L. S. (1999). Client emotional arousal scale–III. Unpublished Manuscript. Toronto: York University.
*Watson, J. C., & Bedard, D. L. (2006). Clients’ emotional processing in psychotherapy: A comparison between cognitive-behavioral and process-experiential therapies. Journal of Consulting and Clinical Psychology, 74(1), 152–159. doi:10.1037/0022-006X.74.1.152.
Watson, J. C., & Prosser, M. (2004). Observer-rated measure of affect regulation (O-MAR). Unpublished manuscript. Toronto: Ontario Institute for Studies in Education of the University of Toronto.
Watson, J. C., Gordon, L. B., Stermac, L., Kalogerakos, F., & Steckley, P. (2003). Comparing the effectiveness of process-experiential with cognitive-behavioral psychotherapy in the treatment of depression. Journal of Consulting and Clinical Psychology, 71(4), 773. doi:10.1037/0022-006X.71.4.773.
*Watson, J. C., McMullen, E. J., Prosser, M. C., & Bedard, D. L. (2011). An examination of the relationships among clients’ affect regulation, in-session emotional processing, the working alliance, and outcome. Psychotherapy Research, 21(1), 86–96. doi:10.1080/10503307.2010.518637.
Westbrook, D., & Kirk, J. (2005). The clinical effectiveness of cognitive behaviour therapy: Outcome for a large sample of adults treated in routine practice. Behaviour Research and Therapy, 43(10), 1243–1261. doi:10.1016/j.brat.2004.09.006.
Whelton, W. J. (2004). Emotional processes in psychotherapy: Evidence across therapeutic modalities. Clinical Psychology & Psychotherapy, 11(1), 58–71. doi:10.1002/cpp.392.
White, J. (2008). CBT and the challenge of primary care: Developing effective, efficient, equitable, acceptable and accessible services for common mental health problems. Journal of Public Mental Health, 7(1), 32–41. doi:10.1108/17465729200800006.
Wiles, N., Thomas, L., Abel, A., Barnes, M., Carroll, F., Ridgway, N., … Metcalfe, C. (2014). The prevalence of treatment-resistant depression in primary care. Health Technology Assessment, No. 18.31. Southampton (UK): NIHR Journals Library. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK261988/.
*Wiser, S. L., & Goldfried, M. R. (1993). Comparative study of emotional experiencing in psychodynamic-interpersonal and cognitive-behavioral therapies. Journal of Consulting and Clinical Psychology, 61(5), 892–895. doi:10.1037/0022-006X.61.5.892.
Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema therapy: A practitioner’s guide. New York: The Guilford Press. doi:10.1016/j.jct.2003.07.002.
Funding
This review did not use any external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Katie Aafjes-van Doorn and Jacques P. Barber declares that they have no conflict of interest.
Human and Animal Rights
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed Consent
This review did not require any informed consent.
Appendices
Appendix A
Detailed Description of the Database Searches
The literature review was conducted using the following databases: ScienceDirect, ERIC, SocINDEX, MEDLINE, PsychInfo, Academic Search Complete, ProQuest Central, PsycArticles and Scopus. Search terms included variations on the terms for: (a) in-session affective experiencing (emotion*, affect*, feeling, experien*, process*, in-session, within-session), (b) cognitive behavioral therapy (cognitive therapy, cognitive behavio* therapy, CBT), and (c) depress*.
The search was conducted on abstracts of peer-reviewed journals with ‘AND’ entered into the database search to link the different categories (a, b and c) of search terms. This means that 21 separate searches were conducted for all the variations of the terms for in-session affective experiencing (a), as well as for all the terms for cognitive behavioral therapy (b):
-
1.
(a) Emotion* AND (b) cognitive therapy AND (c) depress*
-
2.
(a) Affect* AND (b) cognitive therapy AND (c) depress*
-
3.
(a) Feeling AND (b) cognitive therapy AND (c) depress*
-
4.
(a) Experien* AND (b) cognitive therapy AND (c) depress*
-
5.
(a) process* AND (b) cognitive therapy AND (c) depress*
-
6.
(a) In-session AND (b) cognitive therapy AND (c) depress*
-
7.
(a) Within-session AND (b) cognitive therapy AND (c) depress*
-
8.
(a) Emotion* AND (b) cognitive behavio* therapy AND (c) depress*
-
9.
(a) Affect* AND (b) cognitive behavio* therapy AND (c) depress*
-
10.
(a) Feeling AND (b) cognitive behavio* therapy AND (c) depress*
-
11.
(a) Experien* AND (b) cognitive behavio* therapy AND (c) depress*
-
12.
(a) Process* AND (b) cognitive behavio* therapy AND (c) depress*
-
13.
(a) In-session AND (b) cognitive behavio* therapy AND (c) depress*
-
14.
(a) Within-session AND (b) cognitive behavio* therapy AND (c) depress*
-
15.
(a) Emotion* AND (b) CBT AND (c) depress*
-
16.
(a) Affect* AND (b) CBT AND (c) depress*
-
17.
(a) Feeling AND (b) CBT AND (c) depress*
-
18.
(a) Experien* AND (b) CBT AND (c) depress*
-
19.
(a) Process* AND (b) CBT AND (c) depress*
-
20.
(a) In-session AND (b) CBT AND (c) depress*
-
21.
(a) Within-session AND (b) CBT AND (c) depress*
Appendix B
Measurements of AE
Operationalization of AE
The reviewed studies used different measures to operationalize different aspects of AE, focusing on its intensity, mixed cognitive-affective process (e.g. affective exploration) or a sole affective process (expressed bodily arousal or inhibition), with either positive and/or negative valence.
Intensity of Cognitive-Affective Process
The intensity of the patient’s AE in-session was measured by three process measures, whereby AE was conceptualized as an integrated cognitive-affective process. For example, the Experiencing scale (EXP; Klein et al. 1986), which appeared the AE measure with the most robust psychometrics, was used by five studies to measure the patient’s depth of moment-to-moment processing during the therapy hour. Patient statements are rated on a 7-point scale in terms of the extent to which they talk about or use their affective experience as a referent during therapy, and explore and reflect on their inner experience to achieve self-understanding and problem resolution (Klein et al. 1986). Studies differed in the timeframe they used for coding the EXP; rating patient’s AE every minute (e.g. Wiser and Goldfried 1993), per 10-minute segment (e.g. Castonguay et al. 1996), per 20-minute segment (e.g. Watson et al. 2006), session excerpts (e.g. Rudkin et al. 2007). The authors report on the construct validity of the EXP as well as its predictive validity in emotion-focused treatments, with published interrater reliability coefficients ranging from 0.76 to 0.91, with rating-rerating correlation coefficients around 0.80 (Klein et al. 1986). In their respective studies, the authors report interrater reliabilities in the good (e.g. CCI of 0.73 and higher in Watson and Bedard 2006) or excellent range (e.g., CCI of 0.83 in Rudkin et al. 2007; 0.88 in; Castonguay et al. 1996).
In addition to the EXP, Watson et al. (2011) also measured the intensity of patient’s in-session emotional processing (which includes cognitive and affective aspects) on the Observer-Rated Measure of Affect Regulation (O-MAR; Watson and Prosser 2004), whereby observers rated the patient’s (1) Level of Awareness, (2) Modulation of Arousal, (3) Modulation of Expression, (4) Acceptance of Affective Experience, and (5) Reflection on Experience on a 7-point Likert scale. They report on preliminary evidence of internal consistency, and construct and predictive validity (Prosser and Watson 2007) as well as significant interrater reliabilities in their early sessions (ICC = 0.78) and late sessions (ICC = 0.87).
The CHANGE rating scale (Hayes et al. 2006) is an observational coding system designed to measure the frequency and extent of change processes in psychotherapy on a 4-point Likert scale. Previous research indicates good interrater agreement and predictive validity for common disorders, including depression (Adler et al. 2013). Its ‘Emotional Processing’ subscale was used by Abel et al. (2016) to score the overall session on patient insight into and exploration of emotional experiences and affective arousal. They reported good interrater agreement on the raw scores for this subscale for all sessions that were coded after training (ICC = 0.80).
Intensity and Valence of Cognitive-Affective Process
Two AE measures that also conceptualized AE as an integrated cognitive-affective process, extended the measurement of AE intensity by including a rating of valence of the affect. For example, in the Assimilation of Problematic Experiences Scale (APES; Stiles et al. 1991), used by Rudkin et al. (2007) and Basto et al. (2016), raters rated the overall (non) verbal patient expressions per session, based on the assimilation model (Stiles 2002; Stiles et al. 1990). The APES describes the relation of an identified problematic experience to the rest of the patient’s presentation on a spectrum from negative to positive valence and intensity on an 8-point Likert scale ranging from warded off/dissociated, and understanding/ insight, to integration/mastery. The other AE measure that also rated the valence of the affect was the rating scale of Therapy Change Processes (TCP; Hayes and Goldfried 1996), used by Hayes and Strauss (1998) to code each session on different subscales of therapist intervention and patient reaction on a 3-point Likert scale. The patient-reaction subscales on Affective intensity and Destabilization both cover negative AE. Affective intensity was measured as the degree of discomfort (non) verbally expressed by the patient in the session when addressing therapeutic issues. Destabilization was defined as the extent of variability or turbulence in somatic, behavioral, cognitive, and affective functioning, and included signs of emotional distress, anxiety, panic, or the emergence of new emotions. Hayes and Goldfried do not report psychometric properties but do report on the estimates of agreement on the coding categories between two raters in their study (ranging from 0.78 to 0.90), as well as the modal agreement for categories (0.82).
Intensity and Valence of Affective Process
The four other measures not only considered the valence of the affect but also measured AE as a purely affect-related process. For example, the Client Emotional Arousal Scale—III (CEAS-III; Warwar and Greenberg 1999) was used by Basto et al. (2016) to assess the valence and intensity of patient emotions, in multiple passages of text within the session. In each identified emotional passage of the transcript, the patient’ s primary emotion was identified and coded for its intensity on a 7-point Likert scale (modal and peak emotional arousal) and its negative (pain/hurt; sadness; hopelessness/helplessness; loneliness; anger/resentment; contempt/disgust; fear/anxiety; shame/guilt, anger and sadness); or positive valence (love; joy/excitement; contentment/calm/ relief; pride/self-confidence). They report previously established interrater reliability coefficients of 0.70 for modal and of 0.73 for peak arousal ratings on the CEAS-III but do not report on its validity.
Another measure of intensity and valence of affective process is the Psychotherapy Process Q-sort (PQS, Jones 2000). The PQS is rated by clinical judges and yields a score from 1 to 9, from extremely characteristic to extremely un characteristic for a given transcribed treatment session, for each of 100 items describing the patient’ s attitudes, behaviors, or experience; the therapist’ s actions and attitudes; and the nature of their interaction. Although the reviewed studies report good construct and discriminant validity of the PQS, and high interrater reliability among 2 raters (0.82 in Coombs et al. 2012; 0.83 in Ablon and Jones 1999; 0.84 in; Jones and Pulos 1993), this referred to the PQS scores of all 100 items. The reported interrater reliability at the individual Q-item level was diverse, ranging from 0.50 to 0.90, however, it was unclear which items had the low reliability ratings. This is concerning, because the three studies that used the Process Q-set to measure AE, did not use this total score and reported on different combinations of items. For example, Coombs et al. (2012) identified two factors of negative affect in their factor analyses, labeled ‘Patient Painful Affect’ (composed of the PQS items: Patient experiences discomforting or troublesome (painful) affect, & Patient is anxious and tense, & Patient struggles to control feelings or impulses), and ‘Patient Inhibition’ (items: Patient feels shy or embarrassed, & Patient does not express anger, & Patient is unanimated or unexcited). Coombs and colleagues also identified a factor of positive emotions labeled ‘Collaborative Emotional Exploration’ (which amongst other cognitive items includes the affective items: Level of catharsis of the patient, &, Patient does not feel wary or suspicious), items also reported on by Ablon and Jones. (1999). Jones and Pulos (1993) also used items from the Process Q set but looked at negative emotions only. They conceptualized a factor (without reporting on the factor analysis) of ‘Negative Patient Affect’ reflecting the extent to which patients felt depressed and anxious or experienced other troublesome affect during therapy sessions (based on the items: Patient feels sad or depressed & Patient feels inadequate and inferior & Patient experiences discomforting or painful affect, & Patient is self-accusatory; expresses shame or guilt & Patient is anxious or tense). Ablon and Jones (1999) did not report on one factor but also reported on these same individual items of negative expressed emotions.
Also, Mackay et al. (2002) measured the patients’ emotional tone (its valence and intensity of the affective process), for one session of each patient using their protocol (Mackay et al. 1998). Observers in their study rated audiotapes and transcripts for each sentence of patient speech on the dimension of pleasure-displeasure (How pos/neg is the patient’s emotion in this sentence?) and the dimension of arousal (What is the level of activation of the patient’s emotion in this sentence?) on a 9-point Likert scale. Although no psychometric properties of these items were reported, and these dimensions were not used in other studies previously, raters established sufficient inter-rater reliability on the two dimensions (ICC of 0.76 for pleasure and 0.75 for arousal).
Negative Valence of Affective Process
Furthermore, the only study that used a self-report measure (Stringer et al. 2010), to measure the intensity and negative valence of affective process, used the Negative Emotions Subscale of the Emotional Arousal Session Report Measure (EASRM; Warwar and Greenberg 2002). At the end of the third session, patients were asked to indicate on a 7-point Likert scale the extent to which they felt the negative emotions: (a) emotional pain, (b) sadness, (c) helplessness, and (d) hopelessness) during session. These four items had an inter-item reliability of 0.81 at the third or fourth session and 0.89 at the final session in their dataset. According to the authors the subscale demonstrated high construct validity and appears to be a reliable measure of negative emotion.
Observer-Ratings of AE
Despite using multiple raters and establishing sufficient reliability across raters, with intraclass correlations of 0.70 and higher (defined as ‘good’ by Shrout and Fleiss 1979), the exact training procedures for the raters remained unclear in most of the twelve observer-rated studies. Ablon and Jones (1999), for example, reported that all raters were trained in the use of the Q technique and Castonguay et al. (1996) mentioned that the coders received 60 h of training but did not report on formal training procedures or criterion scores of training tapes of established expert benchmarked ratings. Also, Basto et al. (2016), simply reported that when raters reached consensus and mastered the coding of the CEAS-III they were given the sessions to code. This means that although raters might agree with each other (high ICC), they might both have misinterpreted the item. Wiser and Goldfried (1993) addressed this concern by reporting mean reliability with the manual criterion (ICC of 0.80). The training procedures reported by Abel et al. (2016), appeared to be most robust, as it included practice of pre-rated training and criterion sessions that continued until interrater reliability of ICC 0.80 was achieved on all items in the criterion coding, as well as regular supervision meetings between the coders and scale authors to review discrepancies and prevent rater drift.
Rights and permissions
About this article

Cite this article
Aafjes-van Doorn, K., Barber, J.P. Systematic Review of In-Session Affect Experience in Cognitive Behavioral Therapy for Depression. Cogn Ther Res 41, 807–828 (2017). https://doi.org/10.1007/s10608-017-9865-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-017-9865-6