
Abstract
Previous studies have shown an association between eating disorder symptoms and both negative affect and avoidance-based emotion regulation strategies among women and men. The purpose of this study was to examine the relationship between the cognitive emotion regulation strategy of thought suppression and eating disorder symptoms in the understudied population of men. Two-hundred ninety-six undergraduate men completed a series of questionnaires including the Positive and Negative Affect Schedule, the White Bear Suppression Inventory, and the Eating Disorder Examination-Questionnaire. Results supported an association between chronic thought suppression and both global and specific eating disorder symptoms (shape concern, weight concern, eating concern, and, to a lesser extent, restraint) among men. Further, thought suppression was found to fully mediate the relationships between negative affect and both global eating disorder symptoms and the specific eating disorder symptom of shape concern, and to partially mediate the relationship between negative affect and the eating disorder symptoms of eating and weight concerns. These findings suggest that chronic efforts to suppress unpleasant or unwanted thoughts may be one avoidance strategy that underlies the relationship between the experience of negative affect and eating disorder symptoms in men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although the prevalence of eating disorders (e.g., anorexia nervosa and bulimia nervosa) is higher among women than men, men comprise a substantial minority of eating disorder populations (American Psychiatric Association 2000) and have been the focus of a growing number of studies in this area. Overall, findings suggest that men and women tend to be more similar than dissimilar with respect to core eating disorder symptoms (Braun et al. 1999; Carlat et al. 1997; Olivardia et al. 1995). In addition to research on men with full-threshold eating disorders, studies have examined individual eating disorder symptoms and sub-threshold eating disorder presentations among men. For example, Striegel-Moore et al. (2009) examined the prevalence of eating disorder behaviors during the previous 3 months in a random sample of men ages 18–35 recruited through a health maintenance organization. Within the sample, 8% reported engaging in one eating binge each week on average, 4% endorsed fasting, 3% endorsed laxative misuse, and 1.5% endorsed self-induced vomiting. In sum, findings suggest that eating disorder symptoms are a concern for men and highlight the need for further research in this area.
Negative Affect
Although researchers have developed several related theoretical models to explain the pathogenesis of eating disorder symptoms (e.g., the escape theory of binge eating, which posits that the narrowing of attention that occurs during an episode of binge eating provides escape from aversive self-perceptions; Heatherton and Baumeister 1991), one of the most widely studied is the affect regulation model, which conceptualizes eating disorder symptoms as maladaptive efforts to cope with or avoid aversive emotional experiences (e.g., Arnow et al. 1992; Polivy and Herman 1993). Central to this model is the experience of negative affect, which has been identified as a risk factor for eating disorders and a maintenance factor for binge eating among individuals with an eating disorder (Stice 2002). Numerous studies have revealed an association between various indices of negative affect and eating disorder symptoms in males. For example, Keel et al. (1998) found that negative emotionality was associated with disordered eating in a sample of adolescent boys. Similarly, in a sample of late elementary school boys, Pearson et al. (2010) found that the expectation that eating will relieve negative affect was associated with binge eating and purging behaviors. Research has also shown that co-occurring affective disorders are common among men diagnosed with an eating disorder (Olivardia et al. 1995; Woodside et al. 2001). Collectively, these findings suggest that the experience of negative affect may play an important role in eating disorder symptoms among men.
Thought Suppression
Although the affect regulation model views negative affect as a primary factor in the pathogenesis of eating disorders, studies have also revealed that the related construct of emotion dysregulation is associated with eating disorder symptoms in both men and women (e.g., Gupta et al. 2008; Whiteside et al. 2007). Specifically, the findings of these studies suggest that more difficulties in emotion regulation are associated with greater eating disorder symptoms. These findings are theoretically consistent with the affect regulation model, in that individuals who are more emotionally dysregulated may be more likely to engage in eating disorder behaviors as maladaptive efforts to cope with aversive affective states. Therefore, both the experience of negative affect in and of itself and related efforts to regulate or avoid aversive emotional states may be important to consider in affect regulation-based conceptualizations of eating disorder symptoms.
One cognitive emotion regulation strategy that has received substantial attention in the literature in relation to various forms of psychopathology is thought suppression (Aldao and Nolen-Hoeksema 2010; Purdon 1999). Although sometimes effective in reducing distress in the short-term, research suggests that thought suppression is ultimately ineffective due to the tendency for suppression efforts to produce a paradoxical increase in the unwanted thoughts (Wegner et al. 1987). Prior research has shown that chronic thought suppression is associated with a variety of affective disorders (Purdon 1999). However, its relation to global eating disorder symptoms requires further elaboration.
Experimental studies examining the short- and long-term effects of suppressing thoughts relevant to eating disorders (e.g., food- and weight-related cognitions) on a number of outcomes, including subsequent thoughts, eating behaviors, and body weight (Harnden et al. 1997; Johnston et al. 1999; O’Connell et al. 2005; Oliver and Huon 2001), have produced inconsistent results. Johnston et al. (1999) found that both chocolate cravers and noncravers were able to effectively suppress chocolate-related thoughts when given instructions to do so. In contrast, O’Connell et al. (2005) found that individuals high in dietary restraint experienced more food and eating-related thoughts after receiving suppression instructions. More recently, Erskine and Georgiou (2010) found that restrained eaters given instructions to suppress thoughts about chocolate consumed significantly more chocolate than restrained eaters in an expression or control condition.
Other studies have assessed the relationship between specific eating disorder symptoms and the tendency to suppress thoughts more generally. For example, Soetens et al. (2008) found that a tendency to engage in thought suppression was associated with higher levels of dietary restraint and disinhibition among adolescent boys and girls. Further, higher levels of thought suppression have been shown to be uniquely associated with greater bulimic symptoms among both male and female undergraduates (Lavender et al. 2009). However, the literature on the association between generalized chronic thought suppression and global eating disorder symptoms among men remains limited. Furthermore, no studies have examined the extent to which thought suppression mediates the association between negative affect and eating disorder symptoms among men, a hypothesized relationship that is consistent with the affect regulation model of eating disorders. Given evidence that thought suppression mediates the relationship between negative affect and a variety of other clinical difficulties (including general psychological distress, borderline personality disorder symptoms, and posttraumatic stress disorder; see Lynch et al. 2001; Rosenthal et al. 2005, 2006), however, an extension of this research to eating disorder symptoms is both theoretically consistent and clinically relevant.
Current Study
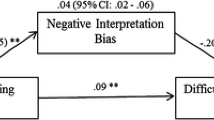
Although prominent theories of the pathogenesis of eating disorders focus on the central role of emotional and/or cognitive avoidance in the development and maintenance of eating disorder symptoms (e.g., escape theory; Heatherton and Baumeister 1991), few studies have assessed the relationship between eating disorder symptoms and the tendency to engage in generalized thought suppression, particularly among men. Therefore, the purpose of the present investigation was to conduct a preliminary examination of the associations between chronic thought suppression, negative affect, and eating disorder symptoms among a non-clinical sample of men. Specifically, the first goal of this study was to examine the unique association between thought suppression (conceptualized as an avoidant cognitive emotion regulation strategy) and global eating disorder symptoms among men, replicating previous findings of an association between thought suppression and bulimic symptoms among men. The second goal was to examine thought suppression as a potential mediator of the relationship between negative affect and both global and specific eating disorder symptoms (see Fig. 1). It was hypothesized that (a) thought suppression would be uniquely associated with global eating disorder symptoms after accounting for body mass index (BMI) and negative affect, and (b) thought suppression would fully mediate the relationship between negative affect and both global eating disorder symptoms and the four specific eating disorder symptoms of restraint, eating concern, shape concern, and weight concern in the current sample of men.

Proposed mediational model depicting total (c), direct (c′), and indirect effects (a × b) of negative affect on eating disorder symptoms
Method
Participants
Two hundred ninety-six undergraduate men from a large public university in the Northeast participated in this study for course credit. The mean (SD) age for participants was 18.9 (1.4) years and the mean (SD) BMI of the sample was 25.4 (4.2) kg/m2. The ethnic breakdown of the sample was as follows: 66.9% White, 11.5% African American, 7.8% Hispanic, 6.8% Asian, and 7.1% other.
Measures
Body Mass Index (BMI)
Research assistants measured the height and weight of each participant. BMI was calculated based on the following formula, in which weight is measured in kilograms and height is measured in meters: (weight/height2).
Positive and Negative Affect Schedule (PANAS; Watson et al. 1988)
The 20-item PANAS is a self-report measure that provides orthogonal subscales of negative and positive affectivity. Only the 10-item negative affect subscale (PANAS-NA) was utilized in the present study. Example items include “nervous,” “distressed,” and “upset.” Participants rated each item in terms of their experiences during the past week on a 5-point Likert-type scale ranging from 1 (very slightly or not at all) to 5 (extremely). A sum score was calculated, with higher scores indicating greater negative affect.
White Bear Suppression Inventory (WBSI; Wegner and Zanakos 1994)
The 15-item WBSI is a self-report measure of the tendency to suppress unpleasant or unwanted thoughts. Example items include “There are things that I try not to think about” and “I have thoughts that I cannot stop.” Participants rated each item on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Possible scores range from 15 to 75 and higher scores reflect a greater tendency to engage in thought suppression.
Eating Disorder Examination-Questionnaire (EDE-Q; Fairburn and Beglin 1994)
The EDE-Q is a 28-item self-report measure that assesses eating disordered attitudes and behaviors. The measure contains a global scale and four subscales: restraint (e.g., “Have you been deliberately trying to limit the amount of food you eat to influence your shape or weight [whether or not you have succeeded]?”), eating concern (e.g., “Have you had a definite fear of losing control over eating?”), shape concern (e.g., “Have you felt fat?”), and weight concern (e.g., “Have you had a strong desire to lose weight?”). Participants rated each item on a 7-point Likert-type scale ranging from 0 to 6, with anchors varying depending on the item. Higher scores on the global scale and subscales are reflective of greater eating disorder symptoms.
Internal consistency values (Cronbach’s α) for all scales and subscales are presented in Table 1.
Procedure
This research protocol was reviewed and approved by the University at Albany Institutional Review Board. Participants responded to a series of questionnaires examining a variety of correlates of behaviors associated with eating disorder symptoms and body image concerns in men. Participants completed the measures in a laboratory setting either individually or in small groups.
Results
Correlational Analyses
Means, standard deviations, and intercorrelations for the primary variables of interest are presented in Table 1. As expected, the EDE-Q global and subscale scores were significantly associated with thought suppression, negative affect, and BMI, with one exception: the EDE-Q restraint subscale was not significantly correlated with negative affect. Furthermore, thought suppression was significantly associated with negative affect. No significant relationships were found between the EDE-Q global or subscale scores and the demographic variables of ethnicity (F(4, 289) < 1.72, P > .15) or age (r < 0.08, P > .15). Given the significant association between BMI and the EDE-Q global and subscale scores, as well as the theoretical relevance of this variable to eating disorder symptoms, BMI was included as a covariate in all subsequent analyses.
Unique Association between Thought Suppression and Global Eating Disorder Symptoms
To examine the unique association between thought suppression and global eating disorder symptoms in men, a hierarchical multiple regression analysis predicting the EDE-Q global score was conducted with BMI (t = 8.27, β = 0.43, P < .001) and the PANAS-NA score (t = 3.89, β = 0.20, P < .001) entered as covariates in the first step of the equation (R2 = 0.23). The WBSI total score (t = 4.62, β = 0.26, P < .001) was then entered in the second step (ΔR2 = 0.05), accounting for an additional 5% of the variance in eating disorder symptoms (with the full model predicting 28% of the variance). Furthermore, although BMI remained uniquely associated with eating disorder symptoms in the second step (t = 8.59, β = 0.43, P < .001), the PANAS-NA score was no longer significant (t = 1.36, β = 0.08, P > .05).
Examining the Mediating Role of Thought Suppression in the Association between Negative Affect and Global Eating Disorder Symptoms
Mediation was examined by directly testing the significance of the indirect effect of the independent variable (negative affect) on the dependent variable (global eating disorder symptoms) through the proposed mediator (thought suppression), calculated as the product of the effect of the independent variable on the mediator (a) and the effect of the mediator on the dependent variable (b). The current study utilized a bootstrapping approach, which provides an estimate of the indirect effect (a x b) based on a mean derived from n samples with replacement from a data set (Preacher and Hayes 2004). In the current study, the indirect effect estimate was derived from the mean of 5,000 bootstrap samples. Bias corrected and accelerated 99% confidence intervals were calculated, and the estimate of the indirect effect was interpreted as significant when zero was not contained within the confidence intervals.
Consistent with the correlational analyses and the hierarchical regression analysis presented above, the total effect (c) of the independent variable on the dependent variable indicated that negative affect was significantly positively associated with eating disorder symptoms (see Table 2). Negative affect was also significantly positively associated with the proposed mediator of thought suppression (a), and thought suppression was significantly positively associated with global eating disorder symptoms (b). Finally, thought suppression was found to fully mediate the relationship between negative affect and global eating disorder symptoms. Specifically, the analysis revealed a significant positive indirect effect (a × b) and a non-significant direct effect (c′), such that negative affect was no longer significantly associated with global eating disorder symptoms after accounting for thought suppression.
Examining the Mediating Role of Thought Suppression in the Association between Negative Affect and Specific Eating Disorder Symptoms
Utilizing the same approach as outlined above, four additional mediation analyses were conducted to test models in which thought suppression was hypothesized to mediate the relationship between negative affect and the four specific eating disorder symptoms: restraint, eating concern, shape concern, and weight concern (see Table 2). Results supported full mediation for the model in which shape concern was the DV, partial mediation for the models in which eating concern and weight concern were the DVs, and no mediation for the model in which restraint was the DV. Specifically, in the shape concern mediation analysis, a significant positive indirect effect and a non-significant direct effect were found, suggesting that negative affect was no longer significantly associated with shape concern after accounting for thought suppression. In contrast, whereas the mediation analyses for eating concern and weight concern also indicated significant positive indirect effects, the direct effects remained significant (albeit reduced), such that negative affect was still significantly positively associated with both eating concern and weight concern after accounting for thought suppression. Finally, consistent with the results of the correlational analyses, findings revealed a lack of a significant total effect of negative affect on restraint, and both the direct and indirect effects were similarly non-significant.
Discussion
Although some models of the pathogenesis of eating disorders emphasize the role of emotional and/or cognitive avoidance in the development and maintenance of eating disorder symptoms, few studies have examined the association between generalized thought suppression and eating disorder symptoms, particularly among men. In addition, despite findings of (a) the mediating role of thought suppression in the relationship between negative affect and various clinical difficulties (Lynch et al. 2001; Rosenthal et al. 2005; Rosenthal et al. 2006) and (b) a link between avoidant emotion regulation strategies and eating disorder symptoms (Aldao and Nolen-Hoeksema 2010; Wildes et al. 2010), no studies have examined the extent to which thought suppression (an avoidant cognitive emotion regulation strategy) mediates the association between negative affect and eating disorder symptoms among men.
As hypothesized, thought suppression was found to be uniquely associated with global eating disorder symptoms in the current sample of men, supporting past findings of an association between generalized thought suppression and bulimic symptoms among women and men (Lavender et al. 2009). In addition, thought suppression was found to fully mediate the relationship between negative affect and both global eating disorder symptoms and the specific eating disorder symptom of shape concern in this sample, and to partially mediate the relationship between negative affect and the eating disorder symptoms of eating and weight concerns. Interestingly, however, negative affect was not significantly associated with the EDE-Q subscale of restraint at a zero-order level, and although significant, the correlation between thought suppression and restraint was substantially lower than the correlations between thought suppression and the other eating disorder symptoms. These findings suggest that negative affect and thought suppression may be more relevant to shape, weight, and eating concerns than restricting behaviors among men. Overall, these results are consistent with both the conceptualization of thought suppression as a cognitive emotion regulation strategy (see Aldao and Nolen-Hoeksema 2010), as well as the affect regulation model of eating disorders and escape theory of binge eating (Arnow et al. 1992; Heatherton and Baumeister 1991; Polivy and Herman 1993).
Given that negative affect has been implicated in both the development and maintenance of eating disorders (e.g., Stice 2002), identifying variables that mediate the relationship between negative affect and eating disorder symptoms is an essential step in clarifying models of the pathogenesis of eating disorders. The mediator examined in the current study was the cognitive emotion regulation strategy of thought suppression. Whereas prior studies have examined the impact of suppressing food and weight-related thoughts in particular on various cognitive, behavioral, and physical outcomes (Harnden et al. 1997; Johnston et al. 1999; O’Connell et al. 2005; Oliver and Huon 2001), the preliminary findings of this study suggest that a more general tendency to suppress unwanted cognitions may be associated with eating disorder symptoms in men, particularly concerns about shape, eating, and weight. More specifically, it is possible that engaging in thought suppression in response to negative affect could be associated with an increased likelihood of experiencing eating disorder symptoms. Alternatively, it may be that these chronic efforts to suppress unpleasant thoughts reflect a more general pattern of experiential avoidance, which is characterized by the refusal to remain in contact with unpleasant physical, cognitive, and affective experiences (Chawla and Ostafin 2007; Hayes et al. 1999). This notion is supported by research that suggests a link between the broader construct of experiential avoidance and eating disorder symptoms in both non-clinical and clinical samples (e.g., Hayaki 2009; Rawal et al. 2010).
Although the results of this study add to the small but growing body of literature on the factors associated with eating disorder symptoms in men, several limitations must be noted. First, although findings provide preliminary support for the mediating role of thought suppression in the association between negative affect and several eating disorder symptoms among men, the effect sizes in this study were small and much of the variance in eating disorder symptoms remained unaccounted for by our models. Thus, future research is needed to explore other factors that may mediate this association among men, including experiential avoidance and other specific emotion regulation strategies (e.g., avoidance or rumination; see Aldao et al. 2010). The relatively small effects found here may also be due, in part, to the restricted range of eating pathology within our sample. Indeed, given that the men in this sample were drawn from a non-clinical setting, the findings may not generalize to relevant clinical populations (e.g., treatment-seeking men with eating disorders). However, several studies indicate that the average age of onset for eating disorders among men is approximately 19–20 years (e.g., Braun et al. 1999; Carlat et al. 1997), supporting the importance of research with college-aged men (due to the potential vulnerability of this population). Further, the recruitment of participants from a nonclinical setting does not preclude the possibility that some participants may have been experiencing clinically significant levels of eating disorder symptoms (e.g., in reference to the past month, 21% of the current sample of men endorsed one or more episodes of binge eating, 6% endorsed four or more episodes of binge eating, and 3% endorsed one or more episodes of self-induced vomiting).
In addition, although the focus on men is a strength of this study, contributing to the relatively understudied area of eating disorder symptoms among men, future studies should examine the interrelations between thought suppression, negative affect, and eating disorder symptoms among women. Indeed, given evidence of higher rates of restricting behaviors among women versus men (e.g., Striegel-Moore et al. 2009), it is possible that negative affect and thought suppression would emerge as more relevant to restraint symptoms within female samples. Furthermore, this study relied exclusively on self-report questionnaires. Although research suggests that the anonymity associated with self-report measures versus face-to-face interviews may result in more honest responding to questions about eating disorder symptoms (Keel et al. 2002; Lavender and Anderson 2009), future studies would benefit from including a structured eating disorder interview. Finally, the cross-sectional design of the current investigation precludes determination of the precise nature and direction of the relations of interest. Whereas a general tendency to suppress unwanted thoughts may function as a risk factor for developing eating disorder symptoms, it is also possible that chronic thought suppression may develop as a consequence of the unpleasant and unwanted cognitions associated with eating disorder symptoms (e.g., thoughts about food, body weight/shape). Additional studies utilizing a prospective design are needed to clarify the nature of these associations and the extent to which thought suppression actually increases the risk for eating disorder symptoms among men.
Despite these limitations and the preliminary nature of the current investigation, the findings of this study may have theoretical and clinical implications, particularly given the availability of newer interventions that target avoidant emotion regulation strategies [e.g., Acceptance and Commitment Therapy (Hayes et al. 1999); Dialectical Behavior Therapy (Safer et al. 2009); Emotion Acceptance Behavior Therapy (Wildes and Marcus 2011; Integrative Cognitive-Affective Therapy (Wonderlich et al. 2009); Mindfulness-Based Eating Awareness Training (Kristeller and Wolever 2011)]. Therapeutic strategies that seek to decrease avoidance and promote awareness and acceptance of internal experiences (e.g., mindfulness and emotion regulation skills training) may be of particular benefit. For instance, preliminary studies suggest that such interventions may hold promise in the treatment of a variety of forms of eating pathology, including anorexia nervosa (Berman et al. 2009; Wildes and Marcus 2011), bulimia nervosa (Safer et al. 2001), and binge eating disorder (Kristeller and Hallett 1999; Kristeller and Wolever 2011).
In sum, the current findings are consistent with theoretical and empirical literature suggesting the relevance of cognitive and emotional avoidance to eating disorder symptoms. Further research will be required to determine the specific role of such avoidance factors, including thought suppression, in the etiology and/or maintenance of eating disorder symptoms in general and among men in particular.
References
Aldao, A., & Nolen-Hoeksema, S. (2010). Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behaviour Research and Therapy, 48, 974–983.
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30, 217–237.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders, (4th ed., text revision). Washington, DC: Author.
Arnow, B., Kennedy, J., & Agras, W. S. (1992). Binge eating among the obese: A descriptive study. Journal of Behavioral Medicine, 15, 155–170.
Berman, M. I., Boutelle, K. N., & Crow, S. J. (2009). A case series investigating acceptance and commitment therapy as a treatment for previously treated, unremitted patients with anorexia nervosa. European Eating Disorders Review, 17, 426–434.
Braun, D. L., Sunday, S. R., Huang, A., & Halmi, K. A. (1999). More males seek treatment for eating disorders. International Journal of Eating Disorders, 25, 415–424.
Carlat, D. J., Camargo, C. A., & Herzog, D. B. (1997). Eating disorders in males: A report on 135 patients. American Journal of Psychiatry, 154, 1127–1132.
Chawla, N., & Ostafin, B. (2007). Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. Journal of Clinical Psychology, 63, 871–890.
Erskine, J. A. K., & Georgiou, G. J. (2010). Effects of thought suppression on eating behaviour in restrained and non-restrained eaters. Appetite, 54, 499–503.
Fairburn, C. G., & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self-report questionnaire? International Journal of Eating Disorders, 16, 363–370.
Gupta, S., Rosenthal, M. Z., Mancini, A. D., Cheavens, J. S., & Lynch, T. R. (2008). Emotion regulation skills mediate the effects of shame on eating disorder symptoms in women. Eating Disorders, 16, 405–417.
Harnden, J. L., McNally, R. J., & Jimerson, D. C. (1997). Effects of suppressing thoughts about body weight: A comparison of dieters and nondieters. International Journal of Eating Disorders, 22, 285–290.
Hayaki, J. (2009). Negative reinforcement, eating expectancies, emotion dysregulation, and symptoms of bulimia nervosa. International Journal of Eating Disorders, 42, 552–556.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (1999). Acceptance and commitment therapy: An experiential approach to behavior change. New York: Guilford Press.
Heatherton, T. F., & Baumeister, R. F. (1991). Binge eating as escape from self-awareness. Psychological Bulletin, 110, 86–108.
Johnston, L., Bulik, C. M., & Anstiss, V. (1999). Suppressing thoughts about chocolate. International Journal of Eating Disorders, 26, 21–27.
Keel, P. K., Crow, S., Davis, T. L., & Mitchell, J. E. (2002). Assessment of eating disorders: Comparison of interview and questionnaire data from a long-term follow-up study of bulimia nervosa. Journal of Psychosomatic Research, 53, 1043–1047.
Keel, P. K., Klump, K. L., Leon, G. R., & Fulkerson, J. A. (1998). Disordered eating in adolescent males from a school-based sample. International Journal of Eating Disorders, 23, 125–132.
Kristeller, J. L., & Hallett, C. B. (1999). An exploratory study of a meditation-based intervention for binge eating disorder. Journal of Health Psychology, 4, 357–363.
Kristeller, J. L., & Wolever, R. (2011). Mindfulness-Based Eating Awareness Training for treating binge eating disorder: The conceptual foundation. Eating Disorders, 19, 49–61.
Lavender, J. M., & Anderson, D. A. (2009). Effect of perceived anonymity in assessments of eating disordered behaviors and attitudes. International Journal of Eating Disorders, 42, 546–551.
Lavender, J. M., Jardin, B. F., & Anderson, D. A. (2009). Bulimic symptoms in college men and women: Contributions of mindfulness and thought suppression. Eating Behaviors, 10, 228–231.
Lynch, T. R., Robins, C. J., Mendelson, J. Q., & Krause, E. D. (2001). A mediation model relating affect intensity, emotion inhibition, and psychological distress. Behavior Therapy, 32, 519–536.
O’Connell, C., Larkin, K., Mizes, J. S., & Fremouw, W. (2005). The impact of caloric preloading on attempts at food and eating-related thought suppression in restrained and unrestrained eaters. International Journal of Eating Disorders, 38, 42–48.
Olivardia, R., Pope, H. G., Mangweth, B., & Hudson, J. I. (1995). Eating disorders in college men. American Journal of Psychiatry, 152, 1279–1285.
Oliver, K. G., & Huon, G. F. (2001). Eating-related thought suppression in high and low disinhibitors. International Journal of Eating Disorders, 30, 329–337.
Pearson, C. M., Combs, J. L., & Smith, G. T. (2010). A risk model for disordered eating in late elementary school boys. Psychology of Addictive Behaviors, 24, 696–704.
Polivy, J., & Herman, C. P. (1993). Etiology of binge eating: Psychological mechanisms. In C. G. Fairburn & G. T. Wilson (Eds.), Binge eating: Nature, assessment, and treatment (pp. 173–205). New York: Guilford Press.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments and Computers, 36, 717–731.
Purdon, C. (1999). Thought suppression and psychopathology. Behaviour Research and Therapy, 37, 1029–1054.
Rawal, A., Park, R. J., & Williams, J. M. G. (2010). Rumination, experiential avoidance, and dysfunctional thinking in eating disorders. Behaviour Research and Therapy, 48, 851–859.
Rosenthal, M. Z., Cheavens, J. S., Lejuez, C. W., & Lynch, T. R. (2005). Thought suppression mediates the relationship between negative affect and borderline personality disorder symptoms. Behaviour Research and Therapy, 43, 1173–1185.
Rosenthal, M. Z., Cheavens, J. S., Lynch, T. R., & Follette, V. (2006). Thought suppression mediates the relationship between negative mood and PTSD in sexually assaulted women. Journal of Traumatic Stress, 19, 741–745.
Safer, D. L., Telch, C. F., & Agras, W. S. (2001). Dialectical behavior therapy for bulimia nervosa. American Journal of Psychiatry, 158, 632–634.
Safer, D., Telch, C., & Chen, E. (2009). Dialectical behavior therapy for binge eating and bulimia. New York, NY: Guilford Press.
Soetens, B., Braet, C., & Moens, E. (2008). Thought suppression in obese and non-obese restrained eaters: Piece of cake or forbidden fruit? European Eating Disorders Review, 16, 67–76.
Stice, E. (2002). Risk and maintenance factors for eating pathology: A meta-analytic review. Psychological Bulletin, 128, 825–848.
Striegel-Moore, R. H., Rosselli, F., Perrin, N., DeBar, L., Wilson, G. T., May, A., et al. (2009). Gender difference in the prevalence of eating disorder symptoms. International Journal of Eating Disorders, 42, 471–474.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070.
Wegner, D. M., Schneider, D. J., Carter, S. R., & White, L. (1987). Paradoxical effects of thought suppression. Journal of Personality and Social Psychology, 53, 5–13.
Wegner, D. M., & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 614–640.
Whiteside, U., Chen, E., Neighbors, C., Hunter, D., Lo, T., & Larimer, M. (2007). Difficulties regulating emotions: Do binge eaters have fewer strategies to modulate and tolerate negative affect? Eating Behaviors, 8, 162–169.
Wildes, J., & Marcus, M. (2011). Development of emotion acceptance behavior therapy for anorexia nervosa: A case series. International Journal of Eating Disorders, 44, 421–427.
Wildes, J. E., Ringham, R. M., & Marcus, M. D. (2010). Emotion avoidance in patients with anorexia nervosa: Initial test of a functional model. International Journal of Eating Disorders, 43, 398–404.
Wonderlich, S. A., Peterson, C. B., Smith, T. L., Klein, M., Mitchell, J. E., Crow, S. J., et al. (2009). Integrative Cognitive-Affective Therapy for bulimia nervosa. In C. M. Grilo & J. E. Mitchell (Eds.), The treatment of eating disorders: A clinical handbook (pp. 317–338). New York: Guilford Press.
Woodside, D. B., Garfinkel, P. E., Lin, E., Goering, P., Kaplan, A. S., Goldbloom, D. S., et al. (2001). Comparisons of men with full or partial eating disorders, men without eating disorders, and women with eating disorders in the community. American Journal of Psychiatry, 158, 570–574.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lavender, J.M., Anderson, D.A. & Gratz, K.L. Examining the Association Between Thought Suppression and Eating Disorder Symptoms in Men. Cogn Ther Res 36, 788–795 (2012). https://doi.org/10.1007/s10608-011-9403-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-011-9403-x