
Abstract
Although social anxiety and problematic alcohol use co-occur at alarmingly high rates, the mechanism for this co-occurrence is not well understood. The current study examined the mediating role of positive social alcohol expectancies (i.e., beliefs related to the desirable social effects of drinking) in the relationship between social anxiety and hazardous drinking (i.e., heavy drinking and negative consequences) among an ethnically and racially diverse (87% racial and/or ethnic minority) sample of undergraduate volunteers (n = 610; Mage = 19.1; 69% women). The results of structural equation modeling analyses (using AMOS 7.0) indicated that social (but not tension reduction, sexual enhancement, positive cognitive changes, or negative affective changes) alcohol outcome expectancies partially mediated the association between social anxiety and hazardous drinking; however, social anxiety had a negative direct effect on hazardous drinking. Findings implicate social alcohol outcome expectancies as a mechanism to target in treatment and prevention among socially anxious students.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Alcohol problems and social anxiety co-occur at alarmingly high rates. Epidemiological studies have found that up to 48% of those with a diagnosis of social anxiety disorder have also had a diagnosis of an alcohol use disorder during their lifetime, with social anxiety developing prior to alcohol problems in the majority of the cases (e.g., Grant et al. 2005; Magee et al. 1996). When controlling for baseline anxiety disorders, mood disorders, conduct disorder, and substance use disorders, Buckner and colleagues (2008) found that adolescents diagnosed with social anxiety disorder at baseline were 4.5 times more likely to meet criteria for alcohol dependence approximately 14 years later than individuals without a social anxiety diagnosis. Likewise, long-term follow-up data from Epidemiological Catchment Study participants suggests that individuals with subclinical social anxiety also are at risk for developing alcohol problems, as participants with subclinical social anxiety at baseline were at a higher risk for developing alcohol abuse when assessed 13 years later than those without social anxiety symptoms at baseline (Crum and Pratt 2001).
College students seem to be particularly at risk for drinking to reduce social anxiety given the high social demands and frequent opportunities to drink inherent in the college environment. College student problem drinking has received attention as an important public health concern, with several national studies indicating that college students frequently engage in heavy, high risk drinking behaviors and experience high rates of alcohol-related negative consequences (e.g., hangovers, accidents, injuries; Hingson et al. 2005; O’Malley and Johnston 2002; Wechsler et al. 2000). Not only is hazardous drinking, or drinking patterns with negative consequences (e.g., getting in trouble due to drinking or having symptoms of dependence), among college students highly prevalent, but college students frequently are exposed to novel social situations in which alcohol is easily accessible, socially acceptable, encouraged, and promoted (e.g., Ham and Hope 2003). However, findings regarding the association between social anxiety and drinking-related variables in college students have been mixed; some studies have reported positive associations (Buckner et al. 2006b; Lewis and O’Neill 2000), while others have found either no relationship or a negative association (e.g., Buckner et al. 2007, 2006a; Eggleston et al. 2004; Ham and Hope 2005, 2006). Although social anxiety and alcohol misuse commonly co-occur and social anxiety appears to serve as a risk factor for alcohol-related disorders, the mechanism for this co-occurrence is not well understood.
Popular, and seemingly intuitive, explanations for the co-occurrence of social anxiety and alcohol-related disorders, such as the tension reduction theory (e.g., Conger 1956) and the self-medication hypothesis (e.g., see Carrigan and Randall 2003 for a review; Khantzian 1985), have not been consistently supported. Such theories assert that alcohol provides a means of alleviating tension or other negative states (i.e., a negative reinforcement process) which may lead to dependence on the substance. Accordingly, the more an individual experiences social anxiety, the more he or she will use alcohol, which eventually may lead to a substance use disorder (see review by Morris et al. 2005). However, these theories do not sufficiently explain empirical findings that some socially anxious individuals actually drink less than non-anxious individuals and/or abstain from alcohol altogether (e.g., Eggleston et al. 2004; Ham and Hope 2005; Crum and Pratt 2001) and that social anxiety reduction from alcohol has not been found consistently in laboratory and naturalistic settings (e.g., see Carrigan and Randall 2003; Tran and Smith 2008).
The stress response dampening model (SRD; Sher and Levenson 1982) extends previous models with the consideration of individual differences that could influence alcohol’s stress-reducing effects. According to the SRD, alcohol may serve as an anxiolytic by relieving or insulating one from “stress”; however, the magnitude of the stress-response dampening experienced from alcohol use may vary across individuals. Alcohol outcome expectancies (AOE) may assist in explicating the relationship between social anxiety and hazardous drinking. According to expectancy theory, AOE are the beliefs concerning the effects of using alcohol that likely influence one’s decision to drink (e.g., Goldman et al. 1999), such that individuals who hold positive expectancies about the effects of alcohol (e.g., be more sociable, feel happy) will be more likely to consume alcohol. Based on SRD and expectancy theory, the expectation of positive social effects from alcohol (e.g., feeling more relaxed in social situations) may mediate the relationship between social anxiety and hazardous drinking. Increased social anxiety might present a heightened risk for hazardous drinking via the presence of stronger AOE pertaining to relief in social situations.
A limitation of many studies focusing on AOE to elucidate the association between social anxiety and drinking is the failure to assess AOE specific to social situations (social AOE; e.g., “I feel less shy,” “I feel more comfortable talking to people”) that may be particularly important to individuals experiencing discomfort in social situations. Instead, studies tend to focus on several global dimensions rather than AOE specific to social situations (e.g., Ham and Hope 2005, 2006). There is evidence to suggest that socially anxious individuals have stronger positive AOE specific to social situations and may attend to these social AOE more so than global AOE. First, socially anxious individuals have been found to report greater social AOE than controls (Ham et al. 2002; Tran and Haaga 2002). In addition, socially anxious individuals have attentional biases toward information related to social and/or evaluative situations more than information unrelated to social/evaluative situations (see Clark and McManus 2002). Recent work found that a community sample of socially anxious individuals reported greater positive AOE for social situations than non-anxious individuals, but not greater positive AOE in general (Ham et al. 2005). Further, social AOE have been consistently linked with elevated drinking and drinking-related problems (e.g., Bruch et al. 1997; Ham et al. 2005; Reis and Riley 2000; Tran et al. 1997). Social AOE appear particularly relevant to socially anxious college students, as the college environment provides a unique social context that would increase pressure for drinking, anxiety in social situations, and availability of alcohol within the anxiety-provoking situations.
Four studies have directly examined the role of social AOE in the association between social anxiety (or social anxiety-related constructs) and drinking behaviors in college students. Studies have found that positive social AOE suppressed an inverse relation between alcohol use and social anxiety (Eggleston et al. 2004) or shyness (Bruch et al. 1992, 1997). Tran et al. (1997) found a weak moderating effect of positive social AOE, such that socially anxious undergraduates with low endorsement of positive social AOE drank less than nonanxious students with low levels of social AOE. Conversely, Eggleston et al. (2004) and Bruch et al. (1992, 1997) found that positive social AOE did not moderate the association between social anxiety or shyness with alcohol use. The mixed findings might be due, in part, to the tendency to measure problem drinking via alcohol consumption rather than hazardous drinking more comprehensively (i.e., quantity/frequency of alcohol use and heavy drinking, frequency of negative consequences, and symptoms of alcohol dependence). Research suggests that social anxiety is differentially associated with various alcohol-related outcomes such that social anxiety is more likely to be positively associated with alcohol problems or symptoms of alcohol dependence than with drinking frequency or quantity (e.g., Gilles et al. 2006; Stewart et al. 2006). The current study therefore improves upon the previous studies by using a measure of hazardous drinking, an outcome variable of considerable clinical interest.
The present study contributes to the growing literature exploring the complex relationship between social anxiety and drinking problems by examining the role of positive social AOE (i.e., beliefs related to the positive social effects of drinking) in comparison to other AOE, assessing hazardous drinking rather than merely alcohol consumption, and utilization of a structural equation modeling (SEM) data analytic approach. Furthermore, in utilizing an ethnically and racially diverse sample in contrast to previous studies, the present study seeks to apply the proposed model to a more diverse student population given that previous samples were predominately non-Hispanic Caucasian. Based on previous studies (e.g., Tran and Haaga 2002; Ham et al. 2005) and models of alcohol use (Goldman et al. 1999; Sher and Levenson 1982), it was hypothesized that positive social AOE, but not other types of positive AOE (e.g., “I get better ideas when I am drinking”) or negative AOE (e.g., “Drinking makes me bad tempered”), would mediate the association between social anxiety and hazardous drinking. It was further expected that social anxiety would be positively related with social AOE, but not other AOE, as well as with hazardous drinking. It was expected that all positive AOE would be associated positively with hazardous drinking, while negative AOE would be inversely related to hazardous drinking.
Methods
Participants
The sample consisted of 610 undergraduate student volunteers (420 [69%] women, 190 [31%] men; Mage = 19.1, SD = 1.8, range = 18–30) attending a southeastern urban public university. Students were recruited through the Psychology Subject Pool, consisting of students from Introductory Psychology, Research Methods in Psychology, and other upper-level psychology courses. Sixty-nine percent of the total sample (n = 423) self-identified as Hispanic/Latino, 13% (n = 82) as White/Caucasian, 6% (n = 39) as African American/Black, 6% (n = 34) as Asian/Pacific Islander, and 5% (n = 30) as “Mixed” or “Other.” Two individuals did not report ethnic/racial information.
Measures
Alcohol Outcome Expectancies
Two measures were administered to assess beliefs regarding the effects of drinking. First, the alcohol expectancies for social evaluative situations scale (AESES; Bruch et al. 1992), a 10-item self-report instrument designed to assess positive AOE related to alcohol’s effects on performance in social situations (e.g., “It is easier to start a conversation with someone if I have had a few drinks”). The AESES has demonstrated adequate internal consistency (α = .84–.91), test–retest reliability (r = .79) and convergent validity among college student samples (Bruch et al. 1992, 1997; Tran et al. 1997). The second measure was the drinking expectancy questionnaire (DEQ; Lee et al. 2003; Young and Knight 1989). The DEQ is a 43-item self-report measure assessing four positive dimensions of AOE, a negative AOE, and a sixth broad factor related to level of alcohol involvement (i.e., Dependence). In the current study, the 10-item Assertion (DEQ-A; e.g., “Drinking makes me feel outgoing and friendly”) dimension was selected as a measure of positive social effects of drinking. DEQ factors of cognitive change (DEQ-CC; 4 items; e.g., “Drinking helps me to be more mentally alert”), sexual enhancement (DEQ-SE; 5 items; e.g., “Drinking makes me more sexually responsive”), and tension reduction (DEQ-TR; 4 items; e.g., “I drink to relieve tension”) were used to assess positive AOE that were not specific to social effects. The DEQ factor of affective change (DEQ-AC; 12 items; e.g., “Drinking makes me feel more violent”), which was designed to assess beliefs about negative affective changes from alcohol, was used to assess a negative AOE. Consistent with Young and Knight (1989), scale scores are constructed by summing scale items, after reverse scoring relevant items. The DEQ factors used in the current study have demonstrated adequate construct validity and internal consistency (α = .78–.94) in community and college student samples, with the exception of one instance of extremely poor internal consistency for DEQ-TR (α = .22; current sample α = .64; Young and Knight 1989).
Social Anxiety
Participants completed the social interaction anxiety scale (SIAS) and social phobia scale (SPS; Mattick and Clarke 1989). The SIAS and SPS are companion self-report measures of social anxiety, intended to assess anxiety related to social interactions and anxiety related to scrutiny by others, respectively. Both measures have demonstrated good internal consistency (SIAS α = .86–.94; SPS α = .87–.94), test–retest reliability (SIAS rs = .86–.92; SPS rs = .66–.93), and construct validity among clinical, community, and college student samples (Heimberg et al. 1992; Mattick and Clarke 1989).
Hazardous Drinking
The alcohol use disorder identification test (AUDIT; Babor et al. 1992, 2001) was used to assess hazardous drinking. The AUDIT is a 10-item self-report questionnaire including items assessing alcohol use quantity and frequency, symptoms of dependence, and alcohol-related problems. The psychometric properties of the AUDIT have been well established for use in a variety of populations, including college-aged samples (e.g., Kokotailo et al. 2004; Reinert and Allen 2002, 2007). Among college students, Kokotailo and colleagues (2004) found that the AUDIT demonstrated good internal consistency (α = .81).
Procedures
All students provided informed consent prior to participating in the study. Participants completed the questionnaire packet including measures of social AOE, social anxiety, and hazardous drinking in a classroom setting. Participants received one research credit for participation in the study.
Data Analytic Plan
Prior to hypothesis-based analyses, the data were examined for missingness, outliers, and non-normality. Missingness bias was examined by creating a dummy variable reflecting the presence or absence of missing data for each variable in the model and correlating this dummy variable with all other model and demographic variables. Missing values (<1%) were imputed using the expectation-maximum method with importance re-sampling. To detect outliers, the AUDIT was regressed onto the social anxiety and AOE variables in limited information regression analyses and outliers were defined as an absolute standardized dfbeta > 1.0 (Bollen 1996). Next, the data for the covariance matrix were evaluated for multivariate outliers by examining the leverage indices and defining an outlier as a leverage score four times greater than the sample mean leverage. Multivariate non-normality was evaluated using of Mardia’s index and univariate non-normality was defined as kurtosis and/or skewness values >2.0.
The primary analytic strategy for the present study consisted of estimating a structural equation model (SEM) to test the relation of social anxiety to hazardous drinking indirectly through AOE. Models were evaluated with AMOS 7.0. Social anxiety (indicators were SIAS and SPS) and social AOE (indicators were AESES and DEQ-A) were operationalized as latent variables. The SPS and DEQ-A were randomly selected as marker variables for social anxiety and social AOE latent variables, respectively. Error variance was correlated among the AOE scales. Given gender differences in hazardous drinking levels (e.g., O’Malley and Johnston 2002; Read et al. 2002), models included gender as a covariate.
Following Brown’s (2006) recommendations, several global fit indices were used, including indices of absolute fit (χ2), comparative fit (comparative fit index [CFI]), and fit with a penalty function for lack of parsimony (root mean square error of approximation [RMSEA]; p-value for close fit). Next, more focused tests of fit were pursued, including examination of standardized residual covariances, modification indices, and parameter estimates for Heywood cases. The full model was trimmed by removing nonsignificant paths. MacKinnon’s (2008) asymmetric distribution of products test was used to assess the extent to which social AOE partially mediated the relationships of social anxiety and hazardous drinking.
Results
As shown in Table 1, preliminary analyses revealed that social anxiety (SIAS and SPS composite score) was positively correlated with measures of social AOE (AESES and DEQ-A), but unrelated to other types of positive AOE (DEQ-SE, DEQ-CC, DEQ-TR). Social anxiety was also positively correlated with the negative AOE (DEQ-AC). All positive AOE measures were positively correlated with hazardous drinking (AUDIT), while DEQ-AC was unrelated to the AUDIT. Social anxiety demonstrated a small inverse association with hazardous drinking.
Structural Equation Modeling
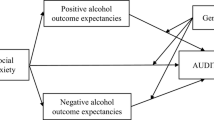
Outlier analyses indicated the presence of five multivariate outliers (0.8% of sample), but proved inconsequential for the analyses (i.e., all major conclusions remained intact when omitted). Thus, the reported results include outliers. Evaluation of non-normality suggested the presence of multivariate non-normality (Mardia’s index = 8.52, p < .05) and kurtosis for the AUDIT score (3.33). All univariate indices of skewness were nonproblematic (highest skewness value = 1.6). The model in Fig. 1 was evaluated using bootstrapping (with 2,000 replicates) to address non-normality. Models estimated with traditional maximum likelihood criteria yielded comparable results.

Model testing social alcohol outcome expectancies as a mediator of the association between social anxiety and hazardous drinking (n = 610). Note. *p < .05. ***p < .001. Non-significant paths were trimmed. The indirect effect (partial mediation via social AOE) of social anxiety on hazardous drinking was .12 (p < .05). SIAS, social interaction anxiety scale; SPS, social phobia scale; AOE, alcohol outcome expectancies; AESES, alcohol expectancies for social evaluative situations scale; DEQ-A, drinking expectancy questionnaire-assertion scale; AUDIT, alcohol use disorders identification test. The covariate (i.e., gender) and correlated error variance were omitted from the figure
Fit indices suggested a good fitting model (RMSEA = 0.06; p-value for test of close fit = 0.16; CFI = .98; GFI = 0.99; absolute standardized residuals <1.96), with the exception of significant Bollen–Stine χ2 (p = .01) which tends to become inflated with a large sample size (e.g., Byrne 2001). Nonsignificant paths were trimmed from the model, including paths to and from the DEQ-CC factor (resulting in this variable being eliminated from Fig. 1) as well as the paths from social anxiety to DEQ-TR and DEQ-SE and from DEQ-AC to the AUDIT. The standardized parameter estimates in Fig. 1 indicate that social anxiety had a negative direct association with hazardous drinking. As expected, social anxiety was related positively to positive social AOE, and social AOE had a positive association with hazardous drinking. Further, social anxiety was unrelated to all other positive AOE, but was positively associated with the negative AOE (i.e., DEQ-AC). DEQ-TR and DEQ-SE were positively associated with the AUDIT. MacKinnon’s (2008) asymmetric distribution of products test indicated that social anxiety had a significant positive indirect effect of .12 (p < .001; bias-corrected confidence interval = .07–.18) on hazardous drinking through social AOE, consistent with partial mediation. The total effect of social anxiety on the AUDIT, given the positive indirect effect and negative direct effect, was −.10 (p = .01; bias-corrected confidence interval = −.18 to −.03).
Moderation Analyses
To provide further confidence in the specificity of the SEM results in light of prior work by Tran et al. (1997) finding that social AOE moderated the association between social anxiety and alcohol use, post hoc hierarchical regression analyses was conducted to test moderation. Block 1 consisted of social anxiety (as an SIAS and SPS composite score) and one of the social AOE (AESES or DEQ-A), the interaction (products of centered main effect variables) entered in Block 2, and the AUDIT as the criterion variable. The interactions were not significant (ΔR2 ≤ .001; p = .53–.73), suggesting that social AOE did not moderate the relationship between social anxiety and hazardous drinking.
Discussion
The current study evaluated the role students’ beliefs related to positive social effects of alcohol played in the association between social anxiety and hazardous drinking in a multicultural sample of college students. Examination of individual path coefficients within the SEM model indicated that social anxiety was related to increased endorsement of social AOE, and social AOE were associated with increased hazardous drinking. As expected, social anxiety was unrelated to the positive AOE of tension reduction, cognitive change, and sexual enhancement. Social anxiety had a small negative association with the negative AOE of affective change; however, affective change AOE was unrelated to hazardous drinking. Consistent with the hypotheses, social AOE, but not other positive or negative AOE, partially mediated the relationship between social anxiety and hazardous drinking such that as social anxiety increased, hazardous drinking increased in association with elevated social AOE. As previous studies did not support the mediating role of general AOE in the association between social anxiety and drinking behavior variables (Eggleston et al. 2004; Ham and Hope 2005, 2006), the partial mediation of social anxiety and hazardous drinking by AOE specific to social effects in the current study lends support for the notion that the assessment of cognitions related to the alcohol’s positive effects specific to social situations might prove useful to understanding the social anxiety—hazardous drinking relationship.
In the present study, model results showed that social anxiety was negatively associated with hazardous drinking. Though contrary to expectations, the findings were consistent with several studies specifically examining college students (Buckner et al. 2007, 2006a, b; Eggleston et al. 2004; Ham and Hope 2005, 2006), providing evidence that the findings generalize to diverse student samples. Similar to previous studies conducted in college samples, social anxiety was related positively with social AOE (e.g., Tran et al. 1997). Surprisingly, the model results suggest varying relationships between social anxiety and hazardous drinking: a positive indirect association (via social AOE), a negative direct association, and nonsignificant total effects of social anxiety on hazardous drinking. Though seemingly contradictory, the results are similar to the suppressor effects (and lack of moderation effects) found by Bruch et al. (1992, 1997) and Eggleston et al. (2004), and may shed light on the mixed findings in social anxiety and drinking research. Together with previous research, the current study results suggest that social anxiety alone does not increase risk for (or may actually protect socially anxious students from) drinking problems in college populations. Instead, it seems that only in the concert with increased beliefs about positive social effects of alcohol, and not positive AOE more generally, do socially anxious college students become vulnerable to hazardous drinking.
Another explanation for the pattern of findings within this model (i.e., inconsistent mediation; e.g., MacKinnon et al. 2007) is that there are other mediating paths that were not considered in the current model that could account for some of the negative effects of social anxiety on hazardous drinking. For instance, another path might be increased negative beliefs about the effects of alcohol in social situations motivating socially anxious students to avoid social drinking situations altogether, resulting in much lower hazardous drinking levels than non-anxious students. However, there are no known measures specifically assessing negative social AOE. Though the current study included a negative AOE, this affective change scale includes items that appear to tap into beliefs that drinking will likely increase anger or aggression, dysphoria, and tension, rather than items specifically targeting one’s beliefs regarding negative social effects (e.g., “I will say something stupid or offensive,” “I would make a fool of myself.”). In the current study, social anxiety was positively correlated with beliefs about negative affective changes from drinking, but this negative AOE was unrelated to hazardous drinking.
The current study was strengthened by the use of empirically validated measures, consideration of AOE specific to social situations and other types of positive and negative AOE within one model, the use of a diverse sample, and a strong data analytic approach in the use of SEM. However, limitations include the lack of causal interpretability due to the correlational design, the use of self-report, and large error variance. Although it was not a goal of the present study, it is not known if current findings would generalize to non-college populations; therefore, additional research is needed in community and clinical samples. Though the influences of gender were controlled in the SEM, research testing the potential moderating effects of gender in the relationships among social anxiety, social AOE, and hazardous drinking is warranted. Future research should consider the use of experimental and longitudinal designs as well as additional measures to address relevant constructs that may not have been included in the current study. For instance, assessment of negative beliefs related to social situations should be considered as holding strong beliefs regarding the negative effects of alcohol in social situations could explain how social anxiety appears to be a protective factor for some individuals. Socially anxious students who expect negative social effects from alcohol may avoid alcohol consumption due to concerns about engaging in disinhibited behavior that may cause embarrassment and/or negative evaluation by others. Additionally, it is possible for individuals to expect certain effects from alcohol, but not actually drink with the goal of achieving those effects (e.g., Leigh 1990). Therefore, future research could consider the anxiety-specific drinking motives in addition to AOE. For example, the modified drinking motives questionnaire-revised assesses coping-anxiety drinking motives (Blackwell and Conrod 2003).
Overall, these findings have significant implications for prevention and treatment of alcohol use disorders. In particular, the assessment of alcohol expectancies specific to social situations could be an important screening device in identifying socially anxious individuals that currently engage in or are at risk for hazardous drinking. Therapeutic interventions using an “expectancy challenge” paradigm (e.g., Wiers and Kummeling 2004) targeting the positive social AOE might prove fruitful given that one’s expectancies regarding AOE do not necessarily correspond with one’s experience and/or the pharmacological effects of alcohol. For instance, Corbin et al. (2008) suggest that positive AOE may persist and promote hazardous drinking despite a lack of corresponding experiences of positive effects from drinking alcohol and even in the presence of high levels of negative consequences, making AOE distinct from (but overlapping with) one’s experience with alcohol. On the other hand, to the degree to which beliefs in regard to positive social effects from alcohol is accurate (at least in the short-term), then interventions focusing on alternative anxiety management strategies to avoid the negative consequences of alcohol use and psychoeducation specific to the longer-term reciprocal effects of alcohol and anxiety would be indicated (see Stewart and Conrod 2008). Over time, recurrent use of alcohol actually increases anxiety, and the effects of alcohol on anxiety would be reduced as tolerance increases.
In sum, the current study extends previous work examining social AOE, social anxiety, and drinking in providing support for the role of social AOE as a partial mediator of the association between social anxiety and hazardous drinking among a diverse sample of college students. This effect appears to be specific to social AOE, and not AOE related to tension reduction, enhanced sexuality, positive cognitive changes, or negative affective changes. Findings implicate social AOE as a possible mechanism involved in hazardous drinking among college students with elevated social anxiety, whereas social anxiety on its own does not appear to increase risk for hazardous drinking outcomes. An avenue for future research may be to examine the utility of social AOE in the identification of socially anxious students at risk for hazardous drinking. Further, interventions for co-occurring social anxiety and problem drinking may benefit from targeting social AOE.
References
Babor, T. F., de la Fluente, J. R., Saunders, J. B., & Grant, M. (1992). AUDIT: The alcohol use disorders identification test: Guidelines for use in primary health care. Geneva, Switzerland: World Health Organization.
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). AUDIT: The alcohol use disorders identification test—Guidelines for use in primary care (2nd ed.). Geneva: World Health Organization.
Blackwell, E., & Conrod, P. J. (2003). A five-dimensional measure of drinking motives. Unpublished manuscript, Department of Psychology, University of British Columbia.
Bollen, K. (1996). An alternative 2SLS estimator for latent variable models. Psychometrika, 61, 109–121. doi:10.1007/BF02296961.
Brown, T. A. (2006). Confirmatory factor analysis for applied research. New York: Guildford Press.
Bruch, M. A., Heimberg, R. G., Harvey, C. H., McCann, M., Mahone, M., & Slavkin, S. (1992). Shyness, alcohol expectancies, and alcohol use: Discovery of a suppressor effect. Journal of Research in Personality, 23, 137–149. doi:10.1016/0092-6566(92)90050-E.
Bruch, M. A., Rivet, K. M., Heimberg, R. G., & Levin, M. A. (1997). Shyness, alcohol expectancies, and drinking behavior: Replication and extension of a suppressor effect. Personality and Individual Differences, 22(2), 193–200. doi:10.1016/S0191-8869(96)00190-0.
Buckner, J. D., Bonn-Miller, M. O., Zvolensky, M. J., & Schmidt, N. B. (2007). Marijuana use motives and social anxiety among marijuana using young adults. Addictive Behaviors, 32, 2238–2252. doi:10.1016/j.addbeh.2007.04.004.
Buckner, J. D., Schmidt, N. B., Bobadilla, L., & Taylor, J. (2006a). Social anxiety and problematic cannabis use: Evaluating the moderating role of stress reactivity and perceived coping. Behaviour Research and Therapy, 44, 1007–1015. doi:10.1016/j.brat.2005.08.002.
Buckner, J., Schmidt, N., & Eggleston, A. (2006b). Social anxiety and problematic alcohol consumption: The mediating role of drinking motives and situations. Behavior Therapy, 37, 381–391. doi:10.1016/j.beth.2006.02.007.
Buckner, J. D., Schmidt, N. B., Lang, A. R., Small, J. W., Schlauch, R. C., & Lewinsohn, P. M. (2008). Specificity of social anxiety disorder as a risk factor for alcohol and cannabis dependence. Journal of Psychiatric Research, 42, 230–239. doi:10.1016/j.jpsychires.2007.01.002.
Byrne, B. (2001). Structural equation modeling with AMOS: Basic concepts, applications, and programming. Mahwah, NJ: Lawrence Erlbaum Associates.
Carrigan, M. H., & Randall, C. L. (2003). Self-medication in social phobia: A review of the alcohol literature. Addictive Behaviors, 28, 269–284. doi:10.1016/S0306-4603(01)00235-0.
Clark, D. M., & McManus, F. (2002). Information processing in social phobia. Biological Psychiatry, 51, 92–100. doi:10.1016/S0006-3223(01)01296-3.
Conger, J. (1956). Reinforcement theory and the dynamics of alcoholism. Quarterly Journal of Studies on Alcohol, 17, 296–305.
Corbin, W. R., Morean, M. E., & Benedict, D. (2008). The positive drinking consequences questionnaire (PDCQ): Validation of a new assessment tool. Addictive Behaviors, 33, 54–68. doi:10.1016/j.addbeh.2007.06.003.
Crum, R. M., & Pratt, L. A. (2001). Risk of heavy drinking and alcohol use disorders in social phobia: A prospective analysis. The American Journal of Psychiatry, 158, 1693–1700. doi:10.1176/appi.ajp.158.10.1693.
Eggleston, A. M., Woolaway-Bickel, K., & Schmidt, N. B. (2004). Social anxiety and alcohol use: Evaluation of the moderating and mediating effects of alcohol expectancies. Journal of Anxiety Disorders, 18, 33–49. doi:10.1016/j.janxdis.2003.07.005.
Gilles, D., Turk, C., & Fresco, D. (2006). Social anxiety, alcohol expectancies, and self-efficacy as predictors of heavy drinking in college students. Addictive Behaviors, 31, 388–398. doi:10.1016/j.addbeh.2005.05.020.
Goldman, M. S., Del Boca, F. K., & Darkes, J. (1999). Alcohol expectancy theory: The application of cognitive neuroscience. In H. Blane & K. Leonard (Eds.), Psychological theories of drinking and alcoholism (pp. 203–246). New York: Guilford Press.
Grant, B. G., Hasin, D. S., Blanco, C., Stinson, F. S., Chou, S. P., Goldstein, R. B., et al. (2005). The epidemiology of social anxiety disorder in the United States: Results from the National Epidemiologic Survey on alcohol and related conditions. The Journal of Clinical Psychiatry, 66, 1351–1361.
Ham, L. S., Carrigan, M. H., Moak, D. H., & Randall, C. L. (2005). Social anxiety and specificity of positive alcohol expectancies. Journal of Psychopathology and Behavioral Assessment, 27(2), 115–121. doi:10.1007/s10862-005-5385-x.
Ham, L. S., & Hope, D. A. (2003). College students and problematic drinking: A review of the literature. Clinical Psychology Review, 23, 719–759. doi:10.1016/S0272-7358(03)00071-0.
Ham, L. S., & Hope, D. A. (2005). Incorporating social anxiety into a model of college problematic drinking. Addictive Behaviors, 30, 127–150. doi:10.1016/j.addbeh.2004.04.018.
Ham, L. S., & Hope, D. A. (2006). Incorporating social anxiety into a model of college problematic drinking: Replication and extension. Psychology of Addictive Behaviors, 20, 348–355. doi:10.1037/0893-164X.20.3.348.
Ham, L. S., Hope, D. A., White, C. S., & Rivers, P. C. (2002). Alcohol expectancies and drinking behavior in adults with social anxiety disorder and dysthymia. Cognitive Therapy and Research, 26, 275–288. doi:10.1023/A:1014582005745.
Heimberg, R., Mueller, G., Holt, C., Hope, D., & Liebowitz, M. (1992). Assessment of anxiety in social interaction and being observed by others: The social interaction anxiety scale and the social phobia scale. Behavior Therapy, 23, 53–73. doi:10.1016/S0005-7894(05)80308-9.
Hingson, R., Heeren, T., Winter, M., & Wechsler, H. (2005). Magnitude of alcohol-related mortality, morbidity among US college students ages 18–24: Changes from 1998 to 2001. Annual Review of Public Health, 26, 259–279. doi:10.1146/annurev.publhealth.26.021304.144652.
Khantzian, E. J. (1985). The self-medication hypothesis of addictive disorders: Focus on heroin and cocaine dependence. In D. Allen (Ed.), The cocaine crisis. New York: Plenum Press.
Kokotailo, P. K., Egan, J., Gangnon, R., Brown, D., Mundt, M., & Fleming, M. (2004). Validity of the alcohol use disorders identification test in college students. Alcoholism, Clinical and Experimental Research, 28, 914–920.
Lee, N., Oei, T., Greeley, J., & Baglioni, A. (2003). Psychometric properties of the drinking expectancy questionnaire: A review of the factor structure and a proposed new scoring method. Journal of Studies on Alcohol, 64, 432–436.
Leigh, B. C. (1990). Alcohol expectancies and reasons for drinking: Comments from a study on sexuality. Psychology of Addictive Behaviors, 4, 91–96.
Lewis, B., & O’Neill, K. (2000). Alcohol expectancies and social deficits relating to problem drinking among college students. Addictive Behaviors, 25, 295–299. doi:10.1016/S0306-4603(99)00063-5.
MacKinnon, D. P. (2008). Introduction to statistical mediation analysis. New York: Lawrence Erlbaum Associates.
MacKinnon, D. P., Fairchild, A. J., & Fritz, M. S. (2007). Mediational analysis. Annual Review of Psychology, 58, 593–614. doi:10.1146/annurev.psych.58.110405.085542.
Magee, W. J., Eaton, W. W., Wittchen, H.-U., McGonagle, K. A., & Kessler, R. C. (1996). Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Archives of General Psychiatry, 53, 159–168.
Mattick, R. P., & Clarke, J. C. (1989). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36, 455–470. doi:10.1016/S0005-7967(97)10031-6.
Morris, E. P., Stewart, S. H., & Ham, L. (2005). The relationship between social anxiety disorder and alcohol use disorders: A critical review. Clinical Psychology Review, 25, 734–760. doi:10.1016/j.cpr.2005.05.004.
O’Malley, P., & Johnston, L. (2002). Epidemiology of alcohol and other drug use among American college students. Journal of Studies on Alcohol, 14, 23–49.
Read, J., Wood, M., Davidoff, O., McLacken, J., & Campbell, J. (2002). Making the transition from high school to college: The role of alcohol-related social influence factors in students’ drinking. Substance Abuse, 23, 53–65. doi:10.1023/A:1013682727356.
Reinert, D. F., & Allen, J. P. (2002). The alcohol use disorders identification test (AUDIT): A review of recent research. Alcoholism, Clinical and Experimental Research, 26, 272–279.
Reinert, D. F., & Allen, J. P. (2007). The alcohol use disorders identification test: An update of research findings. Alcoholism, Clinical and Experimental Research, 31, 185–199. doi:10.1111/j.1530-0277.2006.00295.x.
Reis, J., & Riley, W. L. (2000). Predictors of college students’ alcohol consumption: Implications for student education. The Journal of Genetic Psychology, 16, 282–291.
Sher, K., & Levenson, R. (1982). Risk for alcoholism and individual differences in the stress-response-dampening effect of alcohol. Journal of Abnormal Psychology, 91, 350–367. doi:10.1037/0021-843X.91.5.350.
Stewart, S. H., & Conrod, P. J. (2008). Anxiety disorder and substance use disorder comorbidity: Common themes and future directions. In S. H. Stewart & P. J. Conrod (Eds.), Anxiety and substance use disorders (pp. 239–257). New York: Springer.
Stewart, S., Morris, E., Mellings, T., & Komar, J. (2006). Relations of social anxiety variables to drinking motives, drinking quantity and frequency, and alcohol-related problems in undergraduates. Journal of Mental Health, 15, 671–682. doi:10.1080/09638230600998904.
Tran, G. Q., & Haaga, D. A. F. (2002). Coping responses and alcohol outcome expectancies in alcohol abusing and nonabusing social phobics. Cognitive Therapy and Research, 26(1), 1–17. doi:10.1023/A:1013803803192.
Tran, G. Q., Haaga, D. A. F., & Chambless, D. L. (1997). Expecting that alcohol use will reduce social anxiety moderates the relation between social anxiety and alcohol consumption. Cognitive Therapy and Research, 21, 535–553. doi:10.1023/A:1021857402164.
Tran, G. Q., & Smith, J. P. (2008). Co-morbidity of social phobia and alcohol use disorders: A review of psychopathology research findings. In S. H. Stewart & P. J. Conrod (Eds.), Anxiety and substance use disorders (pp. 59–79). New York: Springer.
Wechsler, H., Lee, J. E., Kuo, M., & Lee, H. (2000). College binge drinking in the 1990s: A continuing problem. Journal of American College Health, 48, 199–210.
Wiers, R. W., & Kummeling, R. H. C. (2004). An experimental test of an alcohol expectancy challenge in mixed gender groups of young heavy drinkers. Addictive Behaviors, 29, 215–220. doi:10.1016/S0306-4603(03)00081-9.
Young, R. M., & Knight, R. G. (1989). The drinking expectancy questionnaire: A revised measure of alcohol-related beliefs. Journal of Psychopathology and Behavioral Assessment, 11, 99–112. doi:10.1007/BF00962702.
Acknowledgments
The author would like to thank the undergraduate research assistants at Florida International University who assisted with data collection and data entry. In addition, thanks are due to Dr. Melissa Norberg for her helpful comments on an earlier draft of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ham, L.S. Positive Social Alcohol Outcome Expectancies, Social Anxiety, and Hazardous Drinking in College Students. Cogn Ther Res 33, 615–623 (2009). https://doi.org/10.1007/s10608-009-9248-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-009-9248-8