
Abstract
The present investigation examined emotional reactivity to stress in men and women with and without prior depression. Subjects with remitted depression (n = 55) and healthy controls with no history of psychiatric illness (n = 55) were studied using Experience Sampling Methodology to assess daily stressors and depressed mood. Main effects were observed for both female gender and past depression in increasing emotional reactivity to daily stressors. However, women experienced significantly greater emotional reactivity than men only among healthy controls and not among those with remitted depression. Formerly depressed men were more reactive to stress than men who never experienced depression, while no differences were observed for women across these groups. These findings suggest that a prior episode of depression renders men and women more equivalent in terms of stress vulnerability, thus helping to explain why gender differences in depression prevalence change as a function of prior episodes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Both gender and psychosocial stress are well-established risk factors for major depression, yet it is currently unknown why each appears to have a diminished impact as a function of episode occurrence. The overall prevalence of major depression is higher among women than men (Kessler 2003), but a salient gender difference is found only for the initial onset of this disorder and not for subsequent episodes (Kessler et al. 1993). Psychosocial stress has been repeatedly shown to precipitate depression, especially in women (Maciejewski et al. 2001), but life events appear to play a differential role in the onset of first as compared to subsequent episodes (Monroe et al. 2007). These patterns suggest that occurrence of a prior episode may modify the relationship of stress and depression, and that this relationship may vary by gender. This possibility remains to be tested directly, and would have important implications both for clinical interventions and for psychological theories of stress vulnerability.
A differential role of stress in the occurrence of major depression has received considerable attention and yielded several alternative theoretical explanations, including a kindling hypothesis suggesting a reduced impact of stress on subsequent depression and a sensitization hypothesis suggesting an increased impact of stress on depression (Monroe and Harkness 2005). One possible explanation for the changing role of stress is that memory networks activated when an individual is depressed reinforce the salience of negative schemas and, as a consequence, progressively lower levels of depressed mood are necessary to activate dysfunctional cognitions in the future (Segal et al. 1996). This process of cognitive sensitization also results in heightened emotional reactivity to stressful events, and less severe stressors are required to trigger subsequent episodes of equivalent severity. In addition to providing a cognitive hypothesis for alterations in the role of stress, this theory may also help to explain the observed changes in risk posed by gender. As women have been shown to be more likely to experience ruminative thinking (Nolen-Hoeksema et al. 1999), perceive events more negatively than men (Almeida and Kessler 1998) and to have greater emotional reactivity to common stressors (Kendler et al. 1995), gender differences may become diminished after a first episode if the reinforcement of dysfunctional cognitions, and resulting reactivity to events, is proportionately greater in men.
From a methodological perspective, the study of stress and emotional reactivity is often based on between-person variance in the occurrence of relatively rare events, and assessed through correlations with clinical outcomes observed for a sample as a whole. This approach hinders the investigation of how events are generally perceived by the individual and prevents characterization of the magnitude of mood reactions over time. The study of cognitive vulnerability and emotional reactivity in relation to daily events therefore provides a useful alternative for the investigation of stress and depression (Gable et al. 2000; Marco et al. 1999). In such research, the use of ambulatory monitoring techniques provides within-person variance in mood under stressful and stress-free conditions. Previous research using this approach has confirmed gender differences in the perception of daily stress (Almeida and Kessler 1998), and some evidence has been found for the capacity of current depression to influence stress reactivity (Peeters et al. 2003). However, the interaction of gender with depression history has not been examined A comparison of particular interest would therefore involve the examination of gender differences relative to both cognitions concerning the severity of daily events and subsequent emotional reactivity as a function of previous but resolved depression.
A final consideration for testing the notion of cognitive sensitization concerns the need to control for diverse factors that co-vary with depression history. In particular, comparisons of differences in formerly depressed individuals and normal controls may be biased by pre-existing cognitive styles or personality vulnerabilities to depression. A central tenet of cognitive models of depression is the notion that, in individuals vulnerable to this disorder, negative cognitions arise when triggered by stressful life events (Abramson et al. 1989; Beck 1987). In turn, the activation of these negative cognitive patterns are associated with the onset and recurrence of depression (Scher et al.2005). Among the most studied of these vulnerabilities are depressogenic attributional style that leads individuals to perceive negative event causes as stable over time and as affecting multiple domains of one’s life (Abramson et al. 1989), and sociotropy or autonomy characteristics that render individuals more sensitive to specific types of events (Beck 1983, 1987). These cognitive vulnerabilities constitute independent risk factors for depression (Gotlib et al. 1993; Spangler et al. 1997) and may co-exist within the same individual. Substance use history also can contribute to risk for depression (Merikangas et al. 1998), and this influence may vary considerably by gender (Swendsen et al. 2000) The adequate control of these individual characteristics when examining the role of past depression should therefore provide a more rigorous test of this theory.
The present controlled investigation examined the influence of depression history and gender on the perceived severity of daily life events and on subsequent changes in depressed mood. Using ambulatory monitoring procedures, previously depressed and never-depressed men and women completed computerized interviews several times a day for a one-week period. We hypothesize that event negativity and subsequent depressed mood reactions would be greater in women as compared to men, and greater for those with a history of major depression as compared to normal controls. In addition, an interaction is expected among these variables whereby the capacity for past depression to increase event negativity and subsequent emotional reactivity would be greater in men as compared to women.
Method
Participants
The sample comprised 179 freshmen from the University of Bordeaux, France who completed all phases of the study which included an initial screening, a 7-day ambulatory monitoring period, and a clinical assessment (Husky et al. 2007). For the present study, two distinct groups were drawn from the 179 completers. A first group with remitted depression was composed of individuals who experienced at least one previous major depressive episode. Of these 71 individuals, we excluded those who were currently experiencing major depression (n = 6) or who had a lifetime history of mania or hypomania (n = 10). The final group of remitted depressed participants was therefore comprised of 55 individuals. A normal control group was also drawn from the sample of 179 completers and was composed of participants who did not meet lifetime criteria for any psychiatric illness. The final group of normal controls comprised 55 individuals. The remaining 53 completers did not meet criteria for inclusion in either the remitted depressed or the normal control group and were not included in the analyses.
Procedure
During the first phase, the initial sample of 1,712 individuals was asked to complete a screening battery including an assessment of recent substance use and cognitive vulnerabilities for depression. Eligible participants were identified based on the presence of high or low cognitive vulnerability for depression (attributional style, sociotropy, autonomy), and frequent or infrequent recent substance use over the previous month (Husky et al. 2007) A portion of participants within each eligible group was randomly selected to participate in the ambulatory monitoring phase, using the Experience Sampling Method (ESM) (Csikszentmihalyi and Larson 1987; de Vries 1992). A 15-min ESM training session was provided by members of the research team. Participants were instructed to carry a hand-held Psion ‘Revo’ computer throughout the day for seven consecutive days. When signaled by the computer, each participant completed a computerized questionnaire concerning depressed mood, the experience of different types of daily life events, the perceived stressfulness of these events, as well as diverse behavioral and contextual variables. Over the following 7 days, the ESM signals occurred five times per day at fixed intervals (randomized across participants) within each of the following time periods: 8:00 am to 11:00 am; 11:00 am to 2:00 pm; 2:00 pm to 5:00 pm; 5:00 pm to 8:00 pm; and 8:00 pm to 11:00 pm. The duration of the electronic questionnaire at each assessment was approximately 1 min and 30 s, and all entries were time-stamped. A one-week period was chosen to assess adequately both work and leisure experiences (i.e., including both work days and weekends). Multiple assessments per day (every 3 h, on average) were used to assess the time-limited associations of minor stressors and mood states that occur over the course of the day (Swendsen 1998). The start day for the study was counterbalanced across the different workdays of the week, and all participants were contacted by telephone approximately halfway through the assessment period to monitor and encourage compliance.
In the final phase of the study, the micro-computer was returned and its databases uploaded. A structured diagnostic interview was then administered to each participant by a clinical psychologist blind to the selection criteria, and each participant received 75 Euros for completing the study.
Materials
Clinical and Cognitive Vulnerability Measures
Cognitive Vulnerabilities to Depression
Attributional style was assessed with the Attributional Style Questionnaire-Extended (Alloy et al. 1988; Haeffel et al. 2008). The ASQ-E is a self-report questionnaire in which the participant is asked to identify and rate the cause of 12 hypothetical events on their level of internality, stability and globality, as well as the importance of each event. The French validation of this instrument demonstrated satisfactory psychometric properties (Swendsen and Blatier 1998). In the present screening sample, both stability and globality had high internal consistencies (α = .83 and .82, respectively), and a generality index was calculated by averaging all items for these two subscales. Sociotropy and autonomy were measured using the Sociotropy-Autonomy Scale (Beck et al. 1983). In this 60-item self-report questionnaire, the respondent is asked to indicate the percentage of time during which each item applies to him or her on a 5-point scale. The French version (Husky et al. 2004) demonstrated alpha coefficients similar to those obtained in the original instrument. In the present screening sample, sociotropy and autonomy had Cronbach alphas of .87 and .78, respectively.
Substance Use Frequency
The frequency of substance use over the previous 30 days was examined through a self-report questionnaire assessing 11 different psychoactive substances including tobacco, alcohol, cannabis, ecstasy, amphetamines, heroine, cocaine, LSD and other hallucinogens. For each of these substances, respondents were asked to specify the frequency at which he or she had used the given substance during the past 30 days, with scores ranging from 1 (Never in the past 30 days) to 7 (Several times a day).
Diagnostic Status
Clinical interviews using the Mini International Neuropsychiatric Interview (MINI) Version 4.4 for DSM-IV (Sheehan et al. 1998) were conducted by trained psychologists blind to both the risk status of participants as well as to their responses collected during the ESM phase of the study. The MINI is a brief structured screening interview similar to the Structured Clinical Interview for DSM-IV (First et al. 1996) and the Composite International Diagnostic Interview (Wittchen et al. 1994) in design and developed to be used in non-clinical populations (Lecrubier et al. 1997). The reliability and validity of the MINI have been assessed in studies of persons with psychiatric symptoms in the US and in France showing that the MINI diagnoses had high inter-rater and test-retest reliability (Lecrubier et al. 1997; Sheehan et al. 1998).
ESM Electronic Assessments
Perceived Stressfulness of Daily Events
Using an open-ended question, participants were instructed to describe in a few words the event that affected them the most since the last signal (covering the previous three hours, on average). Participants were asked to rate the stressfulness of each event on a 7-point Likert scale from 1 (Not at all) to 7 (Extremely stressful).
Depressed Mood State
Depressed mood states were assessed using a 7-point Likert scale on which participants evaluated their mood at the moment each signal occurred, ranging from 1 (Not at all depressed) to 7 (Extremely depressed).
Overview of Analyses
Analyses were conducted using the Hierarchical Linear and Nonlinear Modeling program (Raudenbush et al. 2001). HLM treats the multiple observations gathered for each participant as ‘Level 1’ data that are conceptualized as nested within individuals as ‘Level 2’.
The impact of depression history and gender on between-person differences in the average level of either depressed mood or the stressfulness of events was examined by means-as-outcomes models. This model can be described at Level 1 by the following equation:
in which Depressed Moodij is the Depressed Mood score at observation i for person j; the intercept β0j is the individual’s average Depressed Mood score; and rij is the error term associated with observation i for person j.
The intercept can be explained at level 2 by the following equation:
in which γ00 is the overall intercept; γ01 is the main effect of Gender on β0j; γ02 is the main effect of Prior Depression on β0j; γ03 is the main effect Attributional Style on β0j; γ04 is the main effect of Sociotropy on β0j; γ05 is the main effect of Autonomy on β0j; γ06 is the main effect of Substance Use on β0j; and u0j is the unique increment to the intercept associated with person j.
In order to determine emotional reactivity to stress, associations between depressed mood and daily stress were examined by an intercept-and-slopes-as-outcomes model. Depressed mood scores at level 1 can be described by the following equation:
in which Depressed Moodij is the depressed mood score at observation i for person j; the intercept β0j is the expected mood score for person j when the Daily Stress score is 0; the slope β1j is the expected change in mood score for person j for an increase in the severity of daily stress; Daily Stressij is the severity score of daily stress at observation i for person j; and rij is the error term associated with observation i for person j.
The intercepts and slopes can be explained at level 2 by the following equations:
in which γ00 is the overall intercept; γ01 is the main effect of Gender on β0j; γ02 is the main effect of Prior Depression on β0j; γ03 is the main effect Attributional Style on β0j; γ04 is the main effect of Sociotropy on β0j; γ05 is the main effect of Autonomy on β0j; γ06 is the main effect of Substance Use on β0j; and u0j is the unique increment to the intercept associated with person j; and γ10 is the overall main effect of Daily Stress; γ11 is the cross level interaction term for Gender and Daily Stress; γ12 is the cross level interaction term for Prior Depression and Daily Stress; γ13 is the cross level interaction term for Attributional Style and Daily Stress; γ14 is the cross level interaction term for Sociotropy and Daily Stress; γ15 is the cross level interaction term for Autonomy and Daily Stress; γ16 is the cross level interaction term for Substance Use and Daily Stress; and u1j is the unique increment to the slope associated with person j.
In order to identify interactions effects, the models were then run using an additional Gender X Prior Depression interaction term at level 2. These analyses, like all others, controlled for Sociotropy, Autonomy, Attributional Style, and Substance Use.
Emotional reactivity was also examined in additional stratified analyses performed in the prior depression versus healthy control, and women versus men samples. These models are similar to those presented above.
Results
Table 1 presents the demographic and clinical characteristics of the group with a past history of depression and the control group. No between-group differences were found in age, gender, or the severity of cognitive vulnerabilities. In the remitted depression group, the average number of prior episodes was 3.4 (SD = 2.9), and the average age of onset was 15 years old (SD = 2.9).
The majority of this group (61%) experienced more than one previous episode. Those with a remitted depression were more frequent substance users, χ2(1) = 9.46, P < .01. Concerning comorbidity, 43.6% and 34.5% of this group met lifetime criteria for anxiety or substance use disorders, respectively. An analysis of the ESM data demonstrated that the sample as a whole provided 3,475 valid observations across diverse daily life contexts. Participants missed an average of 3.4 observations out of the 35 possible, and no significant difference between those with remitted depression and the control subjects was observed in the frequency of missing data.
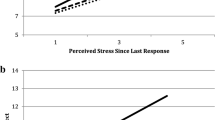
Controlling for cognitive vulnerabilities and recent substance use, a means-as-outcome analysis revealed that women appraised daily events as being more negative on average than men (γ01 = 0.369, t = 2.190, P < .05). Prior depression status also increased the perceived stressfulness of daily events (γ02 = 0.372, t = 2.003, P < .05). The determinants of overall depressed mood levels and emotional reactivity to stress were examined by an intercept-and-slopes-as-outcomes model (Table 2), again controlling for cognitive vulnerabilities and substance use. Women experienced higher depressed mood as compared to men (γ01 = 0.450, t = 3.172, P = <.01), as well as greater emotional reactivity to daily stressors (γ01 = 0.142, t = 3.584, P = <.001). With respect to the main effects of depression history, healthy controls and those with prior depression did not differ in depressed mood levels across the assessment week (γ02 = −0.030, t = −0.194, P > 05). However, those with prior depression were more emotionally reactive to events perceived as stressful as compared to healthy controls (γ02 = 0.071, t = 1.965, P = <.05). A similar analysis was then performed including an interaction term for gender by prior depression. This interaction was significant (γ03 = −0.142, t = −1.961, P = <.05) indicating that gender differences in emotional reactivity to daily stressors were greater in the healthy control group who never experienced depression (see Fig. 1). Within-group comparisons further demonstrated that this effect was mainly attributable to increases in emotional reactivity to stress in men with prior depression relative to men without prior depression (γ02 = 0.164, t = 3.495, P < .001), while no significant difference was observed for women between the group with prior depression and the healthy controls (γ02 = 0.008, t = 0.172, P > 05).

Gender by prior depression interaction in emotional reactivity to stress
Discussion
Stressful life events and female gender are each risk factors for the onset of first episodes of depression, but appear to be less associated with the onset of subsequent episodes (Kessler et al. 1993; Monroe and Harkness 2005; Nolen-Hoeksema 1990) The present controlled investigation examined whether these patterns may reflect the capacity of depression to induce changes in emotional reactivity to negative events, and whether this effect may differ in men and women.
Concerning main effects, gender had salient effects on all outcomes studied. Compared to men, women demonstrated higher depressed mood averages, rated events as being more negative, and experienced greater depressed emotional reactivity following events of equivalent impact. Although gender effects in depression may be explained by cognitive styles in women that enhance predispositions to this disorder (Nolen-Hoeksema et al. 1999), it is important to note that these analyses controlled for attributional style and sociotropy-autonomy traits, all well-documented psychological risk factors for depression (Alloy et al. 2000; Clark et al. 1992; Metalsky et al. 1993; Nietzel and Harris 1990; Robins and Block 1988; Rude and Burnham 1993; Swendsen 1998). In addition, the observed gender effects were independent of recent substance use, an important confounding factor given that men more often use specific substances as a means of regulating negative emotions (Swendsen et al. 2000). As may be expected by the selection of participants on the basis of previous or remitted depression, no differences were observed between healthy controls and previously depressed individuals concerning overall depressed mood levels. However, formerly depressed persons perceived events as being more negative than normal controls. This observation is similar to other ambulatory monitoring studies of persons with current major depression (Peeters et al. 2003), but indicates that the cognitive biases potentially induced by depression may extend to the phase of remission and constitute a vulnerability for future relapse. Past depression was also associated with increased emotional reactivity to daily events, a finding that differs from research on currently depressed individuals and that is inconsistent with the notion of a diminished role of stress in subsequent episodes. In this regard, the decreased emotional reactivity or affective blunting observed in currently depressed patients (Peeters et al. 2003) may not characterize these same individuals when depression is remitted. Moreover, while major life events appear to be less predictive of a depression relapse than they are of a first episode of this disorder (Cassano et al. 1989; Ghaziuddin et al. 1990; Mazure 1998), the present findings argue against the conclusion that depression renders individuals less sensitive to the effects of stress. Rather, an alternative interpretation for this pattern is that prior episodes of depression actually increase sensitivity to stress, including events of considerably lower magnitude. Subsequent episodes of depression may therefore occur in the absence of major life events, while still remaining strongly associated with stress.
Perhaps the most novel finding of this investigation concerns evidence for an interaction between depression history and gender. The effect of past depression on stress sensitization was stronger in men than in women, and gender differences in emotional reactivity were observed only in the healthy control group and not in those with prior depression. Moreover, analyses stratified by gender suggest that this pattern is likely to be attributable mainly to changes in stress reactivity among men. Specifically, men in the remitted depression group were significantly more reactive to negative events than men who had never been depressed, while no differences were observed for women across these groups. This finding parallels results from a longitudinal study of young adults showing that in men with prior depression only, negative attributional style was predictive of psychopathology at follow-up (Lewinsohn et al. 2000). Gender effects had also been observed in adolescents where the vulnerability-stress interaction predicted BDI scores only for boys and not for girls (Hankin et al. 2001). Further, our finding may help to explain why gender differences in rates of depression change as a function of prior episodes (Kendler et al. 2001; Kessler 2000, 2003; Kessler and McLeod 1984), and indicate that a prior episode of this disorder renders men and women more equivalent in terms of vulnerability to depression.
A strength of the present study is its use of the Experience Sampling Method (ESM), which is adapted to the assessment of more common forms of stress that are largely inaccessible to questionnaire or interview-based instruments. The numerous observations collected per individual using this technique also allow depressed mood changes to be examined from a within-person perspective, an approach which has been under-utilized as compared to analyses based solely on between-person variance. A limitation of ambulatory monitoring, however, is that the objective stress exposure is difficult to verify and therefore the findings should be interpreted only within the context of perceived stress. The focus on perceived stress in this investigation does not permit us to rule out that the daily lives of those with prior depression comprised more objective stressors as suggested by the stress generation hypothesis (Hammen 1991). It is also important to note that given the young age of the sample, the possibility exists that different associations may be observed among older individuals or those with more extensive depression histories. Further, in interpreting these findings it is important to consider the possibility that the differences in emotional reactivity in men with and without a history of depression may be due to unknown factors not identified in this study, rather that due to their experience of major depression alone. Finally, although depressed mood is a core feature of major depression, different findings may be observed for other specific symptoms of this disorder. The findings nonetheless provide support for the notion that past depression affects stress reactivity differentially in men and women, and may therefore help to provide an explanation for changes in the risk posed by gender and stress for first versus subsequent episodes. Identifying the mechanisms underlying these changes may lead to the development of possible gender-based interventions for reducing recurrence rates.
References
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory-based subtype of depression. Psychological Review, 96, 358–372. doi:10.1037/0033-295X.96.2.358.
Alloy, L. B., Abramson, L. Y., Hogan, M. E., Whitehouse, W. G., Rose, D. T., Robinson, M. S., et al. (2000). The temple-wisconsin cognitive vulnerability to depression project: Lifetime history of axis I psychopathology in individuals at high and low cognitive risk for depression. Journal of Abnormal Psychology, 109(3), 403–418. doi:10.1037/0021-843X.109.3.403.
Alloy, L. B., Abramson, L. Y., Metalsky, G. I., & Hartlage, S. (1988). The hopelessness theory of depression: Attributional aspects. The British Journal of Clinical Psychology, 27(1), 5–21.
Almeida, D. M., & Kessler, R. C. (1998). Everyday stressors and gender differences in daily distress. Journal of Personality and Social Psychology, 75(3), 670–680. doi:10.1037/0022-3514.75.3.670.
Beck, A. T. (1983). Cognitive therapy of depression: New perspectives. In P. Clayton & J. Barrett (Eds.), Treatment of depression: Old controversies and new approaches (pp. 265–290). New York: Raven Press.
Beck, A. T. (1987). Cognitive models of depression. Journal of Cognitive Psychotherapy: An International Quarterly, 1, 5–37.
Beck, A. T., Epstein, N., Harrison, R. P., & Emery, G. (1983). Development of the Sociotropy-Autonomy Scale: A measure of personality factors in psychopathology. Unpublished Manuscript.
Cassano, G. B., Akiskal, H. S., Musetti, L., Perugi, G., Soriani, A., & Mignani, V. (1989). Psychopathology, temperament, and past course in primary major depressions. Psychopathology, 22(5), 278–288.
Clark, D. A., Beck, A. T., & Brown, G. K. (1992). Sociotropy, autonomy, and life event perceptions in dysphoric and non-dysphoric individuals. Cognitive Therapy and Research, 16, 635–652. doi:10.1007/BF01175404.
Csikszentmihalyi, M., & Larson, R. (1987). Validity and reliability of the experience-sampling method. The Journal of Nervous and Mental Disease, 175(9), 526–536. doi:10.1097/00005053-198709000-00004.
de Vries, M. W. (1992). The experience of psychopathology: Investigating mental disorders in their natural settings. New York: Cambridge University Press.
First, M. B., Spitzer, R. L., Gibson, M., & Williams, J. B. (1996). Structured clinical interview for DSM-IV. Washington, DC: American Psychiatric Association.
Gable, S. L., Reis, H. T., & Elliot, A. J. (2000). Behavioral activation and inhibition in everyday life. Journal of Personality and Social Psychology, 78(6), 1135–1149.
Ghaziuddin, M., Ghaziuddin, N., & Stein, G. S. (1990). Life events and the recurrence of depression. Canadian Journal of Psychiatry, 35(3), 239–242.
Gotlib, I. H., Lewinsohn, P. M., Seeley, J. R., Rohde, P., & Redner, J. E. (1993). Negative cognitions and attributional style in depressed adolescents: An examination of stability and specificity. Journal of Abnormal Psychology, 102, 607–615.
Haeffel, G. J., Gibb, B. E., Metalsky, G. I., Alloy, L. B., Abramson, L. Y., Hankin, B. L., et al. (2008). Measuring cognitive vulnerability to depression: Development and validation of the cognitive style questionnaire. Clinical Psychology Review, 28(5), 824–836.
Hammen, C. L. (1991). Generation of stress in the course of unipolar depression. Journal of Abnormal Psychology, 100, 555–561.
Hankin, B. L., Abramson, L. Y., & Siler, M. (2001). A Prospective test of the hopelessness theory of depression in adolescence. Cognitive Therapy and Research, 25(5), 607–632.
Husky, M. M., Grondin, O. S., & Compagnone, P. (2004). Validation de la version française du questionnaire de sociotropie-autonomie de Beck et al. (1983). Canadian Journal of Psychiatry, 49, 851–858.
Husky, M. M., Mazure, C. M., Maciejewski, P. K., & Swendsen, J. D. (2007). A daily life comparison of sociotropy-autonomy and hopelessness theories of depression. Cognitive Therapy and Research, 31(5), 659–676.
Kendler, K. S., Kessler, R. C., Walters, E. E., MacLean, C., Neale, M. C., Heath, A. C., et al. (1995). Stressful life events, genetic liability, and onset of an episode of major depression in women. American Journal of Psychiatry, 152, 833–842.
Kendler, K. S., Thornton, L. M., & Prescott, C. A. (2001). Gender differences in the rates of exposure to stressful life events and sensitivity to their depressogenic effects. American Journal of Psychiatry, 158, 587–593.
Kessler, R. C. (2000). Gender difference in major depression: Epidemiology findings. In E. Frank (Ed.), Gender and its effect in psychopathology (pp. 61–84). Washington, DC: American Psychiatric Press.
Kessler, R. C. (2003). Epidemiology of women and depression. Journal of Affective Disorders, 74, 5–13.
Kessler, R. C., McGonagle, K. A., Swartz, M., Blazer, D. G., & Nelson, C. B. (1993). Sex and depression in the National Comorbidity Survey: I. Lifetime prevalence, chronicity and recurrence. Journal of Affective Disorders, 29(2–3), 85–96.
Kessler, R. C., & McLeod, J. D. (1984). Sex differences in vulnerability to undesirable events. American Sociological Review, 49, 620–631.
Lecrubier, Y., Sheehan, D. V., Weiller, E., Amorim, P., Bonora, I., Harnett Sheehan, K., et al. (1997). The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: Reliability and validity according to the CIDI. European Psychiatry, 5, 224–231.
Lewinsohn, P. M., Rohde, P., Seeley, J. R., Klein, D. N., & Gotlib, I. H. (2000). Natural course of adolescent major depressive disorder in a community sample: Predictors of reccurrence in young adults. American Journal of Psychiatry, 157(10), 1584–1591.
Maciejewski, P. K., Prigerson, H. G., & Mazure, C. M. (2001). Sex differences in event-related risk for major depression. Psychological Medicine, 31, 593–602.
Marco, C. A., Neale, J. M., Schwartz, J. E., Shiffman, S., & Stone, A. A. (1999). Coping with daily events and short-term mood changes: An unexpected failure to observe effects of coping. Journal of Consulting and Clinical Psychology, 67, 755–764.
Mazure, C. M. (1998). Life stressors as risk factors in depression. Clinical Psychology: Science and Practice, 5, 291–313.
Merikangas, K. R., Mehta, R. L., Molnar, B. E., Walters, E. E., Swendsen, J. D., Aguilar-Gaziola, S., et al. (1998). Comorbidity of substance use disorders with mood and anxiety disorders: Results of the international consortium in psychiatric epidemiology. Addictive Behaviors, 23(6), 893–907.
Metalsky, G. I., Joiner, T. E. J., Hardin, T. S., & Abramson, L. Y. (1993). Depressive reactions to failure in a naturalistic setting: A test of the hopelessness and self-esteem theories of depression. Journal of Abnormal Psychology, 102, 101–109.
Monroe, S. M., & Harkness, K. L. (2005). Life stress, the “Kindling” hypothesis, and the recurrence of depression: Considerations from a life stress perspective. Psychological Review, 112(2), 417–445.
Monroe, S. M., Slavich, G. M., Torres, L. D., & Gotlib, I. H. (2007). Major life events and major chronic difficulties are differentially associated with history of major depressive episodes. Journal of Abnormal Psychology, 116(1), 116–124.
Nietzel, M. T., & Harris, M. J. (1990). Relationship of dependency and achievement/autonomy to depression. Clinical Psychology Review, 10, 279–297.
Nolen-Hoeksema, S. (1990). Sex differences in depression. Stanford, CA: Stanford University Press.
Nolen-Hoeksema, S., Larson, J., & Grayson, C. (1999). Explaining the gender difference in depressive symptoms. Journal of Personality and Social Psychology, 77(5), 1061–1072.
Peeters, F., Nicolson, N. A., Berkhof, J., Delespaul, P., & de Vries, M. (2003). Effects of daily events on mood states in major depressive disorder. Journal of Abnormal Psychology, 112(2), 203–211.
Raudenbush, S. W., Bryk, A. S., Cheong, Y. F., & Congdon, R. T. (2001). HLM 5 Hierarchical linear and nonlinear modeling. Lincolnwood, IL: Scientific Software International, Inc.
Robins, C. J., & Block, P. (1988). Personal vulnerability, life events, and depressive symptoms: A test of a specific interactional model. Journal of Personality and Social Psychology, 54(5), 847–852.
Rude, S. S., & Burnham, B. L. (1993). Do interpersonal and achievement vulnerabilities interact with congruent events to predict depression? Comparison of DEQ, SAS, DAS, and combined scales. Cognitive Therapy and Research, 17, 531–548.
Scher, C. D., Ingram, R. E., & Segal, Z. V. (2005). Cognitive reactivity and vulnerability: Empirical evaluation of construct activation and cognitive diathesis in unipolar depression. Clinical Psychology Review, 25, 487–510.
Segal, Z. V., Williams, J. M., Teasdale, J. D., & Gemar, M. (1996). A cognitive science perspective on kindling and episode sensitization in recurrent affective disorder. Psychological Medicine, 26, 371–380.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., et al. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59(20), 22–33.
Spangler, D. L., Simons, A. D., Monroe, S. M., & Thase, M. E. (1997). Comparison of cognitive models of depression: Relationships between cognitive constructs and cognitive diathesis-stress match. Journal of Abnormal Psychology, 106(3), 395–403.
Swendsen, J. D. (1998). The experience of anxious and depressed moods in daily life: An idiographic and cross-situational test of the Helplessness-Hopelessness theory. Journal of Personality and Social Psychology, 74, 1398–1408.
Swendsen, J. D., & Blatier, C. M. (1998). Styles cognitifs et attributionnels dépressogènes: Validation d’un questionnaire traduit en langue française. Revue Internationale de Psychologie Sociale, 1, 89–97.
Swendsen, J. D., Tennen, H., Carney, M. A., Affleck, G., Willard, A., & Hromi, A. (2000). Mood and alcohol consumption: An experience sampling test of the self-medication hypothesis. Journal of Abnormal Psychology, 109(2), 198–204.
Wittchen, H. U., Zhao, S., Kessler, R. C., & Eaton, W. W. (1994). DSM-III-R Generalized Anxiety Disorder in the National Comorbidity Survey. Archives of General Psychiatry, 51, 335–364.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Husky, M.M., Mazure, C.M., Maciejewski, P.K. et al. Past Depression and Gender Interact to Influence Emotional Reactivity to Daily Life Stress. Cogn Ther Res 33, 264–271 (2009). https://doi.org/10.1007/s10608-008-9212-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10608-008-9212-z