
Abstract
Although childhood shyness has been linked to social anxiety problems, the factors playing a role in this association have gone largely unexplored. Here we examined the potential moderating roles of sex and age on this relation in a sample of 119 (75 girls) children (10–12 years) and adolescents (14–16 years). As predicted, shyness was positively associated with social anxiety symptoms. Sex, but not age, served as a moderating factor in linking shyness and social anxiety. Specifically, shyness was more strongly associated with social anxiety symptoms among girls than boys. These results suggest the importance of considering sex differences when examining the relation between shyness and social anxiety in childhood and adolescence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Temperamental shyness is a stable personality trait that refers to a preoccupation with the self in response to real or imagined social interactions [1]. Early childhood shyness is associated with a range of social, emotional, and adjustment difficulties. For example, shy children are prone to experiencing poor peer relations, including peer rejection, social exclusion, and victimization, as well as deficits in social competence [2]. In addition, shyness in early childhood is a known risk factor for internalizing problems such as depression and anxiety [2].
Previous studies have linked shyness and behavioral inhibition in early childhood to the later development of social anxiety disorder (SAD; e.g., [3–6]). Behavioral inhibition is a temperamental construct closely related to shyness, which is characterized by reticence and withdrawal from novel social and nonsocial situations [7]. For example, Chronis-Tuscano and colleagues [3] reported that early behavioral inhibition was associated with increased risk for a lifetime diagnosis of SAD, but not other diagnoses, during adolescence. In a different study, the rate of lifetime SAD was found to be greater among behaviorally inhibited children compared to behaviorally uninhibited children [5]. The existing literature also provides strong empirical support for the relation between shyness and a broader spectrum of anxiety problems (e.g., [8, 9]).
Although shyness and social anxiety share similar symptomatology, the two constructs differ markedly in a number of ways. First, prevalence rates of shyness are estimated at 61% [10] while prevalence rates of social anxiety are estimated at 7% [11]. Second, shyness is subsyndromal and is often a transitory phenomenon (e.g., [12]) whereas social anxiety is thought to be a chronic, unremitting condition [13]. Finally, individuals who are shy, on average, do not experience the degree of functional impairment that is experienced by individuals with social anxiety [14]. Thus, shyness and social anxiety are not completely synonymous and should be examined as separate constructs.
Although temperamental shyness is a risk factor for the development of social anxiety, not all temperamentally shy children develop social anxiety problems [15]. Given this variability, researchers have begun to explore various factors that may help explain the heterogeneity of psychological outcomes observed among shy children. Two potential moderating factors that have not been fully explored are sex and age. Sex and age are important factors to consider because they both contribute to individual differences in shyness and social anxiety problems. In addition, as shyness and social anxiety problems change from childhood to adolescence, it is critical to examine age differences in order to chart the developmental course of the relation between shyness and social anxiety problems.
Sex Differences
Girls are known to be at greater risk than boys for anxiety disorders [16]. This divergence begins at an early age, and twice as many girls than boys have experienced an anxiety disorder by the age of 6 years [17]. Sex differences are maintained and may even increase throughout development, reaching ratios of 2:1–3:1 in adolescence (e.g., [18, 19]).
Sex differences in childhood behavioral inhibition and shyness in relation to anxiety have also been reported. In early childhood, shy girls have more problems regulating negative emotions than shy boys [20]. In late childhood and early adolescence, girls show higher levels of behavioral inhibition than boys (e.g., [21]). Adolescent females who were inhibited as toddlers are more likely to have generalized social anxiety than males [22]. To date, there appears to be, however, only one study with adolescents that has examined the moderating influence of sex in relation to shyness and social anxiety problems. Hayward and colleagues [23] found that childhood shyness was more strongly associated with social anxiety in adolescent females compared to adolescent males. However, to the best of our knowledge, previous work has not examined this association with younger age groups. Given the sex differences in shyness and social anxiety problems, sex may be an important moderating influence to consider when examining the link between shyness and social anxiety problems.
Age-Related Differences
Previous research has also found that the type and content of anxiety varies with age. For example, adolescents report more social anxiety symptoms than children and symptoms increase with school grade level [24, 25]. Separation anxiety disorder is more common among children compared to adolescents (e.g., [26]). Furthermore, age-related changes in specific phobias are reflected in the types of fears that children and adolescents have. Children predominantly fear animals and adolescents predominantly fear failure and criticism [25].
With respect to age-related changes in childhood shyness, shyness displays moderate stability across development, particularly at the extremes (for a review, see [27]). In general, shyness and behavioral inhibition appear to be less stable during infancy and toddlerhood but increasingly so from early to middle childhood (e.g., [28]). However, there is also evidence for discontinuity of this trait, with some infants and toddlers who were extremely inhibited displaying less withdrawn social behavior as school-age children or adolescents (for a review, see [27]). As shyness and social anxiety problems change across development, it is important to consider the moderating influence of age on the relation between shyness and social anxiety problems in charting the course of this relation from childhood to adolescence.
The Present Study
To the best of our knowledge, previous research has not examined the moderating roles of sex and age in the link between shyness and social anxiety across childhood and adolescence. However, both sex and age have been linked to social anxiety (and other types of anxiety) directly. Accordingly, sex and age are likely to play important roles in the association between shyness and social anxiety problems. Moreover, there is a lack of research comparing age-related changes in the shyness-social anxiety relation between the periods of childhood and adolescence. As the transition from childhood to adolescence has been linked to a marked increase in psychopathology [1], and since childhood anxiety symptoms predict risk for adolescent anxiety [29], it is important to examine the differential impact of moderating factors during this vulnerable period in development. Evaluating the moderating influences of sex and age on the relation between shyness and social anxiety will provide insight into their potential as risk factors for social anxiety problems, aiding case conceptualization and assessment. As some but not all shy children develop social anxiety, identifying moderating factors in the link between shyness and social anxiety will inform the sex and age groups in which to intervene with treatment, potentially altering the course of the relation and reducing present and future social anxiety problems.
The purpose of the present study was to examine the potential moderating roles of sex and age on the relation between shyness and social anxiety problems using a cross-sectional design of children (10–12 years) and adolescents (14–16 years). To this end, we made three predictions. First, based on prior work (e.g., [3]), we predicted that shyness would be positively associated with social anxiety symptoms. Second, given the rates of social anxiety among girls compared to boys reported in the existing literature (e.g., [22]), we predicted that shyness would be more strongly associated with social anxiety symptoms among girls compared to boys. Third, based on previous findings that adolescents report more social anxiety than children (e.g., [24]), we predicted that shyness would be more strongly associated with social anxiety symptoms among adolescents compared to children.
Method
Participants
One hundred and nineteen participants (44 boys, 37%; 75 girls, 63%) and their parents were recruited from a large database that contained the birth records of healthy children born at two hospitals. Fifty-eight participants (20 boys, 34%; 38 girls, 66%) were children between 10 and 12 years, and 61 participants (24 boys, 39%; 37 girls, 61%) were adolescents between 14 and 16 years. At the time of assessment, the mean age of the participants was 12.92 years (SD = 2.23, range = 10–16 years). Exclusion criteria were left-handedness due to electrocortical measures obtained as part of a larger study, but not reported here. Descriptive information for the demographic variables is presented in Table 1. Children and adolescents did not differ with respect to ethnicity, parent marital status, or father’s education, but children’s mothers generally attained a higher level of education than adolescents’ mothers, χ2(4) = 12.09, p = .02. Seven participants (4 children, 3 adolescents) had a history of head injuries (without loss of consciousness) or seizures, and two participants (1 child, 1 adolescent) were taking mood-altering or anti-psychotic medications. These nine participants did not differ from the rest of the sample on the shyness and social anxiety measures, ts > −1.39, ps > 0.17, and thus were retained in the final sample to increase power. All procedures were approved by the Research Ethics Board of the University, and informed written consent and assent were obtained from parents and participants, respectively. During recruitment, parents were told that the study would be examining children’s brain responses to positive and negative feedback. Each participant and their parent completed a series of questionnaires as part of a larger study examining how shyness and sociability were related to behavior, brain function, and psychological outcomes.
Measures
Shyness
Participants’ shyness was assessed using parent-report on the Colorado Childhood Temperament Inventory (CCTI; Buss and Plomin [30], Rowe and Plomin [31]). The CCTI consists of 30 items, and parents indicated the degree to which each statement was true of their child (e.g., “child tends to be shy,” “child takes a long time to warm up to strangers”) along a 5-point Likert-type scale (not at all/strongly disagree = 0, a lot/strongly agree = 4). The CCTI yields six subscale scores including sociability, emotionality, activity level, attention, soothability, and shyness. The five items of the shyness subscale were used in the present study, and inter-item reliability was very good in this sample with α = 0.85.
Social Anxiety
Social anxiety symptoms were measured using the child- and parent-report versions of the Screen for Child Anxiety Related Emotional Disorders (SCARED; Birmaher et al. [32]). This measure consists of 41 items, and participants and their parents indicated the extent to which each statement was true (e.g., “I feel nervous with people I don’t know well/My child feels nervous with people he/she doesn’t know well,” “It is hard for me to talk with people I don’t know well/It is hard for my child to talk with people he/she doesn’t know well”) along a 3-point Likert-type scale (not true or hardly ever true = 0; true or often true = 2). The SCARED yields a total score and five subscale scores including somatic/panic symptoms, generalized anxiety, separation anxiety, school phobia, and social phobia. Of particular interest to the present study was the social phobia subscale, which indexes social anxiety symptoms and problems. Inter-item reliability was good in this sample with α = 0.84 (child) and 0.91 (parent). As the child-report social phobia subscale was significantly correlated with the parent-report social phobia subscale (r = .48, p < .001), child- and parent-reported scores for this subscale were averaged to create a composite social anxiety score. Collapsing across child- and parent-report is consistent with previous research [3, 33–36] and provides a more reliable, objective, multi-informant measure of social anxiety that takes into account the perspectives of both the parent and the child.
Data Analysis
In order to examine whether sex and age moderated the associations between shyness and social anxiety, two hierarchical regression analyses predicting the composite social anxiety score were performed separately for each moderator. For the model testing the moderating influence of sex, shyness (centered) and sex (0 = boys; 1 = girls) were entered as main effect variables at Step 1. In Step 2, the two-way interaction term was entered as a multiplicative product (shyness × sex). The same model was used to test the moderating influence of age except that age (centered) was substituted for sex. The results of multicollinearity tests revealed no significant problems with multicollinearity (shyness and age: tolerance = 0.96–1.00, VIF = 1.001–1.04; shyness and sex: tolerance = 0.32–0.98, VIF = 1.03–3.13). Significant interactions were followed up using the Aiken and West [37] method for testing simple effects.
To probe the number of shy participants who met the clinically significant threshold for social anxiety symptoms and problems by sex and age, separate Chi square analyses were conducted with low shy/high shy groups and clinically significant/not clinically significant groups among the two sex groups and two age groups. To maintain consistency with prior research (e.g., [35, 38, 39]) and facilitate data analyses, we computed a median split on the CCTI shyness scores to create two groups across all participants: low shy participants (n = 63, M = 1.65, SD = 0.39, range = 1–2.20) and high shy participants (n = 56, M = 3.06, SD = 0.53, range = 2.40–4.60). Participants were also divided into two groups with respect to the clinically significant threshold (i.e., score = 8; [32]) on the SCARED social phobia subscale: participants with composite social anxiety scores above or at the threshold (clinically significant group; n = 18, M = 10.39, SD = 1.74, range = 8.50–14), and participants with composite social anxiety scores below the threshold (not clinically significant group; n = 99, M = 4.25, SD = 2.20, range = 0–8).
Results
Descriptive Statistics
Descriptive statistics for the CCTI shyness scores and the SCARED social phobia subscale scores are displayed in Table 2. Correlations among the study variables are presented in Table 3. Consistent with expectations, shyness was significantly and positively associated with social anxiety symptoms as reported by both the participant and their parent.
Hierarchical Regression Analyses
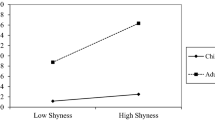
As predicted, there was a significant two-way interaction of shyness by sex on the composite social anxiety measure (see Fig. 1), β = 0.22, SE = 0.48, p = .04. A simple slopes analysis showed that shyness was significantly and positively associated with social anxiety symptoms and problems among girls, β = 0.81, SE = 0.28, p < .001, and boys, β = 0.54, SE = 0.39, p < .001. Furthermore, among low shy participants, social anxiety symptoms and problems did not vary significantly between girls and boys, β = 0.06, SE = 0.52, p = .46. In contrast, among shy participants, social anxiety symptoms and problems were significantly related to sex, such that girls reported more social anxiety symptoms and problems than boys, β = 0.32, SE = 0.60, p = .001.

Shyness by sex interaction on the composite measure of social anxiety symptoms and problems across childhood and adolescence
There were also significant separate effects of shyness, β = 0.54, SE = 0.39, p < .001, and sex, β = 0.19, SE = 0.39, p = .002, on the composite social anxiety measure. Overall, shy individuals reported more social anxiety symptoms and problems than low shy individuals among boys, and girls reported more social anxiety symptoms and problems than boys at the average level of shyness.
Contrary to expectations, there was no significant shyness by age interaction. However, there was a significant effect of shyness on the composite social anxiety measure, β = 0.74, SE = 0.24, p < .001. Overall, shy individuals reported more social anxiety symptoms and problems than low shy individuals at the average age of the sample.
Chi Square Analyses
Sex Differences
Girls who met the clinically significant threshold for the SCARED social phobia subscale were more likely to be shy. Of the 15 girls who reported clinically significant scores, 100% were in the high shy group, and none were in the low shy group, χ2(1) = 17.31, p < .001. There was no difference in clinically significant scores between high and low shy boys, χ2(1) = 1.35, p = .25.
Age Differences
Adolescents who met the clinically significant threshold for the SCARED social phobia subscale were more likely to be shy. Of the 12 adolescents who reported clinically significant scores, 11 were in the high shy group, and only one was in the low shy group, χ2(1) = 10.79, p = .001. In addition, children who met the clinically significant threshold for the SCARED social phobia subscale were more likely to be shy. Of the six children who reported clinically significant scores, 100% were in the high shy group, and none were in the low shy group, χ2(1) = 8.96, p = .003.
Discussion
We examined the potential moderating influences of sex and age on the relation between shyness and social anxiety problems among children and adolescents. Overall, shyness was positively associated with social anxiety symptoms, and girls reported more social anxiety symptoms than boys. Analyses provided support for sex, not age, as a moderating factor in the link between shyness and social anxiety problems. Specifically, shyness was more strongly associated with social anxiety symptoms among girls than boys. Girls with clinically significant social anxiety scores were more likely to be shy. In addition, both children and adolescents with clinically significant social anxiety scores were more likely to be shy. Our findings are in line with previous work and extend to a younger age group.
Shyness and Social Anxiety
Consistent with expectations, shyness was positively associated with social anxiety symptoms. We also found that both children and adolescents with clinically significant social anxiety scores were more likely to be shy. Shyness has been previously linked to higher levels of social anxiety problems in late adolescence and adulthood (e.g., [40–42]). The current results extend this relation to a younger age group and suggest that shy children feel socially anxious even during middle childhood and early to middle adolescence. Although shyness is related to social anxiety across the lifespan, one question that remains is whether shyness is more strongly associated with a specific type of SAD during different developmental periods. SAD is characterized by marked fear or anxiety about one or more social situations including social interactions, being observed, and performing in front of others [43]. There is also a performance only subtype of SAD where the fear is restricted to speaking or performing in public [43]. Symptom presentation of SAD varies by age group [44]. For example, adolescents with SAD endorse a broader pattern of social avoidance compared to their younger counterparts [44]. In addition, earlier classification of a child as inhibited is associated with generalized social anxiety, but not performance anxiety, in adolescence [22]. Given that adolescents report social anxiety across a broader range of situations, shyness may be more strongly associated with more generalized SAD among adolescents, and shyness may be more strongly associated with the performance only subtype of SAD among children. Future research should examine age-related fears about specific social situations to elucidate whether the relation between shyness and social anxiety varies by type of SAD across development.
Shyness and Sex Differences
As predicted, sex was a moderating factor of the relation between shyness and social anxiety problems. Specifically, shyness was more strongly associated with social anxiety symptoms among girls than boys. We also found that girls with clinically significant social anxiety scores were more likely to be shy. The moderating influence of sex in the link between shyness and social anxiety problems has previously been demonstrated in a sample of high school students [23]. The present study extends these findings to a younger age group and suggests that there are differential effects of sex on the relation between shyness and social anxiety problems as early as middle childhood and early to middle adolescence. This sex difference in the relation between shyness and social anxiety problems may reflect sex-specific societal expectations among boys and girls. Sex stereotypes describe boys as being active and outspoken and girls as being withdrawn and quiet [22]. Therefore, shy boys may be more noticeable to health care professionals and parents because their behavior deviates from societal expectations, whereas shy girls may be overlooked because their behavior corresponds to societal expectations [22]. As a result, shy girls may receive less direct and/or subliminal help from their environment, increasing their likelihood of developing SAD [22].
We also found that girls reported more social anxiety symptoms than boys overall. This result replicates earlier work supporting this sex difference in social anxiety problems (e.g., [22]). Sex differences in social anxiety problems may be explained by the different environmental variables that contribute to the development of social anxiety problems among males and females. Specifically, social anxiety problems among females are linked with parental conflicts, childhood physical abuse by a father figure, maternal mania, and failure to complete high school [45, 46]. In contrast, social anxiety problems among males are associated with the absence of a parent or adult confidant [45]. These findings suggest that there are many more risk factors for social anxiety problems among girls compared to boys, which may help to account for the higher prevalence of social anxiety problems among girls. However, it is important to note that the one risk factor for boys may be more common than some of the risk factors for girls, so the findings should be interpreted with reasonable scientific caution. While the present study did not examine the number of participants who experienced these risk factors, future research should consider the prevalence and impact of these environmental influences when examining sex differences in social anxiety problems.
Shyness and Age Differences
Contrary to expectations, age was not a moderating factor of the relation between shyness and social anxiety problems. The unstable nature of SAD among children and adolescents may account for this finding. Merikangas and colleagues [47] observed that no youth who had initially met diagnostic criteria for SAD met criteria continuously at each follow-up assessment. This considerable degree of fluctuation in the diagnostic status of SAD among children and adolescents may have impacted the reliability of social anxiety symptoms and thus the results.
In addition, there was no difference in social anxiety symptoms reported between children and adolescents. This finding may be explained by differences in the age ranges between the present study and earlier studies. Weems and Costa [25] found a significant difference in social anxiety symptoms between children aged 6–13 years and adolescents aged 14–17 years, and Weems and colleagues [48] reported similar findings between children aged 6–11 years and adolescents aged 12–17 years. As the median age at onset of SAD is 13 years [43], the developmentally closer age ranges of children and adolescents examined in the present study may have limited our ability to find a significant difference in social anxiety problems between groups.
Limitations
Several limitations of the present study should be noted. The cross-sectional nature of the study makes it difficult to infer the direction of causal relations among the study variables (e.g., whether social anxiety problems enhance shyness or whether shyness contributes to social anxiety problems). Another limitation concerns the use of self-report measures, which are known to have inherent biases and may have been difficult for the younger participants to accurately complete. The age range of the sample was limited, therefore restricting our capacity to test our hypotheses across a broader developmental range and limiting generalizability. Future studies should employ a longitudinal design and objective measures of the study variables (e.g., behavioral and psychophysiological measures) in order to ensure the reliability of these findings.
Conclusions and Future Directions
The results of the present study replicate and extend earlier work on the moderating influences of the relation between shyness and social anxiety problems to a broader age range than previously studied. Consistent with the existing literature, shyness was positively related to social anxiety symptoms. Both children and adolescents with clinically significant social anxiety scores were more likely to be shy, demonstrating the well-established relation between shyness and social anxiety problems across both developmental periods.
Consistent with the existing literature, girls reported more social anxiety symptoms than boys overall. The current findings also suggest that sex is a moderating factor of the relation between shyness and social anxiety problems. Specifically, shyness was more strongly associated with social anxiety symptoms among girls than boys. In addition, girls with clinically significant social anxiety scores were more likely to be shy. Taken together, these results suggest that prevention and intervention programs should target shy girls in order to reduce present and future social anxiety problems. The results of the present study may also be used to educate health care providers and parents about differences in the relation between shyness and social anxiety problems between girls and boys. Awareness of sex-specific environmental risk factors and societal expectations may assist them in recognizing girls at risk of developing SAD for referral to prevention programs.
Future research should examine moderating influences among children and adolescents who meet clinical criteria for SAD. In addition to sex and age, factors such as social competence, peer social support, and peer victimization should also be investigated. Collecting data from more developmental time points (e.g., from infancy to adulthood) may provide further insight into age-related changes in moderating influences throughout development. Furthermore, future studies should adopt an extreme group design to examine moderating effects only among extremely shy and extremely anxious individuals.
Summary
Although the link between shyness and social anxiety problems has been well established in the literature, the heterogeneity of psychological outcomes observed among shy children suggests that this relation may be moderated by various factors. The present study examined the potential moderating roles of sex and age on the relation between shyness and social anxiety in a sample of children and adolescents. Shyness was measured using parent-report on the CCTI and social anxiety symptoms were assessed using a composite measure of child- and parent-reported social anxiety scores on the SCARED. Consistent with expectations, shyness was positively associated with social anxiety symptoms. Analyses provided support for sex, but not age, as a moderating factor in the link between shyness and social anxiety. Specifically, shyness was more strongly associated with social anxiety symptoms among girls than boys. These findings extend earlier research on the relation between shyness and social anxiety problems to a broader age range than previously studied and suggest the importance of considering sex differences when examining the relation between shyness and social anxiety in childhood and adolescence.
References
Schmidt LA, Buss AH (2010) Understanding shyness: four questions and four decades of research. In: Rubin KR, Coplan RJ (eds) The development of shyness and social withdrawal. Guilford Publications, New York, pp 23–41
Rubin KH, Coplan RJ, Bowker JC (2009) Social withdrawal in childhood. Annu Rev Psychol 60:141–171
Chronis-Tuscano A, Degnan KA, Pine DS, Perez-Edgar K, Henderson HA, Diaz Y et al (2009) Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J Am Acad Child Adolesc Psychiatry 48:928–935
Hayward C, Killen JD, Kraemer HC, Taylor CB (1998) Linking self-reported childhood behavioral inhibition to adolescent social phobia. J Am Acad Child Adolesc Psychiatry 37:1308–1316
Hirshfeld-Becker DR, Biederman J, Henin A, Faraone SV, Davis S, Harrington K et al (2007) Behavioral inhibition in preschool children at risk is a specific predictor of middle childhood social anxiety: a five-year follow-up. J Dev Behav Pediatr 28:225–233
Stemberger RT, Turner SM, Beidel DC, Calhoun KS (1995) Social phobia: an analysis of possible developmental factors. J Abnorm Psychol 104:526–531
Kagan J, Reznick JS, Snidman N (1988) Biological bases of childhood shyness. Science 240:167–171
Hirshfeld DR, Rosenbaum JF, Biederman J, Bolduc EA, Faraone SV, Snidman N et al (1992) Stable behavioral inhibition and its association with anxiety disorder. J Am Acad Child Adolesc Psychiatry 31:103–111
Prior M, Smart D, Sanson A, Oberklaid F (2000) Does shy-inhibited temperament in childhood lead to anxiety problems in adolescence? J Am Acad Child Adolesc Psychiatry 39:461–468
Henderson L, Zimbardo P (1993) Self-blame attributions in shys vs. non-shys in a high-school sample. Paper presented at the annual conference of the Anxiety Disorders Association of America, Charleston, SC
Beesdo K, Knappe S, Pine DS (2009) Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin N Am 32:483–524
Beidel DC, Turner SM (1999) The natural course of shyness and related syndromes. In: Schmidt LA, Schulkin JS (eds) Extreme fear, shyness, and social phobia: origins, biological mechanisms, and clinical outcomes. Oxford University Press, New York, pp 203–223
Turner SM, Beidel DC (1989) Social phobia: clinical syndrome, diagnosis and comorbidity. Clin Psychol Rev 9:3–18
Turner SM, Beidel DC, Townsley RM (1990) Social phobia: relationship to shyness. Behav Res Ther 28:497–505
Tang A, Santesso DL, Segalowitz SJ, Schmidt LA (2016) Distinguishing shyness and sociability in children: an event-related potential study. J Exp Child Psychol 142:291–311
Anderson JC, Williams S, McGee R, Silva PA (1987) DSM-III disorders in preadolescent children: prevalence in a large sample from the general population. Arch Gen Psychiatry 44:69–76
Lewinsohn PM, Gotlib IH, Lewinsohn M, Seeley JR, Allen NB (1998) Gender differences in anxiety disorders and anxiety symptoms in adolescents. J Abnorm Psychol 107:109–117
Pine DS, Cohen P, Gurley D, Brook J, Ma Y (1998) The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry 55:56–64
Wittchen HU, Nelson CB, Lachner G (1998) Prevalence of mental disorders and psychosocial impairments in adolescents and young adults. Psychol Med 28:109–126
Theall-Honey LA, Schmidt LA (2006) Do temperamentally shy children process emotion differently than nonshy children? Behavioral, psychophysiological, and gender differences in reticent preschoolers. Dev Psychobiol 48:187–196
Janson H, Mathiesen KS (2008) Temperament profiles from infancy to middle childhood: development and associations with behavior problems. Dev Psychol 44:1314–1328
Schwartz CE, Snidman N, Kagan J (1999) Adolescent social anxiety as an outcome of inhibited temperament in childhood. J Am Acad Child Adolesc Psychiatry 38:1008–1015
Hayward C, Wilson KA, Lagle K, Kraemer HC, Killen JD, Taylor CB (2008) The developmental psychopathology of social anxiety in adolescents. Depress Anxiety 25:200–206
Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE (2000) Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther 38:835–855
Weems CF, Costa NM (2005) Developmental differences in the expression of childhood anxiety symptoms and fears. J Am Acad Child Adolesc Psychiatry 44:656–663
Cartwright-Hatton S, McNicol K, Doubleday E (2006) Anxiety in a neglected population: prevalence of anxiety disorders in pre-adolescent children. Clin Psychol Rev 26:817–833
Degnan KA, Fox NA (2007) Behavioral inhibition and anxiety disorders: multiple levels of a resilience process. Dev Psychopathol 19:729–746
Pedlow R, Sanson A, Prior M, Oberklaid F (1993) Stability of maternally reported temperament from infancy to eight years. Dev Psychol 29:998–1007
Pine DS (2007) Research review: a neuroscience framework for pediatric anxiety disorders. J Child Psychol Psychiatry 48:631–648
Buss AH, Plomin R (1984) Temperament: early developing personality traits. Erlbaum, Hillsdale
Rowe DC, Plomin R (1977) Temperament in early childhood. J Pers Assess 41:150–156
Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M (1999) Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry 38:1230–1236
Guyer AE, Lau JY, McClure-Tone EB, Parrish J, Shiffrin ND, Reynolds RC et al (2008) Amygdala and ventrolateral prefrontal cortex function during anticipated peer evaluation in pediatric social anxiety. Arch Gen Psychiatry 65:1303–1312
Lahat A, Benson B, Pine DS, Fox NA, Ernst M (2016) Neural responses to reward in childhood: relations to early behavioral inhibition and social anxiety. Soc Cogn Affect Neurosci
Lahat A, Lamm C, Chronis-Tuscano A, Pine DS, Henderson HA, Fox NA (2014) Early behavioral inhibition and increased error monitoring predict later social phobia symptoms in childhood. J Am Acad Child Adolesc Psychiatry 53:447–455
Roy AK, Fudge JL, Kelly C, Perry JS, Daniele T, Carlisi C et al (2013) Intrinsic functional connectivity of amygdala-based networks in adolescent generalized anxiety disorder. J Am Acad Child Adolesc Psychiatry 52:290–299
Aiken LS, West SG (1991) Multiple regression: testing and interpreting interactions. Sage Publications, Thousand Oaks
Howarth GZ, Guyer AE, Pérez-Edgar K (2013) Young children’s affective responses to acceptance and rejection from peers: a computer-based task sensitive to variation in temperamental shyness and gender. Soc Dev 22:146–162
Lahat A, Walker OL, Lamm C, Degnan KA, Henderson HA, Fox NA (2014) Cognitive conflict links behavioral inhibition and social problem solving during social exclusion in childhood. Infant Child Dev 23:273–282
Chavira DA, Stein MB, Malcarne VL (2002) Scrutinizing the relationship between shyness and social phobia. J Anxiety Disord 16:585–598
Heiser NA, Turner SM, Beidel DC (2003) Shyness: relationship to social phobia and other psychiatric disorders. Behav Res Ther 41:209–221
Nelson LJ, Lee CT, Duan XX (2015) Associations between shyness and internalizing and externalizing problems during emerging adulthood in China. Emerg Adulthood 3:364–367
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association, Washington
Rao PA, Beidel DC, Turner SM, Ammerman RT, Crosby LE, Sallee FR (2007) Social anxiety disorder in childhood and adolescence: descriptive psychopathology. Behav Res Ther 45:1181–1191
DeWit DJ, Chandler-Coutts M, Offord DR, King G, McDougall J, Specht J et al (2005) Gender differences in the effects of family adversity on the risk of onset of DSM-III-R social phobia. J Anxiety Disord 19:479–502
Kessler RC, Foster CL, Saunders WB, Stang PE (1995) Social consequences of psychiatric disorders, I: educational attainment. Am J Psychiatry 152:1026–1032
Merikangas KR, Avenevoli S, Acharyya S, Zhang H, Angst J (2002) The spectrum of social phobia in the Zurich cohort study of young adults. Biol Psychiatry 51:81–91
Weems CF, Hammond-Laurence K, Silverman WK, Ginsburg GS (1998) Testing the utility of the anxiety sensitivity construct in children and adolescents referred for anxiety disorders. J Clin Child Psychol 27:69–77
Acknowledgements
This study was based on the first author’s undergraduate honours thesis conducted under the direction of L.A.S. This research was funded by Lawson Foundation and Banting Post-Doctoral Fellowships awarded to A.L., and operating grants from the Natural Sciences and Engineering Council of Canada (NSERC) and the Social Sciences and Humanities Research Council of Canada (SSHRC) awarded to L.A.S. The authors wish to thank Rachael Adcock, Raha Hassan, Lauren Poulin, Valerie Prowse, Anya Swain, Alva Tang, and Richard Xu for their help with data collection and data entry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tsui, T.Y.L., Lahat, A. & Schmidt, L.A. Linking Temperamental Shyness and Social Anxiety in Childhood and Adolescence: Moderating Influences of Sex and Age. Child Psychiatry Hum Dev 48, 778–785 (2017). https://doi.org/10.1007/s10578-016-0702-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-016-0702-z