
Abstract
Attention-deficit/hyperactivity disorder (ADHD) symptoms and aggressive behaviors are both associated with peer rejection, but little is known the nature of this association with respect to the two symptom dimensions of hyperactivity-impulsivity and inattention and different types of aggression. The present study examines the relations between dimensions of ADHD symptomatology, proactive and reactive aggression, and peer rejection in adolescence. Teacher-reported data were obtained for 200 high school students (grades 9–12; 48 % female; predominately Latino). In structural equation modeling path analyses, the indirect effects of reactive aggression accounted for the link between hyperactivity–impulsivity and peer rejection. Within the same model, neither inattention nor proactive aggression were associated with peer rejection. These findings suggest that reactive aggression may be a key mechanism through which hyperactive–impulsive behavior is associated with peer rejection. Future research and intervention efforts should address the role of reactive aggression among youth with ADHD symptomatology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is characterized by attention problems and hyperactive and impulsive behaviors that are developmentally inappropriate and lead to impairment in everyday functioning [1, 2]. In children and adolescents, inattention and hyperactivity–impulsivity are associated with a wide range of social problems, such as having fewer friends, bullying, victimization, and being viewed less favorably by peers [3–5]. In particular, there is strong evidence indicating that youth with ADHD symptoms are more likely to be rejected by their peers [e.g., 6, 7]. This peer rejection appears to be pervasive, impairing, and stable from childhood into adolescence [8, 9]. For example, even after controlling for diagnostic and behavioral risk factors, Mrug et al. [8] found that peer rejection in children diagnosed with ADHD independently predicted global impairment 8 years later in late adolescence.
Although the link between ADHD and peer rejection is well established, there may be numerous factors accounting for this association. Most fundamentally, ADHD is defined and diagnosed partially on the basis of social impairment—as one of the major domains of functional impairment—as well as several symptom criteria referring to socially inappropriate or disruptive behaviors [1, 2]. Indeed, hyperactivity, impulsivity, and inattention can naturally contribute to range of social difficulties, which can sometimes include peer rejection [4]. Given the heterogeneity of ADHD symptoms and the variety of ways they can present in children and adolescents, it is important to consider how these symptoms might contribute to peer rejection through different mechanisms.
However, much of the past research in this area has failed to separately examine the different dimensions of ADHD symptomatology, even though both of those dimensions are often invoked in the interpretation of the results. In addition, explanations that focus solely on social difficulties as a facet (rather than a correlate) of ADHD are inadequate for several reasons. First, they fail to account for the many children with attention deficits or hyperactive–impulsive behavior who do not experience peer rejection. Second, such accounts offer little understanding of the social, behavioral, and cognitive mechanisms that contribute to peer rejection. Finally, although much of the relevant research relates to populations of children diagnosed with ADHD, inattention and hyperactivity–impulsivity are dimensional variables that are associated with social difficulties irrespective of diagnostic status [10–12]. Consistent with a developmental psychopathology framework [13] and dimensional perspectives on ADHD [14], there is a need for research in clinical and nonclinical samples, with attention to categorical diagnoses as well as continuous measures of symptomatology and social functioning. With these considerations in mind, the goal of this investigation was to more closely examine the link between ADHD symptoms and peer rejection, including reactive aggression as a possible intervening mechanism.
Hyperactivity–Impulsivity, Inattention, and Peer Rejection
Several explanations have been offered to account for the link between ADHD symptoms and peer rejection. These accounts can generally be differentiated into two categories according to which of the ADHD symptom dimensions is emphasized as the key mechanism: attention problems or hyperactive–impulsive behaviors.
Attention problems can cause children to appear distracted, off-task, withdrawn, and shy in social situations [4, 5]. Children with attention problems are more likely to show deficits in social knowledge and social cognition. These deficits can contribute to behaviors that are socially problematic in that they may violate implicit social rules and appear immature, insensitive, or inappropriate [12, 15, 16]. Similarly, children with ADHD symptoms have difficulty attending to and understanding social cues [17], which may explain why they are more likely to interpret ambiguous social situations as hostile [18] and have difficulty generating appropriate solutions to social problems [19]. These social-cognitive deficits (especially problems with social comprehension and problem-solving) appear to follow children with ADHD into adolescence and continue to contribute to difficulties with peers [20].
Hyperactive–impulsive behaviors also show direct associations with social problems; youth with these symptoms are more likely than their peers to exhibit behavior that is negative, aggressive, disruptive, restless, intrusive, or annoying [4, 5]. In contrast to the social-cognitive mechanisms hypothesized for inattentive youth, the patterns of social impairment encountered by hyperactive and impulsive youth appear to be more directly related to performance deficits and difficulty inhibiting hyperactive–impulsive behaviors than to limited social knowledge or activity [4, 5]. In their review of the literature on ADHD and social dysfunction, Nijmeyer et al. [4] concluded that hyperactivity–impulsivity appears to contribute to social difficulties through at least two separate but related pathways. First, children who are hyperactive and impulsive are more likely to exhibit verbally and physically aggressive behaviors, which are strong predictors of negative peer ratings in children with and without ADHD. Second, these children are also likely to exhibit restless, intrusive, and disruptive behaviors, which can result in peer rejection independent of aggression. Indeed, youth with ADHD exhibit more aggressive behaviors than their peers [21], and aggression is uniquely related to difficulties in several aspects social functioning, including peer rejection [22].
Thus, of the various factors hypothesized to underlie peer rejection in children with ADHD symptoms, aggressive behaviors appear to play a critical role. More specifically, the literature suggests that aggression may act as a mediator in the link between hyperactive–impulsive behaviors and peer rejection. However, we could only identify one study to date which has tested this hypothesis directly. Tseng et al. [23] found evidence for a model in which physical, but not relational, aggression partially mediated the link between hyperactivity–impulsivity and impaired peer functioning in girls, but not in boys, over a period of 6 months. Although these findings are useful, the authors’ focus on the form of the aggressive behavior fails to elucidate its function, which is critical for understanding the mechanisms and consequences of disruptive behaviors. In particular, a better understanding of reactive, as opposed to proactive, aggression may help account for inconsistencies in the relationships between aggression and peer rejection [24, 25].
The Role of Reactive Aggression
Rather than being defined by specific forms of aggressive acts, reactive and proactive aggression are distinguished according to the motivation behind, or the intended function of, the aggressive behavior. Reactive aggression occurs as a response to a perceived threat; it is emotionally driven and defensive [26]. This function can be best explained by the frustration-aggression hypothesis, which describes aggression as a hostile and retaliatory response to perceived provocation or frustration [27, 28], essentially as a method for protecting oneself from another person who is perceived as a threat [29]. In contrast, proactive aggression refers to goal-oriented aggression that is motivated by external reward; it is instrumental, offensive, and requires no provocation or feelings of anger [26]. Proactive aggression is best explained by the social learning theory [30], which posits that aggressive behavior is acquired through observational learning and reinforcement processes, such that the aggressive behavior is motivated by the expectancy, and reinforced by the attainment, of a reward following an aggressive act. Despite the shared variance between reactive and proactive aggression, theoretical considerations and factor analytic methods support the proactive–reactive dichotomy [25, 31, 32].
Reactive and proactive aggression are differentially associated with ADHD symptom dimensions. Card and Little’s meta-analysis [11] found that reactive aggression shows a moderate correlation with ADHD symptoms, whereas the association between proactive aggression and ADHD symptoms was negligible. Similarly, Connor et al. [33] found that children with the hyperactive–impulsive or combined subtype of ADHD were more aggressive than those in the inattentive and control groups; further, these children showed much higher levels of reactive than proactive aggression. Longitudinal evidence indicates that hyperactivity–impulsivity at 6–7 years of age predicted aggressive behavior and social problems 9 years later at 16–18 years of age, even after controlling for baseline conduct problems [34]. Taken together, these findings suggest that the link between ADHD symptoms and aggression can be traced to a specific, directional association from hyperactive–impulsive symptoms to reactive aggression—an interpretation that is consistent with a neurodevelopmental view of ADHD symptoms [14] and a social information processing model of reactive aggression [18, 26].
Similarly, reactively and proactively aggressive behaviors differentially contribute to children’s social functioning in a number of ways. Children who are reactively aggressive experience less acceptance and greater rejection and victimization from their peers, compared to those who are proactively aggressive or nonaggressive [11, 35, 36]. In contrast, children who display mostly proactively aggressive behavior are more likely to be rated as popular by their peers [11, 35]. Reactively aggressive behaviors are also linked to fewer reciprocal friendships, as well as lower quality and higher conflict within dyadic friendships [37]. Experimental studies indicate that aggression leads to peer rejection, not the converse [38, 39]. However, the specific nature of the relations among hyperactive–impulsive symptoms, reactive aggression, and peer rejection remains unclear.
Finally, it is important to consider the role of gender and ethnicity for several reasons. Much of the research on aggression and ADHD focuses on participants who are predominately male and Caucasian or African American. Only recently have researchers devoted attention specifically to possible gender differences. For example, some studies suggest that attention problems are more commonly observed and more socially impairing in girls compared to boys [e.g., 23, 40]. Girls also seem to show more relational aggression while boys show more physical aggression, with little or no difference in proactive/reactive aggression [25]. However, less is known about how these behavior patterns might affect social functioning differently for boys and girls.
With respect to ethnicity, some research shows that ADHD symptoms are reported less frequently for Latino youth compared to other ethnic groups [41, 42], with similar patterns for diagnosis and treatment [43, 44]. While a number of different cultural factors (e.g., language barriers, perceptions of stigma, cultural differences in help seeking) may account for these differences [45, 46], research does support the construct validity of ADHD in Latino youth, including evidence that symptoms are associated with social impairment [47]. Additionally, Latino adolescents appear to show similar or somewhat more aggression compared all other ethnic groups except for African-Americans [48, 49]. A number of culturally relevant factors are associated with aggression, both positively (e.g., parent-adolescent conflict, perceived discrimination) and negatively (familism, involvement with culture of origin) [50]. However, research focusing on proactive and reactive aggression among Latino youth is limited, highlighting the need for further research.
In sum, the literature reviewed above suggests that reactive aggression may help account for the link between hyperactivity–impulsivity and peer rejection, but this hypothesis has not yet been tested empirically. Accordingly, the present study investigates the associations among ADHD symptom dimensions, functional subtypes of aggression, and peer rejection among a sample of predominately Latino adolescents. In particular, we evaluate an indirect effects model in which hyperactivity–impulsivity and inattention are directly and indirectly associated with peer rejection (i.e., through reactive or proactive aggression). Based on the literature reviewed above, reactive aggression was hypothesized to account for the link between hyperactivity–impulsivity and peer rejection.
Methods
Participants
Participants were 200 adolescents attending a charter high school in a large, Midwestern city. The mission of this school is to target Latino youth at risk for dropping out of school, so a large majority of the student population (approximately 95 %) self-identifies as Latino. School records show that 95 % of their students qualify for free or reduced lunch, indicating a low socioeconomic background for this sample, which is comparable to that of the surrounding public school district (89 % free/reduced lunch). Although cultural variables (e.g., acculturation, family background, language use) were not directly assessed in this investigation, other data collected from this population [51] indicate that a large majority of these students have spent most or all of their life living in the United States, and regularly communicate in both English and Spanish at home and with friends.
Teacher-reported data were collected for all 200 (100 %) students currently enrolled at the school. The final sample consisted of 104 males (52 %) and 96 females (48 %), including 58 (29 %) participants in 9th grade, 57 (29 %) in 10th grade, 43 (21 %) in 11th grade, and 42 (21 %) in 12th grade. Teachers were selected as informants based on previous research supporting the criterion-related validity and reliability of teacher’s ratings—and raising questions about the validity of self-reported ratings—of aggressive, disruptive, and social behaviors in the school context [52–54]. More specifically, second-period teachers were selected as these were all teachers of core academic subjects who had generally taught the same students, at the same time of day for the current school year, thus affording them over 6 months of interaction and observation with the students they were asked to rate.
Procedures
This study was approved by the researchers’ institutional review board. All data were collected within a two-week period during the middle of the spring semester. Ratings of students’ behavior were provided by their second-period teacher through the Qualtrics online survey platform. The measures included in the survey took approximately 10 min to complete for each student. Teachers provided written informed consent prior to beginning the survey and were compensated $10 for each completed survey.
Measures
All data were provided by teacher report, including students’ grade and gender. Likert-type measures (described below) were used for all other variables, with scores calculated as the average of ratings for all items within a scale. Consequently, results can be interpreted according to the numeric and descriptive properties of the original scales on which they were measured.
Inattentive and Hyperactive–Impulsive Symptoms
ADHD symptom dimensions were evaluated using the Disruptive Behavior Disorder Checklist [55], a measure assessing DSM symptoms of ADHD and Oppositional Defiant Disorder, rated on a four-point Likert scale from 1 (Not at all) to 4 (Very much). For the present analyses, only the 18 items pertaining to ADHD were used, including a nine-item subscale of inattentive symptoms (e.g., is often easily distracted, often has difficulty sustaining attention) and a nine-item subscale of hyperactive–impulsive symptoms (e.g., often fidgets with hands or squirms in seat, often interrupts or intrudes on others). This measure demonstrated good internal consistency for both the inattentive scale (α = .95) and the hyperactive–impulsive scale (α = .93).
Peer Rejection
Peer rejection was evaluated using four items from the social problems scale on the Teacher Report Form [10]. These items tap facets of social rejection relative to other members of a peer group (e.g., teasing, social preferences, and interpersonal problems). Teachers rated students on each item using a three-point Likert scale (1 = not true, 2 = somewhat or sometimes true, 3 = very or often true). This subscale demonstrated adequate internal consistency (α = .76). Previous research has used these items as a peer rejection subscale based on teacher reports and has been found to be related to other peer constructs [56, 57], providing evidence for construct validity.
Proactive and Reactive Aggression
Proactive and reactive aggression were assessed using a six-item rating scale [26]. Items were measured on a five-point scale from 1 (never) to 5 (almost always), with three-item subscales assessing proactive (e.g., threatens or bullies others to get his/her own way) and reactive (e.g., when teased or threatened, he/she gets angry easily and strikes back) aggression. Previous research has shown this measure to have strong reliability and validity [e.g., 58, 59], and internal consistency in the sample was good for both proactive (α = .75) and reactive (α = .89) aggression.
Analytic Plan
Proposed associations were evaluated through path models within a structural equation modeling framework using the MPlus 7 statistical package [60]. Less than 5 % of the data were missing. Full information maximum likelihood estimation (FIMLE) was utilized in all analyses, as this approach has been shown to produce unbiased estimates with greater efficiency compared to alternative methods [61]. In addition, robust estimation was utilized to account for non-normality [60]. Indirect effects were evaluated using the biased corrected bootstrap method, drawing 1,000 bootstrapped samples to approximate a normal distribution for indirect effect estimates. This method is more accurate and less biased than other methods for testing indirect effects [62]. Finally, we investigated potential differences between males and females by including gender as a moderator of all regression paths, using the product-of-coefficients strategy for assessing conditional indirect effects [63].
Results
Descriptive Statistics
Table 1 presents correlations, means, and standard deviations for all variables. As expected, positive correlations were found between symptoms of hyperactivity–impulsivity and inattention as well as between proactive and reactive aggression. Both ADHD symptom dimensions were positively correlated with both proactive and reactive aggression, although the magnitudes of these associations were higher for hyperactivity–impulsivity than for inattention. Peer rejection was weakly to moderately associate with both dimensions of ADHD symptoms, and moderately to strongly correlated with both aggression subtypes. Boys exhibited significantly (albeit slightly) higher levels of peer rejection, hyperactivity–impulsivity, and inattention compared to girls; however, no gender differences were found for either aggression subtype. Grade was uncorrelated with all variables except inattention, such that students in higher grades exhibited fewer attention problems.
Although this study involves dimensional symptom measures within a school population, additional analyses were conducted to provide an approximate estimate of proxy ADHD diagnoses within this sample. Teachers’ ratings of students’ hyperactive–impulsive and inattentive symptoms were dichotomized from four-point Likert scale ratings to binary symptom counts, similar to methods commonly used for ADHD diagnostic assessment rating scales [e.g., 64]. When these symptom scores were applied to DSM-5 diagnostic criteria for ADHD, 32 students (16.1 %) met symptom-count criteria for an ADHD diagnosis. Specifically, of these 32 students, 7 students met the symptom counts for combined presentation, 22 for predominately inattentive presentation, and 3 for predominately hyperactive–impulsive presentation. However, these estimates are based only on one rater assessing behavior in only one domain, without any consideration of functional impairment. Therefore, they should not be interpreted as clinical or diagnoses or epidemiological proxies for a diagnosis, as they are likely to overestimate the proportion of students in this sample who reach diagnostic thresholds. Nevertheless, these percentages suggest that ADHD rates among this sample are likely to be at least as high as national epidemiological studies [65, 66] which estimate the lifetime prevalence of ADHD is approximately 4–9 % among adolescents.
Path Models
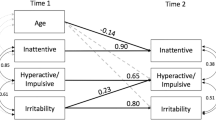
To evaluate the hypothesized mediation model (Fig. 1), peer rejection was regressed on hyperactivity–impulsivity, inattention, proactive and reactive aggression, and grade and gender; and proactive and reactive aggression were, in turn, regressed on all other exogenous variables. Because this model was fully saturated (zero degrees of freedom), providing the most stringent test of indirect effects, model fit statistics are not reported. As shown in Fig. 1, hyperactivity–impulsivity and grade were positively associated with reactive aggression, which was uniquely associated with peer rejection. Hyperactivity–impulsivity was also associated with proactive aggression. However, neither hyperactivity–impulsivity nor proactive aggression was directly associated with peer rejection. Inattention was not significantly associated with peer rejection or either type of aggression.

Estimated path model. Parameter estimates are from bootstrapped path analyses using FIMLE and robust estimation. Standardized path coefficient estimates are reported outside parentheses; unstandardized estimates are inside parentheses. Dashed lines represent estimated but nonsignificant paths. Covariances between all exogenous variables were estimated but are not depicted for clarity purposes. Gender: 1 = male, 2 = female. *p < .05, **p < .01, ***p < .001
Tests of indirect effects indicated that reactive aggression (the ‘ab’ path) accounted for the association between hyperactivity–impulsivity and peer rejection (B = .14, p < .01). That is, high levels of hyperactive–impulsive behavior were associated with high levels of reactive aggression, which in turn were uniquely associated with peer rejection. Applying MacKinnon and Dwyer’s [67] formula, this specific indirect path (hyperactivity–impulsivity → reactive aggression → peer rejection) accounted for 66.7 % of the total variance in the pathway between hyperactivity–impulsivity and peer rejection.
To examine the possibility of gender differences, the hypothesized path model (Fig. 1) was modified to include gender as a moderator of all indirect and direct paths (i.e., all regression paths linking ADHD symptom dimensions, aggression subtypes, and peer rejection). No significant moderation effects were found (ps = .078–.824), indicating that the indirect effects of reactive aggression in the relationship between ADHD symptoms and peer rejection are consistent across males and females in this sample.
Discussion
The relationship between ADHD and social impairment is well established, but less is known about how different dimensions of ADHD symptoms and functions of aggression may account for that association. The present study examined the role of proactive and reactive aggression in the association between ADHD symptom dimensions (inattention, hyperactivity–impulsivity) and peer rejection among a sample of predominately Latino high school students. Results indicated that reactive, but not proactive, aggression accounted for the association between hyperactivity–impulsivity and peer rejection. In addition, hyperactivity–impulsivity predicted proactive aggression; but proactive aggression did not, in turn, uniquely predict peer rejection. Interestingly, inattention did not have any unique contributions to aggression or peer rejection, and the results did not differ across genders.
These findings are consistent with previous research demonstrating links between ADHD and aggression [e.g., 4, 33], aggression and peer rejection [e.g., 22], and ADHD and peer rejection [e.g., 6, 7]. The present study advances the literature by providing clarity as to what aspects of ADHD and aggressive behavior are most detrimental to adolescents’ social functioning. That is, these findings indicate that hyperactive–impulsive symptoms may be more strongly related to peer rejection than inattentive symptoms, and reactive aggression appears to be a key factor accounting for this association. Given that hyperactivity and reactive aggression share a common element of impulsivity, it is likely that reactively aggressive behaviors are one avenue through which hyperactivity–impulsivity is manifested in the social domain, and that it is this particular facet that is associated with peer rejection. Such an interpretation is supported by previous research showing that reactive, not proactive, aggression remains uniquely associated with overall psychosocial impairment even after controlling for symptom severity in both dimensions of ADHD, as well as oppositional behaviors and conduct problems [59]. Phrased in more person-centered terms, there may be a subgroup of hyperactive–impulsive youth who also engage in reactively aggressive behavior, which places them at greater risk for peer rejection.
As hypothesized, proactive aggression (in contrast to reactive aggression) was not uniquely associated with peer rejection in adolescents. This result is consistent with previous research showing nonsignificant and mixed results in the relation between proactive aggression and impaired social functioning, as compared to much stronger and more robust associations for reactive aggression [11]. This differential pattern of associations may be partially explained by evidence showing that reactive, not proactive, aggression is associated with executive function problems in terms of behavioral regulation and metacognition [68]. These executive function deficits are also central to ADHD symptoms [2] and may therefore help explain why reactive aggression accounts for the link between hyperactivity–impulsivity and peer rejection. Conversely, this evidence suggests that proactively aggressive youth are relatively typical in terms of their executive function profile and self-regulation capacities [68], which would provide them with a better foundation for social skill development, friendship formation, and navigating social situations. It may be the case that, for hyperactive and impulsive youth, these unique features of proactive aggression may help mitigate risk for peer rejection, whereas the opposite appears to be true for reactive aggression. Further research is needed to examine this possibility.
In contrast to previous research documenting the association between inattention and impaired social functioning [e.g., 23], the present study found no direct or indirect effects for attention problems contributing to peer rejection. The nonsignificance of these paths may be related to grade levels of the population. The link between inattention and social impairment is commonly found in childhood and early adolescence [4, 5]; less is known about mid to late adolescence. It may be the case that attention problems are more socially impairing during childhood, when social-cognitive and communication skills are being developed, than during adolescence, by which point there has been more opportunity to develop compensatory social skills.
With respect to the possibility of gender differences, the present results were not particularly surprising. Consistent with ADHD prevalence estimates [65, 66] and normative data on dimensional symptom severity [10, 64], boys showed higher overall levels of hyperactivity–impulsivity and inattention. However, gender was not uniquely linked to peer rejection or either aggression subtype in the path analyses; nor were any of the in the model paths moderated by gender. These findings provide support the notion that ADHD symptoms are impairing to a similar degree for both boys and girls [3], but this impairment is not necessarily due to qualitative differences in symptoms or mechanisms as some studies have suggested [23, 68]. The absence of gender differences related to the function of aggression is also consistent with prior research suggesting that boys and girls are more different in the forms than the functions of aggression [25, 40, 69, 70]. Indeed, in a model similar to that of the present study, Tseng et al. [23] found that physical, but not relational, aggression mediated the link between hyperactivity and peer functioning in girls, but not in boys. Considering these findings along with those of the present study, reactive-physical aggression may be the specific subtype most directly linked to peer rejection. Further research is needed to elucidate the roles of gender and form/function of aggression in terms of accounting for the link between ADHD symptoms and peer rejection.
A final noteworthy contribution of this study is that it offers one of the first examinations of teacher-reported ratings of functions aggression and symptom dimensions of ADHD in a sample of Latino adolescents. Descriptive results regarding the frequency distribution of hyperactive–impulsive behaviors and attention problems were not markedly dissimilar from the results of national epidemiological studies [65, 66]; and while such normative data do not exist for aggression subtypes, the patterns of proactive and reactive aggression observed in this sample are more similar to community samples than clinical samples of adolescents [70]. It is not clear to what extent these results may be influenced by specific cultural factors. However, it is notable that these findings appear to be at odds with prior research showing that ADHD symptoms are significantly less likely to be identified in Latino youth compared to those of other ethnic backgrounds [41, 42]. If this is the case, it suggests that teachers could potentially play a key role in identifying externalizing behavior problems in Latino youth, which could in turn help facilitate referrals and access to culturally sensitive intervention services for adolescents and their families.
Limitations and Future Directions
Several limitations should be considered in the interpretation of these findings and in consideration of directions for future research. First, all variables were assessed via teacher report, which may result in mono-informant bias. Future research should strive to incorporate data from multiple informants, such as parents, teachers, self-report, and peer nominations, in order to provide a more thorough understanding across different settings and perspectives. Of course, decisions about converging sources of data should be made with careful consideration of the variables and research objectives. For example, including peer nominations and self-reported data, in addition to teacher-reported data, would likely bolster precision and validity in the measurement of peer rejection. However, compared to those informants, it seems unlikely that parent-reported data would offer incremental utility for the measurement of peer rejection because parents’ impressions of their adolescents’ peer relations are likely be based less on direct observation and more on second-hand information. With respect to the present study, teachers seemed most able to offer accurate ratings of the study variables within a consistent social/academic context [52–54], and any mono-informant bias would be in the direction of nonsignificance or Type II errors. Thus, the significant results can be interpreted as real associations based on teachers’ perspectives of adolescents’ behavior in the school context; however, the mono-informant limitations indicate a need for further research to provide a full picture, particularly the nonsignificant results.
A second limitation is that the sample was recruited from an urban charter school and was predominantly comprised of low-income Latino youth. It is not clear how well the present findings will generalize to other populations. Future research should examine these relations among other community and clinical samples, including youth from different ethnic backgrounds, in order to better understand these relations across different populations. In addition, it is important to note that these cross-sectional findings do not inform the causal nature of the relations among study variables. Although previous research provides some longitudinal support for directionality hypothesized in this model [23, 34, 38, 39], future longitudinal investigations are needed to truly assess mediation associations among ADHD symptoms, proactive/reactive aggression, and peer rejection. Considering this study’s focus on hyperactivity–impulsivity, further research is needed to better understand the mechanisms involved in the link between inattention and peer rejection. In particular, it has been hypothesized [4, 5] that attention problems throughout childhood may contribute to social-cognitive deficits (e.g., social knowledge/cognition, problem-solving, prosocial behavior), which in turn might increase risk for peer rejection [17–20]. Multi-informant/-method designs would be especially helpful for studies testing hypotheses about mechanisms of inattention, considering that self-informant methods are recommended for measuring social-cognitive variables [18].
These findings carry important implications for assessment and intervention with aggressive and hyperactive youth. Among adolescents with hyperactive and impulsive behaviors, those who are exhibit reactively aggressive behaviors may be at a greater risk for peer rejection. Thus, interventions for ADHD should focus particularly on assessing, preventing, and reducing aggressive behaviors. By targeting reactive aggression, treatment for adolescents with ADHD may ultimately lead to better social functioning. A related implication is that interventions for aggressive youth may also consider screening for ADHD symptomatology. From either angle, clinicians and interventionists should consider that reactive aggression is both associated with ADHD symptoms and appears to account for at least some of the social impairment linked to hyperactivity and impulsivity. By maintaining this perspective, interventions addressing hyperactivity–impulsivity or aggression may facilitate a more accurate and complete understanding of the problem behaviors, as well as a more effective approach to assessment and intervention.
Summary
The present study advanced the literature by investigating the role of reactive aggression in the link between hyperactive–impulsive behaviors and peer rejection in adolescents. An indirect effects model was evaluated using teacher ratings of proactive and reactive aggression, ADHD symptom dimensions, and peer rejection in a school-wide sample of predominately Latino high school students. Controlling for grade and gender, results indicated that symptoms of hyperactivity–impulsivity were uniquely associated with reactive aggression, which, in turn, was associated with peer rejection. Hyperactivity–impulsivity was also linked to proactive aggression, but proactive aggression was not associated with peer rejection. Inattention was not associated with peer rejection or either type of aggressive behavior. These results were consistent for both males and females. Findings suggest that reactive aggression may help account for the link between hyperactive–impulsive behaviors and peer rejection. Assessment and intervention efforts should more carefully consider the link between reactive aggression and hyperactive–impulsive behaviors. Future research is needed to examine these associations longitudinally and across different perspectives and populations.
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, 4th edn (text revision). American Psychiatric Association, Washington, DC
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association, Arlington
Hoza B (2007) Peer functioning in children with ADHD. J Pediatr Psychol 32:655–663
Nijmeijer JS, Minderaa RB, Buitelaar JK, Mulligan A, Hartman CA, Hoekstra PJ (2008) Attention-deficit/hyperactivity disorder and social dysfunctioning. Clin Psychol Rev 28:692–708
Wheeler J, Carlson CL (1994) The social functioning of children with ADD with hyperactivity and ADD without hyperactivity: a comparison of their peer relations and social deficits. J Emot Behav Disord 2:2–12
Hoza B, Mrug S, Gerdes A, Hinshaw SP, Bukowski WM, Gold JA et al (2005) What aspects of peer relationships are impaired in children with attention-deficit/hyperactivity disorder? J Consult Clin Psychol 73:411–423
Mrug S, Hoza B, Gerdes AC, Hinshaw S, Arnold LE, Hechtman L, Pelham WE (2009) Discriminating between children with ADHD and classmates using peer variables. J Atten Disord 12:372–380
Mrug S, Molina BSG, Hoza B, Gerdes AC, Hinshaw SP, Hechtman L, Arnold LE (2012) Peer rejection and friendships in children with attention-deficit/hyperactivity disorder: contributions to long-term outcomes. J Abnorm Child Psychol 40:1013–1026
Murray-Close D, Hoza B, Hinshaw SP, Arnold LE, Swanson J, Jensen PS et al (2010) Developmental processes in peer problems of children with attention-deficit/hyperactivity disorder in the Multimodal Treatment Study of Children with ADHD: developmental cascades and vicious cycles. Dev Psychopathol 22:785–802
Achenbach TM, Rescorla LA (2001) Manual for the ASEBA school-age forms profiles. University of Vermont, Research Center for Children, Youth, Families, Burlington
Card NA, Little TD (2006) Proactive and reactive aggression in childhood and adolescence: a meta-analysis of differential relations with psychosocial adjustment. Int J Behav Dev 30:466–480
Pope AW, Bierman KL, Mumma GH (1991) Aggression, hyperactivity, and inattention-immaturity: behavior dimensions associated with peer rejection in elementary school boys. Dev Psychol 27:603–671
Cicchetti D, Rogosch FA (2002) A developmental psychopathology perspective on adolescence. J Consult Clin Psychol 70:6–20
Frick PJ, Nigg JT (2012) Current issues in the diagnosis of attention deficit hyperactivity disorder, oppositional defiant disorder, and conduct disorder. Annu Rev Clin Psychol 8:77–107
Bierman KL, Smoot DL, Aumiller K (1993) Characteristics of aggressive-rejected, aggressive (nonrejected), and rejected (nonaggressive) boys. Child Dev 64:139–151
Maedgen JW, Carlson CL (2000) Social functioning and emotional regulation in the attention deficit hyperactivity disorder subtypes. J Clin Child Psychol 29:30–42
Lorch EP, Eastham D, Milich R, Lemberger RP, Sanchez RP, Welsh R (2004) Difficulties in comprehending causal relations among children with ADHD: the role of cognitive engagement. J Abnorm Psychol 113:56–63
Crick NR, Dodge KA (1994) A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychol Bull 115:74–101
Zentall SS, Javorsky J, Cassady JC (2001) Social comprehension of children with hyperactivity. J Atten Disord 5:11–24
Sibley MH, Evans SW, Serpell ZN (2010) Social cognition and interpersonal impairment in young adolescents with ADHD. J Psychopathol Behav Assess 32:193–202
Erhardt D, Hinshaw SP (1994) Initial sociometric impressions of attention-deficit hyperactivity disorder and comparison boys: predictions from social behaviors and from nonbehavioral variables. J Consult Clin Psychol 62:833–842
Coie JD, Dodge KA, Kupersmidt JB (1990) Peer group behavior and social status. In: Asher S, Coie J (eds) Peer rejection in childhood. Cambridge University Press, New York, pp 17–59
Tseng WL, Kawabata Y, Gau SSF, Banny AM, Lingras KA, Crick NR (2012) Relations of inattention and hyperactivity–impulsivity to preadolescent peer functioning: the mediating roles of aggressive and prosocial behaviors. J Clin Child Adolesc Psychol 41:275–287
Coie D, Dodge KA, Terry R, Wright V (1991) The role of aggression in peer relations: an analysis of aggression episodes in boys’ play groups. Child Dev 62:812–826
Little TD, Henrich CC, Jones SM, Hawley PH (2003) Disentangling the “whys” from the “whats” of aggressive behaviour. Int J Behav Dev 27:122–133
Dodge KA, Coie JD (1987) Social information-processing factors in reactive and proactive aggression in children’s peer groups. J Pers Soc Psychol 53:1146–1158
Berkowitz L (1978) Whatever happened to the frustration-aggression hypothesis? Am Behav Sci 32:691–708
Berkowitz L (1989) Frustration-aggression hypothesis: examination and reformulation. Psychol Bull 106:59–73
Vitaro F, Brendgen M, Barker ED (2006) Subtypes of aggressive behavior: a developmental perspective. Int J Behav Dev 30:12–19
Bandura A (1973) Aggression: a social learning analysis. Prentice-Hall, Englewood Cliffs
Fite PJ, Colder CR, Pelham WE (2010) A factor-analytic approach to distinguish pure and co-occurring dimensions of proactive and reactive aggression. J Clin Child Adolesc Psychol 35:578–582
Raine A, Dodge K, Loeber R, Gatze-Kopp L, Lynam D, Reynolds C, Stouthamer-Loeber M, Jianghong L (2006) The Reactive–Proactive Aggression Questionnaire: differential correlates of reactive and proactive aggression in adolescent boys. Aggress Behav 32:159–171
Connor DF, Chartier KG, Preen EC, Kaplan RF (2010) Impulsive aggression in attention-deficit/hyperactivity disorder: symptom severity, co-morbidity, and attention-deficit/hyperactivity disorder subtype. J Child Adolesc Psychopharmacol 20:119–126
Taylor E, Chadwick O, Heptinstall E, Danckaerts M (1996) Hyperactivity and conduct problems as risk factors for adolescent development. J Am Acad Child Adolesc Psychiatry 35:1213–1226
Boivin M, Dodge KA, Coie JD (1995) Individual-group behavioral similarity and peer status in experimental play groups of boys: the social misfit revisited. J Pers Soc Psychol 69:269–279
Morrow MT, Hubbard JA, McAuliffe MD, Rubin RM, Dearing KF (2006) Childhood aggression, depressive symptoms, and peer rejection: the mediational model revisited. Int J Behav Dev 30:240–248
Poulin F, Boivin M (1999) Proactive and reactive aggression and boys’ friendship quality in mainstream classrooms. Journal of Emotional and Behavioral Disorders 7:168–177
Coie JD, Kupersmidt JB (1983) A behavioral analysis of emerging social status in boys’ groups. Child Dev 54:1400–1416
Dodge KA (1983) Behavioral antecedents of peer status. Child Dev 54:1386–1399
Elkins IJ, Malone S, Keyes M, Iacono WG, McGue M (2011) The impact of attention-deficit/hyperactivity disorder on preadolescent adjustment may be greater for girls than for boys. J Clin Child Adolesc Psychol 40:532–545
Cuffe SP, Moore CG, McKeown RE (2005) Prevalence and correlates of ADHD symptoms in the National Health Interview Survey. J Atten Disord 9:392–401
de Ramirez RD, Shapiro ES (1998) Teacher ratings of attention deficit hyperactivity disorder symptoms in Hispanic children. J Psychopathol Behav Assess 20:275–293
Bauermeister JJ, Canino G, Bravo M, Ramírez R, Jensen PS, Chavez L et al (2003) Stimulant and psychosocial treatment of ADHD in Latino/Hispanic children. J Am Acad Child Adolesc Psychiatry 42:851–855
Stevens J, Harman JS, Kelleher KJ (2004) Ethnic and regional differences in primary care visits for attention-deficit hyperactivity disorder. J Dev Behav Pediatr 25:318–325
Hervey-Jumper H, Douyon K, Falcone T, Franco KN (2008) Identifying, evaluating, diagnosing, and treating ADHD in minority youth. J Atten Disorders 11:522–528. doi:10.1177/1087054707311054
Schmitz MF, Velez M (2003) Latino cultural differences in maternal assessments of attention deficit/hyperactivity symptoms in children. Hisp J Behav Sci 25:110–122. doi:10.1177/0739986303251700
Bauermeister JJ, Matos M, Reina G, Salas CC, Martínez JV, Barkley RA (2005) Comparison of the DSM-IV combined and inattentive types of ADHD in a school-based sample of Latino/Hispanic children. J Child Psychol Psychiatry 46:166–179
Mercado-Crespo M, Mbah AK (2013) Race and ethnicity, substance use, and physical aggression among U.S. high school students. J Interpers Violence 28:1367–1384
Vazsonyi AT, Keiley MK (2007) Normative developmental trajectories of aggressive behaviors in African American, American Indian, Asian American, Caucasian, and Hispanic children and early adolescents. J Abnorm Child Psychol 35:1047–1062
Smokowski PR, Bacallao ML (2006) Acculturation and aggression in Latino adolescents: a structural model focusing on cultural risk factors and assets. J Abnorm Child Psychol 34:657–673
Rubens SL, Fite PJ, Gabrielli J, Evans SC, Hendrickson ML, Pederson CA (2013) Examining relations between negative life events, time spent in the United States, language use, and mental health outcomes in Latino adolescents. Child Youth Care Forum 42:389–402
Henry DB (2006) Associations between peer nominations, teacher ratings, self-reports, and observations of malicious and disruptive behavior. Assessment 13:241–252
Konold TR, Walthall JC, Pianta RC (2004) The behavior of child behavior ratings: measurement structure of the child behavior checklist across time, informants, and child gender. Behavioral Disord 29:372–383
Molina BSG, Smith BH, Pelham WE (2001) Factor structure and criterion validity of secondary school teacher ratings of ADHD and ODD. J Abnorm Child Psychol 29:71–82
Pelham WE, Gnagy EM, Greenslade KE, Milich R (1992) Teacher ratings of DSM-III—R symptoms for the disruptive behavior disorders. J Am Acad Child Adolesc Psychiatry 31:210–218
Fite PJ, Wimsatt AR, Vitulano ML, Rathert JL, Schwartz S (2012) Examination of peer rejection and depressive symptoms as mediators of the link between rule-breaking behavior and poor academic performance. J Psychopathol Behav Assess 34:164–171
Fite PJ, Wynn P, Pardini D (2009) Explaining discrepancies in arrest rates between black and white male juveniles. J Consult Clin Psychol 77:916–927
Dodge KA, Lochman JE, Harnish JD, Bates JE, Pettit GS (1997) Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. J Abnorm Psychol 106:37–51
Waschbusch DA, Willoughby MT, Pelham WE (1998) Criterion validity and the utility of reactive and proactive aggression: comparisons to attention deficit hyperactivity disorder, oppositional defiant disorder, and other measures of functioning. J Clin Child Psychol 27:396–405
Muthén LK, Muthén BO (2012) Mplus user’s guide, 7th edn. Muthén & Muthén, Los Angeles
Enders CK, Bandalos DL (2001) The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Struct Equ Model 8:430–457
MacKinnon DP, Lockwood CM, Williams J (2004) Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivar Behav Res 39:99–128
Preacher KJ, Rucker DD, Hayes AF (2007) Addressing moderated mediation hypotheses: theories, methods, and prescriptions. Multivar Behav Res 42:185–227
Barkley RA (2005) Attention-deficit hyperactivity disorder: a handbook for diagnosis and treatment, 3rd edn. Guilford, New York
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A (1993) Prevalence and development of psychiatric disorders in childhood and adolescence. JAMA 60:837–844
Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L et al (2010) Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 49:980–989
MacKinnon DP, Dwyer JH (1993) Estimating mediated effects in prevention studies. Eval Rev 17:141–158
White BA, Jarrett MA, Ollendick TH (2013) Self-regulation deficits explain the link between reactive aggression and internalizing and externalizing behavior problems in children. J Psychopathol Behav Assess 35:1–9
Bowie BH (2007) Relational aggression, gender, and the developmental process. J Child Adolesc Psychiatr Nurs 20:107–115
Marsee MA, Frick PJ, Barry CT, Kimonis ER, Centifanti LCM, Aucoin KJ (2014) Profiles of the forms and functions of self-reported aggression in three adolescent samples. Dev Psychopathol 26:705–720
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Evans, S.C., Fite, P.J., Hendrickson, M.L. et al. The Role of Reactive Aggression in the Link Between Hyperactive–Impulsive Behaviors and Peer Rejection in Adolescents. Child Psychiatry Hum Dev 46, 903–912 (2015). https://doi.org/10.1007/s10578-014-0530-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-014-0530-y