
Abstract
We sought to identify needs for behavioral health care in a large, urban pediatric primary care (PPC) clinic serving a population covered by Medicaid. Specifically, children (N = 197; 120 girls; 91 % African American) ages 8–17 years and their caregivers completed measures of internalizing and externalizing symptoms (RCADS, RCADS-P, MASC, and SDQ). Clinical elevations on all but one domain of the SDQ were significantly higher than expected. However, self-reported anxiety and depression symptoms were consistent with expectations. These findings suggest urban, low-income, primarily African American youth presenting at a PPC clinic demonstrate significant levels of behavioral and emotional symptoms. Implications of the findings include the need to ask both parents and children about child behavioral health problems and the possible influence of screening tool selection on detection.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Untreated childhood behavioral health problems can lead to a number of problematic sequelae such as future behavioral health [1], sexual risk-taking behavior [2], substance abuse [3], suicide [4], and criminal behavior [5]. Despite documented detrimental effects of untreated behavioral health problems, most children do not receive treatment. In a nationally representative sample of children aged 6–17 in the US, researchers estimated between 15 and 21 % of youth had behavioral health problems, and among those, 75–79 % of those had not received behavioral health services [6]. Further, data suggest that ethnic and racial minority children are more likely to receive fewer and inferior behavioral health care than Caucasian children [7] and are disproportionately affected by socioeconomic disadvantage and other risk factors for behavioral health problems, including poverty [8] and exposure to violence [9, 10].
Poverty in particular has been identified as a condition that fosters the emergence of proximal variables more closely linked with psychopathology, including economic hardship, disrupted family processes, and exposure to violence [11]. Children living in low income households are 5–10 times more likely to suffer from behavioral health problems and be classified as having serious emotional disturbances compared to the general population [12], though they are most likely to have their behavioral health needs go unmet [6]. Taken together, these data make clear that identification of behavioral health problems in youth, particularly for low-income, ethnic minority children, remains a critical area for future public health efforts.
Pediatric primary care (PPC) clinics have been identified as important settings for the identification and treatment of children with behavioral health disorders [13]. Considerable research has demonstrated the prevalence of behavioral health problems among children presenting at PPC clinics for care [14–16]. For example, a 3-year longitudinal study of a representative population sample of children aged 9–13 presenting for PPC services found that 36.7 % of children met criteria for at least one diagnosis [1–7].
When considering PPC clinics as a promising potential point of access to screen and treat traditionally underserved children, several factors must be taken into consideration. First, careful thought must be given to the selection of appropriate screening measures. Researchers have established several criteria identifying good mental health screening tools, including a robust psychometric profile, brevity, ease of completion, basis in DSM criteria, and utility in the absence of trained mental health professionals [18]. Second, these tools must be applicable to the behavioral health problems faced by minority children receiving PPC services; cultural variation in understanding behavioral health problems poses important challenges for screening for psychopathology [23]. This has not been well investigated; the majority of existing literature involves mainly Caucasian samples [14, 17, 19, 20]. This is particularly important given research indicating that African Americans are more likely to interpret psychological symptoms as medical and initiate medical treatment [21, 22].
Attempts have been made to ensure reliable estimates of underrepresented populations. For example, Costello and colleagues [17] oversampled Native American children, and Polaha et al. [16] reported behavioral health symptom data on a medically underserved population. In perhaps the largest and most diverse study to date, Wren et al. [23] provided screening data on a sample of more than 500 children in northern California, with more than 50 % of the sample being non-Caucasian. This small body of research makes clear both the importance of PPC as a potential setting for behavioral health services as well as the importance of understanding the needs of demographic (e.g., race/ethnicity, family income) groups underrepresented in past studies.
The present study seeks to add to the literature on screening diverse youth in PPC. To our knowledge, our study is the first to look specifically at a low-income African American population in a PPC setting. As noted, the present study is part of a larger project designed to identify the needs of an urban PPC clinic serving a population of largely African-American families on Medicaid. We sought to identify the level and type of behavioral health problems present in the patients at the clinic. The second part of the project involved interviewing stakeholders about barriers to implementing an integrated care model in the setting. The present study is the first to examine the prevalence of emotional and behavior problems using both self- and parent-report measures among children presenting in a PPC setting serving a primarily urban, low-income, African American youth population.
Specifically, our goal for this project was to provide descriptive information about the level and type of behavioral health symptoms among the youth treated at the clinic. We also sought to compare the data from our sample to the normative data for the measures we gathered to determine whether the level of behavioral health symptoms exceeded expectations. Given the risk factors present in our sample, we hypothesized that the level of clinically significant behavioral health problems reported on self- and parent-report measures would meet or exceed clinical cutoff for that measure, using an analytic approach akin to benchmarking [24].
Method
Participants
Participants were drawn from a larger sample of 229 children aged 8–17 and their parents or legal guardians recruited in the waiting room of a large PPC clinic associated with an academic medical center located in the mid-Atlantic region of the United States. The clinic serves a primarily minority population, with 73 % of patients identifying as African American, 18 % Hispanic, and 6 % White, and over 90 % of patients receiving publically funded health care. Data from 32 participants were excluded because: a) the child did not meet the required grade range (i.e., 3rd–12th) or b) missing or incomplete questionnaires. Thus, the total number of participants in the current study was 197, ranging in age from 8 to 17 (M = 12.36; SD = 2.55).
Procedure
Parent–child dyads were recruited from the waiting room of a PPC clinic. If the family agreed to participate, a trained research assistant obtained informed consent and assent and provided the guardian and child with questionnaires to be completed before, during, or immediately after their clinic visit. Each family received a $20 retail gift card for participation in the study. The governing Institutional Review Board approved the study.
Measures
Revised Child Anxiety and Depression Scale
The child and parent versions of the RCADS [25, 26] are parallel 47-item self- and parent-report measures that assess symptoms of several DSM-IV anxiety and depressive disorders (i.e., separation anxiety disorder, social phobia, obsessive–compulsive disorder, panic disorder, generalized anxiety disorder, and major depressive disorder). Children or parents indicate whether items such as “I worry about things” or “My child feels sad or empty” happen Never, Sometimes, Often, or Always. Both versions of the measure allow comparisons to a grade normed reference group and have strong psychometric profiles including good internal consistency, convergent and divergent validity, and the ability to discriminate among the targeted disorders. Research with low-income African American youth provides strong support for measurement equivalence [27]. In past studies, Cronbach α coefficients for the six disorder-specific subscales ranged from .71 to .85 for the RCADS [25] and from .81 to .88 for the RCADS-P [26]. Internal consistency coefficients for this study were comparable, ranging from .65 to .82 for the RCADS and from .70 to .82 for the RCADS-P.
Multidimensional Anxiety Scale for Children
The MASC [28] is a 39-item four-point Likert-type child-report measure of anxiety symptoms across several dimensions of anxiety (i.e., physical symptoms, harm avoidance, social anxiety, and separation anxiety). Past studies have suggested the measure is a stable and reliable measure of anxiety in young people with test–retest reliability statistics in the satisfactory to excellent range and strong internal consistency [28]. Further, research supports the use of this measure for African American youth [29]. Cronbach α coefficients for the four subscales ranged from .74 to .85 [28]. Coefficient alphas for the current study ranged from .69 to .86.
Strengths and Difficulties Questionnaire
The SDQ [30] is a 25-item instrument that screens for behavioral health problems across five domains: Conduct Problems, Emotional Symptoms, Hyperactivity-Inattention, Peer Problems, and Prosocial Behavior. The Total Difficulties scale is a summation of the clinical scales and a measure of the severity of the child’s difficulties. The Impairment subscale measures the child’s distress and functional impairment and is calculated independently of the clinical scales. The SDQ has been validated among diverse populations in the United States, Europe, Asia, and Australia, has demonstrated a strong psychometric profile, and provides US-normed clinical cutoff scores for each of the five domains as well as the Total Difficulties and Impairment subscales [31]. The Conduct Problems, Emotional Symptoms, Hyperactivity-Inattention, and Prosocial Behavior subscales, as well as the Total Problems and Impairment scales were retained for analyses. Cronbach α coefficients were as follows: the total difficulties and impairment were .83 and .80, respectively, and the subscales ranged from .63 to .77 [31]. The measure provides numerical scores for each domain that are classified as low, medium, or high difficulty based on age and gender norms; high scores correspond to scores in the 90th percentile or above. Only the parent-report version was used in this study because the lower age limit for the youth version of the SDQ is 11, whereas our sample included a large number of children ages 8–10. Coefficient alphas were comparable to the US study; the four subscales ranged from .69 to .72.
Analytic Plan
Analyses were conducted using Statistical Package for the Social Sciences (SPSS) version 18.0. Descriptive analyses (e.g. means, standard deviations, etc.) were conducted to examine data and identify mean scores for the sample on the clinical measures. Chi square analyses were used to compare observed clinical symptom scores to expected frequencies based on measure-specific cut-points. This method utilizes and expands upon benchmarking methodology used in dissemination and implementation research to compare treatment outcomes obtained in community clinic settings to those obtained research benchmarking clinical trials [24, 32]. Expected clinical frequencies of 6.68 % were used for the RCADS, RCADS-P and MASC to correspond to the clinical T-score of 65 [25, 26, 28]. For the SDQ, the observed frequencies were compared to 10 % to correspond with the “high” difficulties band [31].
Results
Overview
Data preparation and preliminary analyses included handling of missing data. The primary aim of this study was to evaluate the prevalence of emotional and behavior problems in an urban PPC setting. Toward that end, we employed descriptive analyses to examine the sample, independent sample t tests to compare means across gender and age groups, Chi square analyses to compare observed frequencies of clinical scores in this sample to expected frequencies based on normative data, and Chi square analyses to compare observed frequencies of clinical scores across gender and age groups.
Missing Data
The current study excluded data from 32 dyads from the original sample of 229 due to 1) the child being in 1st or 2nd grade (n = 16), 2) missing or incomplete questionnaires equal to missing items totaling >15 % of any measure (n = 13) or missing items totaling >20 % on a single subscale of the RCADS or RCADS-P (n = 3). The remaining sample contained 197 dyads. The cutoff criteria were established following the missing-item conventions of the scale developers [25, 26, 28]. We conducted independent sample t tests and Chi square analyses to examine differences between participants with complete versus missing data on age, gender, and ethnicity variables and found no significant differences between the groups on these demographic variables.
Further, a large percentage of participants did not report certain demographic data (i.e., martial status, income, insurance status). Independent sample t tests and Chi square analyses were conducted using modified Bonferroni correction to protect against type 1 error. Participants with missing demographic data did not differ from participants without on proportion of other missing data or on scores on clinical measures with one exception. Families with missing income data had significantly lower scores on the SDQ Impact scale (M = 0.45, SE = 0.17), t(163.1) = 3.98, p < .001 than did families without income data missing (M = 1.50, SE = 0.20).
Missing values for the self-report measures were imputed following a mean-item substitution method following guidelines for the RCADS [25, 26] and the MASC [28]. Missing values were not imputed for the SDQ, which was scored using the developer’s online scoring program. Subscales with more than one item missing were excluded from analyses. Subscales with one item missing were corrected by substituting the mean of the remaining subscale items for the missing item score. Missing data information for subscale and demographic items is presented in Table 1.
Sample Characteristics
The sample included 197 youth (M = 12.4 years, SD = 2.6 years; 60.9 % girls) and their parents or legal guardian. Children between the ages of 8 and 12 years comprised 54.8 % of the sample; 45.2 % were between the ages of 13 and 17 years. Seventy-six percent of parents reported their annual income, and of these participants, 43.3 % reported income below $18,310, the federal poverty guideline for families of three [33], and 82.7 % of families reported annual income equal to or less than two times the federal poverty guideline. Fewer than half (46.2 %) reported any information about their child’s insurance coverage. Of those who disclosed insurance information, 95.6 % reported their child had health insurance and 70.3 % reported their child was covered by Medicaid. Among caregivers, 44.7 % provided additional information about themselves. Demographic and caregiver information is presented in Tables 2 and 3, respectively. Information about families who declined to participate or provide income or insurance information was not available; however, clinic records indicated that approximately 91 % of the clinic’s patients receive publically funded health care, and the clinic serves approximately 940 children aged 8–17 annually.
Level of Behavioral Health Symptoms
Across the sample, 75.6 % of participants had at least one clinically elevated score on any measure. Thirty-nine percent exceeded the clinical cutoff on at least one subscale of a youth-report measure, and 62.4 % exceeded the clinical cutoff score on at least one subscale of a parent-report measure. Independent sample t tests were used to compare subscale score means between younger and older children (i.e., age 8–12, age 13–17) and gender. Due to the number of statistical tests, we adjusted the alpha level using a modified Bonferroni correction described by Holm [34] and recommended by Jaccard and Guilamo-Ramos [35]. We employed a per-family error rate of .05 for comparisons across each of the self-report measures (RCADS, RCADS-P, SDQ, MASC), though the alpha level for each test depends on the number of tests in the family. As such, the significance level used for each significant test reported is clearly noted.
Means and standard deviations of parent- and child-report measures are presented in Tables 4 and 5, respectively. In addition to examining the group as a whole, we conducted exploratory analyses to compare mean scores and frequency of clinical elevations across gender and age groups. Across gender, only one statistically significant difference emerged. Boys had significantly higher mean scores (M = 4.73, SD = 2.67) on the SDQ Hyperactivity and Attentional Difficulties scale than did girls (M = 3.29, SD = 2.29; t (195) = −4.028, p < .001, η 2 = .077; critical p = .007). Across age groups, only one statistically significant difference emerged. Younger children had statistically significantly lower means (M = 45.74, SD = 8.70) on the RCADS-P Separation scale than older children (M = 49.75, SD = 11.13; t (164.55) = −2.774, p = .006, η 2 = .019; critical p = .006). However, no statistically significant differences emerged between age- or gender-stratified groups in frequency of clinical scores.
Rates of clinically significant scores on the two parent-report measures, the RCADS-P and the SDQ, are presented in Table 6. For the overall sample, Chi square analyses were used to compare frequency of clinical reports to expected frequencies based on clinical cut-offs established by the measure developers (i.e., 6.68 % for RCADS-P, 10 % for SDQ). Chi square analyses were also used to compare frequencies of clinical elevations between age groups and gender. A total of 6.1 % of caregivers reported clinically elevated scores on the RCADS-P Total Anxiety and Depression subscale, and rates of clinically elevated subscale scores ranged from 4.1 % on the Generalized Anxiety subscale to 11.2 % on the Depression subscale. For the RCADS-P, neither overall rates of clinically elevated scores nor rates of scores among age and gender groups were significantly different than the expected rate.
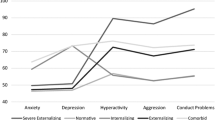
This finding stands in contrast to parent-reported youth distress on the SDQ wherein rates of clinically elevated scores were statistically significantly higher than the 10 % expected for five out of six scales of the SDQ. Rates of clinical elevations ranged from 18.8 % (χ2(1) = 16.88, p ≤ .001, critical p = .025) on the Total Difficulties scale to 26.9 % (χ2(1) = 63.24, p ≤ .001, critical p = .008) on the Impact scale. Although boys and girls and younger and older youth differed in their rates of clinically elevated scores, these differences were not statistically significant.
Frequencies of clinically elevated scores on the two youth self-report measures, the RCADS and MASC, are reported in Table 7. As with parent-report measures, Chi square analyses were used to compare observed to expected frequencies as well as to compare frequencies between gender and age groups. No differences were found in rates of clinical scores among the groups on either youth self-report measure. Similar to parent report on the RCADS-P, rates of clinically significant scores on the RCADS were not statistically significantly different than the expected frequencies. Of the overall sample, 3 % had clinically elevated Total Anxiety and Depression scores on the RCADS, and rates of clinical subscale scores ranged from 2.5 % on the Social Anxiety subscale to 8.6 % on the Separation Anxiety subscale.
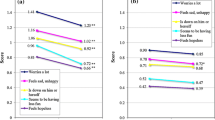
Several statistically significant differences emerged between observed and expected frequencies on the MASC subscales. Specifically, significantly more youth than expected (6.68 %) had clinically elevated scores on the Separation Anxiety subscale (χ2(1) = 23.09, p ≤ .001, critical p = .004) and on the Social Anxiety Performance subscale (χ2(1) = 7.89, p = .005, critical p = .005). Further, significantly fewer youth than expected had clinically significant elevations on the Harm Avoidance Perfectionism subscale χ2(1) = 10.41, p = .001, critical p = .005. Additionally, significantly more children between ages 8 to 12 than expected had clinical scores on the Harm Avoidance, Anxious Coping subscale χ2(1) = 9.00, p = .003, critical p = .005. Further, significantly more girls than expected had clinical scores on the Social Anxiety Total scale, χ2(1) = 8.52, p = .004, critical p = .005. No statistically significant differences in rates of clinically elevated scores emerged between boys and girls or between younger and older children on either the RCADS or the MASC.
Discussion
The present study is the first to our knowledge to examine the level and type of emotional and behavioral problems among children presenting in a PPC clinic serving primarily urban, economically disadvantaged African American youth. We used both self- and parent-report measures across a variety of behavioral health problem areas with a sample of nearly 200 children ages 8–17 and their caregivers. The majority of participants (75.6 %) had at least one subscale score that exceeded the clinical cutoff on either a parent- (62.4 %) or child-report (38.6 %) measure. These elevations were particularly notable on the SDQ where rates of parent elevations on several subscales were between two and three times higher than expected. However, self-reported anxiety and depression symptoms were not more frequent than would be expected in the general population.
Considering our focus on identifying the level of emotional and behavioral symptoms in a PPC clinic serving a predominantly urban, low-income, African-American population, our findings point in a few directions. First, consistent with past research, by parent-report, our sample of low income and ethnic minority youth exhibited higher levels of emotional and behavioral problems as measured by the SDQ. Parents in this clinic reported that their children have high levels of both emotional (e.g., unhappy, worries a lot) and behavioral problems (e.g., fights or bullies, lies or cheats). That they reported higher than expected levels of these problems is not surprising given the fact that the sample was comprised of low-income, ethnic minority youth [6, 36]. Studies suggest that racial and ethnic minority urban youth are at increased risk for exposure to a variety of factors associated with psychological illness, including poverty [8], community or domestic violence [37], and decreased access to behavioral health services [7]. Grant and colleagues [11] have postulated a mechanism through which family processes and economic stress mediate the relation between poverty and emotional and behavioral problems in urban, African American families. Thus, a move toward integrated care in the setting would address a need, at least as evidenced by parent report.
However, these higher-than-expected levels of problems were not in evidence by child-report nor by parent-report on a measure specifically designed to measure anxiety and depressive disorders. For all child-report measures (e.g., except the MASC Separation Anxiety scale, discussed shortly) and for the parent measure of anxiety and depression symptoms, the proportion of youth reported to be exhibiting clinical levels of symptoms was on par with the general population. This suggests a need for screening for these problems, but also indicates that the level of problems in this population may not be more extreme than in other groups. The two discrepancies noted in these data—between parent and child and within parent across measure—warrant consideration.
First, whom one asks about behavioral health problems clearly made a difference, a finding that is consistent with past work [23, 38]. The literature on how to identify the optimal reporter for child/adolescent behavior problems has been inconsistent. In the absence of a gold standard (i.e., there is no diagnostic test for presence/absence of behavioral health problem), researchers and clinicians have typically advocated the use of multiple reporters, given the fact that any one reporter has weaknesses [39]. Our findings support this general trend; screening in this primary care setting would have produced different results if only one reporter was solicited. In contrast to a similar study by Wren et al. [23], however, we did not find that children reported higher levels of anxiety or depression; differences between reporters on the RCADS were not statistically significant (though parents had higher scores).
Another consideration is the fact that rates of problems detected by parent report depended on which measure was used, with rates being higher for the SDQ than for the RCADS-P. Data supporting the psychometric properties of the SDQ in this population are somewhat mixed. Studies have shown that the SDQ possesses strong concurrent validity with diagnostic and other symptoms of psychopathology [40, 41], however, others have provided evidence that an alternate factor structure is a better fit for the parent/teacher version of the SDQ [42] as well as for the self-report version among primarily minority, urban American youth [43], and as such might be more sensitive for screening purposes. The RCADS-P has positive, though less abundant, evidence supporting its validity as a measure to detect clinical disorders in children [26]. The specificity of the RCADS-P items and scales compared to the more global items and scales of the SDQ may be a reason for the discrepancy. The RCADS targets symptoms of five specific anxiety disorders and depression whereas the SDQ captures emotional and behavioral problems more broadly.
Overall, our findings suggest that in this PPC setting, one would have drawn quite different conclusions about the behavioral health of the sample with only one of the two measures. Future studies could provide a more comprehensive assessment to determine which of the two conclusions is a more valid one. Regardless, it may be that using a broader distress measure like the SDQ may serve as a good initial screening measure to identify youth with possible emotional and behavioral symptoms.
One additional finding requires brief discussion. Girls, but not boys, reported clinically elevated symptoms of separation anxiety on the MASC at nearly three times the predicted rate. That more girls than boys demonstrated clinically elevated scores on an age- and gender-normed measure was consistent with previous research suggesting gender differences in anxiety symptoms in the general population [44], specific gender differences related to separation anxiety [45], and gender differences among urban, predominantly African American youth [46]. However, our finding was not consistent with either child or parent reports on the RCADS separation anxiety. Why were there discrepancies within reporter on similar scales across two measures? One reason may be related to differences in the way MASC and RCADS gauge separation anxiety. The MASC Separation Anxiety scale is an empirically derived scale that includes some specific DSM separation anxiety items (e.g., I get scared when my parents are away; I try to stay near my mom or dad) along with items found to be related to separation anxiety but not among the DSM symptoms (e.g., I keep the light on at night; Bad weather, the dark, heights, animals, or bugs scare me). In contrast, the RCADS items are based entirely on DSM-IV symptoms. Thus, whereas these scales are both labeled Separation Anxiety, they may measure slightly different constructs.
Nor was the elevation on separation anxiety we found among females consistent with a past study of African American adolescents from an urban parochial school [47]. In that study, African-American females had relatively low scores on the separation anxiety subscale of the MASC, leading Kingery et al. [47] to suggest that the subscale may be less salient for African American adolescents. The two studies focused on different populations (school vs. pediatric) and thus these differences alone may explain the discrepancy [48]. Further exploration of the possibility of elevated levels of separation anxiety in pediatric samples is warranted.
Our findings have multiple implications for future research and practice. Many have argued that PPC is an important context for screening mental health problems [18, 49]. As Lefler and colleagues outlined [18], screening tools should be psychometrically sound, brief, easy to complete within the context of a PPC visit, assess a broad range of problems, based on established diagnostic criteria, and facilitate physician referral to appropriate follow-up care. As this, and the work of others [42] indicates, more work is needed to determine the applicability and utility of screening measures in varied populations.
As models for integrating screening and assessment services proliferate [19, 50–52], research is needed to guide how to conduct screening and assessment efficiently. Further, more work is needed to understand how to best engage families in mental health screening and to ensure clinicians are equipped and prepared to provide appropriate referrals and follow-ups based on screening outcomes [49].
The present study has several methodological strengths, including a relatively large sample of underrepresented children and their caregivers, the use of parent and child self-report to gauge behavioral health problems, and measurement of a wide range of behavioral health problems. The results also must be considered in light of the study’s limitations. First, these data reflect parent- and child-reported symptom elevation and do not indicate disorder prevalence; families and youth were not queried using diagnostic instruments. Second, the study was designed as a needs assessment rather than a traditional epidemiological survey. As a result, the sample was not randomly drawn from the population of interest. Third, although the assessment battery sampled a wide array of behavioral health problems, several potentially important areas were not assessed, including traumatic stress disorders, pediatric bipolar disorder, pervasive developmental disorders, substance use disorders, and psychotic disorders. Future work could include a broader assessment battery to provide a more comprehensive picture of behavioral health problems in PPC settings.
Despite these limitations, the study represents an important first step in identifying the areas of need for an underserved and underrepresented group of youth in PPC. These data were also useful to a quantitative balance in the second phase of our project, in which we used qualitative methods to understand stakeholder perceptions about the extent of behavioral and emotional problems in the PPC setting and their thoughts about whether, and how best, to integrate behavioral health services into the setting. Overall, our findings underscore the relevance of the field’s evolution toward integrated care in pediatric settings. Further, our data suggest that the composition of a screening battery and the reporter(s) questioned are important considerations.
Summary
PPC clinics present an important setting for screening behavioral health problems, particularly among traditionally underserved ethnic minority children and children in poverty. The present study seeks to add to the current literature by providing descriptive information about the level and type of behavioral health symptoms reported among low-income African American children presenting for services in a PPC setting. Self- and parent-report measures were used across a variety of behavioral health problem areas with a sample of nearly 200 children aged 8–17 and their caregivers. The majority of participants had at least one subscale score that exceeded the clinical cutoff on either a parent- or child-report measure. These elevations were particularly notable on the SDQ where rates of parent elevations on several subscales were between two and three times higher than expected. However, parent- and self-reported anxiety and depression symptoms were not more frequent than would be expected in the general population. Future research is needed to better understand the applicability and utility of behavioral health screening measures, particularly among underserved and underrepresented populations.
References
Reef J, van Meurs I, Verhulst FC, van der Ende J (2010) Children’s problems predict adults’ DSM-IV disorders across 24 years. J Am Acad Child Adolesc Psychiatry 49:1117–1124
Lehrer JA, Shrier LA, Gortmaker S, Buka S (2006) Depressive symptoms as a longitudinal predictor of sexual risk behaviors among US middle and high school students. Pediatrics 118:189–200
Kaplow JB, Curran PJ, Angold A, Costello EJ (2001) The prospective relation between dimensions of anxiety and the initiation of adolescent alcohol use. J Clin Child Psychol 30:316–326
Foley DL, Goldston DB, Costello EJ, Angold A (2006) Proximal psychiatric risk factors for suicidality in youth: the Great Smoky Mountains study. Arch Gen Psychiatry 63:1017–1024
Copeland WE, Miller-Johnson S, Keeler G, Angold A, Costello JE (2007) Childhood psychiatric disorders and young adult crime: a prospective, population-based study. Am J Psychiatry 164:1668–1675
Kataoka SH, Zhang L, Wells KB (2002) Unmet need for mental health care among US children: variation by ethnicity and insurance status. Am J Psychiatry 159:1548–1555
Alegria M, Vallas M, Pumariega AJ (2010) Racial and ethnic disparities in pediatric mental health. Child Adolesc Psychiatr Clin N Am 19:759–774
Slopen N, Fitzmaurice G, Williams DR, Gilman SE (2010) Poverty, food insecurity, and the behavior for childhood internalizing and externalizing disorders. J Am Acad Child Adolesc Psychiatry 49:444–452
Flannery DJ, Wester KL, Singer MI (2004) Impact of exposure to violence in school on child and adolescent mental health and behavior. J Commun Psychol 32:559–573
Horowitz K, Weine S, Jekel J (1995) PTSD symptoms in urban adolescent girls: compounded community trauma. J Am Acad Child Adolesc Psychiatry 34:1353
Grant KE, Compas BE, Thurm AE, McMahon SD, Gipson PY, Campbell AJ et al (2006) Stressors and child and adolescent psychopathology: evidence of moderating and mediating effects. Clin Psychol Rev 26:257–283
Qi CH, Kaiser AP (2003) Behavior problems of preschool children from low-income families: review of the literature. Topics Early Child Spec Educ 23:188–216
Kelleher KJ, McInerny JK, Gardner WP, Childs GE, Wasserman RC (2000) Increasing identification of psychosocial problems. Pediatrics 105:1313–1321
Chavira AD, Stein MB, Bailey K, Stein MT (2004) Child anxiety in primary care: prevalent but untreated. Depress Anxiety 20:155–164
Costello EJ, Edelbrock C, Costello AJ, Dulcan MK, Burns BJ, Brent D (1988) Psychopathology in pediatric primary care: the new hidden morbidity. Pediatrics 82:415–424
Polaha J, Dalton WT, Allen S (2011) The prevalence of emotional and behavior problems in pediatric primary care serving rural children. J Pediatr Psychol 36:652–660
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A (2003) Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry 60:837–844
Lefler EK, Hartung CM, Fedele DA (2012) Psychometric properties of a primary care mental health screening tool for young children. Child Health Care 41:79–96
Brown JD, Riley AW, Wissow LS (2007) Identification of youth psychosocial problems during pediatric primary care visits. Adm Policy Ment Health 34:269–281
Costello EJ, Shugart MA (1992) Above and below the threshold: severity of psychiatric symptoms and functional impairment in a pediatric sample. Pediatrics 90:359–368
Neal AM, Turner SM (1991) Anxiety disorders research with African Americans: current status. Psychol Bull 109:400–410
Neighbors HW (1988) The help-seeking behavior of Black Americans: a summary of findings from the national survey of Black Americans. J Natl Med Assoc 80:1009–1012
Wren FJ, Berg EA, Heiden LA, Kinnamon CJ, Ohlson LA, Bridge JA et al (2007) Childhood anxiety in a diverse primary care population: parent-child reports, ethnicity, and SCARED factor structure. J Am Acad Child Adolesc Psychiatry 46:332–340
Weersing VR, Iyengar S, Kolko DJ, Birmaher B, Brent DA (2006) Effectiveness of cognitive-behavioral therapy for adolescent depression: a benchmarking investigation. Behav Ther 37:36–48
Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE (2000) Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther 38:835–855
Ebesutani C, Bernstein A, Nakamura BJ, Chorpita BF, Weisz JR (2010) A psychometric analysis of the Revised Child Anxiety and Depression Scale—Parent Version in a clinical sample. J Abnorm Child Psychol 38:249–260
Brown RC, Yaroslavsky I, Quinoy AM, Friedman AD, Brookman RR, Southam-Gerow MA (2013) Factor structure of measures of anxiety and depression symptoms in African American youth. Child Psychiatry Hum Dev 44:525–536
March JS, Parker JDA, Sullivan K, Stallings P, Conners CK (1997) The Multidimensional Anxiety Scale for Children (MASC): factor structure, reliability, and validity. J Am Acad Child Adolesc Psychiatry 36:554–565
Brown RC, Yaroslavsky I, Quinoy AM, Friedman AD, Brookman RR, Southam-Gerow MA (2013) Psychometric evaluation of measures of anxiety and depression symptoms in an urban African American sample. Child Psychiatry Hum Dev 44:525–536
Goodman R (1997) The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry 38:581–586
Bourdon KH, Goodman R, Rae DS, Simpson G, Koretz DS (2005) The Strengths and Difficulties Questionnaire: U.S. normative data and psychometric properties. J Am Acad Child Adolesc Psychiatry 44:557–564
Shirk SR, Kaplinski H, Gudmundsen G (2009) School-based cognitive-behavioral therapy for depression: a benchmarking study. J Emot Behav Disord 17:106–117
US Department of Health and Human Services (2009) Annual update of the HHS poverty guidelines. Fed Regist 74:4199–4201
Holm S (1979) A simple sequentially rejective multiple test procedure. Scand Stat Theory Appl 6:65–70
Jaccard J, Guilamo-Ramos V (2002) Analysis of variance frameworks in clinical child and adolescent psychology: issues and recommendations. J Clin Child Adolesc Psychol 31:130–146
Centers for Disease Control and Prevention (2010) Youth risk behavior surveillance—United States, 2009. MMWR Surveill Summ 59:1–142
Fitzpatrick KM, Boldizar JP (1993) The prevalence and consequences of exposure to violence among African American youth. J Am Acad Child Adolesc Psychiatry 32:424–430
Manassis K, Ickowicz A, Picard E, Antle B, McNeill T, Chahaver A et al (2009) An innovative child CBT training model for community mental health practitioners in Ontario. Acad Psychiatry 33:394–399
De Los Reyes A, Kazdin AE (2005) Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull 131:483–509
Goodman A, Goodman R (2009) Strengths and difficulties questionnaire as a dimensional measure of child mental health. J Am Acad Child Adolesc Psychiatry 48:400–403
Goodman A, Goodman R (2011) Population mean scores predict child mental disorder rates: validating SDQ prevalence estimators in Britain. J Child Psychol Psychiatry 52:100–108
Dickey WC, Blumberg SJ (2004) Revisiting the factor structure of the Strengths and Difficulties Questionnaire: United States, 2001. J Am Acad Child Adolesc Psychiatry 43:1159–1167
Ruchkin V, Jones S, Vermeiren R, Schwab-Stone M (2008) The Strengths and Difficulties Questionnaire: the self-report version in American urban and suburban youth. Psychol Assess 20:175–182
McLean CP, Anderson ER (2009) Brave men and timid women? A review of the gender differences in fear and anxiety. Clin Psychol Rev 29:496–505
Poulton R, Milne BJ, Craske MG, Menzies RG (2001) A longitudinal study of the etiology of separation anxiety. Behav Res Ther 39:1395–1410
Foster JD, Kuperminc GP, Price AW (2004) Gender differences in posttraumatic stress and related symptoms among inner-city minority youth exposed to community violence. J Youth Adolesc 33:59–69
Kingery JN, Ginsburg GS, Burstein M (2009) Factor structure and psychometric properties of the Multidimensional Anxiety Scale for Children in an African American adolescent sample. Child Psychiatry Hum Dev 40:287–300
Lambert SF, Cooley MR, Campbell KDM, Benoit MZ, Stansbury R (2004) Assessing anxiety sensitivity in inner-city African American children: psychometric properties of the Childhood Anxiety Sensitivity Index. J Clin Child Adolesc Psychol 33:248–259
Wissow LS, Brown J, Fothergill KE, Gadomski A, Hacker K, Salmon P et al (2013) Universal mental health screening in pediatric primary care: a systematic review. J Am Acad Child Adolesc Psychiatry 52:1134–1147
Bailey KA, Chavira DA, Stein MT, Stein MB (2006) Brief measures to screen for social phobia in primary care pediatrics. J Pediatr Psychol 31:512–521
Foy JM, Kelleher KJ, Laraque D, the American Academy of Pediatrics Task Force on Mental Health, (2010) Enhancing pediatric mental health care: strategies for preparing a primary care practice. Pediatrics 125:S87–S108
Weersing VR, Gonzalez A, Campo JV, Lucas AN (2008) Brief behavioral therapy for pediatric anxiety and depression: piloting an integrated treatment approach. Cogn Behav Pract 15:126–139
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hourigan, S.E., Southam-Gerow, M.A. & Quinoy, A.M. Emotional and Behavior Problems in an Urban Pediatric Primary Care Setting. Child Psychiatry Hum Dev 46, 289–299 (2015). https://doi.org/10.1007/s10578-014-0469-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-014-0469-z