
Abstract
The Social Responsiveness Scale (SRS) is a well-established measure of autism spectrum disorder (ASD), yet it is known to suffer reduced specificity in samples of children with comorbid emotional or behavioural problems. This research examined the specificity of the SRS in children with mixed presentations of internalising and externalising psychopathology and ASD. Participants were 522 (397 male) children aged between 4 and 16 years. The associations between SRS total scores and diagnoses were determined using partial correlations and analyses of variance. A subsample of participants with a single diagnosis was used to identify a subset of questions that distinguished between ASD and all other diagnoses. These items were used to create the 16-item SRS-brief. The SRS was found to have good reliability and sensitivity but poor specificity. The SRS-brief had good psychometric properties and was found to be a more accurate tool for the screening of ASD than the original SRS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is characterised by deficits in social communication and social interaction, and by repetitive behaviours/interests and/or sensory sensitivity [1]. The severity and expression of these symptoms can vary remarkably from mild difficulties in interpreting the nuances of social situations to a complete lack of verbal communication and adaptive deficits requiring substantial support.
The Social Responsiveness Scale (SRS) [2–4] is a 65 item scale that was developed to provide a measure of ASD that could be completed by a parent or teacher. The SRS was originally designed to be sensitive to the large range symptoms included in autistic disorder, Asperger’s syndrome and pervasive developmental delay-not otherwise specified (PDD-NOS), in accordance with DSM-IV diagnoses, and, by doing so, identify subtle forms of dysfunction across the core domains of the disorders. The Social Responsiveness Scale version 2 (SRS-2) [5] is identical to the original SRS for school-aged children (4–18 years) and has been found to have acceptable model fit with the two-factor structure of ASD as defined by DSM-5. As the original SRS and the SRS-2 are identical for the age range of children included in this research, the measure will simply be referred to as the SRS.
The SRS has been shown to have good predictive validity for ASD [3] that compares favourably with more time-intensive diagnostic tools such as the autism diagnostic interview-revised (ADI-R) [3]. In this respect the SRS is unique in that it offers a measurement of ASD that does not require specific clinical training to complete and, as such, is frequently utilised in both research and clinical settings.
Despite having been shown to have good predictive validity, the SRS has received some criticism. It has been argued that the SRS is too general and identifies children with broad behavioural deficits rather than those related to ASD specifically [6, 7]. The lack of specificity of the measure has recently been posited to be particularly important when using the SRS to detect ASD in clinical populations [6–8]. For example, Hus et al. [6] demonstrated that non-ASD behaviour problems were positively associated with SRS scores both for children with ASD and their unaffected siblings. As children with ASD commonly present with comorbid psychopathologies [9], and children with disruptive behaviour problems have been found often to have undetected disorders of social communication [10], the positive association between SRS scores and general behaviour problems is a challenge for the specificity of the SRS in clinical samples. This comorbidity is problematic for caregiver rating scales. While a clinical interview is flexible and allows for the interrogation of overlapping symptoms between diagnoses, a questionnaire measure, such as the SRS, must rely purely on the content of individual items to maximise its specificity and discriminant validity.
Overlap between the social/communication impairment seen in ASD and features of other childhood disorders and forms of dysfunction have often been emphasised in the clinical literature [9, 11, 12]. Children with anxiety disorders, for example, may be intimidated by social situations and may have problems interacting appropriately or making new friends. Towbin et al. [8] demonstrated that a substantial proportion of children with mood and anxiety disorders scored in the “ASD-likely” range of the SRS which, for children with ASD, represents at least mild to moderate impairment in everyday social interactions. Similarly, children with attention deficit hyperactivity disorder (ADHD) may find some aspects of social interaction and communication more difficult than healthy children. The impulsiveness commonly demonstrated by children with ADHD can negatively influence peer relations as these children often find prosocial behaviours such as turn-taking, cooperation, and responding appropriately to social cues difficult. Inattention and hyperactivity in the classroom can also isolate children with ADHD from their peers who may avoid social interactions due to their behaviour.
Another characteristic that influences social communication and interaction style in childhood is the presence of high levels of callous-unemotional (CU) traits. Children with high levels of CU traits are characterised by a set of social impairments including; lack of empathy, low levels of guilt and shallow affect. These features, when in the presence of conduct problems often index more serious and chronic difficulties with antisocial behaviour [13, 14] and have been included as a specifier to a diagnosis of conduct disorder (CD) in DSM-V [1]. For this reason, some features of CU traits appear to overlap with those of ASD. For example, a parent might describe their child as being “unsympathetic when another child is upset”. Both children with high levels of CU traits and those with ASD may be described accordingly but for different reasons. A child with ASD is likely not to understand why the child is upset—and so not know how to help appropriately. In contrast, a child with high levels of CU traits is more likely to understand why the child is upset but may not be inclined to help them. The apparent overlap between features of ASD and CU traits has attracted a great deal of attention in the clinical literature [15–17]. However, research demonstrates that they are distinct with respect to neural and genetic signatures [18, 19], underlying cognitive deficits [15, 16] and mechanisms of change [20].
The aim of this research was to test the specificity and sensitivity of the SRS in identifying ASD in a clinical sample of children with behavioural problems. Specifically, we intended to determine whether scores on the SRS were associated with childhood psychopathologies other than ASD and, if so, whether the SRS could be adapted to make the measure less sensitive to these diagnoses thereby improving its discriminant validity in mixed clinical samples.
Methods
Participants
Families were recruited between 2007 and 2012 for assessment and treatment of a behaviour problem. Participants were (N = 522; 397 male) children aged from 4 to 16 years (M = 8.40, SD = 3.10). All children met the criteria of referral for behavioural problems associated with a diagnosis of oppositional-defiant disorder (ODD) or CD, ADHD, ASD (originally diagnosed with autistic disorder or Asperger’s syndrome when using DSM-IV criteria), anxiety or depressive disorder (Anx/Dep) using DSM-IV criteria [21]. Primary and secondary diagnoses were as follows: primary diagnosis; ODD/CD = 54 %, ADHD = 28 %, ASD = 9 %, anxiety/depression = 9 %; Secondary diagnosis: ODD/CD = 26 %, ADHD = 18 %, ASD = 3 %, anxiety/depression = 13 %, no other diagnosis = 40 %. Comorbidity was common in this sample; 47 % had two diagnoses and 13 % had three or more. Participants with a single primary diagnosis were used to form a “pure diagnostic” subsample (N = 224, male = 163). Participants who had two or more diagnoses were grouped to form the second “comorbid” subsample (N = 298, male = 234). In total N = 66 participants were diagnosed with ASD; 18 of these participants had a single diagnosis of ASD and 48 had a diagnosis of ASD in addition to a comorbid diagnosis. Additional inclusion criteria were: no developmental delay (assessed by a clinical psychologist and confirmed, where possible, by a full scale IQ > 70) and no major medical disability (according to parent report). The SRS has been demonstrated to have lower specificity for participants with IQ < 70 than for those with IQ >= 70 [7], hence the exclusion of the low IQ participants. Table 1 shows the diagnostic characteristics of the whole sample and of each diagnostic group.
Measures
The SRS [4] is a 65 item scale that requires parents to rate their children’s behaviours in the past 6 months. The SRS is designed to capture autistic symptoms and impairments in natural setting [22]. Each item is rated on a 4 point scale ranging from 0 (never true) to 3 (almost always true) with 17 items reverse scored. The SRS yields a total raw (SRS-Raw) score and gender-normed T-scores. Higher scores indicate greater severity of social impairment; T-scores <60 are considered normal, T-scores between 60 and 75 inclusive indicate clinically significant impairment in the mild to moderate range, and T-scores >75 indicate severe social impairment. As such, T-scores greater than or equal to 60 are used to indicate that a diagnosis of ASD may be appropriate [4]. The SRS measures impairment across four broad areas: social information processing, capacity for reciprocal responses, social use of language, and stereotypic/repetitive behaviours and preoccupations. The scale items are classified into five categories (social cognition, social motivation, social communication, social awareness and autistic mannerisms) accordingly [22]. Confirmatory factor analysis demonstrates that the SRS (for children aged 4–18 years) has acceptable model fit for a two-factor structure of ASD that corresponds to DSM-5 criteria of social communication impairment and restricted, repetitive behaviour [5].
Cronbach’s alpha reliability of the SRS total in this sample was high α = 0.91. Mothers and fathers (where available) completed the SRS. Correlations were high between mother and father reported SRS scores (N = 262, r = 0.65, p < 0.001). Only 262 out of the 522 participants had father-reported SRS scores in addition to mother-reported SRS scores. Therefore only mother-reported SRS scores were used in this research.
Callous-Unemotional traits were measured by combining the parent report on the antisocial process screening device (APSD) [23] and the prosocial subscale of the Strengths and Difficulties Questionnaire (SDQ) [24]. Scores can range from 0 to 16. This method has been validated by factor analysis [25] and has been used in previous research [25–27]. In this study Cronbach’s reliability of the CU traits scale was high α = 0.71. CU traits were measured by multi-informants (mother, father and teacher). Mother-rated CU traits were used in this research as they provided the most data and because correlations were large between mother and father reported CU traits (N = 266, r = 0.52, p < 0.001). Correlations between mother and teacher reported CU traits were also significant and of a small to medium effect size [28] (N = 330, r = 0.20, p < 0.001).
Current diagnostic status of the child was derived by the assessing psychiatrist/psychologist using a weighted combination of: (1) DSM-IV criteria [21] assessed using the diagnostic interview schedule for children, adolescents, and parents (DISCAP) [29, 30] with parents, and the child for those older than 8 years, (2) historical information and diagnoses in referral letters from medical practitioners, and (3) interviews, where possible, with current school teachers. Diagnoses were rated in severity on a scale from 0 to 6 where a rating of three or more indicates clinically relevant levels of symptom severity. Diagnostic reliability was assessed for approximately 20 % of cases by having a specialist team of psychologists/psychiatrists make an independent diagnosis while ‘blind’ to the primary clinician’s formulation. Kappa agreements across all diagnoses were 0.77.
In line with the use of CU traits as a specifier in DSM-V, children with conduct problems (CP: a diagnosis of CD or ODD) were categorised into two groups according to their level of CU traits. Previous research suggests a range between the top 45 and 20 % of aggressive/antisocial groups to represent high CU traits [13, 25, 31]; thus, children with CP and a CU traits score that were equal to or less than the 33rd percentile were categorised as the CPCU− group. Children with CP and a CU traits score greater than this value were categorised into the CPCU+ group.
Procedure
Ethics approval was from the Human Research Ethics Committee of the University of New South Wales (UNSW). Participants were referrals (either self-referrals from parents or referred by school teachers, mental health professionals, general practitioners or social workers) to the Child Behaviour Research Clinic at the UNSW and Royal Far West, Manly. Participants and at least one of their primary caregivers volunteered to take part in the research. Primary caregivers provided written informed consent to take part in the research and also provided written informed consent on behalf of their participating child/children. Adolescents (over the age of 12) were required to provide independent written informed consent. The child’s primary caregiver completed the questionnaire measures (SRS, APSD and SDQ) at the initial assessment.
Results
Statistical analyses were performed using SPSS 20.0 (IBM Statistics, Chicago). Prior to analyses the SRS total, individual SRS items, and the CU traits scale were evaluated and found to meet the assumptions of univariate and multivariate normality. As the sample used in this research comprised males and females, raw SRS scores were converted into gender-normed T-scores so that the sample would not need to be split by gender for analyses. These gender-normed T scores are used throughout.
The Relationship Between SRS Total Score and Diagnostic Severities in a Mixed Clinical Sample
Our approach to analysis was carried out in stages. The first step was to assess the relationships between SRS total T scores, ASD severity, and symptom severity of the main diagnostic categories. For this analysis, the whole sample (N = 522) was used so as to represent the typical mixed clinical presentations (single diagnoses and comorbid diagnoses of varying severities) found in non-ASD-specialist childhood psychopathology centers. To this end, partial correlations were conducted controlling for age as this variable has been indicated by previous research to influence SRS scores [6] and was significantly associated with SRS total scores in this sample (age, r = 0.30, p < 0.001). Power calculations show that for a two-tailed correlation analysis a sample size of 522 is large enough to detect an effect size of r = 0.1 with adequate power (β = 0.80) at an alpha level of 0.05.
The results from the partial correlations indicated that total SRS scores were significantly and substantially correlated with ASD (r = 0.40, p < 0.001) and CU traits (r = 0.35, p < 0.001), and significantly but weakly correlated with anxiety/depression (r = 0.10, p = 0.028). As this sample included children with a diagnosis (primary, secondary or tertiary) of ASD, partial correlations were next conducted while controlling for ASD severity so that the independent relationships between the other diagnostic severities and SRS scores could be determined. When controlling for ASD severity and age, significant but very weak positive correlations were found between SRS total scores and ADHD (r = 0.14, p = 0.001), Anx/Dep (r = 0.11, p = 0.014) and CP (r = 0.10, p = 0.021). SRS total scores were significantly and moderately correlated with CU traits (r = 0.35, p < 0.001).
Differences in SRS Total Score Between Diagnostic Groups
In order to unpack the nature of the associations between SRS total scores and non-ASD clinical diagnoses, the following analyses were conducted using the pure diagnostic subsample of children (N = 224). The pure diagnostic subsample was used so that the independent relationships between SRS scores and the five pure diagnostic groups [ASD (N = 18), Anx/Dep (N = 22), ADHD (N = 38), CPCU− (N = 99) and CPCU+ (N = 47)] could be determined with the knowledge that the associations were not being influenced by comorbid features of ASD or other diagnoses.
First, analyses of variance were conducted to compare mean SRS total scores between the five diagnostic groups while controlling for age. Power calculations show that a total sample size of 224 is large enough to detect an effect size of F = 0.2 with adequate power (β = 0.80) at an alpha level of 0.05. Age-adjusted mean SRS total score was significantly higher for the ASD group [M = 82.2, SEM = 2.9, 95 % CI (76.4, 87.9)] than for all other diagnostic groups [ADHD: M = 63.8, SEM = 2.1, 95 % CI (59.6, 67.9); Anx/Dep: M = 65.7, SEM = 2.7, 95 % CI (60.5, 71.0); CPCU−: M = 62.4, SEM = 1.3, 95 % CI (59.9, 65.0); CPCU+: M = 69.3, SEM = 1.8, 95 % CI (65.7, 72.8)] [F(4,218) = 10.84, p < 0.001]. Post-hoc pairwise comparisons demonstrated that a significant difference in mean SRS total score was also present between the CPCU− and CPCU+ groups showing that children with CPCU+ had significantly higher mean SRS total scores that children with CPCU− (Mean diff = 12.35, SE = 4.31, p = 0.005). Mean SRS total T scores for all diagnostic groups (ASD, ADHD, CPCU−, CPCU+ and Anx/Dep) were found in this sample to be above the “normal” cut-off score and fell into the “mild to moderate” range of ASD symptom severity according to the SRS test interpretation manual [4].
Determining Item-Specific Diagnostic Overlap
As the mean SRS total T scores for the four non-ASD diagnostic groups (ADHD, CPCU−, CPCU+ and Anx/Dep) were higher than would be expected from a sample without ASD, we next ran analyses of variance to determine which items on the SRS were failing to distinguish between ASD and other diagnoses. To this end, diagnostic group (ASD, ADHD, Anx/Dep, CPCU−, CPCU+) was included as the independent factor, age was included as a covariate and mean score on each of the 65 items of the SRS were included as the dependent variables. The results of these analyses are summarized in Table 2. Only 16 items from the original 65 were found to distinguish the ASD group from all other diagnostic groups; these items are displayed in Table 3.
The Creation of a Brief Version of the SRS for Use in Clinical Samples
In order to test whether a brief version of the SRS (SRS-brief), comprised only of these 16 items that distinguished ASD from other diagnostic groups, could be useful as a tool for use in mixed clinical samples, we first calculated the mean raw scores for these 16 items for each participant. Next, these mean scores were converted into T scores by first multiplying the mean score by 65/16 to make it comparable to mean scores for the original SRS and then by transforming these scores into their corresponding T scores according to the participant’s gender [4]. These scores were then termed “SRS-brief total scores”.
The SRS and SRS-Brief as Indicators of an ASD Diagnosis
As the SRS-brief was developed from data obtained only from the pure diagnostic subsample (N = 224), the psychometric properties of the SRS-brief were first assessed in this subsample and were then tested again in the independent comorbid subsample (N = 298). In the pure diagnostic subsample reliability for the SRS-brief (α = 0.91) was found to be marginally better than for the original SRS (α = 0.90). Reliability was then checked in the comorbid sample and was found to be marginally greater in the original SRS (α = 0.90) than in the SRS-brief (α = 0.89). In both samples, reliabilities of the original SRS and SRS-brief were excellent [32].
Next, the sensitivity and specificity of the SRS-brief were tested and compared to the original SRS by plotting ROC curves. ROC analyses were conducted with the optimal cut-off for sensitivity and specificity selected by calculating the point on the graphs with the shortest distance from the optimal point (0, 1). Both ROC plots are displayed in Fig. 1.

ROC curves depicting the relationship between sensitivity and one minus specificity (false positive rate) for the original SRS (dashed line) and SRS-brief (solid line) total t scores
For the pure diagnostic subsample, the SRS-brief demonstrated good accuracy [33] [area under the curve was 0.89, p < 0.001 (95 % CI 0.82–0.96)]. As an optimal test the SRS-brief cut-off was 72 with a sensitivity of 0.81 and a false positive rate of 0.22. For a cut-off score of 60 indicating “ASD likely”, the sensitivity of the SRS-brief was 1.00 with a false positive rate of 0.42. The ROC area for the original SRS in this sample was 0.87, p < 0.001 (95 % CI 0.80–0.94), indicating good accuracy. The optimal original SRS cut-off score for discriminating participants diagnosed with ASD from those without ASD was 73.5 with a sensitivity of 0.81 and a false positive rate of 0.24. For a cut-off score of 60 indicating “ASD likely”, the sensitivity of the SRS-brief was 1.00 with a false positive rate of 0.55.
For the comorbid subsample, the SRS-brief demonstrated good accuracy [area under the curve was 0.81, p < 0.001 (95 % CI 0.75–0.87)]. As an optimal test the SRS-brief cut-off was 74 with a sensitivity of 0.76 and a false positive rate of 0.30. For a cut-off score of 60 indicating “ASD likely”, the sensitivity of the SRS-brief was 0.96 with a false positive rate of 0.58. The ROC area for the original SRS in this sample was 0.80, p < 0.001 (95 % CI 0.74–0.87), indicating good accuracy. The optimal cut-off score for discriminating participants diagnosed with ASD from those without ASD was 76.5 with a sensitivity of 0.82 and a false positive rate of 0.28. For a cut-off score of 60 indicating “ASD likely”, the sensitivity of the original SRS was 0.96 with a false positive rate of 0.75.
Differences in SRS Total Score Between Pure Diagnostic Groups
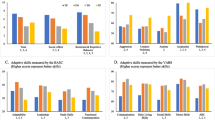
As the SRS-brief was shown to have excellent internal consistency and good accuracy we next tested whether the SRS-brief would demonstrate greater discriminant validity than the original SRS in the pure diagnostic subsample. Thus, the relationships between SRS-brief scores and the five pure diagnostic groups [ASD (N = 18), Anx/Dep (N = 22), ADHD (N = 38), CPCU− (N = 99) and CPCU+ (N = 47)] were assessed by means of analyses of variance. Mean SRS-brief total scores were compared between the five diagnoses while controlling for age. The mean SRS-brief total scores for each diagnosis are displayed in Table 4 alongside the corresponding raw scores. Mean SRS-brief total score was significantly higher for the ASD group than for all other diagnostic groups [F(4,218) = 11.74, p < 0.001]. Post-hoc pairwise comparisons demonstrated that there were no other significant differences in mean SRS-brief scores between any of the other diagnoses (ps > 0.30). The mean SRS-brief total score for the children with a single primary diagnosis of ASD was 88.8. Mean SRS-brief total scores for all other diagnostic groups (ADHD, CPCU−, CPCU+ and Anx/Dep) ranged from 58.6 (ADHD) to 62.5 (CPCU+) with only the mean score for children in the CPCU+ group falling above the upper cut-off for the “normal” range of ASD characteristics according to the SRS test interpretation manual [4]. Age-adjusted mean total scores on the original SRS and the SRS-brief are plotted in Fig. 2. The percentage of children in each diagnostic group scoring at or above the SRS total T score cut-off (60) for an “ASD-likely” diagnosis are shown in Table 4.

Bar graph depicting the estimated marginal mean SRS T scores for the original SRS (light bars) and SRS-brief (dark bars) according to diagnostic group and controlling for age (evaluated at 8.26 years). Scores under 60 (indicated by the dashed horizontal line) are considered to be in the normal range
Discussion
The SRS (and SRS-2 for school-aged children) is a commonly used questionnaire for assessing ASD that fulfils the need for a brief index of ASD. Recently, however, the specificity of the SRS in clinical samples has been brought under question. It is important that in a clinical sample of children the SRS is able to distinguish between ASD and features associated with comorbid diagnoses and traits.
This research aimed to determine the discriminant validity of the SRS in clinical samples of children with common diagnoses (ASD, ADHD, CPCU−, CPCU+ and Anx/Dep). The results demonstrated that across the whole sample, which included children with a single diagnosis and children with comorbid pathologies, total scores on the SRS were associated with anxiety/depression, ADHD, CP and levels of CU traits when controlling for ASD. Children with a single diagnosis of ADHD, Anx/Dep, or CP (associated with, and without, high levels of CU traits) were found to have SRS total scores that fell above the cut-off used to indicate that a diagnosis of ASD is likely. As such, the associations between individual items of the SRS and discrete diagnoses were tested and it was found that only 16 items from the SRS distinguished between ASD and all other diagnoses. These 16 items were used to create an abbreviated scale (SRS-brief) which was then tested for reliability, specificity, sensitivity first in the subsample of children with a single diagnosis and then again in a subsample of children with comorbid diagnoses. The discriminant validity of the SRS-brief was then tested in the pure diagnostic subsample.
This research demonstrated that the original SRS has good reliability and high sensitivity in mixed clinical samples of children. As a screening tool, however, the specificity of the original SRS was poor with a false positive rate of 0.55 in the pure diagnostic subsample and a false positive rate of 0.75 in the comorbid subsample. In other words, the original SRS incorrectly classified the majority of children in both subsamples as being likely of having a diagnosis of ASD.
The SRS-brief that comprised 16 items from the original SRS was found to have excellent reliability. ROC analyses of the SRS-brief demonstrated that this abbreviated measure had better accuracy than the original SRS in both the pure diagnostic subsample and the comorbid sample. In the subsample of children with a single diagnosis the sensitivity of the SRS-brief was found to be equivalent to the original SRS both at the optimal point and at the screening total score of 60. The sensitivity of the SRS-brief as a screening measure was also shown to be better than that of the original SRS in this sample with a false positive rate of 0.42 as compared to 0.55. In the comorbid sample, both the sensitivity (0.76) and specificity (false positive = 0.30) of the SRS-brief were not as good as those of the original SRS (sensitivity = 0.82, false positive = 0.28). However, when used as a screening measure in the comorbid sample (using a cut-off score of 60 to indicate “ASD-likely”), the SRS-brief was found to have equivalent sensitivity (0.96) and a lower false positive rate than the original SRS (0.58 as opposed to 0.75).
The results from this research are in accordance with findings from previous research that has suggested that the SRS may over-identify ASD in clinical populations [6, 8, 34]. The SRS-brief was created in order to try and improve the discriminant validity of the SRS in clinical samples and to provide a reliable and valid ASD screening tool that is less influenced by comorbid diagnoses and traits. Initial results from the sample used in this research suggest that the SRS-brief may be a useful adaptation to the original SRS with specific utility in the screening of ASD in comorbid clinical samples. As with the original SRS, the SRS-brief should only be used as a tool to indicate which children may benefit from further assessment of an ASD diagnosis and should not be used to indicate the presence or absence of an ASD diagnosis itself. The lower false positive rates found for the SRS-brief than for the original SRS when used as a screening measure suggest that the SRS-brief will be useful in reducing the number of children without ASD who are needlessly sent for further assessment. As the full assessment of ASD requires a clinical psychologist or psychiatrist and multi-informants a tool that can help to reduce the number of children incorrectly identified as needing assessment would save time and money for both research and clinical settings.
While the SRS-brief has improved discriminant validity as compared to the original SRS, mean SRS-brief scores were still over the cut-off for an “ASD-likely” diagnosis for the group of children with conduct problems characterised by high levels of CU traits. Indeed, for all other diagnostic groups (ADHD, Anx/Dep, CPCU−), the percentage of children that scored above this cut-off ranged from 40 to 59 %. As such, it is important to note that limitations to the discriminant validity of the SRS-brief in clinical samples remain. As the sample used in this research did not include a non-clinical control group, it remains to be seen whether the SRS-brief has improved sensitivity and specificity as a screening tool for ASD in non-clinical populations. Other possible limitations include the use of a small sample of children (N = 18) with a single ASD diagnosis to determine the items to be included in the SRS-brief, the use of only mother-reported SRS scores, and the exclusion of children with IQ < 70. As such, further research and testing of the SRS-brief in a variety of clinical and non-clinical samples should be conducted using multi-informants before any conclusions regarding the generalizability of the SRS-brief can be made. Despite these limitations and the need for further testing and validation, the SRS-brief shows promise as an adaptation to the original SRS that may improve the applicability and efficacy of the measure as a screening tool in clinical settings.
Summary
The SRS is a widely used and well-established measure of ASD, yet it is known to suffer reduced specificity in samples of children with comorbid emotional or behavioural problems. This research examined the specificity of the SRS in two clinical samples of children with mixed presentations of internalising and externalising psychopathology and ASD. Participants were 522 (397 male) children aged between 4 and 16 years referred for behavioural problems associated with a diagnosis of ODD or CD, ADHD, ASD, Anx/Dep. For use in analyses, participants were subdivided into two independent subsamples; participants in the first sample had a single primary diagnosis while those in the second sample had two or more diagnoses. The associations between SRS total scores and diagnoses were determined using partial correlations and analyses of variance. The first subsample of participants with a single diagnosis was used to identify a subset of questions that distinguished between ASD and all other diagnoses. These items were used to create the SRS-brief. The accuracies and discriminant validities of the original SRS and the SRS-brief were assessed in both samples. SRS total scores were positively associated with CU traits, anxiety/depression, conduct problems and ADHD. The SRS had good reliability and sensitivity but poor specificity. The SRS-brief was found to have good psychometric properties and to be a more accurate tool for the screening of ASD than the original SRS. The SRS-brief is an adaptation to the SRS that may be a useful screening tool in research and clinical settings.
References
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington, VA
Constantino JN, Przybeck T, Friesen D, Todd RD (2000) Reciprocal social behaviour in children with and without pervasive developmental disorders. J Dev Behav Pediatr 21(1):2–11
Constantino JN, Davis SA, Todd RD et al (2003) Validation of a brief quantitative measure of autistic traits: comparison of the social responsiveness scale with the Autism diagnostic interview-revised. J Autism Dev Disord 33(4):427–433
Constantino JN, Gruber CP (2005) The Social Responsiveness Scale. Western Psychological Services, Los Angeles
Frazier TW, Ratliff KR, Gruber C et al (2013) Confirmatory factor analytic structure and measurement invariance of quantitative autistic traits measured by the Social Responsiveness Scale-2. Autism 18(1):31–44
Hus V, Bishop S, Gotham K, Huerta M, Lord C (2012) Factors influencing scores on the social responsiveness scale. J Child Psychol Psychiatry 54(2):216–224
Charman T, Baird G, Simonoff E et al (2007) Efficacy of three screening instruments in the identification of autistic-spectrum disorders. Br J Psychiatry 191:554–559
Towbin KE, Pradella A, Gorrindo T, Pine DS, Leibenluft E (2005) Autism spectrum traits in children with mood and anxiety disorders. J Child Adolesc Psychopharmacol 15(3):452–464
Simonoff E, Pickles A, Charman T et al (2008) Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am Acad Child Adolesc Psychiatry 47(8):921–929
Donno R, Parker G, Gilmour J, Skuse DH (2010) Social communication deficits in disruptive primary-school children. Br J Psychiatry 196(4):282–289
Storch EA, Arnold EB, Jones AM et al (2012) The role of co-occurring disruptive behaviour in the clinical presentation of children and adolescents with anxiety in the context of autism spectrum disorders. Child Psychiatry Hum Dev 43(5):734–746
Taurines R, Schwenck C, Westerwald E et al (2012) ADHD and autism: differential diagnosis or overlapping traits? A selective review. Atten Defic Hyperact Disord 4(3):115–139
Rowe R, Maughan B, Moran P et al (2010) The role of callous and unemotional traits in the diagnosis of conduct disorder. J Child Psychol Psychiatry 51(6):688–695
Frick PJ, Stickle TR, Dandreaux DM, Farrell JM, Kimonis ER (2005) Callous-unemotional traits in predicting the severity and stability of conduct problems and delinquency. J Abnorm Child Psychol 33(4):471–487
Jones AP, Happé FGE, Gilbert F, Burnett S, Viding E (2010) Feeling, caring, knowing: different types of empathy deficit in boys with psychopathic tendencies and autism spectrum disorder. J Child Psychol Psychiatry 51(11):1188–1197
Rogers J, Viding E, Blair RJ, Frith U, Happé F (2006) Autism spectrum disorder and psychopathy: shared cognitive underpinnings or double hit? Psychol Med 36(12):1789–1798
Blair RJR (2008) Fine cuts of empathy and the amygdala: dissociable deficits in psychopathy and autism. Q J Exp Psychol 61(1):157–170
Cox CL, Uddin LQ, Di martino A et al (2012) The balance between feeling and knowing: affective and cognitive empathy are reflected in the brain’s intrinsic functional dynamics. Soc Cogn Affect Neurosci 7(6):727–737
Jones AP, Larsson H, Ronald A et al (2009) Phenotypic and aetiological associations between psychopathic tendencies, autistic traits, and emotion attribution. Crim Justice Behav 36(11):1198–1212
Hawes DJ, Dadds MR, Brennan J, Rhodes T, Cauchi A (2013) Revisiting the treatment of conduct problems in children with callous-unemotional traits. Aust N Z J Psychiatry 47(7):646–653
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, 4th edn. American Psychiatric Association, Washington, DC
Constantino JN, Gruber CP, Davis S et al (2004) The factor structure of autistic traits. J Child Psychol Psychiatry 45(4):719–726
Frick PJ, Hare RD (2001) Antisocial process screening device. Multi-Health Systems, Toronto
Goodman R (1997) The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry 38(5):581–586
Dadds MR, Frost A, Fraser J, Hawes DJ (2005) Disentangling the underlying dimensions of psychopathy and conduct problems in childhood: a community study. J Consult Clin Psychol 73(3):400–410
Dadds MR, El Masry Y, Wimalaweera S, Guastella AJ (2008) Reduced eye gaze explains “fear blindness” in childhood psychopathic traits. J Am Acad Child Adolesc Psychiatry 47(4):455–463
Pasalich DS, Dadds MR, Hawes DJ, Brennan J (2012) Attachment and callous-unemotional traits in children with early onset conduct problems. J Child Psychol Psychiatry 52(8):838–845
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159
Holland D, Dadds MR (1997) Inventors. The diagnostic interview schedule for children, adolescents, and parents. Griffith University, Brisbane
Dadds MR, Cauchi AJ, Wimalaweera S, Hawes DJ, Brennan J (2012) Outcomes, moderators, and mediators of empathic-emotion recognition training for complex conduct problems in childhood. Psychiatry Res 199(3):201–207
Frick PJ, Moffitt TE (2010) A proposal to the DSM–V childhood disorders and the ADHD and Disruptive behaviour disorders work groups to include a specifier to the diagnosis of conduct disorder based on the presence of callous-unemotional traits. American Psychiatric Association, Washington
George D, Mallery P (2003) SPSS for Windows step by step: a simple guide and reference. 11.0 update, 4th edn. Allyn & Bacon, Boston
Kleinbaum DG, Klein M (2010) Logistic regression: a self-learning text. Springer, New York
Aldridge FJ, Gibbs VM, Schmidhofer K, Williams M (2012) Investigating the clinical usefulness of the Social Responsiveness Scale (SRS) in a tertiary level, autism spectrum disorder specific assessment clinic. J Autism Dev Disord 42(2):294–300
Acknowledgments
The authors would like to thank the staff of the Child Behaviour Research Clinic, University of New South Wales and Royal Far West, Manly and the children and their families who took part in this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moul, C., Cauchi, A., Hawes, D.J. et al. Differentiating Autism Spectrum Disorder and Overlapping Psychopathology with a Brief Version of the Social Responsiveness Scale. Child Psychiatry Hum Dev 46, 108–117 (2015). https://doi.org/10.1007/s10578-014-0456-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-014-0456-4