
Abstract
Despite progress in research on evidence-based treatments (EBTs) for youth psychopathology, many youths with mental health needs do not receive services, and EBTs are not always effective for those who access them. Wise interventions (WIs) may help address needs for more disseminable, potent youth mental health interventions. WIs are single-component, social–psychological interventions designed to foster adaptive meaning-making. They have improved health-related and interpersonal youth outcomes, yet their potential to reduce youth psychopathology has not been systematically explored. Accordingly, we conducted a systematic, descriptive review characterizing WIs’ potential to reduce youth mental health problems. Across 25 RCTs (N = 9219 youths, ages 11–19) testing 13 intervention types, 7 WIs qualified as “Well-Established,” “Probably Efficacious,” or “Possibly Efficacious” for reducing one or more types of youth psychopathology, relative to controls. Among these, 5 WIs significantly reduced youth depressive symptoms; 3, general psychological distress; and 1 each, eating problems, anxiety, and substance use. Three of these 7 WIs were self-administered by youths, and four by trained interventionists; collectively, they were 30–168 min in length and targeted clinic-referred and non-referred samples in clinical, school, and laboratory settings. Overall, certain WIs show promise in reducing mild-to-severe youth psychopathology. Given their brevity and low cost relative to traditional (i.e., therapist-delivered, 12- to 16-week, clinic-based) EBTs, WIs may represent beneficial additions to the youth mental healthcare ecosystem. Priorities for future research are proposed, including testing WIs for parents, younger children, and externalizing problems; as EBT adjuncts; and in schools and primary care clinics to increase access to brief, effective supports.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Efforts to deploy evidence-based treatments (EBTs) for psychopathology have advanced greatly, yet they have not reduced the overall burden of youth mental illness. This discrepancy stems partly from service accessibility and potency: up to 80% of youth with mental health problems do not receive services, and EBTs are not always effective for those who do access them (Kataoka et al. 2002; Konrad et al. 2009; Weisz et al. 2018). Social–psychological research on wise interventions (WIs) may help address this need through more readily accessible yet potent strategies to reduce psychopathology for youths and families in need. Wise interventions (WIs) are precise, theory-based, brief techniques that target specific psychological processes to help people flourish across diverse life domains. WIs aim to systematically promote adaptive meaning-making and attributions about the self and social worlds—particularly in response to stress, threat, and challenge. In turn, these more adaptive ways of thinking can spur changes in beliefs and behavior in ways that accrue over time (Walton and Wilson 2018). In controlled studies and field trials, WIs have yielded benefits for interpersonal and health-related outcomes for youth (Duckworth et al. 2013; Walton 2014; Walton and Wilson 2018; Yeager and Dweck 2012). However, their promise in reducing and preventing youth mental health problems remains largely unexplored. Accordingly, the goal of this manuscript is to systematically review the evidence to date, and present future possibilities, for applying WIs to treating and preventing psychopathology in youth—including internalizing problems, externalizing problems, and substance use. We first provide a working definition of WIs, noting their similarities and differences from existing evidence-based treatments (EBTs) for youth mental health problems. Next, we summarize evidence supporting positive effects of WIs on youths’ interpersonal, academic, and physical health outcomes, providing descriptions of commonly tested WIs and introducing their potential to address diverse youth mental health concerns. We then present a systematic review of randomized trials that have evaluated the effects of WIs on youth mental health problems, outlining their design, content, and effectiveness for reducing youth psychopathology.Footnote 1 Finally, we propose priority areas for future work on WIs for youth mental health. We hope to offer a roadmap toward a translational social–clinical intervention science, incorporating WIs, EBTs, and their integration to improve the potency and accessibility of psychological supports for youth.
Defining and Differentiating “Wise” Interventions
WIs have been defined by Walton and Wilson (2018) as “[interventions] that focus on (are “wise to”) the meanings and inferences people draw about themselves, other people, or a situation they are in and use precise, theory- and research-based techniques to alter these meanings.” (p. 6). The “meanings” that WIs are designed to alter have been referenced in myriad ways in social and clinical psychological literatures, including lay theories (Furnham 1988), causal attributions (Weiner 1985), and cognitive distortions (Beck 2008). In sum, these “meanings” are people’s guiding beliefs about the self and the social world that directly guide their interpretations of stress, their inclinations toward adaptive versus maladaptive coping strategies, and in turn, their functioning across critical life domains. Consistent with cognitive-behavioral models of psychopathology (Beck 1967), WIs are rooted in the scientific premise that people’s behavior stems from their interpretations of themselves and their social environment, and that those interpretations are modifiable through targeted, precise interventions.
Based on past thematic analyses of WIs and meta-analyses of clinical interventions for youth mental health (Walton and Wilson 2018; Weisz et al. 2018), WIs both overlap with and differ from traditional EBTs for youth mental health—i.e., those that are clinic-based, span 12–16 weekly sessions, and are designed for delivery by a trained therapist (Weisz et al. 2018). Their primary similarity appears to rest in the types of basic, beliefs that WIs are designed to address, categorized into three groups through a review and thematic analysis conducted by Walton and Wilson (2018): beliefs promoting understanding (viewing the world in a realistic way that matches lived experience), self-integrity (thinking well of one’s self), or belongingness (feeling connected to valued others). In other words, Walton and Wilson’s review identified WIs as being used to target and strengthen thinking styles (i.e., beliefs) linked to adaptive functioning, both intra- and interpersonally. Traditional EBTs for youth internalizing and externalizing psychopathology routinely address a similar set of beliefs. For instance, cognitive-behavioral and interpersonal treatments for youth depression teach youths to combat unrealistic predictions about the likelihood of negative outcomes (understanding), reduce negative self-talk (self-integrity), and restore feelings of connectedness with others (belonging); and evidence-based treatments for youth aggression and behavior problems often aim to neutralize hostile attribution bias (understanding), mitigate views of one’s self as a “bad kid” (self-integrity), and reduce conflict with peers and family members (belonging). Thus, both WIs and many traditional EBTs focus explicitly on modifying a shared set of adaptive beliefs that foster adaptive, personally valued behavior change.
However, other characteristics of WIs differentiate them from EBTs, which are generally designed for delivery by trained therapists in brick-and-mortar clinical settings. First, WIs appear to be designed as single-component interventions: Interventions that include a streamlined, focused activity to support adoption of a specific way of thinking or making attributions (for a more thorough description, see Yeager and Walton 2011). Accordingly, WIs tend to be extremely brief, including just one or a handful of sessions (Walton and Wilson 2018), whereas traditional youth-focused EBTs tend to teach multiple skills and strategies across many weekly sessions (sixteen, on average; see Weisz et al. 2018).Footnote 2,Footnote 3
Second, WIs have been described as explicitly focused on shifting participants’ beliefs in order to spur ‘recursive’ recovery processes, whereby shifts in key beliefs (namely, beliefs that improve senses of belongingness, understanding, and self-integrity) facilitate behavior change, which in turn reinforce initial, adaptive belief change—ultimately supporting long-term progress both cognitively and behaviorally (Yeager and Walton 2011). That is, the effects of WIs rely almost entirely on personally guided learning embedded in real-world experiences. Traditional youth-focused EBTs tend to include strategies addressing both beliefs and behaviors to support patterns of change (as in behavioral activation for depression, graded exposure therapy for anxiety, or behavior parent training), rather than focusing specifically and exclusively on changing beliefs. In EBTs, adaptive changes are reinforced largely through structured, therapist-guided practice in clinical settings.
Finally, WIs and traditional EBTs are structured and presented to participants in notably different ways. WIs are designed to be non-stigmatizing, unobtrusive (e.g., delivered via technology or lay providers in real-world contexts they regularly frequent, rather than separate, clinical settings), and relevant to youths with and without severe psychopathology (e.g., Schleider and Weisz 2016; Schleider and Weisz 2018a, b; Miu and Yeager 2015). Some WIs designed to address youth psychopathology never once mention “depression,” “conduct problems,” or “anxiety” to their participants (similar to other interventions designed for non-treatment-seeking populations), despite the relevance of the intervention’s targeted beliefs to each problem type. In contrast, clinic-based EBTs for youth psychopathology make clear reference to the problem or disorder being addressed, as most are designed for actively treatment-seeking populations.
In sum, WIs and EBTs aim to restore a shared set of beliefs (promoting a sense of belonging, self-integrity, and understanding); however, WIs routinely differ in length (typically briefer), presentation (as non-stigmatizing and non-specific to clinical populations), and focus (on a single belief or strategy, as opposed to many interconnected ones) versus traditional EBTs.
WIs for Youth Academic and Interpersonal Outcomes
Many of the above-mentioned differences between WIs and EBTs stem from the fact that, in large part, WIs are designed to address non-clinical social problems. To contextualize the promise of WIs applied to clinical youth problems and populations, we briefly summarize extant literature on the effects of three well-tested WIs—self-affirmation, mental contrasting with implementation intentions, and growth mindset (incremental theory) interventions—on academic and interpersonal outcomes in youth. (Note that multiple reviews have been written on each of these WIs and their impacts on academic and interpersonal outcomes in non-clinical youth populations; see Oettingen and Reininger 2016; Walton and Wilson 2018; (Sherman and Cohen 2014; Yeager and Dweck 2012) for comprehensive reviews).
Self-affirmation interventions give participants opportunities to assert their core values, especially when those values might be under threat (Cohen and Sherman 2014). These affirmations often involve brief writing sessions (as short as 10 min) where participants write about themselves in a way that affirms a positive, authentic sense of self (Sherman and Cohen 2006). These affirmations can be about large personal accomplishments, but even “small” affirmations can have outsized effects on participants if they are personally meaningful (Yeager and Walton 2011). These affirmations may in turn broaden participants’ attention beyond whatever current threat they are experiencing (e.g., being a person of color in an academic environment with white peers), see the threat as less relevant to who they are as a person (e.g., not attributing a bad grade to a deficient, less deserving academic self), and cultivating an approach orientation toward threat rather than avoidance (e.g., starting to look over the problems missed on the assignment so they have a better chance of performing better on the next assignment). These more adaptive behaviors may compound over time and improve outcomes long after the original intervention is completed (Miller et al. 2017).
Self-affirmation interventions can decrease the achievement gap between students of color and White students during their middle school years (Cohen et al. 2006, 2009; Sherman et al. 2013). There is evidence that the gap between Latinx students and White students remained narrower among the affirmed students 3 years later after the students entered high school (Sherman et al. 2013). These interventions narrowed the achievement gap by decreasing the rate at which grades decreased among minority students, not increasing their grades. This “slowing down” of a negative process is a feature of other wise interventions as well and could in principle be clinically useful, especially in prevention contexts (Walton 2014). Self-affirmation interventions have also lowered the achievement gap between first-generation college students and continuing generation college students in introductory science courses (Harackiewicz et al. 2014; Miyake et al. 2010). Self-affirmation interventions do not always produce significant treatment effects (Hanselman et al. 2017), implying that further investigation with different outcomes could help us better understand their boundary conditions.
Mental Contrasting with Implementation Intentions (MCII) is a self-regulation strategy designed to increase both goal commitment (via mental contrasting), and in turn, likelihood of goal implementation (through implementation intentions). In completing MCII, individuals first name their most important wish in a particular domain, such as academics (e.g., a wish to improve performance in math class). Second, participants imagine and elaborate the desired future of having successfully fully addressed this concern (e.g., increasing one’s math class grade). Lastly, they imagine and elaborate the primary obstacle in the way of realizing their wish (e.g., feeling discouraged when class material is challenging). By drawing the person’s attention to the fact that their strongest wish is unrealized, naming this obstacle is thought to activate expectations of success and motivation to pursue the desired future (Oettingen 2012). The latter portion of the exercise (implementation intentions) is designed to capitalize on this motivation, guiding individuals to devise an “if–then” plan regarding when, where, and how their goal intention (“I wish to do better in math class”) should be implemented (e.g., “if I feel discouraged because the material is challenging, then I will ask my mother or teacher for help with the assignment!”). This “implementation intention” is thought to strengthen readiness to take action toward a desired goal if and when the specified obstacle emerges (Achtziger et al. 2011; Webb and Sheeran 2007).
MCII has been adapted for self-administration via pen-and-paper or a publicly available mobile phone app (www.woopmylife.org, where the app-based activity is publicly available in multiple languages). It has also been adapted for delivery by trained interventionists in classroom settings for large groups of students (Duckworth et al. 2013). Research has shown beneficial effects of self- and interventionist-administered MCII interventions on youths’ academic persistence and behavior at school. In one RCT, tenth grade students who completed a brief MCII intervention completed more academic practice items over their summer break than did students who received an information-only control (Gollwitzer et al. 2011). Separately, fifth grade students who completed a classroom-based MCII exercise showed improvements in grades and school attendance relative to youths who received a ‘positive thinking’ control intervention (Duckworth et al. 2013). Youths with mental health challenges have also benefited from MCII: among children at high risk for ADHD, those who received an MCII intervention showed improvements in homework completion and organization at school compared to those who did not (Gawrilow et al. 2011, 2013). In another study, early college students who completed a brief MCII exercise about an important academic concern scheduled twice as many hours of their time for the upcoming week as participants who completed control exercises (Oettingen et al. 2015).
Growth Mindset (Incremental Theory) Interventions encourage participants to believe traits are malleable (growth mindset) rather than unchangeable (fixed mindset). Endorsing this growth mindset in turn may lead to greater effort, more help seeking, and better outcomes in important domains like interpersonal functioning and academics (Yeager and Dweck 2012). Notably, there is no uniform standard for what constitutes a mindset intervention, and interventions targeting mindsets of different types (e.g., mindsets with respect to intelligence versus mindsets with respect to personality) have notable differences both in their content and targets. Here, we will focus on mindset interventions targeting malleability beliefs about personality (i.e., personal traits such as shyness, sadness, and social skills), as these programs carry greater theoretical relevance to mental health outcomes than do mindset interventions targeting beliefs about intelligence (Schleider and Schroder 2018). In general, these programs are self-administered by youth, teach the “brain science” behind why it is possible for various personal qualities to change, contain testimonial quotes reinforcing the possibility of change from peers, and involve the completion of a “self-persuasion” exercise where youth write about how change is possible to help another youth who is struggling (Yeager et al. 2016b). These interventions are thought to remove a barrier for expanding effort in the face of difficulty and asking for help, especially for marginalized groups, following a Lewinian field theory principle that removing crucial barriers can facilitate success (Lewin 1944).
Growth mindset interventions targeting the malleability of personality in adolescents do appear to improve interpersonal functioning. For example, adolescents who receive a growth mindset of personality intervention compared to an active control encouraging sharing of feelings recover more quickly according to physiological markers following the Trier Social Stress Test (Schleider and Weisz 2016). Importantly, improvements in personality growth mindset were associated with faster recovery from social stress, indicating a plausible causal pathway between improvement in growth mindset and improvements in responses to social stress. These more adaptive responses to a laboratory social stress test following randomization to a growth mindset of personality condition compared to a control have also replicated in a separate sample (Yeager et al. 2016a). In a second sample within that study, youth who received the growth mindset of personality intervention compared to the control saw a decreased coupling of daily diary reported social stress and daily threat appraisals and physiological markers of stress. Therefore, youth in the growth mindset interventions respond more adaptively to social stress in the laboratory and in day to day life. Based on these initial studies, growth mindset of personality interventions has shown the potential for clinical utility.
WIs for Youth Psychopathology?
Given EBTs’ and WIs’ overlapping targets (core, maladaptive beliefs, and attributions), WIs might be harnessed to help address specific maladaptive beliefs underlying youth psychopathology. Indeed, WIs may be viewed as well-targeted, theoretically precise strategies to mitigate cognitive vulnerabilities (maladaptive beliefs or cognitive styles, as in the cognitive vulnerability-stress model of psychopathology: Beck 1967; Mathews and MacLeod 2005), thereby increasing adaptive coping and reducing hopelessness, aggression, and distress in the face of setbacks and stressors. WIs teaching growth mindset offer an example of this possibility. Youths holding fixed mindsets of personal traits and abilities (i.e., viewing those traits as inherently unchangeable; (Dweck 2008) tend to report higher levels of psychopathology (Schleider et al. 2015) and increased internalizing problems over time (Schleider and Weisz 2015; Romero et al. 2014). Indeed, fixed views of personal traits routinely lead to maladaptive attributions following social challenge: for instance, thinking “I must be a terrible person” after arguing with a friend, or “life will always be impossible” after experiencing a depressive episode (Schleider and Schroder 2018; Yeager and Dweck 2012). Youths with fixed mindsets are likely to perceive intra- and interpersonal stressors as indicative of permanent deficits or problems; those perceptions, in turn, foster feelings of helplessness, defeat, and maladaptive coping, all of which have been shown to underlie psychological symptoms and disorders (Abramson et al. 1990; Webb et al. 2012). Thus, holding fixed as opposed to growth mindsets may reflect a cognitive vulnerability for psychopathology in youth: one that WIs have been shown to mitigate. Thirty- to ninety-minute, computer-based WIs teaching adolescents that personal traits are malleable have prevented depression symptoms and improved well-being in non-clinical samples (Miu and Yeager 2015, OR .55, with the WI group showing lower odds of reporting clinically elevated levels of depression; (Smith et al. 2018), d = .11, with the WI group showing relative improvements in well-being at school) and reduced depression and anxiety symptoms in high-risk adolescent samples (Schleider and Weisz 2018a, b), all compared to active control interventions. Thus, growth mindset WIs, along with other WIs addressing different cognitive vulnerabilities, may represent well-targeted strategies for reducing distress in adolescents with varying levels of clinical need.
Pursuing this possibility may carry great practical value, given WIs’ high potential for disseminability. Indeed, WIs routinely meet the criteria for disseminable, novel psychosocial treatments described by Kazdin and Rabbitt (2013). They routinely hold potential to improve treatment reach (the capacity to reach individuals not usually served or well served by traditional service delivery models, given their brevity), are frequently scalable (they possess the capacity to be applied on a large scale or larger scale than traditional service delivery—e.g., through delivery to entire schools or classrooms simultaneously: Miu and Yeager 2015), are affordable (relatively low cost compared to that of the usual model, which relies on individual treatment by highly trained professionals, as in free online WIs: Oettingen and Reininger 2016), may help expansion the non-professional workforce (increases the number of providers who can deliver interventions, as in teacher-delivered WIs: Conrod et al. 2013); they may expand settings where interventions are provided [they may bring mental health interventions to locales and everyday settings where people in need are likely to participate or attend already, such as schools, (Halliwell and Diedrichs 2014), and personal mobile devices (Kauer et al. 2012)], and possess feasibility and flexibility of intervention delivery (capacity for interventions to be implemented and adapted to varied local conditions to reach diverse groups in need, as in multiple growth mindset intervention adaptations for unique populations: Schleider and Weisz 2016, 2018a, b; Miu and Yeager 2015; Smith et al. 2018). Based on these metrics (identified by Kazdin and Rabbitt 2013 and Kazdin 2018 as key indicators of interventions’ disseminability potential), when tailored to youth mental health needs, evidence-based WIs may dramatically expand the accessibility of mental health supports for the many youths who might not otherwise receive them, and perhaps improve the potency of those services for those who do.
Present Review
In sum, WIs have reduced youth psychopathology across several studies, and WIs may hold promise to expand the reach of youth mental health supports. However, no systematic review has investigated WIs’ effectiveness and promise for reducing and preventing youth mental health problems. Accordingly, the goal of this review is to better characterize the effectiveness of WIs for various types of youth psychopathology; identify where and how they have been effectively administered; the populations they have and have not benefited; and the qualities of WIs that may have helped or hindered their efficacy. By overviewing the types of and ways in which brief WIs have reduced psychopathology in youths to date, this review may offer a roadmap for testing the promise and place for WIs in the greater youth mental health ecosystem, whether as stand-alone programs, adjunctive treatments, or low cost, non-stigmatizing ‘boosters’ to maintain initial gains achieved in traditional EBTs.
Method
Search Strategy
We conducted searches in multiple bibliographic databases (PsychINFO, MEDLINE, Web of Science, Eric, ProQuest—Dissertations, PsyArXiv) as well as manual reviews of relevant literature (e.g., Walton and Wilson 2018; Schleider and Weisz 2017) to identify peer-reviewed randomized controlled trials and unpublished manuscripts describing the effects of WIs on youth psychopathology (date range: January 1, 2003 through September 1, 2018). Search terms including combinations of the following: child, adolescent, youth, pediatric, or parent, mother, or father; along with mental health, psychopathology, depression, anxiety, aggression, internalizing or externalizing; along with intervention, prevention, treatment, randomized trial, workshop, field trial, or training (to be as inclusive as possible of the ways in which “interventions” might be described across fields). As our goal was to be over-inclusive in the initial screening stage of potentially eligible studies, we also checked references of earlier reviews and contacted researchers conducting work in this domain to help ensure thoroughness. At the same time, to focus the scope of our review on WIs for psychopathology and clinical problems, we omitted search terms such as “well-being” and “happiness” in our search; such outcomes are of course important to consider in the context of overall youth development, but they were outside the scope of this review.
Inclusion and Exclusion Criteria
Criteria for study inclusion were as follows: (1) English-language articles; (2) mean youth age no older than 19.0 years; (3) youths (and/or caregivers) randomly assigned to a psychosocial (non-pharmacological) WI or a comparison condition, including no-treatment, waitlist, and “active” controls, such as attention-only, psychoeducation, or psychosocial placebo; (4) the RCT includes one or more intervention outcomes related to youth (not parent/caregiver) mental health or psychopathology, assessed at both pre- and post-intervention in the intervention and control groups (such trials were eligible for inclusion regardless of whether youth psychopathology was the primary intervention target); (5) trial was published in the past 15 years, given advances in technology that dramatically change the ways in which WIs can be developed and delivered; (6) the intervention being tested qualified as both a wise intervention and a brief intervention.
We determined whether an intervention qualified as “wise” and “brief” in the following three ways. First, the intervention must have been designed to alter youths’ and/or caregivers’ ways of making meaning about themselves and the social world, interpreting themselves and the social world, or their belief systems about themselves and the social world (e.g., understanding, belonging, self-integrity), per Walton and Wilson’s (2018) definition. Second, the intervention must be single-component by nature, as WIs are routinely characterized by their focus on a single message, skill, or strategy to promote adaptive meaning-making (Weisz et al. 2017a, b; Yeager and Walton 2011). Interventions teaching a cognitive skill or strategy along with one or more other skills or strategies, as is common in traditional cognitive-behavioral and behavioral parent training interventions, were therefore excluded from this review. Third, given our focus on wise interventions that are also scalable and have high potential for disseminability, we focused on interventions not exceeding 240-min or four 60-min sessions in length: i.e., interventions 75% shorter than traditional evidence-based treatments for youth psychopathology (Weisz et al. 2018).Footnote 4 Notably, “brief intervention” has been defined in myriad ways to date, from single-session interventions (Schleider and Weisz 2017) to those including eight or fewer sessions (i.e., 50% briefer than traditional youth therapies; Öst and Ollendick 2017). We defined “brief” wise interventions more moderately for the purposes of this review, based partly on the mean number of sessions (3.9, on average) that youth typically complete in real-world clinical settings prior to terminating services (Harpaz-Rotem et al. 2004).
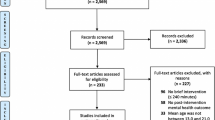
Figure 1 shows the study search and identification flowchart. Initial study selection (i.e., article screening) was conducted by the first author and 13 trained undergraduate and postgraduate research assistants. Specifically, abstracts were evaluated by two individuals on the research team according to whether they met the 4 of the 6 inclusion criteria outlined above (English-language article; youth age ≤ 19 years; randomized controlled trial; published in the previous 15 years). Rate of agreement across both raters for decisions to include versus exclude a study based on abstract review was 97.82%. Full texts were extracted for all articles generating disagreements between raters to minimize odds of missing relevant studies. At the second stage of review (after full texts were extracted), articles were coded by two reviewers each on the remaining two inclusion criteria: (1) the RCT includes one or more intervention outcomes related to youth (not parent/caregiver) mental health or psychopathology, assessed at both pre- and post-intervention in the intervention and control groups, and (2) the intervention being tested qualified as both a wise intervention and a brief intervention (compliance with the prior four criteria were double-checked, as well, as some features may not have been clear from abstracts alone). Specific study features guiding decisions to include versus exclude at this stage are detailed in Fig. 1 (e.g., “intervention was multi-component,” or taught multiple types of skills and strategies, which would indicate disqualification as a ‘Wise’ intervention). Across the 812 full-text articles screened, inter-rater agreement was 94.58% on decisions to include versus exclude in the review. The 38 remaining studies were discussed by members of the research team, including the first author. A majority of these studies were ultimately excluded for being multi-component interventions. Twenty-five were included in the review.

PRISMA diagram
Data Extraction, Coding, and Processing
Studies meeting inclusion criteria were coded for study and sample characteristics. These included study and intervention characteristics, and indices of WI effectiveness. Given the novelty of the present topic, diversity of mental health outcomes and intervention types, and relatively small number of studies eligible for inclusion, we conducted a descriptive systematic review as opposed to a quantitative meta-analysis, which would have posed substantial interpretation challenges. Characteristics of all 25 included studies are presented in Table 1. All studies were doubly coded by the first author and one of seven trained undergraduate or postgraduate research assistants. Disagreements were resolved via discussion and collaborative article review. Agreement on all coded variables was acceptable (for applicable variables, kappas = .76–1.0; ICCs = .81–.98). The manual used to guide coding, written by the first author, is enclosed as a supplement to this manuscript.
We coded each study’s year and publication status (peer-reviewed publication versus unpublished manuscript); sample type, including recruitment strategy (community versus clinic-referred sample); participant demographics including mean age, percentage of males versus females, and racial and ethnic identities; primary WI target (that is, was the WI designed to address academic outcomes, interpersonal outcomes, mental health, or substance use?); and type of mental health outcomes assessed in the RCT (oppositional behavior and aggression, anxiety, depression including suicidal ideation, eating problems, substance use, or general psychological distress, such as low self-esteem and hopelessness). We also included descriptions of the WI evaluated in each study, characterized each study’s comparison or control condition (treatment as usual; placebo; psychoeducation; no treatment), and coded RCT follow-up length (in weeks), number of participants assigned to each study’s WI and control conditions, along with retention rates by group at final follow-up; and the setting in which the WI was delivered (mental healthcare setting; school; general hospital; research lab; community center; or via technology/remotely). To characterize intervention intensity and potential for scalability, we coded each WI’s delivery format (therapist administered; self-administered; school staff administered), length (in total minutes, number of discrete sessions, and number of total weeks), training required for therapists to administer the intervention (in hours, for therapist-administered interventions only), and the reported availability of a given WI for public and/or therapist use.
To qualitatively gauge WIs’ promise in reducing youth psychopathology, we created brief summaries of each study’s results (paraphrasing authors’ reported results), describing the effects of WIs on all mental health outcomes assessed in a given RCT. We also coded the number of mental health outcomes assessed within each RCT, as well as whether each study’s WI exhibited any statistically significant, positive effect on a youth mental health-related outcome—and, if so, for which outcomes (anxiety; depression eating problems; generalized psychological distress; oppositional behavior; substance use)—compared to respective control conditions. Based on these codes, we characterized each type of WI identified in our review as being well-established, probably efficacious, possibly efficacious, experimental, or questionable for specific youth mental health outcomes, based on previously defined criteria that are commonly used within clinical psychological science (see Table 2, drawn from criteria created and refined by Chambless 1996a; Chambless and Hollon 1998; Chambless and Ollendick 2001; Huey and Polo 2008; Silverman and Hinshaw 2008; Southam-Gerow and Prinstein 2014). That is, we evaluated each WI on its efficacy in reducing a specific type of youth mental health outcome, resulting in multiple classifications for WIs that have been used for multiple youth problem types. Although this classification approach has previously noted shortcomings (see Huey and Polo 2008; Southam-Gerow and Prinstein 2014)—for instance, it focuses on a treatment’s overall effect and does not systematically account for potential moderators or contextual predictors of a treatment’s promise—we adopted it for two reasons. First, we sought to maintain consistency between this review and the broader clinical science literature. Second, the early state of the literature on WIs for youth psychopathology precluded our ability to conduct robust assessments of WIs’ effects on certain subgroups or in specific contexts. As such, our focus in this review is on overall effects of WIs on youth psychopathology as opposed to context-specific effects, which may be helpful to consider in future work, particularly as the literature grows.
We also coded whether each study’s WI addressed one or more of the three basic beliefs identified by Walton and Wilson (2018; beliefs promoting a sense of understanding, self-integrity, and belongingness) to examine whether interventions targeting particular domains were more likely to reduce psychopathology in youth. Finally, to assess possible study bias, we coded methodological quality variables used in previous systematic reviews of psychosocial RCTs and recommended by the Cochrane Consumers and Communication Review Group (Ryan 2013) that were reported with sufficient frequency and clarity to be applied across most studies. These variables were subject blindness to intervention condition by participants; personnel blindness to outcome assessments; and participant attrition (percentage of participants at randomization available at the final post-intervention assessment).
Results
Study Selection and Inclusion
Of the 4046 examined abstracts (3721 after excluding duplicate records), 812 full-text articles were retrieved for further consideration. Of these, 787 were excluded; reasons for exclusion are illustrated in Fig. 1. The 25 remaining studies (24 published articles, 1 unpublished dissertation) were coded in full by both the first author and a trained research assistant.
Characteristics of Included Studies
We identified a total of 25 RCTs of WIs published in the past 15 years that assessed at least one youth mental health outcome, which collectively included 9219 youths (Table 1). Across these RCTs, most of the WIs evaluated (n = 18) were explicitly designed to address mental health concerns in participants. Some were designed to target substance use (n = 4), interpersonal problems (n = 2), or academic outcomes (n = 1).
All of the included WI trials targeted pre-adolescents or adolescents (overall M age = 14.7, ranging from 11 to 19). Of the 25 included WI trials, 12 assessed effects on depressive symptoms (including suicidal ideation), 3 assessed anxiety and/or trauma symptoms, 6 assessed substance use, 3 assessed oppositional behavior or aggression, 8 assessed general psychological distress (e.g., self-esteem, hopelessness, negative self-perception, mental health-related quality of life, etc.), and 3 assessed disordered eating or body image problems (several studies assessed more than one mental health outcome, hence the total n > 25). None assessed problems related to attention or impulsivity/hyperactivity. The modal number of youth mental health outcomes assessed per RCT was 1 (mean = 1.92; range 1–5).
In 14 of the 25 included RCTs, WIs addressed more than one of the three core domains identified by Walton and Wilson (beliefs that foster a sense of belongingness, self-integrity, and understanding). In 11 RCTs, WIs addressed only one of these three domains, and in 5 RCTs, WIs appeared to address all 3 domains.
Twelve of the RCTs included clinical or high-risk samples, and 13 included community samples. More than half of the WIs were administered in school settings (n = 13); an additional three were administered in mental healthcare settings, one in a general hospital setting, four in laboratory settings, two in community centers, and two remotely, via technology (web-based or mobile phone delivered interventions). None of the WIs qualifying for inclusion in this review were directed toward parents or caregivers; generally, WIs that were caregiver-directed did not include youth mental health outcome assessments.
All WIs eligible for inclusion in this review were brief (four sessions or fewer), but they varied considerably in length and delivery format. Interventions ranged from 5 to 180 min (M = 71.5 min) and 1–4 sessions (M = 1.80), and 1–42 weeks (reflecting length of time elapsed between first and final session; M = 9.93, Median = 8). Thirteen were self-administered by youths and 12 were administered by trained therapists or school staff. Some form of pre-intervention therapist training was noted in 10 of the 12 studies in which therapist-administered WIs were assessed, although the amount of training required was unreported in all of these studies but two. In those two studies, therapists reportedly received 20–24 total hours of training prior to intervention delivery.
Risk of bias in included studies, here assessed based on intervention condition allocation concealment, was variable. In 11 of the included studies, participants were aware of their intervention condition or allocation concealment was not mentioned, and in 13 of the included studies, no mention was made as to whether assessors were aware of participants’ intervention condition assignments. Attrition at final follow-up assessment exceeded 20% in 10 of the 25 included studies; however, the total follow-up length varied considerably across RCTs, ranging from 0 weeks (immediately post-intervention) to 36 weeks in other studies.
Do WIs Improve Youth Mental Health?
WIs tested in 16 of the 25 RCTs showed a statistically significant, positive effect on one or more youth mental health outcomes, per authors’ reported results (effects of each WI on specific types of youth mental health outcomes are detailed in Table 3 and in-text, below). Eight RCTs showed no significant positive WI effects on any mental health outcome, and one RCT showed a significant iatrogenic WI effect on youth mental health.
Of the 16 WIs demonstrating one or more positive effects on youth mental health outcomes, 6 had no-treatment control groups, 5 had placebo or attention-only controls, 1 had a ‘treatment as usual’ control, and 4 had psychoeducation control groups; 7 were focused on clinic-referred or high-risk samples, and 9 on community samples; and the average follow-up length in these 16 RCTs was 15.81 weeks (range 0–36). Nine of these 16 RCTs took place in school settings, 2 were completed remotely via technology, 2 were completed in laboratory settings, and 1 each were completed in mental healthcare, general hospital, and community center settings. On average, these sixteen WIs lasted 92.69 min each (range 30–180 min) across 1.88 sessions (range 1–4 sessions; 75% 1–2 sessions) and took an average of 8.20 weeks to administer (range 1–28). Half (8 of 16) of these WIs were self-administered by individual youths, with the remaining eight administered by professional therapists, non-professional interventionists, or school staff, typically in group settings.
Which WIs Improved Youth Mental Health?
Because some WIs (or versions of a given WI) were tested in multiple RCTs, seven types of WIs met criteria for being “well-established,” “probably efficacious,” or “possibly efficacious” in reducing youth psychopathology of one or more types (either at the symptom level or the disorder level, as RCTs included in this review test WIs as both preventive interventions and treatments). Effects of each intervention on specific youth mental health outcomes, and their characterization as well-established, probably or possibly efficacious, experimental or questionable for specific mental health outcomes, are detailed in Table 3.
Interventions teaching growth mindset, or incremental theories of personal attributes, were the only WI type to qualify as “Well-Established” for reducing youth depressionFootnote 5 and “Probably Efficacious” for anxiety and general psychological distress. These WIs which ranged from one to two sessions and 30 to 90 min in length were self-administered by adolescents via computers or paper, and delivered in school or laboratory settings. They used principles from brain science and testimonials from peers to impart the belief that personal attributes are malleable rather than fixed. Additionally, these interventions include writing exercises (e.g., ‘saying-is-believing’ activities, wherein teens write letters to younger peers explaining how and why personal traits can change) to facilitate internalization of the interventions’ primary message. In RCTs utilizing active, psychosocial placebo-controlled conditions, these WIs reduced youth depressive symptoms in both RCTs in which it was assessed as an outcome; youth anxiety symptoms in the one RCT in which it was assessed as an outcome; and well-being at school in the one RCT in which it was assessed as an outcome.
WIs utilizing cognitive dissonance-based activities, assessed in four RCTs, qualified as “Probably Efficacious” for youth depression and eating-related problems and “Possibly Efficacious” for general psychological distress. These WIs were either classroom based and led by trained therapists or teachers (3 of 4 RCTs) or self-administered via a computer activity (1 of 4 RCTs) and ranged from one 90-min session to four 20-min sessions. The WIs varied in specific content but were generally designed to increase youths’ awareness of appearance comparisons (the act of comparing one’s own appearance to that of peers or media images); to teach youths about humans’ natural biases toward making ‘upward comparisons’ (comparing the self to others perceived as superior in some way), which can lead to negative self-talk and self-dislike; and to guide youths through exercise teaching youths to identify and challenge appearance comparisons when they occur.
Five additional WIs qualified as “Probably” or “Possibly Efficacious” based on the results of one RCT each. For instance, mental contrasting with implementation intentions qualified as “Probably Efficacious” for reducing oppositional behavior in youth. In this therapist-administered, classroom-based, two-session WI, trained interventionists (who had received training in the WI protocol, but not as professional therapists) guided non-referred students through a structured exercise in which youths were led to identify a wish related to academic progress at school; their primary obstacle to achieving their wish, including where and when they were likely to encounter that obstacle; a strategy to overcome that obstacle; and a plan to implement that strategy in their everyday life, using an “if…, then…” template (if obstacle occurs, then I will engage in plan/action). That is, youths were taught to create an “implementation intention” and to rehearse this plan independently to build their belief that they can (and are likely to) take action toward a personal goal. This WI reduced youth oppositional behavior at school relative to the control intervention (a “positive thinking” activity).
Other “Probably Efficacious” WIs included a self-awareness intervention, a problem-orientation discussion intervention, and a personality-targeted cognitive restructuring intervention. In the self-administered, mobile phone-based self-awareness intervention, high-symptom youths self-monitored and recorded the type and intensity of their moods, the stressors they encountered, their reactions to those stressors, and their sleep, substance use, and other daily activities three times per day for 2–4 weeks (approximately 6 min per day; 84–168 min total). Youths received individualized summaries of their own self-report data, which highlighted associations between daily activities, stress, and mood. Youths who completed this intervention reported greater decreases in depressive symptoms than did youths who self-monitored only their sleep and daily activities via mobile phone technology.
The brief problem-orientation intervention consisted of a brief (35-minute) video, delivered to youth experiencing suicidal ideation. The video was designed to teach youths that everyday problems, such as feelings of anhedonia, sadness, or difficulty making friends, are identifiable and solvable through personal effort. The video walks through a CBT-based strategy for identifying and generating solutions for common intra- and interpersonal difficulties that may relate to depression. Youths in the intervention group reported significantly larger short-term declines in depressive symptoms and suicidal ideation relative to youths in an attention-only comparison group.
The personality-targeted cognitive restructuring intervention was delivered by school staff (including teachers and counselors) who completed a 2- to 3-day training in order to administer the program. This two-session classroom-based program was delivered to groups of students, and content differed based on students’ previously identified areas of difficulty (e.g., elevations in impulsivity, anxiety sensitivity, excessive sensation-seeking, or hopelessness). Facilitators taught youths to identify and challenge personality-specific cognitive distortions and were encouraged to identify and challenge personality-specific cognitive distortions that may lead to personality-specific problem behaviors (e.g., panic or avoidance in the case of anxiety sensitivity or aggression in the case of impulsivity), relating cognitive restructuring strategies to avoiding substance use. Youths who completed this intervention, relative to youths in an educational comparison program, reported less alcohol use during and following the trial.
An additional “Possibly Efficacious” WI for depressive symptoms was a brief, solution-focused discussion intervention, which consisted of up to one hour of web-based chat sessions with a trained therapist; chats were initiated by high-symptom youth participants. During chat sessions, the therapist asks youths to imagine a future in which their present problems are no longer present, guiding the youth to imagine and describe steps she might take toward achieving such a future. Youths determined when chat sessions would end (or whether an additional brief web-based chat would be scheduled) based on whether the youth perceived her progress toward a stated goal has been met. Compared to youths in a no-treatment control group, youths in the WI group reported significant reductions in symptoms of depression.
Notably, the full contents of most of these WIs were not clearly accessible to others for use in other contexts, with the exception of versions of the growth mindset WI (Smith et al. 2018—available via Open Science Framework; Schleider and Weisz 2018a, b—available from authors upon request), mental contrasting with implementation intentions (Duckworth et al. 2013; see www.woopmylife.org), and one WI that qualified as Questionable in efficacy for general distress and aggression, a values-affirmation WI (Thomaes et al. 2012; WI procedure fully detailed in-text).
WI Effects on Specific Youth Symptom Types
Among RCTs that assessed WI effects on youth depression (n = 12), 8 showed positive effects on those symptoms and 4 showed non-significant effects. The eight RCTs showing positive effects on depression included those evaluating growth mindset interventions (in 2 of 2 RCTs; met “Well-Established” criteria for depression), the self-monitoring intervention (in 1 of 1 RCT; met “Probably Efficacious” criteria for depression), cognitive dissonance interventionsFootnote 6 (in 2 out of 2 RCTs; met “Probably Efficacious” criteria for depression), a brief solution-focused discussion intervention (in 1 of 1; met “Possibly Efficacious” criteria for depression), a problem-orientation intervention (in 1 of 1 RCT; met “Probably Efficacious” criteria for depression), and a cognitive bias modification (in 1 of 3 RCTs; met “Experimental” criteria for depression). Interventions that did not influence depressive symptoms included self- or values-affirmation interventions and an intervention designed to normalize post-trauma cognitions.
Among RCTs that assessed WI effects on alcohol or drug use (n = 6), 3 showed positive effects on those symptoms. These were a motivational interviewing intervention (in 2 of 4 RCTs; met “Experimental” criteria for substance use) and a personality-targeted cognitive restructuring intervention (in 1 of 1 RCT; met “Probably Efficacious” criteria for substance use). Interventions that did not influence substance use included a social norms intervention, and in 2 of 4 RCTs, motivational interviewing activities.
Among RCTs that assessed WI effects on anxiety or trauma symptoms (n = 3), only one, a growth mindset intervention (1 of 1 RCT; met “Probably Efficacious” criteria for anxiety), showed positive effects on those symptoms. Interventions that did not influence anxiety symptoms included cognitive bias modification and an intervention designed to normalize post-trauma cognitions.
Among RCTs that assessed WI effects on oppositional behavior or aggression (n = 2), only one, mental contrasting with implementation intentions, showed significant, positive effects on those symptoms (1 of 1 RCT; met “Probably Efficacious” criteria for oppositional behavior). In another RCT, a values-affirmation intervention showed no significant overall effects on aggressive behavior.
Among RCTs that assessed WI effects on disordered eating or body image (n = 3), all three showed positive effects on those symptoms. Each of these WIs was a cognitive dissonance-based intervention delivered in groups by trained therapists (met “Probably Efficacious” criteria for eating or body image problems).
Among RCTs that assessed WI effects on general psychological distress (n = 8), 5 showed positive effects on those symptoms across 5 different RCTs. These were a growth mindset intervention, a cognitive dissonance intervention, and a self-awareness intervention (all of which met “Probably Efficacious” criteria for general psychological distress), as well as a motional interviewing intervention (1 of 2 RCTs; met “Experimental” criteria for general psychological distress), and an intervention designed to normalize post-trauma cognitions (because this WI failed to produce significant reductions in symptoms anxiety, trauma, or depression, we did not classify this WI as efficacious). Interventions that did not significantly improve psychological distress were a values-affirmation intervention and a targeted advertisement exposure intervention (this WI produced increases in general distress and is detailed below).
What Characterized WIs that Did Not Improve Youth Mental Health?
Of the eight RCTs in which WIs showed no overall effects on youth mental health outcomes, one had a no-treatment control, 4 had placebo or attention-only controls, and 3 had a ‘treatment as usual’ controls; 5 were focused on clinic-referred or high-risk samples, and 3 on community samples; their mean follow-up length was 4.78 weeks (range 0–12); 3 RCTs took place in school settings, 2 were conducted in laboratory settings, 2 were conducted in mental healthcare settings, and 1 was conducted in a community center. Two were cognitive bias modification interventions targeting mood difficulties and depression, one was a social norm-based intervention targeting substance use, three were self- or values-affirmation interventions targeting oppositional behavior, aggression, and depression, and two were motivational interviewing-based interventions targeting substance use or general psychological distress. Four of these interventions were administered by therapists, and four were self-administered. On average, these eight interventions lasted 45.38 min each (range 5–120 min) across 1.67 sessions (range 1–4 sessions; 87.5% 1–2 sessions), and took an average of 14.5 weeks to administer (range 1–42).
One WI demonstrated an iatrogenic effect, predicting increases in youths’ self-reported maladaptive coping at post-intervention compared to a psychoeducation control (Klimes-Dougan et al. 2009). This single-session, therapist-guided WI, delivered to youths individually, involved viewing a mock billboard advertisement about the importance of seeking treatment for depression and suicidal thoughts, and immediately afterwards, administration of a mental imagery activity related to the billboard advertisement.
Discussion
Effect sizes for youth mental health interventions have failed to significantly improve in the past 50 years, and in fact have decreased significantly for some problem types (depression and conduct problems; Weisz et al. 2018) creating a need for innovative, potent strategies for reducing symptoms and disorders. Social–psychological wise interventions (WIs) may help fill the pressing need for novel approaches to reducing youth psychopathology using innovative delivery systems and designs. To gauge this possibility, we conducted the first systematic, descriptive review characterizing the promise of WIs for mental health problems in youth. Across 25 RCTs, collectively representing 9219 youths and testing 13 types of WIs, 7 types across 12 RCTs qualified as “Well-Established,” “Probably Efficacious,” or “Possibly Efficacious” in reducing or preventing one or more types of youth psychopathology; 2 types of WIs across 7 RCTs, as “Experimental” in efficacy; and 4 types of WIs across 6 RCTs, as “Questionable” in efficacy. Among the 7 types of WIs identified as well-established or probably/possibly efficacious, 5 showed promise in reducing youth depressive symptoms or suicidal ideation, 3 in reducing general psychological distress, and 1 each in reducing eating or body image problems, anxiety, and substance use. Three of these WIs were self-administered by youths, four were delivered by school staff or trained therapists, and overall, they ranged from 30 to 168 min in length and targeted clinic-referred, high-risk, and community youth samples. Overall, these findings suggest that certain WIs have shown promise in reducing youth psychopathology—and these WIs may be brief, low cost, and require minimal or no therapist training. Some may be deliverable across a wide range of settings, with benefits across a wide range of mental health problems, from mild (e.g., general distress) to severe (suicidal ideation). WIs may therefore represent beneficial additions to the youth mental healthcare ecosystem. Below, we highlight takeaways and questions raised by the present review; priorities for future research evaluating WIs for youth psychopathology; and propose strategies for further evaluation, adaptation, and integration of evidence-based WIs in real-world settings.
Together, the patterns observed here add to a growing body of literature showing the possible benefits of brief, and in some cases self-administered interventions for psychopathology in youth (for reviews, see Schleider and Weisz 2017; Öst and Ollendick 2017). This review in particular suggests that single-component interventions—those focused on instilling just one skill, thinking style, or belief system in its participants—can affect meaningful change for certain youth mental health problem types. Indeed, the notion that single- and multi-component interventions can both yield meaningful, positive outcomes has been demonstrated in other fields. In a meta-analysis of 213 social–emotional learning programs including 270,034 kindergartens through high school-aged students, multi-component programs were no more effective than single-component programs in improving teachers’ attitudes, or students’ academic or social outcomes (Durlak et al. 2011). Separately, an overview of 25 systematic reviews yielded no evidence that multifaceted interventions were more effective than single-component interventions in changing behaviors in medical healthcare professionals (e.g., interventions designed to increase evidence-based practices, such as reducing antibiotics prescriptions or adherence to hand hygiene guidelines; Durlak et al. 2011; Squires et al. 2014). This, if appropriately targeted to specific clinical challenges, streamlined, brief, and single-component interventions hold potential to improve a wide range of outcomes, including mental health in youth. The relative and combined efficacy of single- versus multi-component interventions for particular types of youth psychopathology, and the possible cost-effectiveness of single-component interventions such as WIs, remain largely unexplored areas within intervention science research, and thus may be prioritized in RCTs moving forward.
Among WIs that were well established or potentially efficacious, more WIs showed promise in preventing or reducing youth depression than any other youth problem type. This is striking, as up to 65% of adolescents who receive cognitive-behavioral depression treatment fail to respond (March et al. 2007) and interventions for youth depression have shown substantially smaller effect sizes than interventions for other types of youth psychopathology (for full-length EBTs, meta-analytic gs = .29 for depression, .62 for anxiety, .46 for conduct, and .34 for ADHD, Weisz et al. 2018; for single-session interventions, mean gs = .21 for depression, .56 for anxiety, and .54 for conduct problems, Schleider and Weisz 2017). WIs in this review were successful in reducing depressive symptoms in both community and clinical samples, via self-administered interventions (Fitzpatrick et al. 2005; Kauer et al. 2012; Miu and Yeager 2015; Schleider and Weisz 2018a, b), and in both prevention (Miu and Yeager 2015) and treatment contexts, including for youth experiencing active suicidal ideation (Fitzpatrick et al. 2005). Notably, a larger body of literature on WIs for mental health will be needed in order to directly compare the magnitude of effects of WIs and traditional interventions. However, the present review does suggest that several WIs may help reduce mild, moderate, and severe symptoms of adolescent depression to some degree. There are several possible reasons for this promising pattern. For example, self-administered WIs may help strengthen participants’ sense of agency and perceived control, which are often low and linked to increased hopelessness in youths experiencing depression. This may be especially true for WIs that explicitly place youths in an active, “helper” role (as in saying-is-believing exercises within growth mindset interventions: see Miu and Yeager 2015, and Schleider and Weisz 2018a, b) and WIs in which youths choose when and where activities are completed (as in self-monitoring WIs; Kauer et al. 2012). Indeed, larger immediate increases in perceived control following a growth mindset WI predicted larger subsequent reductions in adolescent depression and anxiety symptoms, suggesting that early shifts in agency may help explain this WI’s effects (Schleider et al 2019).
Results of this review also revealed gaps in the literature on WIs for youth psychopathology, which may explain certain patterns of results that emerged. All of the WIs in this review were evaluated on pre-adolescent or adolescent samples and few targeted externalizing psychopathology (WI effects on oppositional behavior were assessed in only two RCTs, and impulsivity and hyperactivity were assessed in none). The studies’ focus on adolescents may help explain why WIs emerged as most promising for depression, eating problems, and substance use, which all typically emerge (and are thus more often assessed) during adolescence. In contrast, externalizing problems tend to emerge earlier in development; most RCTs testing interventions for ADHD and oppositional behavior have focused on pre-adolescent children (Weisz et al. 2017a, b). The lack of evidence supporting WIs for externalizing problems and younger children may not reflect a lack of potential but rather gaps in the literature to date. For instance, compared to an active control intervention, mental contrasting with implementation intentions (MCII) has improved organization of school materials and homework completion in youths of ages 11–13 with elevated ADHD symptoms (Gawrilow et al. 2013). Although no mental health outcomes were assessed in this study, results suggest that MCII may promote adaptive behavior change youths at risk for ADHD. Separately, evidence-based cognitive-behavioral therapies are routinely adapted for elementary school-aged populations, despite complex content (e.g., teaching youths about cognitive distortions and restructuring or problem-solving; see, as examples Weisz et al. 2012, 2017a). Thus, exploring the promise of MCII and other WIs to reduce youth externalizing problems, and diverse types of psychopathology in younger populations, remains a priority for future research.
Another gap highlighted by this review was the lack of parent-directed WIs designed to reduce psychopathology in youth. In some respects, it is unsurprising that WIs have been largely youth-directed they are designed to alter guiding cognitions and meaning-making processes, which are subjectively held by youths themselves. However, it is possible that using WIs to promote adaptive belief change in parents’ could exert downstream effects on youth mental health outcomes. For example, parents’ expectancies and attitudes toward youth psychotherapy can influence whether their offspring access, engage in, and benefit from psychotherapy (see Acri et al. 2017; Chacko et al. 2014, 2016). In fact, a recent study found that WIs may help instill more positive psychotherapy expectancies in caregivers. In an RCT with a psychoeducational control, Schleider and Weisz (2018a, b) found that a 15-min, online intervention for parents—which taught growth mindset of emotion, along with the notion that failures and setbacks are enhancing rather than debilitating—improved parents’ optimism that psychotherapy could be effective, both for themselves and their children. Neither treatment-seeking behaviors nor youth mental health problems were assessed as outcomes in this study (hence its exclusion from the present review). Nonetheless, its results raise the possibility that targeting parents’ beliefs via WIs might support youths’ likelihood of accessing, completing, longer-term treatment, which future trials may investigate directly.
Alongside WIs’ positive effects, it is notable that several WIs showed null or even iatrogenic effects on youth mental health outcomes. Effective and ineffective WIs did not show apparent differences in the types of psychopathology they addressed, the settings in which they were administered, or their delivery systems (self- versus therapist administered); WIs identified as both helpful and unhelpful varied widely along all of these dimensions. However, certain types of WIs, such as cognitive interpretation and cognitive bias modification, showed limited or mixed efficacy across multiple studies, suggesting that certain approaches may have limitations in influencing youth mental health outcomes (the broader literature on CBM for youths and adults, including multi-session CBM and CBM combined with other therapeutic approaches, is similarly mixed: Jones and Sharpe 2017; Krebs et al. 2018). However, several WIs that did not significantly influence youth psychopathology were evaluated in just one study, in a single context, as stand-alone interventions. It remains possible that some of these strategies may prove useful as adjunctive supports, or in reducing types of youth symptoms not assessed in the RCTs in this review.
How much context matters for the success of WIs targeting psychopathology remains an open question that will be critical to explore in future work. Indeed, a shortcoming of the efficacy-classification system used in this review—which has been used in many reviews of clinical treatments to date—is its focus on overall rather than context-specific treatment effects in evaluating a program’s utility. The current theories undergirding many WIs imply some conditions under which interventions would be more and less likely to be successful (Bryan et al. 2016; Sherman and Cohen 2014; Yeager and Dweck 2012). However, these theoretically derived moderators do not always have the expected influence on intervention effects (Hanselman et al. 2017). For example, Hanselman et al. (2017) conducted 17 separate, theoretically informed analyses and found no evidence for any of the theoretically predicted contextual effects on a self-affirmation intervention targeting academic performance. Testing the overall effects of contextual moderators in this sample is not possible due to the relatively low sample size of 25 studies; however, it is important to note that one study included in this review found that a self-affirmation WI significantly reduced aggression in a specific subgroup of youth—those who simultaneously displayed low state self-esteem and high narcissism at baseline—but did not significantly reduce aggression overall in the study’s sample, relative to an active control (N = 405; Thomaes et al. 2009). By pre-registering theoretically driven predictions about context-driven intervention effects, and recruiting large samples to enable well-powered tests of those predictions, future studies and replications may reveal circumstances under which certain WIs may hold more promise for reducing youth psychopathology than overall effect sizes reveal. Indeed, WIs targeting psychopathology—especially those that are brief and self-administered, like the self-affirmation program noted above—offer the possibility of collecting much larger sample sizes than are typical for traditional treatment trials (Cuijpers et al. 2018). The potential scalability of WIs could therefore facilitate well-powered tests of theoretically derived moderators of clinical outcomes. These tests could advance WI theory and allow for well-powered tests of contextual factors derived from clinical science. Pre-registration of the specific analytic plans to define and test these contextual moderators would also allow the field to better distinguish between signal (context-specific effects) and noise (Meehl 1990). Determining how, when, and for whom interventions work best is a crucial step toward improving mental health (Ng and Weisz 2016).
Limitations
More than 300 trials of WIs have been conducted to date, with over 100 focused on youth populations (Walton and Wilson 2018). However, psychopathology-related outcomes have been assessed in a minority of these studies. This suggests that mental health outcomes are rarely assessed in trials of youth-focused WIs not explicitly designed to reduce emotional or behavioral problems; it also creates inherent limitations to the present review. For instance, due to the diversity of mental health outcomes and WI types across the RCTs and relatively small number of included studies, we were unable to conduct a quantitative meta-analysis of WIs’ effects on youth mental health. We therefore could not directly compare effect sizes of WIs to those of traditional EBTs for youth mental health, which would be a helpful direction for future research. Additionally, there are many interaction effects that might help explain where, for whom, and to what degree certain WIs might reduce youth psychopathology. Some WIs may be especially potent for clinic-referred youth samples when delivered in certain ways (e.g., by a trained therapist as opposed to self-administration). For instance, self-administered WIs might potentially yield greater effects on youth internalizing than externalizing psychopathology, as youth with oppositional behavior may benefit from added structure provided by a therapist. Alternatively, specific WIs (growth mindset interventions; MCII) may be more effective for certain forms of youth psychopathology than others, or for youths at specific developmental stages (e.g., adolescence versus younger childhood). Beyond these interactions, the overall promise of parent-directed WIs and WIs for younger children remains largely untested. As mental health outcomes are included in more WI trials, and novel WIs are developed specifically for clinical populations, these and related questions will grow increasingly addressable.
Future Directions
This review suggests multiple ways in which WIs might be incorporated into the youth mental health system across traditional and non-traditional treatment settings. These avenues may provide opportunities to simultaneously evaluate the acceptability of administering WIs via diverse modalities for multiple populations and settings, along with the efficacy of particular WIs in improving myriad mental health outcomes.
In traditional, clinic-based treatment settings, WIs may be evaluated as adjunctive or supportive interventions to enhance longer-term, multi-component EBTs and systems of care. There is some evidence that WIs can augment optimism about the effectiveness of psychotherapy (Schleider and Weisz 2018a, b) and increase readiness to change maladaptive behaviors (e.g., drinking in at-risk adults, Wittleder et al. 2019; and engagement physical activity among chronic pain patients, Christiansen et al. 2010). Additionally, studies have shown adults who endorse beliefs that WIs are designed to instill—such as malleability beliefs (growth mindsets) about anxiety and emotion—may strengthen likelihood of pursuing mental health treatment (Schroder et al. 2014) and predict larger symptom reductions following cognitive-behavioral therapy (Schroder et al. 2018). As such, by instilling the notion that personal change is possible or strengthening commitment to engaging in behavior change, administering WIs at or near the start of full-length EBTs might strengthen youths’ and parents’ motivation, engagement, or clinical response to treatment. However, these possibilities have yet to be tested in youth populations, suggesting a promising path for future research.
WIs may also be evaluated as interim interventions for parents and youths on waitlists for psychotherapy. Youth with mental health problems and their families encounter significant variability in wait times for psychological treatment, with some facing waits of several months or years (Kowalewski et al. 2011; Reid and Brown 2008; Smith and Hadorn 2002). Excessive wait times may exacerbate risk for suicide or hospitalization (Williams et al. 2008), and longer waits predict reduced odds of families attending future appointments (Sherman et al. 2009). Thus, administering WIs to youths and parents facing extended waits before treatment may help protect against clinical deterioration prior to therapy, or even help reduce levels of youth symptomatology as stand-alone interventions. They may also increase and help maintain motivation for attending treatment later on (e.g., by using MCII to strengthen intentions to pursue therapy once the wait is over). WIs have yet to be tested in these ways, but given the ubiquitous nature of waitlists in youth mental health clinics and the possible consequences of delaying intervention, WIs (and especially self-administered WIs, which require limited personnel to administer) may serve as a low-cost strategy worthy of formal investigation.
WIs may also be incorporated in less traditional settings to help improve broad accessibility to youth mental health supports. Primary care (PC) may represent one such opportunity. For instance, in 2018, the American Academy of Pediatrics released updated practice guidelines promoting screening of youth depression in PC clinics across the country (Zuckerbrot et al. 2018). This represents a critical step toward increasing early depression detection; however, the challenge of bridging screening with service delivery remains. Even when diagnosed by PC providers, less than half of youth with elevated depression access treatment of any kind (Zuckerbrot et al. 2018). Thus, there is a need for youth depression interventions that are more feasible for youths and parents to access and complete—and that may also strengthen parents’ likelihood of pursuing additional, longer-term services for their child in the future. If paired with PC-based mental health screening (e.g., by offering WIs via tablets, smartphones, or laptops to youths screening who screen high on depression symptoms at annual visits), self-administered WIs may hold potential to address this need. Future RCTs may address this possibility directly.
Schools offer another logical setting for delivering student-administered WIs, and in fact, this strategy was used in several RCTs included in this review. Delivering WIs in schools, particularly as universal classroom-based interventions, has the added benefit of serving as relatively non-stigmatizing form of intervention, consistent with how WIs are already structured. Some WIs may also serve as easily-administered Tier 2 interventions for youths with identified emotional or behavioral needs, although this possibility is untested as of yet. Finally, self-administered technology-based WIs raise the prospect of disseminating WIs via app-based programs, completable at home. There are multiple potential challenges to this dissemination strategy, including questions regarding WI compliance and youths’ motivation to complete interventions fully independently. Nonetheless, certain WIs may potentially offer scientifically validated alternatives to the many untested app-based programs claiming mental health benefits that have proliferated in recent years (Chandrashekar 2018).
Better understanding how and for whom wise interventions are most effective could be a boon to research across all of these potential delivery contexts. Future pre-registered, contextual-focused research will allow researchers and treatment providers to better understand which youth could be helped by these brief, cost-effective interventions. Better understanding treatment mechanisms for specific wise interventions and taking a prediction-focused approach to who responds best to certain interventions (Yarkoni and Westfall 2017) could both also contribute to better matching youth with appropriate WIs.
In summary, certain WIs have shown promise in reducing and preventing mental health problems in youth. More specifically, one or more WIs showed promise in reducing youth depressive symptoms, general psychological distress, eating problems, substance use, and youth conduct problems; effective WIs were brief, were designed for clinical and community settings alike, and were variably administered by trained therapists or youths themselves. Although their efficacy relative to traditional EBTs remains unclear, their high potential for disseminability and low cost relative to full-length treatments could produce public health benefit, particularly if delivered on a large scale. Future research should continue to evaluate the limits of WIs for youth mental health (including possible iatrogenic effects, as in Klimes-Dougan et al. 2009) as well as their capacity to help reduce youth psychopathology as stand-alone and adjunctive forms or support.
Notes
In this review, we focus on WIs that have been evaluated as brief, stand-alone interventions for reducing symptoms of psychopathology in youth. Initially, we had also intended to evaluate extant evidence on WIs as adjunctive interventions to foster engagement and retention in traditional EBTs. However, we found no existing RCTs that combined traditional EBTs with adjunctive WIs. We were able to identify one trial evaluating the effects of WIs on parents’ attitudes toward youth mental health treatment (Schleider and Weisz 2018a, b); however, this trial did not evaluate WI effects on youth mental health and was thus excluded from our review. Additionally, some of the RCTs included in this review assessed WI effects on youths’ knowledge of mental health problems and motivation for treatment (Bailey et al. 2004; Klimes-Dougan et al. 2009). We therefore discuss the promise of using WIs as adjunctive interventions in the discussion section of this manuscript, although this possibility has yet to be tested empirically.
WIs may intersect in notable ways with components of EBTs for youth psychopathology. Embry and Biglan (2008) define evidence-based “kernels” as "fundamental units of behavioral influence that underlie effective prevention and treatment." From our perspective, WIs may be understood as a specific type or sub-category of kernels, which share defining features of their own. For instance, unlike many other kernels, WIs are generally designed and evaluated as stand-alone interventions (although we also suggest how WIs might complement multi-component EBTs for youth mental health problems).
Notably, brief and even single-session interventions (SSIs) have shown promise in reducing youth psychopathology of multiple types; see Schleider and Weisz 2017, for a meta-analysis of SSIs for youth psychopathology. However, not all SSIs qualify as WIs, due to the criteria noted in this section.
13 studies in this review were excluded on the basis of intervention length. However, of these 13 interventions, only 4 would have been excluded based on intervention length alone. More commonly, these studies would have qualified for exclusion based on failure to meet other criteria, regardless of whether the intervention length criteria had been in place. (For instance, interventions containing more than five sessions tended to also teach more than one skill or strategy, violating the ‘single-component’ criterion.).
In this paper, our characterization of WIs as “Well-Established,” “Probably Effective,” “Possibly Effective,” “Experimental,” or “Questionable” references each WI type’s demonstrated capacity to reduce levels of symptoms or a disorder of a specific type.
Cognitive dissonance-based programs are based on the counter-attitudinal advocacy paradigm studied extensively in the field of persuasion (Brehm & Cohen, 1962). In this paradigm, participants are induced to advocate (via writing exercises, typically) for a topic inconsistent with their initial beliefs; because humans are motivated to maintain consistency with their attitudes and behaviors, this paradigm theoretically generates cognitive dissonance, facilitating attenuation of those initial beliefs. In programs targeting clinical problems, such as eating disorders, dissonance activities are used to induce critiques of the “thin ideal” in verbal, written, and behavioral exercises (e.g., write a letter about the costs of pursuing this ideal; Halliwell & Dietrichs, 2014). Critiquing the thin ideal theoretically prompts participants to reduce their belief to this ideal, which is thought to decrease body dissatisfaction, negative affect, and disordered eating behaviors.
References
Abramson, L. Y., Alloy, L. B., & Dykman, B. M. (1990). Cognitive theory and therapy of emotional disorders: A lay epistemic reconstruction? Psychological Inquiry,1(3), 198–200.
Achtziger, A., Bayer, U. C., & Gollwitzer, P. M. (2011). Committing to implementation intentions: Attention and memory effects for selected situational cues. Motivation and Emotion,36(3), 287–300.
Acri, M., Hooley, C. D., Richardson, N., & Moaba, L. B. (2017). Peer models in mental health for caregivers and families. Community Mental Health Journal,53(2), 241–249.
Baer, J. S., Garrett, S. B., Beadnell, B., Wells, E. A., & Peterson, P. L. (2007). Brief motivational intervention with homeless adolescents: Evaluating effects on substance use and service utilization. Psychology of Addictive Behaviors,21(4), 582.
Bailey, K., Baker, A., Webster, R., & Lewin, T. (2004). Pilot randomized controlled trial of a brief alcohol intervention group for adolescents. Drug and Alcohol Review,23(2), 157–166.
Bannink, R., Broeren, S., Joosten-van Zwanenburg, E., van As, E., van de Looij-Jansen, P., & Raat, H. (2014). Effectiveness of a web-based tailored intervention (E-health4Uth) and consultation to promote adolescents’ health: Randomized controlled trial. Journal of Medical Internet Research,16(5), e143.
Beck, A. T. (1967). Depression: Clinical, experimental, and theoretical aspects. Philadelphia, PA: University of Pennsylvania Press.
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry,165(8), 969–977.
Brehm, J. W., & Cohen, A. R. (1962). Explorations in cognitive dissonance. Hoboken: Wiley.
Bryan, C. J., Walton, G. M., & Dweck, C. S. (2016). Psychologically authentic versus inauthentic replication attempts. Proceedings of the National academy of Sciences of the United States of America,113(43), E6548.
Chacko, A., Bedard, A. C., Marks, D. J., Feirsen, N., Uderman, J. Z., Chimiklis, A., et al. (2014). A randomized clinical trial of Cogmed working memory training in school-age children with ADHD: A replication in a diverse sample using a control condition. Journal of Child Psychology and Psychiatry,55(3), 247–255.
Chacko, A., Jensen, S. A., Lowry, L. S., Cornwell, M., Chimklis, A., Chan, E., et al. (2016). Engagement in behavioral parent training: Review of the literature and implications for practice. Clinical Child and Family Psychology Review,19(3), 204–215.
Chambless, D. (1996a). Identification of empirically supported psychological interventions. PsycEXTRA Dataset. https://doi.org/10.1037/e328832004-001.
Chambless, D. L. (1996b). In defense of dissemination of empirically supported psychological interventions. Clinical Psychology: Science and Practice,3(3), 230–235
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology,66(1), 7–18.
Chambless, D. L., Baker, M. J., Baucom, D. H., Beutler, L. E., Calhoun, K. S., Crits-Christoph, P., et al. (1998). Update on empirically validated therapies, II. The Clinical Psychologist,51(1), 3–16.
Chambless, D. L., & Ollendick, T. H. (2001). Empirically supported psychological interventions: Controversies and evidence. Annual Review of Psychology,52, 685–716.
Chan, S. W., Lau, J. Y., & Reynolds, S. A. (2015). Is cognitive bias modification training truly beneficial for adolescents? Journal of Child Psychology and Psychiatry,56(11), 1239–1248.
Chandrashekar, P. (2018). Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. mHealth,4, 6.
Christiansen, S., Oettingen, G., Dahme, B., & Klinger, R. (2010). A short goal-pursuit intervention to improve physical capacity: A randomized clinical trial in chronic back pain patients. Pain,149(3), 444–452.
Cohen, G. L., Garcia, J., Apfel, N., & Master, A. (2006). Reducing the racial achievement gap: A social-psychological intervention. Science,313(5791), 1307–1310.
Cohen, G. L., Garcia, J., Purdie-Vaughns, V., Apfel, N., & Brzustoski, P. (2009). Recursive processes in self-affirmation: Intervening to close the minority achievement gap. Science,324(5925), 400–403.
Cohen, G. L., & Sherman, D. K. (2014). The psychology of change: Self-affirmation and social psychological intervention. Annual Review of Psychology,65, 333–371.
Conrod, P. J., O’Leary-Barrett, M., Newton, N., Topper, L., Castellanos-Ryan, N., Mackie, C., et al. (2013). Effectiveness of a selective, personality-targeted prevention program for adolescent alcohol use and misuse. JAMA Psychiatry,70(3), 334.
Cuijpers, P., Reijnders, M., & Huibers, M. J. H. (2018). The role of common factors in psychotherapy outcomes. Annual Review of Clinical Psychology. https://doi.org/10.1146/annurev-clinpsy-050718-095424.
Diedrichs, P. C., Atkinson, M. J., Steer, R. J., Garbett, K. M., Rumsey, N., & Halliwell, E. (2015). Effectiveness of a brief school-based body image intervention ‘Dove Confident Me: Single Session’ when delivered by teachers and researchers: Results from a cluster randomised controlled trial. Behaviour Research and Therapy,74, 94–104.
Duckworth, A. L., Kirby, T., Gollwitzer, A., & Oettingen, G. (2013). From fantasy to action: Mental contrasting with implementation intentions (MCII) improves academic performance in children. Social Psychological and Personality Science,4(6), 745–753.
Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development,82(1), 405–432.
Dweck, C. S. (2008). Can personality be changed? The role of beliefs in personality and change. Current Directions in Psychological Science,17(6), 391–394.
Embry, D. D., & Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioral influence. Clinical Child and Family Psychology Review,11, 75-113.
Fitzpatrick, K. K., Witte, T. K., & Schmidt, N. B. (2005). Randomized controlled trial of a brief problem-orientation intervention for suicidal ideation. Behavior Therapy,36, 323–333.
Fu, X., Du, Y., Au, S., & Lau, J. Y. (2013). Reducing negative interpretations in adolescents with anxiety disorders: A preliminary study investigating the effects of a single session of cognitive bias modification training. Developmental Cognitive Neuroscience,4, 29–37.
Fu, X., Du, Y., Au, S., & Lau, J. Y. (2015). Single-session cognitive bias modification of interpretations training in high-anxious adolescents. Journal of Cognitive Psychotherapy,29(3), 253–272.
Furnham, A. (1988). Lay theories: Everyday understanding of problems in the social sciences. Elmsford, NY: Pergamon Press.
Gawrilow, C., Morgenroth, K., Schultz, R., Oettingen, G., & Gollwitzer, P. M. (2013). Mental contrasting with implementation intentions enhances self-regulation of goal pursuit in schoolchildren at risk for ADHD. Motivation and Emotion,37(1), 134–145.
Gollwitzer, A., Oettingen, G., Kirby, T. A., Duckworth, A. L., & Mayer, D. (2011). Mental contrasting facilitates academic performance in school children. Motivation and Emotion,35(4), 403–412.
Goti, J., Diaz, R., Serrano, L., Gonzalez, L., Calvo, R., Gual, A., & Castro, J. (2010). Brief intervention in substance-use among adolescent psychiatric patients: A randomized controlled trial. European Child & Adolescent Psychiatry,19(6), 503–511.
Halliwell, E., & Diedrichs, P. C. (2014). Testing a dissonance body image intervention among young girls. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association,33(2), 201–204.
Hanselman, P., Rozek, C. S., Grigg, J., & Borman, G. D. (2017). New evidence on self-affirmation effects and theorized sources of heterogeneity from large-scale replications. Journal of Educational Psychology,109(3), 405–424.
Harackiewicz, J. M., Canning, E. A., Tibbetts, Y., Giffen, C. J., Blair, S. S., Rouse, D. I., et al. (2014). Closing the social class achievement gap for first-generation students in undergraduate biology. Journal of Educational Psychology,106(2), 375–389.
Harpaz-Rotem, I., Leslie, D., & Rosenheck, R. A. (2004). Treatment retention among children entering a new episode of mental health care. Psychiatric Services,55(9), 1022–1028.
Heyes, S. B., Pictet, A., Mitchell, H., Raeder, S. M., Lau, J. Y. F., Holmes, E. A., & Blackwell, S. E. (2017). Mental imagery-based training to modify mood and cognitive bias in adolescents: Effects of valence and perspective. Cognitive Therapy and Research,41(1), 73–88.
Huey, S. J., Jr., & Polo, A. J. (2008). Evidence-based psychosocial treatments for ethnic minority youth. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53,37(1), 262–301.
Jones, E. B., & Sharpe, L. (2017). Cognitive bias modification: A review of meta-analyses. Journal of Affective Disorders,223, 175–183.
Kataoka, S. H., Zhang, L., & Wells, K. B. (2002). Unmet need for mental health care among U.S. children: Variation by ethnicity and insurance status. The American Journal of Psychiatry,159(9), 1548–1555.
Kauer, S. D., Reid, S. C., Crooke, A. H. D., Khor, A., Hearps, S. J. C., Jorm, A. F., et al. (2012). Self-monitoring using mobile phones in the early stages of adolescent depression: Randomized controlled trial. Journal of Medical Internet Research,14(3), e67.
Kazdin, A. E. (2018). Innovations in psychosocial interventions and their delivery: Leveraging cutting-edge science to improve the world’s mental health. Oxford: Oxford University Press.
Kazdin, A. E., & Rabbitt, S. M. (2013). Novel models for delivering mental health services and reducing the burdens of mental illness. Clinical Psychological Science,1(2), 170–191.
Klimes-Dougan, B., Yuan, C., Lee, S., & Houri, A. K. (2009). Suicide prevention with adolescents: Considering potential benefits and untoward effects of public service announcements. Crisis,30(3), 128–135.
Konrad, T., Ellis, A., Thomas, K., Holzer, C., & Morrissey, J. (2009). County-level estimates of need for mental health professionals in the United States. Psychiatric Services. https://doi.org/10.1176/appi.ps.60.10.1307.
Kowalewski, K., McLennan, J. D., & McGrath, P. J. (2011). A preliminary investigation of wait times for child and adolescent mental health services in Canada. Journal of the Canadian Academy of Child and Adolescent Psychiatry,20(2), 112–119.
Kramer, J., Conijn, B., Oijevaar, P., & Riper, H. (2014). Effectiveness of a web-based solution-focused brief chat treatment for depressed adolescents and young adults: Randomized controlled trial. Journal of Medical Internet Research,16(5), e141.
Krebs, G., Pile, V., Grant, S., Degli Esposti, M., Montgomery, P., & Lau, J. Y. F. (2018). Research review: Cognitive bias modification of interpretations in youth and its effect on anxiety: A meta-analysis. Journal of Child Psychology and Psychiatry and Allied Disciplines,59(8), 831–844.
Lewin, G. W. (1944). Constructs in field theory (1944). Resolving social conflicts and field theory in social science (pp. 191–199). New York: Harper and Brothers.
March, J. S., Silva, S., Petrycki, S., Curry, J., Wells, K., Fairbank, J., et al. (2007). The treatment for adolescents with depression study (TADS): Long-term effectiveness and safety outcomes. Archives of General Psychiatry,64(10), 1132–1143.
Mathews, A., & MacLeod, C. (2005). Cognitive vulnerability to emotional disorders. Annual Review of Clinical Psychology,1, 167–195.
Meehl, P. E. (1990). Appraising and amending theories: The strategy of Lakatosian defense and two principles that warrant it. Psychological Inquiry,1(2), 108–141.
Miller, D. T., Dannals, J. E., & Zlatev, J. J. (2017). Behavioral processes in long-lag intervention studies. Perspectives on Psychological Science: A Journal of the Association for Psychological Science,12(3), 454–467.
Miu, A. S., & Yeager, D. S. (2015). Preventing symptoms of depression by teaching adolescents that people can change. Clinical Psychological Science,3(5), 726–743.
Miyake, A., Kost-Smith, L. E., Finkelstein, N. D., Pollock, S. J., Cohen, G. L., & Ito, T. A. (2010). Reducing the gender achievement gap in college science: A classroom study of values affirmation. Science,330(6008), 1234–1237.
Naify, A.M. (2009). The effectiveness of a brief strength-based intervention on depression in at-risk adolescent girls. Unpublished Dissertation, ProQuest Information & Learning, US.
Ng, M. Y., & Weisz, J. R. (2016). Annual research review: Building a science of personalized intervention for youth mental health. Journal of Child Psychology and Psychiatry and Allied Disciplines,57(3), 216–236.
Oettingen, G. (2012). Future thought and behaviour change. European Review of Social Psychology,23(1), 1–63.
Oettingen, G., Kappes, H. B., Guttenberg, K. B., & Gollwitzer, P. M. (2015). Self-regulation of time management: Mental contrasting with implementation intentions. European Journal of Social Psychology,45(2), 218–229.
Oettingen, G., & Reininger, K. M. (2016). The power of prospection: Mental contrasting and behavior change. Social and Personality Psychology Compass,10(11), 591–604.
Öst, L.-G., & Ollendick, T. H. (2017). Brief, intensive and concentrated cognitive behavioral treatments for anxiety disorders in children: A systematic review and meta-analysis. Behaviour Research and Therapy,97, 134–145.
Reid, G. J., & Brown, J. B. (2008). Money, case complexity, and wait lists: Perspectives on problems and solutions at Children’s Mental Health Centers in Ontario. The Journal of Behavioral Health Services & Research,35(3), 334–346.
Romero, C., Master, A., Paunesku, D., Dweck, C. S., & Gross, J. J. (2014). Academic and emotional functioning in middle school: The role of implicit theories. Emotion,14(2), 227–234.
Schleider, J. L., Abel, M. R., & Weisz, J. R. (2015). Implicit theories and youth mental health problems: A random-effects meta-analysis. Clinical Psychology Review,35, 1–9.
Schleider, J. L., Abel, M., & Weisz, J. R. (2019). Do immediate gains predict long-term symptom change? Findings from a randomized trial of a single-session intervention for youth anxiety and depression. Child Psychiatry & Human Development. https://doi.org/10.1007/s10578-019-00889-2.
Schleider, J. L., & Schroder, H. S. (2018). Implicit theories of personality across development: Impacts on coping, resilience and mental health. The SAGE Handbook of Personality and Individual Differences: Volume I: The Science of Personality and Individual Differences (pp. 152–166). Thousand Oaks: Sage.
Schleider, J. L., & Weisz, J. R. (2015). Implicit theories relate to youth psychopathology, but how? A longitudinal test of two predictive models. Child Psychiatry and Human Development,47(4), 603–617.
Schleider, J. L., & Weisz, J. R. (2016). Reducing risk for anxiety and depression in adolescents: Effects of a single-session intervention teaching that personality can change. Behaviour Research and Therapy,87, 170–181.
Schleider, J. L., & Weisz, J. R. (2017). Little treatments, promising effects? Meta-analysis of single-session interventions for youth psychiatric problems. Journal of the American Academy of Child and Adolescent Psychiatry,56(2), 107–115.
Schleider, J. L., & Weisz, J. R. (2018a). Parent expectancies and preferences for mental health treatment: The roles of emotion mind-sets and views of failure. Journal of Clinical Child and Adolescent Psychology,47, S480–S496.
Schleider, J., & Weisz, J. (2018b). A single-session growth mindset intervention for adolescent anxiety and depression: 9-month outcomes of a randomized trial. Journal of Child Psychology and Psychiatry,59(2), 160–170.
Schroder, H. S., Dawood, S., Yalch, M. M., Brent Donnellan, M., & Moser, J. S. (2014). The role of implicit theories in mental health symptoms, emotion regulation, and hypothetical treatment choices in college students. Cognitive Therapy and Research,39(2), 120–139.
Schroder, H. S., Kneeland, E. T., Silverman, A. L., Beard, C., & Björgvinsson, T. (2018). Beliefs about the malleability of anxiety and general emotions and their relation to treatment outcomes in acute psychiatric treatment. Cognitive Therapy and Research. https://doi.org/10.1007/s10608-018-9985-7.
Sherman, M. L., Barnum, D. D., Buhman-Wiggs, A., & Nyberg, E. (2009). Clinical intake of child and adolescent consumers in a rural community mental health center: Does wait-time predict attendance? Community Mental Health Journal,45(1), 78–84.
Sherman, D. K., & Cohen, G. L. (2006). The psychology of self-defense: Self-affirmation theory. Advances in Experimental Social Psychology, vol 38 (pp. 183–242). Amsterdam: Elsevier.
Sherman, D. K., & Cohen, G. L. (2014). Social psychological interventions and social change: A self-affirmation perspective. PsycEXTRA Dataset. https://doi.org/10.1037/e578192014-019.
Sherman, D. K., Hartson, K. A., Binning, K. R., Purdie-Vaughns, V., Garcia, J., Taborsky-Barba, S., et al. (2013). Deflecting the trajectory and changing the narrative: How self-affirmation affects academic performance and motivation under identity threat. Journal of Personality and Social Psychology,104(4), 591–618.
Silverman, W. K., & Hinshaw, S. P. (2008). The second special issue on evidence-based psychosocial treatments for children and adolescents: A 10-year update. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53,37(1), 1–7.
Smith, D. H., & Hadorn, D. C. (2002). Lining up for children’s mental health services: A tool for prioritizing waiting lists. Journal of the American Academy of Child and Adolescent Psychiatry,41(4), 367–376.
Smith, E. N., Romero, C., Donovan, B., Herter, R., Paunesku, D., Cohen, G. L., et al. (2018). Emotion theories and adolescent well-being: Results of an online intervention. Emotion,18(6), 781–788.
Southam-Gerow, M. A., & Prinstein, M. J. (2014). Evidence base updates: The evolution of the evaluation of psychological treatments for children and adolescents. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53,43(1), 1–6.
Squires, J. E., Sullivan, K., Eccles, M. P., Worswick, J., & Grimshaw, J. M. (2014). Are multifaceted interventions more effective than single-component interventions in changing health-care professionals’ behaviours? An overview of systematic reviews. Implementation Science: IS,9, 152.
Stallard, P., Velleman, R., Salter, E., Howse, I., Yule, W., & Taylor, G. (2006). A randomised controlled trial to determine the effectiveness of an early psychological intervention with children involved in road traffic accidents. Journal of Child Psychology and Psychiatry,47(2), 127–134.
Stanford, J. N., & McCabe, M. P. (2005). Evaluation of a body image prevention programme for adolescent boys. European Eating Disorders Review: The Professional Journal of the Eating Disorders Association,13(5), 360–370.
Thomaes, S., Bushman, B. J., Castro, B. O. D., Cohen, G. L., & Denissen, J. J. (2009). Reducing narcissistic aggression by buttressing self-esteem: An experimental field study. Psychological Science,20(12), 1536–1542.
Thomaes, S., Bushman, B. J., de Castro, B. O., & Reijntjes, A. (2012). Arousing “gentle passions” in young adolescents: Sustained experimental effects of value affirmations on prosocial feelings and behaviors. Developmental Psychology,48, 103.
Walker, D. D., Roffman, R. A., Stephens, R. S., Wakana, K., & Berghuis, J. (2006). Motivational enhancement therapy for adolescent marijuana users: A preliminary randomized controlled trial. Journal of Consulting and Clinical Psychology,74(3), 628.
Walton, G. M. (2014). The new science of wise psychological interventions. Current Directions in Psychological Science,23(1), 73–82.
Walton, G. M., & Wilson, T. D. (2018). Wise interventions: Psychological remedies for social and personal problems. Psychological Review,125(5), 617–655.
Webb, C. A., Auerbach, R. P., & Derubeis, R. J. (2012). Processes of change in CBT of adolescent depression: Review and recommendations. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53,41(5), 654–665.
Webb, T. L., & Sheeran, P. (2007). How do implementation intentions promote goal attainment? A test of component processes. Journal of Experimental Social Psychology,43(2), 295–302.
Weiner, B. (1985). An attributional theory of achievement motivation and emotion. Psychological Review,92(4), 548–573.
Weisz, J., Bearman, S. K., Santucci, L. C., & Jensen-Doss, A. (2017a). Initial test of a principle-guided approach to transdiagnostic psychotherapy with children and adolescents. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53,46(1), 44–58.
Weisz, J. R., Chorpita, B. F., Palinkas, L. A., Schoenwald, S. K., Miranda, J., Bearman, S. K., et al. (2012). Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: A randomized effectiveness trial. Archives of General Psychiatry,69(3), 274–282.
Weisz, J. R., Kuppens, S., Ng, M. Y., Eckshtain, D., Ugueto, A. M., Vaughn-Coaxum, R., et al. (2017b). What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice. The American Psychologist,72(2), 79–117.
Weisz, J. R., Kuppens, S., Ng, M. Y., Vaughn-Coaxum, R. A., Ugueto, A. M., Eckshtain, D., et al. (2018). Are psychotherapies for young people growing stronger? Tracking trends over time for youth anxiety, depression, attention-deficit/hyperactivity disorder, and conduct problems. Perspectives on Psychological Science: A Journal of the Association for Psychological Science,14(2), 216–237.
Williams, M. E., Latta, J., & Conversano, P. (2008). Eliminating the wait for mental health services. The Journal of Behavioral Health Services & Research,35(1), 107–114.
Wittleder, S., Kappes, A., Oettingen, G., Gollwitzer, P. M., Jay, M., & Morgenstern, J. (2019). Mental contrasting with implementation intentions reduces drinking when drinking is hazardous: An online self-regulation intervention. Health Education Behavior. https://doi.org/10.1177/1090198119826284.
Yarkoni, T., & Westfall, J. (2017). Choosing prediction over explanation in psychology: Lessons from machine learning. Perspectives on Psychological Science,12(6), 1100–1122.
Yeager, D. S., & Dweck, C. S. (2012). Mindsets that promote resilience: When students believe that personal characteristics can be developed. Educational Psychologist,47(4), 302–314.
Yeager, D. S., Lee, H. Y., & Jamieson, J. P. (2016a). How to improve adolescent stress responses: Insights from integrating implicit theories of personality and biopsychosocial models. Psychological Science,27(8), 1078–1091.
Yeager, D. S., Romero, C., Paunesku, D., Hulleman, C. S., Schneider, B., Hinojosa, C., et al. (2016b). Using design thinking to improve psychological interventions: The case of the growth mindset during the transition to high school. Journal of Educational Psychology,108(3), 374–391.
Yeager, D. S., & Walton, G. M. (2011). Social-psychological interventions in education. Review of Educational Research,81(2), 267–301.
Zuckerbrot, R. A., Cheung, A., Jensen, P. S., Stein, R. E. K., Laraque, D., & GLAD-PC STEERING GROUP. (2018). Guidelines for adolescent depression in primary care (GLAD-PC): Part I: practice preparation, identification, assessment, and initial management. Pediatrics,141, e20174081.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no potential conflicts to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Schleider, J.L., Mullarkey, M.C. & Chacko, A. Harnessing Wise Interventions to Advance the Potency and Reach of Youth Mental Health Services. Clin Child Fam Psychol Rev 23, 70–101 (2020). https://doi.org/10.1007/s10567-019-00301-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10567-019-00301-4