
Abstract
We review 85 empirical articles published since 2000 that measured the acquisition and/or utilization of parent management skills and/or child cognitive-behavioral skills in the context of an evidence-based treatment (EBT) for childhood behavior problems. Results showed that: (1) there are no standardized measures of skill acquisition or skill utilization that are used across treatments, (2) little is known about predictors, correlates, or outcomes associated with skill acquisition and utilization, and (3) few studies systematically examined techniques to enhance the acquisition and utilization of specific skills. Meta-analytic results from a subset of 68 articles (59 studies) showed an overall treatment–control ES = .31, p < .01 for skill acquisition and ES = .20, p = ns for skill utilization. We recommend that future research focus on the following three areas: (1) development of standardized measures of skill acquisition and utilization from a “common elements” perspective that can used across EBTs; (2) assessment of the predictors, correlates, and outcomes associated with skill acquisition and utilization; and (3) development of innovative interventions to enhance the acquisition and utilization of cognitive-behavioral and parent management skills.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The focus of much psychotherapy research over the past few decades has been on defining, evaluating, and cataloguing evidence-based treatments (EBTs; e.g., Chambless and Hollon 1998; Ollendick et al. 2006). EBTs have been shown to be effective in treating a wide range of childhood and adolescent disorders, including disruptive behavior disorders (DBDs), relative to no treatment (Weisz et al. 1987, 1995), and even relative to usual care (Weisz et al. 2006). A recent review article identified no less than 16 different psychosocial EBTs for children and adolescents with disruptive behaviors (Eyberg et al. 2008). Examples include Parent Management Training (Patterson et al. 1975), Problem-Solving Skills Training (Kazdin 2003), and the Incredible Years program (Webster-Stratton and Reid 2003).
Skill Acquisition and Utilization
The acquisition and utilization of skills is central to many behavior therapy (BT) and cognitive-behavioral therapy (CBT) treatments, including treatments for disruptive behavior disorders. For example, in Parent–Child Interaction Therapy (PCIT; Funderburk and Eyberg 2011; McNeil and Hembree-Kigin 2011), parents must demonstrate mastery of a set of skills before moving on to the next phase of treatment and graduating from treatment. Therapists are trained to assess mastery of skills by coding parent–child interactions using a behavior observation coding system during each treatment session. Parents are also given homework sheets to report on their daily skill-use between treatment sessions. The purpose of this review and meta-analysis is to summarize the recent literature (since 2000) on skill acquisition and utilization, constructs that are central to psychosocial treatments for disruptive behavior.
Definitions
There are no standard definitions of skill acquisition or skill utilization, and other terms have been used to describe similar constructs. For example, the term treatment receipt is similar to skill acquisition. Bellg and colleagues define treatment receipt as, “the degree to which the participant understands and demonstrates knowledge of and ability to use treatment skills” (Bellg et al. 2004, p. 444). Likewise, the term treatment enactment is similar to skill utilization. Treatment enactment is defined by Bellg and colleagues as, “the degree to which the participant applies the skills learned in treatment in his or her daily life” (p. 444). For the purposes of this review and meta-analysis, we use the terms skill acquisition and skill utilization, as these terms are more commonly used in the DBD literature (e.g., Lyon and Budd 2010; Nash et al. 2003; O’Callaghan et al. 2003; Shanley and Niec 2010; Thornberry and Brestan-Knight 2011; Timmer et al. 2011; Ware et al. 2008).
Skill Acquisition
We defined skill acquisition as the degree to which a parent/child can perform a skill learned during the course of treatment. This definition includes only the formal assessment of a skill by an “expert” rater (e.g., therapist, clinician, and assessor) using a rubric, checklist, behavior observation, or rating scale. It does not include a parent’s self-report on a parenting measure (e.g., Parenting Practices Inventory or Alabama Parenting Questionnaire). An example of a measure that meets our definition of skill acquisition is the Dyadic Parent–Child Interaction Coding System (DPICS; Eyberg et al. 2005). The DPICS is an observational coding system used to record the frequency of encouraged behaviors and discouraged behaviors that are taught in PCIT. For example, Bagner et al. (2010) used the DPICS to measure skill acquisition in both treatment and control groups. In their study, trained coders observed 5-min parent–child interactions and recorded “do skills” (behaviors encouraged in PCIT: behavior descriptions, reflections, and praises) and “don’t skills” (behaviors discouraged in PCIT: questions, commands, and negative talk).
Skill Utilization
We defined skill utilization as the degree to which a parent/child uses a skill in his/her daily life outside of treatment sessions. This might include the practice of a skill assigned as “homework” or “home practice” by the therapist, but this is only a very small piece of the definition. Rather, the term refers more generally to skill-use that is initiated by the parent/child on a day-to-day basis. An example of a study that meets our definition of skill utilization is Leathers and colleagues’ KEEP study (Leathers et al. 2011). Parent skill utilization was measured using a telephone interview. Foster parents were asked to report on the number of times they had used intervention skills in the past 3 days. The KEEP intervention skills that were assessed included praise and specific discipline techniques (e.g., time-out, privilege loss, and work chores).
Rationale for a Review and Meta-analysis
Whereas there is a growing research literature on predictors and moderators of treatment outcome (e.g., symptom severity, comorbid conditions, and parent psychopathology), less is known about specific mechanisms through which these variables exert their influence on the course of treatment. From behavior therapy (BT) and cognitive-behavioral therapy (CBT) perspectives, these variables may influence the course of treatment via several mechanisms, including (a) participation/engagement, (b) skill acquisition, (c) skill utilization, and (d) maintenance of cognitive and behavioral changes. In order to improve treatment outcome, therefore, it is critical to measure these constructs in order to pinpoint barriers to treatment progress. Traditional randomized clinical trials have focused on assessing outcome in terms of symptoms, diagnoses, and functioning, with less attention to measuring these theoretically central intermediate processes (Nock and Ferriter 2005). A review and meta-analysis of skill acquisition and utilization is needed to guide future research and refine existing treatments for childhood behavior problems. Although numerous reviews and meta-analyses have focused on DBD treatments (e.g., Eyberg et al. 2008; Kaminski et al. 2008; Reyno and McGrath 2006), this is the first to focus exclusively on the constructs of skill acquisition and utilization. The most closely related prior reviews are perhaps studies by Kaminski et al. (2008) and Boyle and Lutzker (2011). The Kaminski et al. (2008) study is a component analysis, with a focus on treatment content and delivery method, but includes skill acquisition as one of several outcomes for a subset of the studies. Boyle and Lutzker (2011) examined the generalization (i.e., skill utilization) of parent training skills in 16 studies. However, their review did not estimate effect sizes or include studies on the generalization of child skills. In contrast to these prior reviews, the purpose of the current review and meta-analysis was to focus explicitly on skill acquisition and skill utilization for both parent skills and child skills and to estimate effect sizes.
Current Study
The aim of the current study was to summarize the recent literature (since 2000) on skill acquisition and skill utilization for psychosocial DBD treatments. We chose 2000 as our cutoff to focus on the most recent decade (approximately) and thereby reflect the current state of the field. The aim of the review was to summarize (1) measurement approaches; (2) predictors, correlates, and outcomes examined in relation to these constructs; and (3) the frequency with which these constructs are specific targets of intervention. This information will be useful for identifying knowledge gaps and guiding future areas of research. The goal of the meta-analysis was to estimate effect sizes for skill acquisition and skill utilization. This information has the potential to inform treatment refinement (e.g., which skills are not being learned well by parents and children?) and generate hypotheses about specific mechanisms of change (e.g., which skills do parents and children actually use in their day-to-day lives?).
Method
Procedure
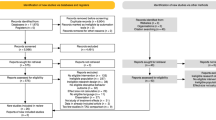
Articles were included in the review and meta-analysis based on the following criteria: (1) the target of treatment fell within the group of symptoms related to disruptive behavior disorders (e.g., externalizing behavior, behavior problems, conduct problems, and oppositional behavior); (2) the treatment was evidence-based (i.e., efficacy or effectiveness supported by at least one published study in a peer-reviewed journal); (3) the treatment was not primarily school-based; (4) there was a measure of skill acquisition and/or skill utilization; and (5) the measures were consistent with our definitions described above. As this article focuses on the recent literature, only articles published from January 2000 through January 2012 were included. A total of 85 articles were found and included in the review using these methods. Of these 85 articles, 68 were also included in the meta-analysis (see Fig. 1).

Study selection flow chart
Study Selection
Studies included in the review and meta-analysis were identified through a systematic online database search of PsycINFO and Medline. The search was comprised of terms related to disruptive behavior disorders (DBDs) and skill acquisition or skill utilization. We began with an initial list of terms and added to this list as more terms were identified through the literature. DBD-related terms included: Disruptive Behavior Disorders, DBD; Conduct Disorder, CD; Oppositional Defiant Disorder, ODD; disruptive behavior, behavior problems, conduct problems, externalizing behavior, aggressive behavior, antisocial behavior, oppositional behavior, and noncompliance. Skill acquisition terms included: skill acquisition, skill mastery, and skill competence. Skill utilization terms included: skill utilization, skill use, skill practice, compliance, adherence, generalization, and skill implementation. DBD terms were crossed once with each skill acquisition term and once with each skill utilization term for a total of 154 permutations. The search yielded 9,172 possible articles. Our literature search also yielded a brief quantitative review on the generalization of parent skills learned in behavioral parent training programs (Boyle and Lutzker 2011), which gave us an additional 16 possible articles. Of the articles identified through our literature search and the quantitative review, 15 met our inclusion criteria and were included in the review.
For a more thorough search of the literature, we also manually searched through articles published in relevant journals. A list of possible journals to search was compiled prior to the literature search. The publication titles of the articles found through the database search were added to this list. We added only the journals in which at least one relevant article was found, as these journals would be likely to have published relevant articles. The following journal titles were searched: Behavior Therapy, Behavioral Disorders, Behavioral Interventions, Child and Family Behavior Therapy, Child Psychiatry and Human Development, Clinical Psychology Review, Clinical Psychology: Science and Practice, Education and Treatment of Children, International Journal of Child & Adolescent Health, Journal of Abnormal Child Psychology, Journal of Applied Behavior Analysis, Journal of Child Psychology and Psychiatry, Journal of Clinical Child and Adolescent Psychology, Journal of Consulting and Clinical Psychology, Journal of Emotional and Behavioral Disorders, Journal of Marital and Family Therapy, Journal of Pediatric Health Care, and Psychology in the Schools. Eleven articles meeting our inclusion criteria were found using this method.
A second online database search using PsycINFO and Medline was conducted using the names of DBD treatments and models found in our first 26 articles. Keyword searches of behavioral parent training, Fast Track, Incredible Years. Keeping Foster Parents Trained and Supported, KEEP, Multidimensional Treatment Foster Care, MTFC, Parent–Child Interaction Therapy, PCIT, Parent Management Training, PMT, Parent Management Training Oregon Model, PMTO, Positive Parenting Program, Triple P, Problem Solving Skills Training, and PSST yielded 1,358 articles. Fifty-nine of these articles met our inclusion criteria and were included in our review. Thus, our literature searches yielded a total of 85 articles on skill acquisition and/or skill utilization that met our inclusion criteria were included in the review.
Seventeen of the initial 85 articles were excluded from the meta-analysis because we were unable to calculate an effect size for skill acquisition and/or skill utilization based on the information provided in the article. For seven articles, skill acquisition and/or skill utilization was measured only once (e.g., at post-treatment) and the study did not have a control group, so no effect size could be calculated. For two articles, skill acquisition and/or skill utilization was measured during treatment sessions but not at post-treatment, so no effect size could be calculated. Five articles that measured skill utilization by tracking homework completion were also excluded. For these articles, homework completion (skill utilization) was measured for the treatment group throughout the intervention. No control group data and no pre- and post-data were collected, so no effect size could be calculated. For nine articles, statistics required for calculating an effect size (e.g., means and standard deviations) were not reported in the published article and the authors of these articles were contacted for additional data. The authors of six articles responded and were included in the analysis; the authors from three articles did not respond and were excluded. A total of 68 articles were included in the final meta-analysis.
Study Coding
Study coding methods were based on Lipsey and Wilson’s (2001) recommendations. The studies were coded using the coding procedures described in Appendices 1 and 2. The second author was trained by the first author in all coding procedures. Any questions or discrepancies were resolved through discussion between the first and second author. Individual skills within each study were coded by the first and second authors to assess reliability (88.4 % inter-rater agreement). Consistent with meta-analytic methods, multiple articles describing the same dataset were coded as a single study. We therefore had 68 articles but only 59 separate studies included in the meta-analysis. Study variables included in the meta-analysis were as follows (see Appendices 1 and 2 for a complete list of codes and operationalized definitions):
-
1.
Research design descriptors: Total sample size, treatment group sample size, and control group sample size.
-
2.
Nature of intervention descriptors: Intervention name, whether it was prevention or treatment, and type of control group (no treatment, waitlist, treatment as usual, alternative treatment, or no control group).
-
3.
Skill descriptors: Whether the skill measured was acquisition or utilization, whether it was a parent skill or a child skill, and the specific category of skill (Positive Parenting, Negative Parenting, Praise, Verbal/Nonverbal Communication, Positive/Negative Consequences, Other Parent Skill, Emotion Labeling, Problem-solving, Anger management, Social Skills, or Other Child Skill).
-
4.
Effect size descriptor: Whether the effect size was calculated for pre–post change or treatment–control difference (analyzed separately).
The studies were analyzed at multiple levels of specificity according to the above variables. In the first set of analyses, we examined effect sizes for overall skill acquisition and overall skill utilization. In the second set of analyses, we divided the effect sizes further and examined parent skill acquisition, parent skill utilization, child skill acquisition, and child skill utilization separately. In the final set of analyses, we examined effect sizes for parent/child skill acquisition and skill utilization for each of our 11 skill categories (Positive Parenting, Negative Parenting, Praise, Communication, Consequences, Other Parent Skill, Emotion Labeling, Problem-solving, Anger management, Social Skills, or Other Child Skill; see Appendix 2 for category definitions).
Analyses
Meta-analyses were conducted with Lipsey and Wilson’s (2001) SPSS macros. First, a meta-analytically derived mean effect size (d) was obtained for each outcome. Pre–post effects were analyzed separately from treatment–effect sizes. We relied on random effects models because this more conservative approach allows generalization beyond included samples (Rosenthal and DiMatteo 2001). A homogeneity statistic (Q) was derived based on these effect sizes to examine the amount of heterogeneity in the effect sizes. The Q statistic has a chi-square distribution based on k − 1 degrees of freedom, with k representing the number of effect sizes in the analysis. A statistically significant homogeneity Q statistic supports a heterogeneous distribution.
Results
Overview
The 85 articles that were included in the final review are summarized in Tables 1 and 2. Seventy-four (87 %) of the articles included in this review measured skill acquisition. A variety of skill acquisition measures were used, but the majority were observational (n = 60; 81.1 %). The rest included clinician report (n = 3; 4.1 %), self-report (n = 1; 1.4 %), or a test of knowledge/performance assessment to measure skill acquisition (n = 12; 16.2 %). A large number of these articles measured only the acquisition of parent skills (n = 64; 86.5 %) and did not examine child skills. Twenty-four (32 %) of the articles included in this review measured skill utilization. Types of measures used in these articles included observational (n = 7; 29.2 %), clinician report (n = 1; 4.2 %), self-report (n = 5; 20.8 %), parent report (n = 1; 4.2 %), test of knowledge/performance assessment (n = 1; 4.2 %), and homework (n = 10; 41.7 %). Articles measuring skill utilization also tended to assess parent skills (n = 21; 87.5 %) rather than child skills.
Many of these articles examined skill acquisition and skill utilization as a primary measure of treatment outcome. While these articles reported parent and child competency in performance of target skills and/or frequency of use of target skills in their daily lives, these constructs were not studied as specific mechanisms of change. In other words, a large number of the articles we reviewed did not examine any antecedents/predictors of, outcomes associated with, or ways to enhance skill acquisition and utilization. Thirty-five (47.3 %) skill acquisition articles and 11 (50 %) skill utilization articles measured skill acquisition and utilization but did not further examine antecedents, correlates, or outcomes.
Methods of Assessment
Articles varied greatly in methods and procedures of assessment of skill acquisition and utilization (see Tables 1, 2). There was no discernable pattern in the frequency, duration, and sampling of assessments. For example, although many articles used observations to assess skill acquisition and utilization, the specific methods for observation were different across most articles. Observation periods ranged from 5 to 75 min long and they included both structured tasks and play interactions. Frequency of observations ranged from once or twice during pretreatment and/or post-treatment to every treatment session. Coding methods also varied and included coding of every utterance/parent–child exchange, selected nonverbal behaviors, a set number of parent instructions/demands, and behaviors occurring at specific time intervals (e.g., 10 s). Other types of assessments such as clinician report and self-report used several different factors (e.g., homework completion, session attendance, and general impressions of skill competency) to come up with composite ratings of skill acquisition and utilization. Homework and tests of knowledge/performance assessments were generally tailored to the specific treatment or intervention used in the study, so their assessment procedures were very different from each other.
Antecedents/Predictors of Skill Acquisition and Utilization
Only 13 skill acquisition articles and five skill utilization articles looked at antecedents and predictors of skill acquisition and utilization (see Tables 1, 2). A study by Nock and Kazdin (2005) looked at parent motivation and its relation to skill acquisition and utilization in PMT. Before treatment, parents were given a self-report measure of motivation (Parent Motivation Inventory [PMI; Nock and Photos 2006]) to assess their Desire for Child Change, Readiness to Change, and Perceived Ability to Change. Skill acquisition and skill utilization were measured at three sessions throughout treatment via clinician and parent self-report. This study found that a few parent motivation variables (readiness to participate, perceived ability to participate) were related to clinician reports of parent skill utilization (Nock and Kazdin 2005). Another study by Forgatch et al. (2005) looked at clinician treatment adherence and competence and its effects on skill acquisition. Clinicians conducting PMT were rated on competent adherence to PMT according to the Fidelity of Implementation Rating System (FIMP; Knutson et al. 2003). Parents were rated on use of PMT skills during parent–child interactions by observers. According to the results of this study, clinician treatment adherence and competence had a positive effect on parents’ acquisition of PMT skills (Forgatch et al. 2005).
Outcomes Associated with Skill Acquisition and Utilization
Outcomes were most frequently investigated with 21 skill acquisition articles and seven skill utilization articles in this category (see Tables 1, 2). The majority of these articles looked at the relationship between skill acquisition and utilization and improvement rates in child behavior problems, finding a positive correlation between the variables (Delaney and Kaiser 2001; Kling et al. 2010; Marchant and Young 2001; Marchant et al. 2004; Marcus et al. 2001; Martinez and Forgatch 2001). For example, Martinez and Forgatch (2001) conducted a study relating child noncompliance levels to parents’ acquisition of PMT skills. Skill acquisition was measured via laboratory observations of structured parent–child interactions. This study showed that both coercive discipline and positive parenting skills mediated treatment outcome. Rates of child noncompliance improved as use of coercive discipline decreased and positive PMT skills increased (Martinez and Forgatch 2001).
Enhancing Skill Acquisition and Utilization
Enhancement was studied in a small number of these articles. Eleven skill acquisition articles and six skill utilization articles investigated specific methods for improving enhancement of skill acquisition and utilization (see Tables 1, 2). Shanley and Niec (2010) studied the effects of in vivo feedback on skill acquisition among parents receiving PCIT. For parent–child pairs in the coaching group, parents received feedback and coaching during play interactions with their children. Parents were coached using modeling and praise via a bug-in-the-ear device. Parents who were coached during play interactions had significantly higher rates of PCIT skill acquisition than parents who were not coached (Shanley and Niec 2010). In Nock and Kazdin’s (2005) study with families in PMT, they developed a participant enhancement intervention (PEI) designed to improve both skill acquisition and utilization among parents. Parents in the PEI group received an added 5- to 15-min discussion during sessions one, five, and seven. These discussions focused on parent plans for change and potential barriers to treatment participation. Parents also completed a worksheet on plans to overcome these barriers as they occurred during treatment. Parents who received this added discussion scored significantly higher on clinician and self-report measures of PMT skill acquisition and utilization (Nock and Kazdin 2005). Kling et al. (2010) compared practitioner-assisted group training and self-administered training in terms of their effects on skill utilization among parents receiving PMT. Parents in the self-administered training group received a single training session and then implemented PMT on their own. Those in the group training met weekly with other parents for instruction, discussion, and practice of PMT skills. Homework completion (a component of skill utilization) was significantly higher for parents receiving group training versus those receiving self-administered training (Kling et al. 2010).
Meta-Analytic Results
Of the 85 articles included in the review, 68 were included in the final meta-analysis (see Fig. 1). These 68 articles represented 59 separate studies. Of these 68 articles, 62 measured skill acquisition and eight articles measured skill utilization. (Two articles measured both skill acquisition and utilization). Effect sizes are summarized in Table 3 (skill acquisition) and Table 4 (skill utilization). Separate sub-category (e.g., positive parenting) effect sizes were only calculated when three or more studies met inclusion criteria. Because there were so few studies on skill utilization, separate effect sizes could not be estimated for the utilization of child CBT skills or for the utilization of separate skill categories. Figure 2 depicts a histogram of the mean treatment–control effect sizes for individual studies.

Mean treatment–control effect sizes for individual studies
Pre–post Versus Treatment–Control Effect Sizes
In every instance, pre–post effects sizes were substantially larger than treatment–control effect sizes, by a magnitude of 300–1400 %. Across all analyses, average pre–post effect sizes ranged from 1.15 to 2.02 compared to treatment–control effect sizes which ranged from .04 to .66. We focus the remainder of this section on treatment–control effects sizes as the more conservative estimate of effect sizes.
Skill Acquisition
The overall treatment–control effect size for skill acquisition was .31 (p < .01; see Table 3). Orwin’s (1983) fail-safe N calculation indicated that an additional 21 studies with null findings would be necessary to reduce the mean effect size below d = .20 (Cohen’s minimum d for a small effect size). All fail-safe N estimates listed below are for the same effect size standard of d = .20. The effect size was .40 (p < .01; fail-safe N = 7) for child skills and .30 (p < .01; fail-safe N = 17) for parent skills. Separate effect size estimates were calculated for positive parenting strategies (ES = .41, p < .01; fail-safe N = 25), negative parenting strategies (ES = .26, p < .01; fail-safe N = 9), praise (ES = .66, p < .05; fail-safe N = 14), communication skills (ES = .13, p = ns), and consequences (ES = .04, p = ns). For child skills, a separate effect size was calculated for problem-solving (ES = .17, p = ns).
Skill Utilization
The overall treatment–control effect size for skill utilization was .20 (p = ns; see Table 4). All three effect sizes included in this effect size estimate were for parent skills. A separate effect size could not be calculated for child skills or for separate skill categories.
Discussion
Based on the results of our review and meta-analysis, we recommend that future research focus on three areas in order to fill gaps in the empirical literature. First, we recommend that researchers seek to develop standardized measures and methods for assessing the acquisition and utilization of cognitive-behavioral skills that can be used across the various EBTs for childhood behavior problems. Second, we recommend additional research on the determinants, correlates, and sequelae of skill acquisition/utilization. Third, we recommend that research focus on innovative ways to enhance the acquisition and utilization of BT and CBT skills.
Need for Standardized Measures of Skill Acquisition and Utilization
The absence of standardized measures and methods for assessing skill acquisition and skill utilization makes it difficult to compare the extent to which patients and families are using the skills they are learning in treatment in their day-to-day lives across treatments. This makes it difficult to compare treatment results with one another across the various psychosocial EBTs for childhood disruptive behavior problems. Measures of skill acquisition were generally specific to a particular treatment protocol and tended to assess either broad categories, such as positive or negative parenting, or a very narrow set of skills such as praise and problem-solving. To this end, we recommend the development of a measure from a “common elements” perspective (e.g., Chorpita and Weisz 2009) that can be used to assess the acquisition of a wide range of BT and CBT skills that are common across several psychosocial EBTs for childhood disruptive behavior problems. Researchers (McLeod and Weisz 2005) have developed an observational measure of therapist behavior from a “common elements” approach (Therapy Procedures Observational Coding System) to understand the content and extensiveness of skills reviewed by therapists in treatment sessions. A similar approach may be helpful to measure parent and/or child skill acquisition and utilization.
Measures of skill utilization were largely retrospective self-reports or infrequent (often just one time) home observations. Both modalities appear to have their place as self-reports are more convenient and less costly, whereas behavioral observations in the home are typically more accurate indicators of day-to-day functioning. Therefore, efforts should be taken to evaluate the utility of self-report versus observational methods of skill utilization as it unclear whether the more costly and labor-intensive behavioral observation approach is necessary. In terms of specific assessment methods, we recommend the development of an ecologically valid time-sampling or event-sampling approach to gather data on skill utilization between treatment sessions. There are several approaches to collecting valid data outside of the laboratory (or clinic) including daily diary methods (e.g., Bolger et al. 2003), ecological momentary assessment (EMA; Stone and Shiffman 1994), experience sampling methods (ESM; Reis and Gable 2000), and ambulatory assessment (AA; Ebner-Priemer and Trull 2009). Such methods have numerous advantages over traditional retrospective self-reports including ecological validity, real-time assessment, and the opportunity for multiple assessments (e.g., Bolger et al. 2003; Ebner-Priemer and Trull 2009).
Determinants, Correlates, and Sequelae of Skill Acquisition/Utilization
Although BT and CBT skills are conceptualized as specific mechanisms of change, they are rarely examined as such in the empirical literature. To this end, it will be important in future research to explore the determinants, correlates, and sequelae of skill acquisition and utilization. For example, it will be important to assess the association between skill utilization and the reduction in child behavior problems. A good exemplar of such a study was conducted by Chamberlain and colleagues (Chamberlain, et al. 2008). In the study, specific parenting skills (e.g., positive reinforcement) were found to mediate the reduction of behavior problems in a group of foster children. More studies like this one will have important implications for understanding and addressing nonresponse and partial response to treatment. If poor or infrequent skill utilization is strongly associated with treatment response and outcome, then targeting skill utilization may enhance treatment response and outcome.
Enhancing the Utilization of Skills
Finally, we recommend developing interventions designed specifically to increase skill utilization outside of treatment sessions beyond traditional “homework” or “home practice” assignments. These interventions would not be stand-alone treatments, but rather designed to supplement or augment existing skill-based treatments. Although there are numerous possibilities for such interventions, procedures would likely involve increased between-session contact between families and clinician through additional phone contact with the primary clinician, a third-party skills coach, or virtual contact and feedback through the use of digital technologies (e.g., PDA, iTouch, or smart phone). We recommend that any protocol receive ongoing input from families and clinicians to ensure acceptability, feasibility, and clinical utility. This input could be in the form of formal consultation or focus groups. Once a protocol has been developed, its efficacy could be examined through a randomized clinical trial comparing those who receive an augmented skills-enhancement protocol versus those who receive a standard skills-based treatment alone. It will be especially important to examine group differences in terms of: (1) skill utilization, (2) symptom reduction, and (3) treatment outcome.
Effect Sizes
Overall, the treatment–control effect size for skill acquisition was significantly different from zero, but in the “small to moderate” range by traditional standards. However, there was some variability noted within specific skill categories with praise having the largest effect size, falling in the “moderate to large” range by traditional standards. This suggests that some skills might be easier to acquire than others. There were far fewer studies on skill utilization compared to skill acquisition. This is not surprising, given that skill utilization is more of a distal outcome and requires assessing children and parents outside of the clinic setting. Overall, the treatment–control effect size for skill utilization was in the “small” range by traditional standards and not significantly different from zero. Pre–post effect sizes appeared to be substantially inflated in comparison with effect sizes from studies using more rigorous treatment–control designs. In light of this, we recommend that studies using pre–post designs be interpreted very cautiously.
Summary
This review and meta-analysis of the empirical literature on psychosocial EBTs for DBDs showed an overall treatment–control ES = .31 for skill acquisition and ES = .20 for skill utilization. Our review of the literature also highlights the need for additional research on the acquisition and utilization of BT and CBT skills. Filling in this gap is especially important as BT and CBT skills are conceptualized as being specific factors of change. We recommend the development of standardized assessment measures and methods for assessing skill acquisition and utilization from a “common elements” perspective, followed by the investigations of determinants, correlates, and sequelae of skill acquisition and utilization. This research will likely have implications for enhancing treatment delivery through interventions targeting skill utilization which can be used to supplement or augment existing skills-based treatments. Such an approach has the potential to reduce rates of nonresponse and partial response to treatment.
References
* denotes articles included in the meta-analysis.
† denotes articles include in the review.
†*Bagner, D. M. & Eyberg, S. M. (2007). Parent-child interaction therapy for disruptive behavior in children with mental retardation: A randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 36(3), 418–429.
†*Bagner, D. M., Sheinkopf, S. J., Vohr, B. R., & Lester, B. M. (2010). Parenting intervention for externalizing behavior problems in children born premature: An initial examination. Journal of Developmental and Behavioral Pediatrics, 31(3), 209–216. doi:10.1097/DBP.0b013e3181d5a294.
Bellg, A. J., Borrelli, B., Resnick, B., Hecht, J., Minicucci, D. S., Ory, M., et al. (2004). Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychology, 23(5), 443–451. doi:10.1037/0278-6133.23.5.443.
†Benoit, D. A., Edwards, R. P., Olmi, D. J., Wilczynski, S. M., & Mandal, R. L. (2001). Generalization of a positive treatment package for child noncompliance. Child & Family Behavior Therapy, 23(2), 19–32. doi:10.1300/J019v23n02_02.
†Berkovits, M. D., O’Brien, K. A., Carter, C. G., & Eyberg, S. M. (2010). Early identification and intervention for behavior problems in primary care: A comparison of two abbreviated versions of parent-child interaction therapy. Behavior Therapy, 41(3), 375–387. doi:10.1016/j.beth.2009.11.002.
†Bierman, K. L., Nix, R. L., Maples, J. J., Murphy, S. A., & Conduct Problems Prevention Research Group. (2006). Examining clinical judgment in an adaptive intervention design: The fast track program. Journal of Consulting and Clinical Psychology, 74(3), 468–481. doi:10.1037/0022-006X.74.3.468.
Bolger, N., Davis, A., & Rafaeli, E. (2003). Diary methods: Capturing life as it is lived. Annual Review of Psychology, 54, 579–616. doi:10.1146/annurev.psych.54.101601145030.
†*Bor, W., Sanders, M. R., & Markie-Dadds, C. (2002). The effects of the triple P-positive parenting program on preschool children with co-occurring disruptive behavior and attentional/hyperactive difficulties. Journal of Abnormal Child Psychology, 30(6), 571-587. doi:10.1023/A:1020807613155.
Boyle, C. L., & Lutzker, J. R. (2011). A quantitative analysis of generalization outcomes found in behavioral parent training programs for reduction of child problem behavior. International Journal of Child and Adolescent Health, 4, 7–15.
†*Boyle, C. L., Sanders, M. R., Lutzker, J. R., Prinz, R. J., Shapiro, C., & Whitaker, D. J. (2010). An analysis of training, generalization, and maintenance effects of primary care Triple P for parents of preschool-aged children with disruptive behavior. Child Psychiatry and Human Development, 41, 114–131. doi:10.1007/s10578-009-0156-7.
†*Brotman, L. M., Gouley, K. K., Chesir-Teran, D., Dennis, T., Klein, R. G., & Shrout, P. (2005). Prevention for preschoolers at high risk for conduct problems: Immediate outcomes on parenting practices and child social competence. Journal of Clinical Child and Adolescent Psychology, 34(4), 724–734. doi:10.1207/s15374424jccp3404_14.
†*Budd, K. S., Hella, B., Bae, H., Meyerson, D. A., & Watkin, S. C. (2011). Delivering parent-child interaction therapy in an urban community clinic. Cognitive and Behavioral Practice, 18(4), 502–514. doi:10.1016/j.cbpra.2010.12.002.
†*Bullard, L.,Wachlarowicz, M., DeLeeuw, J., Snyder, J., Low, S., Forgatch, M., DeGarmo, D. (2010). Effects of the Oregon model of Parent Management Training (PMTO) on marital adjustment in new stepfamilies: A randomized trial. Journal of Family Psychology, 24(4), 485–496.
†Calzada, E. J., Eyberg, S. M., Rich, B., & Querido, J. (2004). Parenting disruptive preschoolers: Experiences of mothers and fathers. Journal of Abnormal Child Psychology, 32(2), 203–213.
†Chacko, A., Wymbs, B. T., Flammer-Rivera, L. M., Pelham, W. E., Walker, K. S., Arnold, F. W., et al. (2008). A pilot study of the feasibility and efficacy of the strategies to enhance positive parenting (STEPP) program for single mothers of children with ADHD. Journal of Attention Disorders, 12(3), 270–280. doi:10.1177/1087054707306119.
†*Chacko, A., Wymbs, B. T., Wymbs, F. A., Pelham, W. E., Swanger-Gagne, M. S., Girio, E., et al. (2009). Enhancing traditional behavioral parent training for single mothers of children with ADHD. Journal of Clinical Child and Adolescent Psychology, 38(2), 206–218. doi:10.1080/15374410802698388.
†*Chamberlain, P., Price, J., Leve, L. D., Laurent, H., Landsverk, J. A., & Reid, J. B. (2008). Prevention of behavior problems for children in foster care: Outcomes and mediation effects. Prevention Science, 9, 17–27. doi:10.1007/s11121-007-0080-7.
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology, 66(1), 7–18.
Chorpita, B. F., & Weisz, J. R. (2009). Modular approach to therapy for children with anxiety, depression, trauma, or conduct problems (MATCH-ADTC). Satellite Beach, FL: PracticeWise, LLC.
†*Chronis-Tuscano, A., O’Brien, K. A., Johnston, C., Jones, H. A., Clarke, T. L., Raggi, V. L., et al. (2011). The relation between maternal ADHD symptoms & improvement in child behavior following brief behavioral parent training is mediated by change in negative parenting. Journal of Abnormal Child Psychology, 39(7), 1047–1057. doi:10.1007/s10802-011-9518-2.
†*Conduct Problems Prevention Research Group (2002). Evaluation of the first 3 years of the fast track prevention trial with children at high risk for adolescent conduct problems. Journal of Abnormal Child Psychology, 30, 19–35. doi:10.1023/A:1014274914287.
†*Conduct Problems Prevention Research Group. (2004). The effects of the fast track program on serious problem outcomes at the end of elementary school. Journal of Clinical Child and Adolescent Psychology, 33(4), 650–661. doi:10.1207/s15374424jccp3304_1.
†*Cummings, J. G., & Wittenberg, J. (2008). Supportive expressive therapy–parent child version: An exploratory study. Psychotherapy: Theory, Research, Practice, 45(2), 148–164. doi:10.1037/0033-3204.45.2.148.
†*Danforth, J. S., Harvey, E., Ulaszek, W. R., & McKee, T. E. (2006). The outcome of group parent training for families of children with attention-deficit hyperactivity disorder and defiant/aggressive behavior. Journal of Behavior Therapy and Experimental Psychiatry, 37(3), 188–205. doi:10.1016/j.jbtep.2005.05.009.
†*DeGarmo, D. S., Chamberlain, P., Leve, L. D., & Price, J. (2009). Foster parent intervention engagement moderating child behavior problems and placement disruption. Research on Social Work Practice, 19:4, 423–433. doi:10.1177/1049731508329407.
†*DeGarmo, D. S., Patterson, G. R., & Forgatch, M. S. (2004). How do outcomes in a specified parent training intervention maintain or wane over time? Prevention Science, 5(2), 73–89.
†*Delaney, E. M., & Kaiser, A. P. (2001). The effects of teaching parents blended communication and behavior support strategies. Behavioral Disorders, 26(2), 93–116.
†*Drugli, M. B., & Larsson, B. (2006). Children aged 4–8 years treated with parent training and child therapy because of conduct problems: Generalisation effects to day-care and school settings. European Child & Adolescent Psychiatry, 15(7), 392–399. doi:10.1007/s00787-006-0546-3.
†*Drugli, M. B., Larsson, B., & Clifford, G. (2007). Changes in social competence in young children treated because of conduct problems as viewed by multiple informants. European Child & Adolescent Psychiatry, 16(6), 370–378. doi:10.1007/s00787-007-0609-0.
†*Eames, C., Daley, D., Hutchings, J., Whitaker, C. J., Jones, K., Hughes, J. C., & Bywater, T. (2009). Treatment fidelity as a predictor of behaviour change in parents attending group-based parent training. Child: Care, Health and Development, 35(5), 603–612. doi:10.1111/j.1365-2214.2009.00975.x.
Ebner-Priemer, U. W., & Trull, T. J. (2009). Ambulatory assessment: An innovative and promising approach for clinical psychology. European Psychologist, 24(2), 109–119. doi:10.1027/1016-9040.14.2.109.
†*Eyberg, S. M., Funderburk, B. W., Hembree-Kigin, T. L., McNeil, C. B., Querido, J. G., & Hood, K. K. (2001). Parent-child interaction therapy with behavior problem children: One and two year maintenance of treatment effects in the family. Child & Family Behavior Therapy, 23(4), 1–20. doi:10.1300/J019v23n04_01.
Eyberg, S. M., Nelson, M. M., & Boggs, S. R. (2008). Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. Journal of Clinical Child & Adolescent Psychology, 37(1), 215–237. doi:10.1080/15374410701820117.
Eyberg, S. M., Nelson, M., M., Duke, M., & Boggs, S. R. (2005). Manual for the dyadic parent-child interaction coding system (3rd ed.).
†Fabiano, G. A., Chacko, A., Pelham, W. E., Robb, J., Walker, K. S., Wymbs, F., et al. (2009). A comparison of behavioral parent training programs for fathers of children with attention-deficit/hyperactivity disorder. Behavior Therapy, 40(2), 190–204. doi:10.1016/j.beth.2008.05.002.
†*Farrell, A. D., Meyer, A. L., & White, K. S. (2001). Evaluation of Responding in Peaceful and Positive Ways (RIPP): A school-based prevention program for reducing violence among urban adolescents. Journal of Clinical Child Psychology, 30(4), 451–463.
†Feinfield, K. A., & Baker, B. L. (2004). Empirical support for a treatment program for families of young children with externalizing problems. Journal of Clinical Child and Adolescent Psychology, 33(1), 182–195.
†Feldman, M. A., & Werner, S. E. (2002). Collateral effects of behavioral parent training on families of children with developmental disabilities and behavior disorders. Behavioral Interventions, 17, 75–83.
†Fernandez, M. A., & Eyberg, S. M. (2009). Predicting treatment and follow-up attrition in parent–child interaction therapy. Journal of Abnormal Child Psychology, 37(3), 431–441. doi:10.1007/s10802-008-9281-1.
†*Forgatch, M. S., DeGarmo, D. S., & Beldavs, Z. G. (2005). An efficacious theory-based intervention for stepfamilies. Behavior Therapy, 36(4), 357–365. doi:10.1016/S0005-7894(05)80117-0.
†*Forgatch, M. S., Patterson, G. R., & DeGarmo, D. S. (2005). Evaluating fidelity: Predictive validity for a measure of competent adherence to the Oregon model of parent management training. Behavior Therapy, 36, 3–13. doi:10.1016/S0005-7894(05)80049-8.
Funderburk, B., & Eyberg, S. M. (2011). Parent-child interaction therapy. In J. C. Norcross, G. R. VandenBos, & D. K. Freedheim (Eds.), History of psychotherapy: Continuity and change (2nd ed., pp. 415–420). Washington, DC: American Psychological Association.
†*Gardner, F., Burton, J., & Klimes, I. (2006). Randomised controlled trial of a parenting intervention in the voluntary sector for reducing child conduct problems: Outcomes and mechanisms of change. Journal of Child Psychology and Psychiatry, 47(11), 1123–1132. doi:10.1111/j.1469-7610.2006.01668.x.
†*Gardner, F., Hutchings, J., Bywater, T., & Whitaker, C. (2010). Who benefits and how does it work? moderators and mediators of outcome in an effectiveness trial of a parenting intervention. Journal of Clinical Child and Adolescent Psychology, 39(4), 568–580. doi:10.1080/15374416.2010.486315.
†*Hahlweg, K., Heinrichs, N., Kuschel, A., Bertram, H., & Naumann, S. (2010). Long-term outcome of a randomized controlled universal prevention trial through a positive parenting program: Is it worth the effort? Child and Adolescent Psychiatry and Mental Health, 4(14), 1–14. doi:10.1186/1753-2000-4-14.
†Harwood, M. D., & Eyberg, S. M. (2004). Therapist verbal behavior early in treatment: Relation to successful completion of parent-child interaction therapy. Journal of Clinical Child and Adolescent Psychology, 33(3), 601–612. doi:10.1207/s15374424jccp3303_17.
†*Hawes, D. J., & Dadds, M. R. (2005). The treatment of conduct problems in children with callous-unemotional traits. Journal of Consulting and Clinical Psychology, 73(4), 737–741. doi:10.1037/0022-006X.73.4.737.
†*Hawes, D. J., & Dadds, M. R. (2006). Assessing parenting practices through parent-report and direct observation during parent-training. Journal of Child and Family Studies, 15(5), 555–568. dio:10.1007/s10826-006-9029-x.
†*Hutchings, J., Bywater, T., Davies, C., & Whitaker, C. (2006). Do crime rates predict the outcome of parenting programmes for parents of ‘high-risk’ preschool children? Educational and Child Psychology, 23(2), 15–24.
†*Hutchings, J., Gardner, F., Bywater, T., Daley, D., Whitaker, C., Jones, K., et al. (2007). Parenting intervention in sure start services for children at risk of developing conduct disorder: Pragmatic randomised controlled trial. BMJ: British Medical Journal, 334(7595), 678–678. doi:10.1136/bmj.39126.620799.55.
†*Hutchings, J., Lane, E., Owen, R. E., & Gwyn, R. (2004). The introduction of the Webster-Stratton Incredible Years Classroom Dinosaur School Programme in Gwynedd, North Wales: A pilot study. Educational and Child Psychology, 21(4), 4–15.
†Jensen, S. A., & Grimes, L. K. (2010). Increases in parent attendance to behavioral parent training due to concurrent child treatment groups. Child & Youth Care Forum, 39(4), 239–251. doi:10.1007/s10566-010-9101-y.
†*Jones, K., Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2007). Efficacy of the Incredible Years Basic parent training programme as an early intervention for children with conduct problems and ADHD. Child: Care, Health and Development, 33(6), 749–756. doi:10.1111/j.1365-2214.2007.00747.x.
Kaminski, J. W., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36(4), 567–589. doi:10.1007/s10802-007-9201-9.
Kazdin, A. E. (2003). Problem-solving skills training and parent management training for conduct disorder. In A. E. Kazdin & J. R. Weisz (Eds.), Evidence-based psychotherapies for children and adolescents (pp. 241–262). New York: Guildford.
†Kling, A., Forster, M., Sundell, K., & Melin, L. (2010). A randomized controlled effectiveness trial of parent management training with varying degrees of therapist support. Behavior Therapy, 41, 530–542. doi:10.1016/j.beth.2010.02.004.
Knutson, N. M., Forgatch, M. S., & Rains, L. A. (2003). Fidelity of Implementation Rating System (FIMP): The training manual for PMTO. Eugene: Oregon Social Learning Center.
†*Leathers, S. J., Spielfogel, J. E., McMeel, L. S., & Atkins, M. S. (2011). Use of a parent management training intervention with urban foster parents: A pilot study. Children and Youth Services Review, 33(7), 1270–1279. doi:10.1016/j.childyouth.2011.02.022.
†*Leung, C., Tsang, S., Heung, K., & Yiu, I. (2009). Effectiveness of Parent—Child interaction therapy (PCIT) among Chinese families. Research on Social Work Practice, 19(3), 304–313. doi:10.1177/1049731508321713.
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Thousand Oaks: Sage.
†*Lyon, A. R., & Budd, K. S. (2010). A community mental health implementation of Parent–Child interaction therapy (PCIT). Journal of Child and Family Studies, 19(5), 654–668. doi:10.1007/s10826-010-9353-z.
†Marchant, M., & Young, K. (2001). The effects of a parent coach on parents’ acquisition and implementation of parenting skills. Education & Treatment of Children, 24, 351–373.
†*Marchant, M., Young, K., & West, R. P. (2004). The effects of parental teaching on compliance behavior of children. Psychology in the Schools, 41, 337–350. doi:10.1002/pits.10165.
†*Marcus, B. A., Swanson, V., & Vollmer, T. R. (2001). Effects of parent training on parent and child behavior using procedures based on functional analysis. Behavioral Interventions, 16, 87–104. doi:10.1002/bin.87.
†*Martinez, C. R., & Forgatch, M. S. (2001). Preventing problems with boys’ noncompliance: Effects of a parent training intervention for divorcing mothers. Journal of Consulting and Clinical Psychology, 69, 416–428. doi:10.1037/0022-006X.69.3.416.
†*McCabe, K., & Yeh, M. (2009). Parent-child interaction therapy for Mexican Americans: A randomized clinical trial. Journal of Clinical Child and Adolescent Psychology, 38(5), 753–759. doi:10.1080/15374410903103544.
†*McGilloway, S., Mhaille, G. N., Bywater, T., Furlong, M., Leckey, Y., Kelly, P., et al. (2012). A parenting intervention for childhood behavioral problems: A randomized controlled trial in disadvantaged community-based settings. Journal of Consulting and Clinical Psychology, 80(1), 116–127. doi:10.1037/a0026304.
McLeod, B. D., & Weisz, J. (2005). The Therapy Process Observational Coding Sytem-Alliance Scale: Measure characteristics and prediction of outcome in usual clinical practice. Journal of Consulting and Clinical Psychology, 73(2), 323–333. doi:10.1037/0022-006X.73.2.323.
McNeil, C., & Hembree-Kigin, T. (2011). Parent-child interaction therapy (2nd ed.). New York: Springer.
†*Miles, N. I., & Wilder, D. A. (2009). The effects of behavioral skills training on caregiver implementation of guided compliance. Journal of Applied Behavior Analysis, 42, 405–410. doi:10.1901/jaba.2009.42-405.
†*Nash, J. K., Fraser, M. W., Galinsky, M. J., & Kupper, L. L. (2003). Early development and pilot testing of a problem-solving skills-training program for children. Research on Social Work Practice, 13(4), 432-450. doi:10.1177/1049731503013004002.
†*Nixon, R. D. V., Sweeney, L., Erickson, D. B., & Touyz, S. W. (2003). Parent-child interaction therapy: A comparison of standard and abbreviated treatments for oppositional defiant preschoolers. Journal of Consulting and Clinical Psychology, 71(2), 251–260. doi:10.1037/0022-006X.71.2.251.
†*Nixon, R. D. V., Sweeney, L., Erickson, D. B., & Touyz, S. W. (2004). Parent-child interaction therapy: One- and two-year follow-up of standard and abbreviated treatments for oppositional preschoolers. Journal of Abnormal Child Psychology, 32(3), 263–271. doi:10.1023/B:JACP.0000026140.60558.05.
Nock, M. K., & Ferriter, C. (2005). Parent management of attendance and adherence in child and adolescent therapy: A conceptual and empirical review. Clinical Child and Family Psychology Review, 8(2), 149–166. doi:10.1007//s10567-005-4753-0.
†Nock, M. K, & Kazdin, A. E. (2005). Randomized controlled trial of a brief intervention for increasing participation in parent management training. Journal of Consulting and Clinical Psychology, 73, 872–879. doi:10.1037/0022-006X.73.5.872.
Nock, M. K., & Photos, V. (2006). Parent motivation to participate in treatment: Assessment and prediction of subsequent participation. Journal of Child and Family Studies, 15(3), 345–358. doi:10.1007/s10826-006-9022-4.
†*O’Callaghan, P. M., Reitman, D., Northup, J., Hupp, S. D. A., & Murphy, M. A. (2003). Promoting social skills generalization with ADHD-diagnosed children in a sports setting. Behavior Therapy, 34, 313–330. doi:10.1016/S0005-7894(03)80003-5.
†*Ogden, T., & Hagen, K. A. (2008). Treatment effectiveness of parent management training in Norway: A randomized controlled trial of children with conduct problems. Journal of Consulting and Clinical Psychology, 76, 607–621. doi:10.1037/0022-006X.76.4.607.
Ollendick, T. H., King, N. J., & Chorpita, B. F. (2006). Empirically supported treatments for children and adolescents. In P. C. Kendall (Ed.), Child and adolescent therapy: Cognitive-behavioral procedures (pp. 492–520). New York: Guilford.
Orwin, R. G. (1983). A fail-safe N for effect size in meta-analysis. Journal of Educational Statistics, 8, 157–159.
Patterson, G. R., Reid, J. B., Jones, R. R., & Conger, R. E. (1975). A social learning approach to family intervention: Families with aggressive children (Vol. 1). Eugene, OR: Castilia.
†*Pearl, E., Thieken, L., Olafson, E., Boat, B., Connelly, L., Barnes, J., et al. (2011). Effectiveness of community dissemination of parent–child interaction therapy. doi:10.1037/a0022948.
†*Plant, K. M., & Sanders, M. R. (2007). Reducing problem behavior during care-giving in families of preschool-aged children with developmental disabilities. Research in Developmental Disabilities, 28(4), 362–385. doi:10.1016/j.ridd.2006.02.009.
†*Presley, J. A., & Hughes, C. (2000). Peers as teachers of anger management to high school students with behavioral disorders. Behavioral Disorders, 25(2), 114–130.
†*Reid, M. J., Webster-Stratton, C., & Baydar, N. (2004). Halting the development of conduct problems in head start children: The effects of parent training. Journal of Clinical Child and Adolescent Psychology, 33(2), 279–291. doi:10.1207/s15374424jccp3302_10.
†*Reid, M. J., Webster-Stratton, C., & Beauchaine, T. P. (2001). Parent training in head start: A comparison of program response among African American, Asian American, Caucasian, and Hispanic mothers. Prevention Science, 2(4), 209–227. doi:10.1023/A:1013618309070.
†*Reid, M. J., Webster-Stratton, C., & Hammond, M. (2007). Enhancing a classroom social competence and problem-solving curriculum by offering parent training to families of moderate- to high-risk elementary school children. Journal of Clinical Child and Adolescent Psychology, 36(4), 605–620.
Reis, H. T., & Gable, S. L. (2000). Event sampling and other methods for studying everyday experience. In H. T. Reis & C. M. Judd (Eds.), Handbook of research methods in social and personality psychology (pp. 190–222). New York: Cambridge University Press.
†Research Units on Pediatric Psychopharmacology (RUPP) Autism Network. (2007). Parent training for children with pervasive developmental disorders: A multi-site feasibility trial. Behavioral Interventions, 22, 179–199. doi:10.1002/bin.236z.
Reyno, S. M., & McGrath, P. J. (2006). Predictors of parent training efficacy for child externalizing behavior problems: A meta-analytic review. Journal of Child Psychology and Psychiatry, 47(1), 99–111. doi:10.1111/j.1469-7610.2005.01544.x.
†*Roberts, C., Mazzucchelli, T., Studman, L., & Sanders, M. R. (2006). Behavioral family intervention for children with developmental disabilities and behavioral problems. Journal of Clinical Child and Adolescent Psychology, 35(2), 180–193. doi:10.1207/s15374424jccp3502_2.
Rosenthal, R., & DiMatteo, M. R. (2001). Meta-analysis: Recent developments in quantitative methods for literature reviews. Annual Review of Psychloy, 52, 59–82. doi:10.1146/annurev.psych.52.1.59.
†*Sanders, M. R., Bor, W., & Morawska, A. (2007). Maintenance of treatment gains: A comparison of enhanced, standard, and self-directed triple P-positive parenting program. Journal of Abnormal Child Psychology, 35(6), 983–998. doi:10.1007/s10802-007-9148-x.
†*Sanders, M. R., Markie-Dadds, C., Tully, L. A., & Bor, W. (2000). The triple P-positive parenting program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology, 68(4), 624–640. doi:10.1037/0022-006X.68.4.624.
†*Scott, S., O’Connor, T. G., Futh, A., Matias, C., Price, J., & Doolan, M. (2010). Impact of a parenting program in a high-risk, multi-ethnic community: The PALS trial. Journal of Child Psychology and Psychiatry, 51(12), 1331–1341. doi:10.1111/j.1469-7610.2010.02302.x.
†*Scott, S., Sylva, K., Doolan, M., Price, J., Jacobs, B., Crook, C., et al. (2010). Randomised controlled trial of parent groups for child antisocial behaviour targeting multiple risk factors: The SPOKES project. Journal of Child Psychology and Psychiatry, 51(1), 48–57. doi:10.1111/j.1469-7610.2009.02127.x.
†*Shanley, J. R., & Niec, L. N. (2010). Coaching parents to change: The impact of in vivo feedback on parents’ acquisition of skills. Journal of Clinical Child and Adolescent Psychology, 39(2), 282–287. doi:10.1080/15374410903532627.
Stone, A. A., & Shiffman, S. (1994). Ecological momentary assessment (EMA) in behavioral medicine. Annals of Behavioral Medicine, 16, 199–202.
†*Thornberry, T., & Brestan-Knight, E. (2011). Analyzing the utility of dyadic parent-child interaction coding system (DPICS) warm-up segments. Journal of Psychopathology and Behavioral Assessment, 33(2), 187–195. doi:10.1007/s10862-011-9229-6.
†*Timmer, S. G., Ho, L. K. L., Urquiza, A. J., Zebell, N. M., & Boys, D. (2011). The effectiveness of parent–child interaction therapy with depressive mothers: The changing relationship as the agent of individual change. Child Psychiatry and Human Development, 42(4), 406–423. doi:10.1007/s10578-011-0226-5.
†*Timmer, S. G., Zebell, N. M., Culver, M. A., & Urquiza, A. J. (2010). Efficacy of adjunct in-home coaching to improve outcomes in parent–child interaction therapy. Research on Social Work Practice, 20(1), 36–45. doi:10.1177/1049731509332842.
†*Turner, K. M. T., & Sanders, M. R. (2006). Help when it’s needed first: A controlled evaluation of brief, preventive behavioral family intervention in a primary care setting. Behavior Therapy, 37(2), 131–142. doi:10.1016/j.beth.2005.05.004.
†Ware, L. M., McNeil, C. B., Masse, J., & Stevens, S. (2008). Efficacy of in-home parent-child interaction therapy. Child & Family Behavior Therapy, 30(2), 99–126. doi:10.1080/07317100802060302.
Webster-Stratton, C., & Reid, M. (2003). The Incredible Years parents, teachers, and children training series: A multifaceted treatment approach for young children with conduct problems. In A. E. Kazdin & J. R. Weisz (Eds.), Evidence-based psychotherapies for children and adolescents (pp. 224–240). New York: Guildford.
†*Webster-Stratton, C., Reid, M. J., & Beauchaine, T. (2011). Combining parent and child training for young children with ADHD. Journal of Clinical Child and Adolescent Psychology, 40(2), 191–203. doi:10.1080/15374416.2011.546044.
†*Webster-Stratton, C., Reid, M. J., Hammond, M. (2001a). Preventing conduct problems, promoting social competence: A parent and teacher training partnership in head start. Journal of Clinical Child Psychology. 30(3), 283–302.
†*Webster-Stratton, C., Reid, J., & Hammond, M. (2001b). Social skills and problem-solving training for children with early-onset conduct problems: Who benefits? Journal of Child Psychology and Psychiatry, 42(7), 943–952.
†*Webster-Stratton, C., Reid, M. J., & Stoolmiller, M. (2008). Preventing conduct problems and improving school readiness: Evaluation of the Incredible Years teacher and child training programs in high-risk schools. Journal of Child Psychology and Psychiatry, 49(5), 471–488. doi:10.1111/j.1469-7610.2007.01861.x.
†*Webster-Stratton, C., Rinaldi, J., & Reid, J. M. (2011). Long-term outcomes of Incredible Years parenting program: Predictors of adolescent adjustment. Child and Adolescent Mental Health, 16(1), 38–46. doi:10.1111/j.1475-3588.2010.00576.x.
Weisz, J. R., Jensen-Doss, A., & Hawley, K. M. (2006). Evidence-based youth psychotherapies versus usual clinical care: A meta-analysis of direct comparisons. American Psychologist, 61(7), 671–689. doi:10.1037/0003-066X.61.7.671.
Weisz, J. R., Weiss, B., Alicke, M. D., & Klotz, M. L. (1987). Effectiveness of psychotherapy with children and adolescents: A meta-analysis for clinicians. Journal of Consulting and Clinical Psychology, 55(4), 542–549.
Weisz, J. R., Weiss, B., Han, S. S., Granger, D. A., & Morton, T. (1995). Effects of psychotherapy with children and adolescents revisited: A meta-analysis of treatment outcome studies. Psychological Bulletin, 117(3), 450–468.
†Werba, B. E., Eyberg, S. M., Boggs, S. R., & Algina, J. (2006). Predicting outcome in parent-child interaction therapy: Success and attrition. Behavior Modification, 30(5), 618–646. doi:10.1177/0145445504272977.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
Study-Level Codes
Bibliographic Reference (APA)
-
1.
Study ID #. Assign a unique identification # to each study. Formatted as TX# (PCI 01, PCI 02, IYR 01, IYR 02, etc.)
- BPT:
-
Behavioral parent training
- FTR:
-
Fast Track
- IYR:
-
Incredible years
- KEE:
-
KEEP
- PCI:
-
PCIT
- PMT:
-
PMT/PMTO
- PPP:
-
Triple P
- OTH:
-
Other (includes BCBS, BMFC, BST, Making choices, Positive parenting, RIPP, Social skills training, TEAM, and Walker social skills)
-
2.
Paper #. Assign each manuscript a unique #. Number in order from 1 to 85.
-
3.
Publication year (last two digits).
Sample Descriptors
-
4.
Mean age of sample at the beginning of the intervention (missing = 999).
-
5.
Description of sample (eligibility criteria, severity of symptoms, etc.):
Research Design Descriptors
-
6.
Method of assignment to conditions (random, non-random).
- 1:
-
random
- 2:
-
non-random
- 9:
-
cannot tell
- 0:
-
no control group
-
7.
Total sample size (start of study)
-
8.
Treatment group sample size (start of study)
-
9.
Control group sample size (start of study; no control = 0)
Nature of the Treatment Descriptors
-
10.
Intervention name
-
1
Behavioral parent training
-
2
Fast Track
-
3
Incredible years
-
4
KEEP
-
5
PCIT
-
6
PMT/PMTO
-
7
Triple P
-
8
Other (Definition: includes BCBS, BMFC, BST, Making choices, Positive parenting, RIPP, Social skills training, TEAM, and Walker social skills)
-
1
-
11.
Intervention type
-
1
treatment
-
2
prevention
-
1
-
12.
Intervention target
-
1
parent
-
2
child
-
1
-
13.
Avg # of sessions for treatment group (missing = 999)
-
14.
Nature of control group
-
1
receives nothing (Definition: no evidence of any treatment)
-
2
wait list (Definition: delayed treatment control, etc.)
-
3
treatment as usual (Definition: control receives the usual treatment for DBD without special enhancement that constitutes the treatment of interest)
-
4
alternative treatment (Definition: control is not really a control but another treatment [other than usual treatment] being compared with the focal treatment)
- 9:
-
cannot tell
- 0:
-
no control group
-
1
Appendix 2
Effect Size Level Codes
-
1.
Study ID #
-
2.
Paper #
-
3.
Effect size #. Assign each effect size within a study a unique #. Number multiple effect sizes within a study sequentially (e.g., 1, 2, 3, 4…)
Dependent Measure Descriptors
-
4.
Type of skill-use
- 1:
-
acquisition
- 2:
-
utilization
-
5.
Parent or child skill
-
1
parent skill
-
2
child skill
-
1
-
6.
Description of skill:
-
7.
Category of skill:
-
1
Positive parenting (Definition: study measure is a composite of multiple positive parenting behaviors, such as praise, positive affect, encouragement, positive reflections/descriptions of child behavior, and problem-solving)
-
2
Negative parenting (Definition: study measure is a composite of multiple negative parenting behaviors, such as criticism, negative physical contact, vague instructions, vague commands, and interruptions)
-
3
Parent praise (Definition: measures verbal and nonverbal affirmation of child)
-
4
Parent verbal/nonverbal communication (Definition: measures increase in positive or decrease in negative verbalizations, social attention, or physical touch)
-
5
Parent positive/negative consequences (Definition: measures effective use of consequences)
-
6
Parent other (Definition: includes measures of monitoring, balance of turns, problem-solving, and broad treatment skills that are not clearly described)
-
7
Child emotion labeling (Definition: measures identification of positive or negative feelings)
-
8
Child problem-solving (Definition: measures positive strategies to address social problems)
-
9
Child anger management (Definition: measures strategies for controlling anger such as relaxation techniques)
-
10
Child social skills (Definition: measures understanding of social cues or appropriate engagement with peers)
-
11
Child other (Definition: includes measures of broad treatment skills that are not clearly described)
-
1
-
8.
Statistical nature of skill
- 1:
-
continuous
- 2:
-
dichotomous
- 3:
-
artificial dichotomous
- 4:
-
ordinal
-
9.
Skill compared to treatment outcome (e.g., child externalizing behavior)?
- 1:
-
yes
- 0:
-
no
-
10.
Effect size type
- 1:
-
pre–post
- 2:
-
treatment–control (at post)
Effect Size Data
-
11.
Type of data effect size based on
- 1:
-
means and SDs
- 2:
-
t value or F value
- 3:
-
Chi-square (df = 1)
- 4:
-
frequencies or proportions
-
12.
Page number where data found
-
13.
Pre–post score correlation Only needed if effect size type is “pre–post” (i.e., #9 is coded as 1). If not needed (i.e., #9 is coded as 2), enter 999
When means and standards deviations are reported or can be estimated (**NOTE: for pre–post effect size comparisons, report post-data where it says “treatment group” and pre-data where it says “control group”):
- 14a.:
-
Treatment group sample size (or post-sample size; NA = 999)
- 14b.:
-
Control group sample size (or pre-sample size; NA = 999)
- 15a.:
-
Treatment group mean (or post-mean; NA = 999)
- 15b.:
-
Control group mean (or pre-mean; NA = 999)
- 16a.:
-
Treatment group SD (or post-SD; NA = 999)
- 16b.:
-
Control group SD (or pre-SD; NA = 999)
When proportions or frequencies are reported or can be estimated (**NOTE: for pre–post effect size comparisons, report post-data where it says “treatment group” and pre-data where it says “control group”):
- 17a:
-
n of treatment group with a successful outcome (or n at post; NA = 999)
- 17b.:
-
n of control group with a successful outcome (or n at pre; NA = 999)
- 18a.:
-
Proportion of treatment group with a successful outcome (or proportion at post; NA = 999)
- 18b.:
-
Proportion of control group with a successful outcome (or proportion at pre; NA = 999)
When significance test information is reported:
- 19a.:
-
t value (NA = 999)
- 19b.:
-
F value (NA = 999)
- 19c.:
-
Chi-square value (NA = 999)
Calculated Effect Size
- 20:
-
Effect size (NA = 999)
Rights and permissions
About this article
Cite this article
Lindhiem, O., Higa, J., Trentacosta, C.J. et al. Skill Acquisition and Utilization During Evidence-Based Psychosocial Treatments for Childhood Disruptive Behavior Problems: A Review and Meta-analysis. Clin Child Fam Psychol Rev 17, 41–66 (2014). https://doi.org/10.1007/s10567-013-0136-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10567-013-0136-0