
Abstract
Background
The reported prevalence of depression and anxiety among African American children and adolescents and their negative sequalae suggest a need to further explore factors that may be protective of depression and anxiety among this population.
Objective
The aim of this review was to examine empirical studies that focus on the association between family-level factors (e.g., parenting practices, family functioning) and depression and anxiety in African American children. Specifically, we examined the studies’ characteristics and the relationship between various family-level factors and depression and anxiety outcomes and assessed the methodological quality of studies.
Methods
This review was guided by systematic review methods postulated by Gough and colleagues and the Prisma Group. Electronic databases searched were Social Work Abstracts, PsycINFO, SocIndex, PubMed, Social Service Abstracts, and Sociological Abstracts. Thirty-one studies published from 2003 to 2014 were included and assessed for methodological strength using the Quantitative Research Assessment Tool.
Results
The majority of the study samples were low income and resided in metropolitan or urban areas, and primary caregivers were female. Parenting practices (58 % of studies) were by far the most frequently examined family-level factor associated with depression and anxiety.
Conclusion
Positive family-level factors (e.g., positive parenting, healthy family functioning and environment) was associated with decreased depression and anxiety. Findings from this review can inform the development or adaptation of family-based interventions that can effectively reduce depression and anxiety symptoms in African American children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Childhood and adolescence have been identified as a significant time of susceptibility to mental health problems. Indeed, Kessler et al. (2005) report that 50 % of the lifetime occurrences of mental disorders have an onset at age 14 and that 75 % begin by the age of 24, suggesting that mental disorders at this stage has implications for problems into adulthood (Copeland et al. 2009). Other research has shown that approximately one in five children and adolescents experience significant symptoms of emotional distress (Knopf et al. 2008) and that 10 % of children and adolescents suffer from emotional disorders, including depression and anxiety, that impair their personal, school, and family lives (Knopf et al. 2008; U.S. Department of Health and Human Services [USDHHS] 1999). Among children and adolescents, depression is widely studied because of its contribution to the global disease burden (Merry et al. 2004); however, both anxiety and depression have been commonly reported among youth (Knopf et al. 2008). For example, over two million children, aged 12–17, experienced a major depressive disorder during 2014 (Center for Behavioral Health Statistics and Quality [CBHSQ] 2015), and lifetime prevalence rates have been reported around 11.7 % (Merikangas et al. 2010). An even greater lifetime prevalence of 32 % (Merikangas et al. 2010) and 12-month prevalence ranging from 8.6 to 20.9 % (Costello et al. 2005) has been reported for anxiety.
Further, depression and anxiety have been reported to co-occur (Costello et al. 2005; Hjemdal et al. 2007), which compounds the effect of both in the lives of youth. Among racial and ethnic subgroups of youth, early symptoms of both disorders have been linked to later adolescent depression (Canals et al. 2002), adult mental disorders (e.g., Copeland et al. 2009), and poor academic functioning (Birmaher et al. 2004; Fergusson and Woodward 2002; Rothon et al. 2009). Similarly, depression has also been shown to be correlated with suicide attempts (Center for Substance Abuse Treatment 2008) and lower levels of education and self-worth (Franko et al. 2005), while anxiety increases the risk for substance use and lower social interaction (Anxiety and Depression Association of America 2016). In studies that examined African American populations, depression has also been linked to aggressive behavior, attention problems, and lower academic functioning (Steele et al. 2000).
Research on differences in patterns of depression and anxiety among racial or ethnic groups of adolescents is discrepant (Austin and Chorpita 2004). Some studies have reported greater depressive symptoms among non-White adolescents (e.g., Rushton et al. 2002). Kessler et al. (2012) report somewhat similar rates of lifetime depression (11.2–11.1) among non-Hispanic Black and White youth, respectively, and slightly higher rates of 12-month depression among non-Hispanic Black youth (8.8) compared with non-Hispanic White youth (7.6). Other studies reported lower rates of major depression among Black adolescents compared with their White or Hispanic counterparts but greater reports of anxiety and comorbidity among Black youth than any other ethnic group (Chen et al. 2005). Similarly, increased rates of lifetime anxiety disorders have been reported among non-Hispanic Black adolescents (37.8) compared with non-Hispanic White adolescents (29.9) (Merikangas et al. 2010). However, Lewis et al. (2012) reported no differences in anxiety symptoms between African–American and White adolescents.
Notwithstanding, African American youth are disproportionately exposed to risk factors (e.g., poverty, negative life events, community violence, and discrimination) that may increase the risk of developing depression and anxiety (APA 2008; Lewis et al. 2012; McCabe et al. 1999). For example, considerably greater proportions of African American youth compared with White youth are living below the poverty line (DeNavas-Walt et al. 2009), and poverty has been shown to predict the onset of mental disorders (McLaughlin et al. 2011). Concomitantly, living in poorer neighborhoods, characterized by crime and violence, increases the risk of exposure to negative life events (e.g., community violence; Lewis et al. 2012) and may result in greater anxiety rates for African American youth (Cooley-Quille et al. 2001; Lewis et al. 2012; McCabe et al. 1999). Further, research has documented the adverse impact of racial discrimination on depression and anxiety among African American youth (e.g., Gaylord-Harden and Cunningham 2009; Neblett et al. 2008). Thus, these risk factors can influence the development of increased depression and anxiety, and in turn, increased implications for the negative sequalae associated with both disorders among African American youth.
Historically, a deficit-based framework has been emphasized as a means of understanding mental health with a focus on risk factors that contribute to negative outcomes among children (Loh and Wragg 2004). Specifically, research on African American children and adolescents have well-documented individual, sociohistorical, and contextual factors (e.g., poverty, substance misuse, delinquency, violence exposure, and discrimination) that place African American children and adolescents at risk of mental and behavior problems (e.g., APA 2008); however, the positive impact of family-level factors (e.g., parenting practices, family functioning) on anxiety and depression has received less attention. Exploring the influence of family-level factors on mental health outcomes is critical, given the importance of family to the development of children and adolescents. Children and adolescents do not develop in isolation. The social contexts within which they experience life and establish social relationships shape their behavioral and emotional development (Murray and Greenberg 2000). Family is regarded as the primary socialization agent during childhood and provides an important social context within which constant interactions shape developmental adjustment and functioning among children and adolescents (e.g., Grusec 2011; Knopf et al. 2008). Indeed, researchers have documented the importance of family factors on African American children’s social and academic outcomes (e.g., Washington et al. 2013; Washington et al. 2014), externalizing behavioral problems (Grant et al. 2000; Washington et al. 2015), psychosocial well-being outcomes (Rose et al. 2014), and internalizing difficulties (e.g., anxiety, depression; Margolin 2006).
To summarize, the negative sequalae of depression and anxiety and the reported prevalence among African American children and adolescents, coupled with the compounding effect of other social contexts, suggests a need to further explore factors that may be protective of depression and anxiety among this population (Hjemdal et al. 2007; Keyes 2006; Margolin 2006). Given the vital importance of family to child and adolescent development, the authors were interested in identifying how family-level factors are related to depression and anxiety among African American children. Accordingly, the main aim of this review is to explore associations between family-level factors and depression and anxiety among African American children. Specifically, we examined the studies’ characteristics (e.g., design, sample demographics, instrumentation) and the relationship between various family-level factors and depression and anxiety outcomes and we assessed the methodological quality of studies. We expect that positive family-level factors (e.g., positive parenting practices, healthy family functioning and environments) will have a protective role in buffering depression and anxiety symptoms among African American children. Thus, the results of this review will provide avenues for prevention and intervention research, an essential resource for direct practice practitioners working with children and families, and inform clinical applications and policies designed to address depression and anxiety among this population.
Method
Eligibility Criteria
This review is guided by systematic review methods postulated by Gough et al. (2012) and Moher et al. (2009). The studies for this review were selected using the following inclusion criteria: (a) sample population is exclusively African Americans under age 18; (b) scholarly, empirical literature published between 2003 and 2014; (c) mental health outcomes including depression and anxiety; and (d) predictor variables are family-level factors (variables that refer to a family’s characteristics). This review included studies that focused exclusively on African American children, as such studies are most likely to include instruments designed specifically for or validated for this population. Studies excluded from this review include intervention studies not conducted in English and those involving children living outside the United States and children in specialized placements such as foster care or a detention center.
The database and protocol search strategies were developed by the research team in consultation with a university librarian, who specializes in systematic reviews. The databases searched for this review included Social Work Abstracts, PsycINFO, SocIndex, PubMed, Social Service Abstracts, and Sociological Abstracts. These databases were selected based on the aim of the review, as well as recommendations from the university librarian. For example, we included disciplinary topic-specific databases that contain relevant journals on children and families and mental health. In addition, databases were initially searched from August 2003 through September 2013, because the authors were interested in investigating studies within the past decade on the review’s topic. However, due to the time lapse between when databases were initially searched and when the review was submitted for publication, another database search was conducted from September 2013 to February 2014. We searched these databases for combinations of the following keywords and phrases: African American, Black, children, adolescence, youth, mental health, depression, anxiety, and psychological well-being. We also used wild card searches to capture different version of the words. The thesaurus tools available in databases were utilized to identify controlled terms for keywords and phrases when appropriate.
We also used additional methods to locate studies that may not have been identified by the database searches, such as reverse searches (i.e., citations and references of studies are examined). Further, an article located by the database revealed that in 2013 the Journal of Child and Family Studies published a special edition focused on the mental health of African American youth. Thus; due to the special edition’s focus, we reviewed every article in this edition to determine its eligibility for our review. To store and manage the wide range and volume of information collected for the review, we utilized RefWorks, an online research management program designed to help researchers gather, manage, and store information, as well as to generate citations and bibliographies (RefWorks 2009).
Study Selection
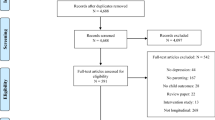
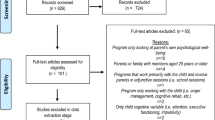
The searches initially identified 3874 studies; however, 1167 were removed because they were duplicates (see Fig. 1). The initial screening process consisted of research team members reviewing the titles and abstracts of studies, using the review’s protocol to establish whether they met the eligibility criteria. To help ensure reliability of the titles and abstracts screening process, a random spot-checking was conducted that included the calculation of Cohen’s kappa (Gough et al. 2012). Researchers’ results were compared and interrater agreement exceeded 90 %. Next, team members reviewed 387 full-text studies, and random spot checking and comparison of the results of this process revealed that the interrater agreement exceeded 90 %. The study selection process yielded 31 studies that met the inclusion criteria.

PRISMA diagram
Data Collection and Analysis
Following the review of full-text studies, the team members used a data extraction tool to independently code each study. This tool was developed by the leader of the research team in consultation with other team members, and it was pilot-tested by a research assistant. The tool was used to collect data on study design, sample characteristics, outcome measures, and key findings for each study. The tool, along with a companion codebook and discussions at team meetings, was used to clarify key constructs. In addition, we used a modified version of the Quantitative Research Assessment Tool, developed by Child Care and Early Education Research Connections (CCEERC n.d.), to assess the methodological strength of the studies included in our review.
Results
Study Characteristics
Of the 31 studies included in this systematic review, most had a cross-sectional design (n = 20; 65 %), while 11 (35 %) were longitudinal (see Table 1 for details). The majority of the study populations resided in urban or metropolitan areas (n = 24; 77 %) and had household incomes at or below the poverty line (n = 23; 74 %). Almost all of the studies (n = 27; 87 %) included in the review report that the gender of children who participated in the studies were nearly equally divided between male and female; however, two studies consisted of solely female participants (Coley 2003; Constantine 2006). Of the 31 studies included in the review, 27 (87 %) reported the mean age of the children, which was 12.7 years old, with an age range of 6–18 years old. Within this review, the majority of the studies identified women (e.g., mothers, grandmothers) as the primary caregivers, while some reported female-headed households. One study focused exclusively on adolescent mothers (Buckingham-Howes et al. 2011). However, for several studies it was unclear who the household members were and whether they included fathers or “father figures.”
Twenty-one (68 %) studies within this systematic review solely examined depression in African American children. Four (13 %) studies examined anxiety as the only mental health outcome, and six studies (19 %) examined both depression and anxiety. The Child Depression Inventory (n = 9; Kovacs 1981) was the most frequently used scale to measure children’s depressive symptoms, followed by the Center for Epidemiological Studies Depression Scale (n = 7; Radloff 1977). The State-Trait Anxiety Inventory for Children (n = 2; Spielberger et al. 1973) was the most frequently used scale to assess anxious symptoms.
Methodological Quality of Studies
A modified version of the Quantitative Research Assessment Tool assessed the methodological strength of the studies included in our review. The tool was designed to provide general guidelines evaluating the quality of research studies (see appendix for the full tool). Seven items (2, 5–7, 9–11) of the tool were germane for our assessment. Items 1 and 3 (population, sample) were not relevant, as all of our studies focused on a specific subset of the population (i.e., African American children). In addition, more than half of the studies were secondary analyses, so Item 4 (response/attrition rate) was excluded. Further, missing data may not have been addressed if all data were present, which was unclear in many cases. Each item could be rated −1, 0, 1, or NA; thus our scores could range from −7 to 7. Consistent with the specifications of the tool, studies with lower scores should be regarded with more caution compared with studies that have higher scores. The majority of our studies (87 %) had a score of 5 or above (see Table 1).
Family-Level Factors and Depression and Anxiety
Parenting Practices
Parenting practices were by far the most frequently examined family-level factor in the review. Of the 31 studies included in the review, 18 (58 %) examined the relationships between parenting practices and African American children’s depression and anxiety (see Table 2). Parenting practices were categorized into five subsets: parental monitoring, positive parenting (e.g., parental warmth, encouragement, and support; quality of parent–child relationship), discipline (e.g., corporal punishment/spanking), parental psychological and behavioral control, and other parenting characteristics. A few of the studies (n = 5) examined more than one parenting practice (see Table 2). Of the five subsets, parental monitoring and positive parenting were the most examined parenting characteristics in the studies.
Parental Monitoring
Of the studies that examined parental monitoring (4 of 31; 13 %), two studies found a significant association between parental monitoring and African American children’s depression levels (see Table 2). For example, Sagrestano et al. (2003) investigated the association between family risk factors and mental health outcomes and found that a decrease in parental monitoring was associated with increases in child’s depressive symptoms. Similarly, Tolou-Shams et al. (2007) suggested that children were less likely to display depressive symptoms (i.e., distress) during adolescence if mothers were more knowledgeable about their children’s whereabouts and peer groups and if they had had stricter house rules when children were younger.
Positive Parenting
Thirteen studies examined the impact of positive parenting on depression and anxiety among African American children (see Table 2). All of these studies (n = 13; 42 %) found a significant negative relationship between positive parenting and children’s anxiety and/or depression. For example parental support (Bean et al. 2006; Cooper et al. 2013), positive role models (e.g., mother/father; Bryant and Zimmerman 2003), and parental encouragement (Nebbitt and Lambert 2009) were all found to have a significant negative association with anxiety and/or depression. In addition, one study investigated interactions between maternal depressive symptoms and mother–child relationship quality and depressive symptoms among children of mothers with and without human immunodeficiency virus infection and acquired immune deficiency syndrome status (HIV/AIDS; McKee et al. 2007). This study found that lower depressive symptoms were observed for children of noninfected mothers when the mother–child relationship was categorized as warm and when mothers had lower levels of depression. Also, a warm and supportive mother–child relationship was associated with fewer depressive symptoms among children whose mothers were infected with HIV/AIDS and when maternal depressive symptoms were high. Furthermore, several studies provide knowledge about the relationships between positive parenting and anxiety and/or depression over time (e.g., Sagrestano et al. 2003; Tolou-Shams et al. 2007). For instance, Hammack et al. (2004a, b) longitudinal study examined the relationships among parent–child relationship, community violence and depressive and anxiety symptoms in inner-city African American children and adolescents. These researchers found that when maternal closeness was low, witnessing violence predicted higher anxiety. Similarly, high maternal closeness in the context of high witnessing of violence was associated with fewer depressive symptoms compared with children and adolescents reporting less maternal closeness in the context of high witnessing of violence.
Discipline and Parental Psychological and Behavior Control
Two studies found a significant positive relationship between corporal punishment and adolescent’s depression and/or anxiety (McLoyd et al. 2007; Simons et al. 2013). For example, Simons et al. (2013) suggest that corporal punishment in the absence of responsiveness (warmth) puts children at an increased risk for displaying depressive symptoms. Two out of the three studies that examined the relationship between parental psychological control (e.g., affection withdrawal and guilt introduction) and children’s depression and/or anxiety did not show a statistically significant relationship (Bean et al. 2006; Tolou-Shams et al. 2007). However, Mandara and Pikes (2008) found that there was a positive association only between parental psychological control and depressive symptoms in girls, even though both girls and boys reported the same level of parental psychological control. The one study that examined parental behavior control on children depressive symptoms was not significant (Bean et al. 2006).
Other Parenting Practices
Other parenting variables examined by researchers include maternal expressed emotions (a measure of specific aspects of one’s attitude toward others; Kwon et al. 2006) and parental attachment. Kwon et al. (2006) indicated a positive association between maternal expressed emotions and children’s anxiety symptoms. Constantine (2006) reported that the path between parental attachment and depressive symptoms was significant and negative; meaning African American girls who reported lower levels of parental attachment had greater levels of depression.
Other Family-Level Factors
Across the 31 studies examined in this review, 18 (58 %) investigated the contribution of family-level factors other than, or in addition to, parenting practices on adolescent’s depression and/or anxiety (see Table 3). We labeled these factors as other family-level factors and grouped them into five categories: family functioning (e.g., supportive and engaged family) and environment (e.g., type of home setting), family conflict and violence, parental mental health, family socioeconomic status, and presence or absence of adverse life events. The most frequently examined other family-level factors were family functioning and environment and family conflict and violence.
Family Functioning and Environment
Seven (23 %) studies examined the impact of family functioning and environment on African American children’s depression and/or anxiety, and several of these studies found significant associations. Gaylord-Harden et al. (2007) reported that perceived support from family members predicted fewer depressive and anxiety symptoms in children. In addition, Fitzpatrick et al. (2005) found that social capital (e.g., social relationships within the family) was negatively correlated with depressive symptoms, and Hall et al. (2008) found that being female and having low levels of family support were significant in predicting depression symptoms. Longitudinally, for girls time spent with family emerged as a protective factor over time for anxiety symptoms (Hammack et al. 2004a, b). This means girls who reported less time with family in the context of witnessing high violence at Time 1 reported a greater increase in anxiety at Time 2. Children and adolescences who were exposed to violence and reported spending more time with family also reported fewer depressive symptoms than youth who spent less time with family, revealing time with family as protective. However, for those with very high levels of exposure to violence, time with family did not protect youth from experiencing depressive symptoms.
Family Conflict and Violence
Six studies (19 %) examined the relationship between family conflict and violence and African American children’s depression and/or anxiety. Of these six studies, four focused on conflict, and one found that high mother–grandmother psychological conflict (e.g., insulting, swearing, shouting, threatening, name-calling, and destroying property) was a marginally significant predictor of children’s internalizing problems, resulting in depression and/or anxiety (Buckingham-Howes et al. 2011). Barton et al. (2015) highlighted that, for African American youth, escalated rates of change in interparental conflict predicted higher levels of youth depression. Similarly, Forehand and Jones (2003) found that lower levels of coparent conflict protected girls from depressive symptoms. Sagrestano et al. (2003) examined associations between family risk factors and children’s depression who reside in low-income urban areas. Their longitudinal study showed that increases in child reports of parent–child conflict and decreases in child reports of parental monitoring were concurrently associated with increases in child depression from Time 1 to Time 2.
Of the two studies that examined family violence and its relation to children’s depression and anxiety, only one had significant findings. Jenkins et al. (2009) found that family violence was significantly related to children’s depression and anxiety symptoms. This study also reported that having a family member (or friend) die or having that person injured in a nonviolent incident was not related to any adverse outcomes for girls, but it was inversely related to depression and anxiety symptoms for boys.
Family Socioeconomic Status
Two studies examined the relationship between family socioeconomic status and African American children’s depression. Taylor et al. (2014) found that financial pressure was positively associated with children’s depressive symptoms. Hammack et al. (2004a, b) found that females who scored higher on a poverty index and who had higher levels of family stress had more depressed moods compared with peers (also family stress significantly mediated the relationship between poverty and adolescent depressed mood).
Parental Mental Health
Two studies examined the impact of parental mental health on African American children’s depression and anxiety. According to Chapman et al. (2012), the children of anxious parents were four times more likely than the children of nonanxious parents to meet criteria for an anxiety disorder. Boyd and Waanders (2013) reported that maternal depression severity was not associated with child depression symptoms.
Adverse Life Events
One study examined the association between adverse life events (e.g., having a family member become ill and/or losing a family member) and African American children’s depression over time. In this longitudinal study, for girls, there was a significant positive association between adverse family life events and depressive symptoms; however, the strength of the association decreased over time (Sanchez et al. 2012). For boys, there was a significant positive association between adverse family life events and depressive symptoms, and this association was consistent over time.
Discussion
The main aim of this review was to explore associations between family-level factors and the prevalence of depression and anxiety among African American children. To our knowledge, this is the first review to systematically document research that examines the relationship between family factors and depression and anxiety in African American children.
First, we summarized study characteristics, such as research design, sample demographics, and instruments used to assess children’s depressive and anxious symptoms. The findings revealed that the majority of studies included in this review focused on depression as opposed to anxiety, using mainly the Child Depression Inventory or the Center for Epidemiological Studies–Depression Scale to measure children’s depressive symptoms (Kovacs 1981; Radloff 1977). The inattention to anxiety suggests a gap in the literature and may be informed by existing findings regarding prevalence of anxiety disorders among African American children, particularly as these findings are discrepant. The review also revealed that the design of approximately 35 % of the studies were longitudinal. Conducting longitudinal research is key to understanding the complexity of experiences of African American children and adolescents, because they allow researchers to observe the relationships between variables of interest (e.g., family-level factors and anxiety) over time. The longitudinal studies we reviewed provided information of the trajectory of family-level factors and anxiety and depression among African American children.
In this review, the majority of the study samples were low-income families. While the intended focus of this review was not on low-income families and children, this skewed sample is understandable yet potentially misleading. That is, a majority of studies and reports that focus on African American children and adolescents examine risk factors and their association with negative outcomes. African American youth are disproportionately exposed to risk factors (e.g., poverty, negative life events, community violence, and discrimination) that may increase the risk of developing depression and anxiety (APA 2008; Lewis et al. 2012; McCabe et al. 1999). Thus, given the societal realities (i.e., overrepresentation of African American youth in comparison to White youth living below the poverty line; DeNavas-Walt et al. 2009) and poverty shown to predict the onset of mental disorders (McLaughlin et al. 2011), African American youth clearly face challenges that can compromise their health and well-being. However, this reality results in a skewed perspective of African American children and adolescents by highlighting poor adjustment and poor mental health. We contend that the vulnerabilities and risks African American youth face derive from proximal concerns, such as underresourced schools and neighborhoods, inaccessibility to sufficient mental health care and disparities and not are due to genetic disposition (e.g., Spencer 2006; Weinstein 2002). Because of these extraneous variables, fostering family level factors such as healthy family functioning and environments for children residing in low income homes to buffer against proximal risks is pivotal to their healthy development and emotional well-being.
While studies in this review primarily reported the primary caregiver as female, they failed to report the members of a household; specifically, it was unclear whether a male (father or father figure) was present in the home. These findings suggest a gap in knowledge about the role of fathers or father figures in African American children’s mental health and expressions of depression and anxiety.
We examined studies that explore the association between family-level factors and depression and anxiety among African American children. As expected, we found that positive family-level factors (e.g., positive parenting practices, healthy family functioning and environments) have a protective role in buffering depression and anxiety symptoms among African American children. This review found parenting practices to be the most frequently examined family-level factor, and more specifically, positive parenting. All studies that examined whether positive parenting predicted less depression and anxiety symptoms had a significant inverse relationship between positive parenting (e.g., parental support, positive parental role models, parental encouragement) and children’s anxiety and/or depression. This is particularly relevant as family is regarded as the primary socialization agent during childhood providing a context that shapes developmental outcomes (e.g., Grusec 2011). These findings suggest the importance of strengthening parenting practices as part of a comprehensive approach to addressing depression and anxiety among African American children.
Among other family-level factors, family functioning and environment, as well as family conflict and violence were the most frequently assessed, and about half of these studies found that healthy family functioning and environment (e.g., family support, social capital) and less family conflict and violence was associated with lower levels of children’s depression and anxiety. These findings are key given the disproportionate exposure of African American children to community violence and other such risk factors (e.g., Lewis et al. 2012), which may be, for the most part, beyond family’s control. For example, a focus on fostering better functioning within the family environment may, in turn, help to buffer some of the negative consequences (e.g., depression) of these factors (e.g., community violence) on African American children’s mental health. In sum, the literature we reviewed seemed to suggest that family-level factors were significantly associated with African American children’s mental health (i.e., depression and anxiety). In particular, positive family-level factors (e.g., positive parenting, healthy family functioning and environment) was associated with decreased depression and anxiety, and this knowledge provide points of intervention for practitioners working with African American children dealing with depression and anxiety.
Limitations
Although, this review presented key results, similar to most reviews there are limitations that must be acknowledged. First, despite our search strategies aimed to include the greatest number of relevant studies, arguably, some publications were overlooked or excluded from the review. Second, it is also possible literature relevant to the review may have been published after the database searches were conducted, and it is possible other databases that we did not select could have had relevant studies for our review. Third, the authors acknowledge that some researchers (e.g., Neblett et al. 2008) consider racial socialization as a family-level factor. However, in our review, we did not conceptualize racial socialization as such, thus limiting the inclusion of studies that may address the buffering nature of parental racial socialization in relation to the depression and anxiety among African American children. Finally, this review only included studies that exclusively focused on African American children, thus, it omits knowledge that could be gain by studies that focused on diverse populations but that included results specifically for African Americans.
Implications for Future Research
The limitations aside, findings from the systematic review highlight the relationship between family level factors and anxiety and depression among African American children who are low income, live in urban areas, and primarily reside in female-headed households. Future research might consider a holistic examination of African American children and family life by including variation in family structure, such as middle-income, two-parent families, single father-headed households and other nontraditional family structures (e.g., kinship care families). Future research should also examine how geographic differences (e.g., rural vs urban) may impact mental health related outcomes for African American children.
The fact that a majority of studies and reports that focus on African American children and adolescents examine risk factors and their association with negative outcomes results in a deficit framing of African American children. Future studies should highlight strengths and protective competencies that to date have largely been ignored. A balanced perspective would assume and integrate both risk and protection as part of African American youth lived experience and would provide the next generation of researchers, clinicians and policy makers with a useful more accurate lens through which to view African American children.
The present review focused exclusively on African American children; however, we recognize the potential for within group differences as it relates to the influence of family on mental health outcomes among Black children. Future studies could explore if key findings from this review hold across other ethnic subgroups of Black children (e.g., Black Caribbean children, Black African immigrant children).
Existing literature exemplifies the significance of the role of race in the life experiences of African Americans (e.g., Schaefer 2004) and the importance of parenting strategies that specifically reflect cultural experiences (e.g., Stevenson et al. 2001). Thus, continued examination of societal level conditions, such as racism and other racial, ethnic, and/or cultural nuances and competencies that influence or inhibit the relationships between family-level factors and African American children’s mental health outcomes are encouraged. Given that discrimination continues to cause stressful life experiences, determining the psychological outcomes associated with the discriminatory attribution process, in relation to anxiety, worry, and trauma are warranted.
Conclusion
Finally, this review showed that positive family-level factors (e.g., positive parenting, healthy family functioning and environments) serve as protective factors for African American children’s mental health. Findings from this review can inform the development or adaptation of family-based preventive and treatment interventions targeting African American children at risk for or experiencing depression and/or anxiety.
References
American Psychological Association, & Task Force on Resilience and Strength in Black Children and Adolescents. (2008). Resilience in African American children and adolescents: A vision for optimal development. Washington, DC: Author.
Anxiety and Depression Association of America. (2016). Children and teens. Retrieved from http://www.adaa.org/living-with-anxiety/children.
Austin, A. A., & Chorpita, B. F. (2004). Temperament, anxiety, and depression: Comparisons across five ethnic groups of children. Journal of Clinical Child and Adolescent Psychology, 33(2), 216–226.
Barnett, T. E., Rowley, S., Zimmerman, M. A., Vansadia, P., & Caldwell, C. H. (2011). A longitudinal study of household change on African American adolescents. Journal of Community Psychology, 39(3), 303–315. doi:10.1002/jcop.20434.
Barton, A. W., Beach, S. H., Kogan, S. M., Stanley, S. M., Fincham, F. D., Hurt, T. R., et al. (2015). Prevention effects on trajectories of African American adolescents’ exposure to interparental conflict and depressive symptoms. Journal of Family Psychology, 29(2), 171–179. doi:10.1037/fam0000073.
Bean, R. A., Barber, B. K., & Crane, D. R. (2006). Parental support, behavioral control, and psychological control among African American youth: The relationships to academic grades, delinquency, and depression. Journal of Family Issues, 27(10), 1335–1355. doi:10.1177/0192513X06289649.
Birmaher, B., Bridge, J. A., Williamson, D. E., Brent, D. A., Dahl, R. E., Axelson, D. A., et al. (2004). Psychosocial functioning in youths at high risk to develop major depressive disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 839–846.
Boyd, R. C., & Waanders, C. (2013). Protective factors for depression among African American children of predominantly low-income mothers with depression. Journal of Child and Family Studies, 22(1), 85–95. doi:10.1007/s10826-012-9588-y.
Bryant, A. L., & Zimmerman, M. A. (2003). Role models and psychosocial outcomes among African American adolescents. Journal of Adolescent Research, 18(1), 36–67. doi:10.1177/0743558402238276.
Buckingham-Howes, S., Oberlander, S. E., Hurley, K. M., Fitzmaurice, S., & Black, M. M. (2011). Trajectories of adolescent mother–grandmother psychological conflict during early parenting and children’s problem behaviors at age 7. Journal of Clinical Child and Adolescent Psychology, 40(3), 445–455. doi:10.1080/15374416.2011.563473.
Canals, J., Domènech-Llaberia, E., Fernández-Ballart, J., & Martí-Henneberg, C. (2002). Predictors of depression at eighteen. European Child and Adolescent Psychiatry, 11(5), 226–233.
Center for Behavioral Health Statistics and Quality. (2015). Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15-4927, NSDUH Series H-50). Retrieved from http://www.samhsa.gov/data/.
Center for Substance Abuse Treatment. (2008). Substance abuse and suicide prevention: Evidence and implications—A white paper. DHHS Pub. No. SMA-08-4352. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Chapman, L. K., Petrie, J., Vines, L., & Durrett, E. (2012). The co-occurrence of anxiety disorders in African American parents and their children. Journal of Anxiety Disorders, 26(1), 65–70. doi:10.1016/j.janxdis.2011.08.014.
Chen, K. W., Killeya-Jones, L. A., & Vega, W. (2005). Prevalence and co-occurrence of psychiatric symptom clusters in the US adolescent population using DISC predicative scales. Clinical Practice and Epidemiology in Mental Health, 1, 1–12. doi:10.1186/1745-0179-1-22.
Chester, C., Jones, D. J., Zalot, A., & Sterrett, E. (2007). The psychosocial adjustment of African American youth from single mother homes: The relative contribution of parents and peers. Journal of Clinical Child and Adolescent Psychology, 36(3), 356–366. doi:10.1080/15374410701444306.
Child Care and Early Education Research Connections (CCEERC). (n.d.). Quantitative research assessment tool. Retrieved from http://www.researchconnections.org/childcare/datamethods/downloads/quantitativeresearch.pdf.
Coley, R. L. (2003). Daughter–father relationships and adolescent psychosocial functioning in low-income African American families. Journal of Marriage and Family, 65(4), 867–875. doi:10.1111/j.1741-3737.2003.00867.x.
Constantine, M. G. (2006). Perceived family conflict, parental attachment, and depression in African American female adolescents. Cultural Diversity and Ethnic Minority Psychology, 12(4), 697–709. doi:10.1037/1099-9809.12.4.697.
Cooley-Quille, M., Boyd, R. C., Frantz, E., & Walsch, J. (2001). Emotional and psychophysiological impact of exposure to community violence in urban adolescents. Journal of Child Clinical Psychology, Special Section: Violence & Youth, 30, 199–206.
Cooper, S., Brown, C., Metzger, I., Clinton, Y., & Guthrie, B. (2013). Racial discrimination and African American adolescents’ adjustment: Gender variation in family and community social support, promotive and protective factors. Journal of Child and Family Studies, 22(1), 15–29.
Copeland, W. E., Shanahan, L., Costello, E. J., & Angold, A. (2009). Childhood and adolescent psychiatric disorders as predictors of young adult disorders. Archives of General Psychiatry, 66(7), 764–772.
Costello, E. J., Egger, H. L., & Angold, A. (2005). The developmental epidemiology of anxiety disorders: Phenomenology, prevalence, and comorbidity. Child and Adolescent Psychiatric Clinics of North America, 14(4), 631–648.
DeNavas-Walt, C., Proctor, B. D., & Smith, J. C. (2009). Income, poverty, and health insurance coverage in the United States: 2008 (U. S. Census Bureau, Current 134 Population Reports No. P60-236). Washington, DC: U.S. Government Printing Office. Retrieved from http://www.census.gov/prod/2009pubs/p60-236.pdf.
Fergusson, D. M., & Woodward, L. J. (2002). Mental health, educational, and social role outcomes of adolescents with depression. Archives of General Psychiatry, 59(3), 225–231.
Fitzpatrick, K. M., Dulin, A., & Piko, B. (2010). Bullying and depressive symptomatology among low-income, African–American youth. Journal of Youth and Adolescence, 39(6), 634–645. doi:10.1007/s10964-009-9426-8.
Fitzpatrick, K. M., Piko, B. F., Wright, D. R., & LaGory, M. (2005). Depressive symptomatology, exposure to violence, and the role of social capital among African American adolescents. American Journal of Orthopsychiatry, 75(2), 262–274. doi:10.1037/0002-9432.75.2.262.
Forehand, R., & Jones, D. J. (2003). Neighborhood violence and coparent conflict: Interactive influence on child psychosocial adjustment. Journal of Abnormal Child Psychology, 31(6), 591–604. doi:10.1023/A:1026206122470.
Franko, D. L., Striegel-Moore, R. H., Bean, J., Tamer, R., Kraemer, H. C., Dohm, F. A., et al. (2005). Psychosocial and health consequences of adolescent depression in Black and White young adult women. Health Psychology, 24(6), 586.
Gaylord-Harden, N. K., & Cunningham, J. A. (2009). The impact of racial discrimination and coping strategies on internalizing symptoms in African American youth. Journal of Youth and Adolescence, 38(4), 532–543.
Gaylord-Harden, N. K., Ragsdale, B. L., Mandara, J., Richards, M. H., & Petersen, A. C. (2007). Perceived support and internalizing symptoms in African American adolescents: Self-esteem and ethnic identity as mediators. Journal of Youth and Adolescence, 36(1), 77–88. doi:10.1007/s10964-006-9115-9.
Gough, D., Oliver, S., & Thomas, J. (2012). An introduction to systematic reviews. London: Sage.
Grant, K. E., O’koon, J. H., Davis, T. H., Roache, N. A., Poindexter, L. M., Armstrong, M. L., et al. (2000). Protective factors affecting low-income urban African American youth exposed to stress. Journal of Early Adolescence, 20(4), 388–417. doi:10.1177/0272431600020004002.
Gray, C. M., Carter, R., & Silverman, W. K. (2011). Anxiety symptoms in African American children: Relations with ethnic pride, anxiety sensitivity, and parenting. Journal of Child and Family Studies, 20(2), 205–213.
Grusec, J. (2011). Socialization processes in family: Social and emotional development. Annual Review of Psychology, 62, 243–269. doi:10.1146/annurev.psych.121208.131650.
Hall, D. M., Cassidy, E. F., & Stevenson, H. C. (2008). Acting ‘tough’ in a ‘tough’ world: An examination of fear among urban African American adolescents. Journal of Black Psychology, 34(3), 381–398. doi:10.1177/0095798408314140.
Hammack, P. L., Richards, M. H., Luo, Z., Edlynn, E. S., & Roy, K. (2004a). Social support factors as moderators of community violence exposure among inner-city African American young adolescents. Journal of Clinical Child and Adolescent Psychology, 33(3), 450–462. doi:10.1207/s15374424jccp3303_3.
Hammack, P. L., Robinson, W. L., Crawford, I., & Li, S. T. (2004b). Poverty and depressed mood among urban African–American adolescents: A family stress perspective. Journal of Child and Family Studies, 13(3), 309–323. doi:10.1023/B:JCFS.0000022037.59369.90.
Hjemdal, O., Aune, T., Reinfjell, T., Stiles, T. C., & Friborg, O. (2007). Resilience as a predictor of depressive symptoms: A correlational study with young adolescents. Clinical Child Psychology and Psychiatry, 12(1), 91–104.
Jenkins, E. J., Wang, E., & Turner, L. (2009). Traumatic events involving friends and family members in a sample of African American early adolescents. American Journal of Orthopsychiatry, 79(3), 398–406. doi:10.1037/a0016659.
Jones, D. J., Forehand, R., Rakow, A., Colletti, C. M., McKee, L., & Zalot, A. (2008). The specificity of maternal parenting behavior and child adjustment difficulties: A study of inner-city African American families. Journal of Family Psychology, 22(2), 181–192. doi:10.1037/0893-3200.22.2.181.
Kessler, R. C., Avenevoli, S., Costello, J., Georgiades, K., Green, J. G., Gruber, M. J., et al. (2012). Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the national comorbidity survey replication adolescent supplement [Appendix tables]. Archives of General Psychiatry, 69, 372–380. http://www.hcp.med.harvard.edu/ncs/publications.php.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602.
Keyes, C. L. M. (2006). Mental health in adolescence: Is America’s youth flourishing? American Journal of Orthopsychiatry, 76(3), 395–402.
Knopf, D., Park, M. J., & Mulye, T. P. (2008). The mental health of adolescents: A national profile, 2008. San Francisco, CA: National Adolescent Health Information Center. Retrieved from http://nahic.ucsf.edu/downloads/MentalHealthBrief.pdf.
Kovacs, M. (1981). Rating scales to assess depression in school-aged children. Acta Paedopsychiatrica, 46, 305–315.
Kwon, J., Delaney-Black, V., Covington, C., Abell, S. C., Nordstrom-Bailey, B., Sokol, R. J., et al. (2006). The relations between maternal expressed emotion and children’s perceived self-competence, behavior and intelligence in African–American families. Early Child Development and Care, 176(2), 195–206. doi:10.1080/0300443042000302681.
Lewis, K. M., Byrd, D. A., & Ollendick, T. H. (2012). Anxiety symptoms in African–American and Caucasian youth: Relations to negative life events, social support, and coping. Journal of Anxiety Disorders, 26(1), 32–39.
Loh, E., & Wragg, J. (2004). Developmental perspective. In K. N. Dwivedi & P. B. Harper (Eds.), Promoting the emotional well-being of children and adolescents and preventing their mental ill-health: A handbook (pp. 29–48). London: Jessica Kingsley Publishers.
Mandara, J., & Pikes, C. L. (2008). Guilt trips and love withdrawal: Does mothers’ use of psychological control predict depressive symptoms among African American adolescents? Family Relations: An Interdisciplinary Journal of Applied Family Studies, 57(5), 602–612. doi:10.1111/j.1741-3729.2008.00526.x.
Margolin, S. (2006). African American youths with internalizing difficulties: Relation to social support and activity involvement. Children and Schools, 28(3), 135–144.
McCabe, K. M., Clark, R., & Barnett, D. (1999). Family protective factors among urban African American youth. Journal of Clinical Child Psychology, 28(2), 137–150.
McKee, L., Jones, D. J., Roland, E., Coffelt, N., Rakow, A., & Forehand, R. (2007). Maternal HIV/AIDS and depressive symptoms among inner-city African American youth: The role of maternal depressive symptoms, mother-child relationship quality, and child coping. American Journal of Orthopsychiatry, 77(2), 259–266. doi:10.1037/0002-9432.77.2.259.
McLaughlin, K. A., Breslau, J., Green, J. G., Lakoma, M. D., Sampson, N. A., Zaslavsky, A. M., et al. (2011). Childhood socio-economic status and the onset, persistence, and severity of DSM-IV mental disorders in a US national sample. Social Science and Medicine, 73(7), 1088–1096.
McLoyd, V. C., Kaplan, R., Hardaway, C. R., & Wood, D. (2007). Does endorsement of physical discipline matter? Assessing moderating influences on the maternal and child psychological correlates of physical discipline in African American families. Journal of Family Psychology, 21(2), 165–175. doi:10.1037/0893-3200.21.2.165.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in US adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989.
Merry, S., McDowell, H., Wild, C. J., Bir, J., & Cunliffe, R. (2004). A randomized placebo-controlled trial of a school-based depression prevention program. Journal of the American Academy of Child and Adolescent Psychiatry, 43(5), 538–547.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(6), e1000097.
Murray, C., & Greenberg, M. T. (2000). Children’s relationship with teachers and bonds with school an investigation of patterns and correlates in middle childhood. Journal of School Psychology, 38(5), 423–445.
Nebbitt, V. E., & Lambert, S. F. (2009). Correlates of anxiety sensitivity among African American adolescents living in urban public housing. Journal of Community Psychology, 37(2), 268–280. doi:10.1002/jcop.20292.
Neblett, E. W., White, R. L., Ford, K. R., Philip, C. L., Nguyen, H. X., & Sellers, R. M. (2008). Patterns of racial socialization and psychological adjustment: Can parental communications about race reduce the impact of racial discrimination? Journal of Research on Adolescence, 18(3), 477–515.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
RefWorks Home Page. (2009). Retrieved November 30, 2015, from http://www.refworks.com/.
Rose, T., Joe, S., Shields, J., & Caldwell, C. H. (2014). Social integration and the mental health of Black adolescents. Child Development, 85(3), 1003–1018.
Rothon, C., Head, J., Clark, C., Klineberg, E., Cattell, V., & Stansfeld, S. (2009). The impact of psychological distress on the educational achievement of adolescents at the end of compulsory education. Social Psychiatry and Psychiatric Epidemiology, 44(5), 421–427.
Rushton, J. L., Forcier, M., & Schectman, R. M. (2002). Epidemiology of depressive symptoms in the National Longitudinal Study of Adolescent Health. Journal of the American Academy of Child and Adolescent Psychiatry, 41(2), 199–205.
Sagrestano, L. M., Paikoff, R. L., Holmbeck, G. N., & Fendrich, M. (2003). A longitudinal examination of familial risk factors for depression among inner-city African American adolescents. Journal of Family Psychology, 17(1), 108–120. doi:10.1037/0893-3200.17.1.108.
Sanchez, Y. M., Lambert, S. F., & Ialongo, N. S. (2012). Life events and depressive symptoms in African American adolescents: Do ecological domains and timing of life events matter? Journal of Youth and Adolescence, 41(4), 438–448. doi:10.1007/s10964-011-9689-8.
Schaefer, R. T. (2004). Racial and ethnic groups. Upper Saddle River, NJ: Pearson-Prentice Hall.
Simons, L. G., Simons, R. L., & Su, X. (2013). Consequences of corporal punishment among African Americans: The importance of context and outcome. Journal of Youth and Adolescence, 42(8), 1273–1285. doi:10.1007/s10964-012-9853-9.
Spencer, M. B. (2006). Phenomenology and ecological systems theory: Development of diverse groups. In W. Damon & R. Lerner (Series Eds.) & R. M. Lerner (Vol. Ed.), Handbook of child psychology: Vol. 1. Theoretical models of human development (6th ed., pp. 829–893). New York: Wiley.
Spielberger C. D., Edwards C. D., Montuori J., & Lushene D. (1973). How i feel. Questionnaire (State-Trait Anxiety Inventory for Children). Counseling Psychologists Press, Palo Alto, CA.
Steele, R. G., Armistead, L., & Forehand, R. (2000). Concurrent and longitudinal correlates of depressive symptoms among low-income, urban, African American children. Journal of Clinical Child Psychology, 29(1), 76–85.
Stevenson, H. C., Davis, G., & Abdul-Kabir, S. (2001). Stickin’ to, watchin’ over, and gettin’ with: An African American parent’s guide to discipline. San Francisco, CA: Jossey-Bass.
Taylor, R. D., Budescu, M., Gebre, A., & Hodzic, I. (2014). Family financial pressure and maternal and adolescent socioemotional adjustment: Moderating effects of kin social support in low income African American families. Journal of Child and Family Studies, 23(2), 242–254. doi:10.1007/s10826-012-9688-8.
Tolou-Shams, M., Paikoff, R., McKirnan, D. J., & Holmbeck, G. N. (2007). Mental health and HIV risk among African American adolescents: The role of parenting. Social Work in Mental Health, 5(1–2), 27–58. doi:10.1300/J200v05n01_02.
U.S. Department of Health and Human Services. (1999). Mental health: A report of the surgeon general. Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health. Retrieved from http://store.samhsa.gov/product/Mental-Health-A-Report-of-the-Surgeon-General-Full-Report/SG-RPT.
Washington, T., Cryer, Q., Coakley, T., Labben, J., Gleeson, J., & Shears, J. (2014). Examining maternal and paternal involvement as promotive factors of competence in African American children in informal kinship care. Children and Youth Services Review, 44, 9–15.
Washington, T., Gleeson, J. P., & Rulison, K. L. (2013). Competence and African American children in informal kinship care: The role of family. Children and Youth Services Review, 35(9), 1305–1312.
Washington, T., Rose, T., Colombo, G., Hong, J. S., & Coard, S. I. (2015). Family-level factors and African American children’s behavioral health outcomes: A systematic review. Child & Youth Care Forum, 44(6), 819–834. doi:10.1007/s10566-015-9308-z.
Weinstein, R. S. (2002). Reaching higher: The power of expectations in schooling. Cambridge, MA: Harvard University Press.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest for any author of the manuscript.
Animals or Humans Involved/Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Washington, T., Rose, T., Coard, S.I. et al. Family-Level Factors, Depression, and Anxiety Among African American Children: A Systematic Review. Child Youth Care Forum 46, 137–156 (2017). https://doi.org/10.1007/s10566-016-9372-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10566-016-9372-z