
Abstract
In the present study, we investigated the relationship between blood pressure (BP) and pulse transit time (PTT) and evaluated the accuracy of the PTT-based cuffless BP estimation on 14 normotensive subjects. Least-squares regression was used to estimate BP in the first test and a repeatability test carried out half year later. BP in the repeatability test was also estimated using the regression coefficients in the first test. The results illustrated that in the first and repeatability tests (1) arterial BP increased and PTT decreased acutely after the exercises and (2) systolic BP was highly correlated with PTT. In the repeatability test, the estimation differences from the references were 0.0 ± 5.3 mmHg and 0.0 ± 2.9 mmHg for systolic and diastolic BPs respectively using least-squares regression. However, the estimation differences increased to 1.4 ± 10.2 mmHg and 2.1 ± 7.3 mmHg for systolic and diastolic BPs, respectively when the regression coefficients in the first test were used for prediction. In summary, reasonable BP estimations were given in the first and repeatability tests but not using the regression coefficients obtained 6 months ago for some subjects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cardiovascular diseases and hypertension are prevalent in both developing and developed countries in recent decades (Ezzati et al. 2004; Kearney et al. 2005). Cardiovascular diseases ranked as the leading cause of deaths (World Health Organization 2005). It accounted for the deaths of 17.5 million people globally in 2005. In China, approximate US$ 558 billion of national income will be foregone in the coming 10 years as a result of the pre-mature deaths caused by heart diseases, stroke and diabetes. Consequently, there is an urgent need for cuffless and continuous monitoring of blood pressure (BP) to improve management of hypertension and evaluation of the cardiovascular diseases.
Pulse transit time (PTT), or known as the inverse of pulse wave velocity, has been demonstrated as one of the potential parameters for a cuffless and non-invasive BP measurement (Newlin 1981; Allen et al. 1981; Lane et al. 1983; Pollak and Obrist 1983; Poon and Zhang 2005). PTT is the duration for a pressure pulse to propagate through a segment of the arterial tree. It is measured between the characteristic points of electrocardiogram (ECG) and peripheral pressure pulse. Photoplethysmogram (PPG) is one of the popular choices for the peripheral pressure pulse. Besides the potential use to cuffless BP measurement, PTT is also employed in other applications, such as the measurements of arterial stiffness (Wilkinson et al. 1998; Laurent et al. 2001) and respiratory efforts (Brock et al. 1993; Pitson et al. 1995; Smith et al. 1999; Foo 2007) as well as an index of sympathetic nervous system effects on the vasculature (Pitson et al. 1994). Recently, PTT has also been shown to respond to the stress which is useful for psychological evaluation and stress management (Pan and Li 2007).
In recent decades, many literatures associated with PTT-based cuffless BP measurement have been published. Repeatability test for investigating the relationship between BP and PTT and the accuracy of the BP estimation using PTT-approach after several months, however, has not been conducted systematically. Thus, in the present study, we organized experiments including the first test and a repeatability test after half year to evaluate the accuracy of PTT-based BP estimation on same group of subjects.
Materials and Methods
Experiments in the first test have been conducted on 41 normotensive subjects, aged 25 ± 4 years (from 20 to 36 years), and included 22 males. No subjects have been diagnosed with cardiovascular diseases during the experimental period. After half year, only 14 subjects, aged 26 ± 4 years (from 21 to 34 years) and included eight females, participated in the repeatability test. Data collected from these 14 subjects were used in the following analysis. Participants were instructed about the procedures and gave informed consent prior to the participation.
Devices and Experimental Procedures
The same devices and experimental procedures were used in the two tests. An in-house-designed circuitry was used to detect the derivative of ECG (dECG) and PPG. The circuitry was connected to a sensor unit with electrodes, light emitting diode and photodetector. The aforementioned sensor unit and circuitry have been used in previous literatures (Wong and Zhang 2005, 2006). The analog dECG and PPG were sampled at 1 kHz by an A–D converter (Model DI-220, DATAQ Instrument WINDAQ, USA). Brachial BP was measured intermittently by an automatic BP machine (Model HEM-907, OMRON, Japan) at subject’s right arm. Exercise was included in the experimental procedures and it was carried out on a treadmill (Model C956, Precor, USA).
Experimental procedures have been described in previous literatures (Wong and Zhang 2005, 2006). Briefly, the experimental procedures were arranged into four sessions, namely, Pre-exercise, Post-exercise1, Post-exercise2 and Recovery. Figure. 1 illustrates the steps in each session. In the Pre-exercise session, subject sat upright and rested for 3 min. It was followed with four BP measurements (BPM) with three signal recordings (SR) (Datasets 1–3) in between any two BPM. In each SR, dECG and PPG were captured from subject’s left index finger, right index and middle fingers simultaneously for 45 s. As contact force between the fingers and sensors could influence the signal collection which in turn affected PTT measurement (Teng et al. 2004; Teng and Zhang 2006, 2007), subject was reminded to maintain stable contact force throughout SR.

An outline of experimental procedures in the first and repeatability tests
Afterwards, subject ran on the treadmill at 10 km/h for 3 min. It was followed by the Post-exercise1 session. Four BPM with three SR (Datasets 4–6) in between two BPM were conducted. Later on, subject ran on the treadmill with lower speed, 8 km/h, for 3 min. He/she underwent the Post-exercise2 session afterwards and repeated the procedures in the Post-exercise1 session (Datasets 7–9). In the Recovery session, four more SR (Datasets 10–13) and BPM were acquired from subject 15, 20, 25, and 40 min, respectively after the end of the Post-exercise2 session.
Signal Processing and Data Analysis
The collected dECG and PPG were analyzed offline using Matlab®. Beat-to-beat PTT was measured from the peak of dECG to the peak of PPG derivative by a tailor-made program. Average PTT was calculated for each dataset. Heart rate (HR) was measured as the reciprocal of average successive time intervals between the peaks of dECG multiplied by 60. BP in the Pre-exercise, Post-exercise1, Post-exercise2 sessions were the average of successive readings.
Student t-test was used for testing a hypothesis on the basis of a difference between sample means: p < 0.05 indicated that the means were statistically significant. The correlation between a pair of parameters was analyzed by the correlation coefficient r, wherein r > 0.8 or r < −0.8 was considered as close correlation between the pair. The linear regression line was determined using the least-squares method. The results were presented in the form of mean ± standard deviation (SD).
Results
Baseline Study
Figure 2 shows the means ± SDs of basal systolic BP (SBP), diastolic BP (DBP), HR and PTT in the first and repeatability tests. The baselines were the averages in the Pre-exercise session. SBP, DBP, HR and PTT in the first test were 103.9 ± 9.6 mmHg, 59.8 ± 8.9 mmHg, 71.1 ± 6.8 bpm and 217.1 ± 17.3 ms, respectively. No parameters showed significant differences (p > 0.05) in the repeatability test, wherein SBP, DBP, HR and PTT were 103.0 ± 11.3 mmHg, 59.3 ± 8.1 mmHg, 68.7 ± 6.2 bpm and 216.8 ± 27.3 ms, respectively.

The means ± SDs of the basal a HR, PTT and b BP in the first and repeatability tests
Variations after Exercises
Figure 3 depicts the variations of PTT, HR, SBP and DBP throughout the experiment in the first and repeatability tests. It was shown that PTT decreased and BP and HR increased acutely after exercises (Datasets 4, 7). PTT decreased and SBP increased significantly (p < 0.05) from Dataset 4 to Dataset 8 in both tests. In Dataset 9, only PTT in the first test and SBP in both tests changed significantly (p < 0.05). Significant DBP increased (p < 0.05) in Datasets 4, 7 and 8 in the first test but not in the repeatability test. It was noteworthy that HR increased pronouncedly after exercise.

The variations of a PTT b HR c SBP and d DBP throughout the experiment in the first test (1st test) and repeatability test (Re-test). * and # indicate that the parameters are significantly (p < 0.05) different from the basal values (Base.) in the first and repeatability tests, respectively
The Linearity Between BP and PTT
Table 1 shows the linear regressions between SBP and PTT in two tests. The slope β was always negative which indicated that SBP was inversely proportional to PTT. Even though the y-intercept α and slope β in the first and repeatability tests were different, the differences were insignificant (p = 0.963 and p = 0.891 for α and β, respectively).
Similarly, Table 2 summarizes the linear regressions between DBP and PTT in individuals. The regression coefficients α and β in the first and repeatability tests were insignificantly different (p = 0.323 and p = 0.481 for α and β, respectively). Compared with the regression coefficients in Table 1, the magnitudes of both α and β in Table 2 were always smaller.
Table 3 concludes the average correlation coefficients r and means ± SDs of differences in the regressions of all subjects. SBP was highly correlated with PTT in the first (r = −0.92) and repeatability tests (r = −0.87), however, the SD of differences in the repeatability test was significantly (p = 0.030) larger than that in the first test. On the other hand, PTT was less correlated with DBP (r = −0.38 in the first test and r = −0.30 in the repeatability test). The SD of differences in the tests was insignificantly (p = 0.155) different with the other.
BP Estimation in the Repeatability Test Using Regression Coefficients in the First Test
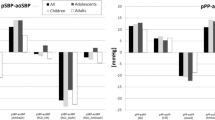
Blood pressure in the repeatability test was estimated using the regression coefficients in the first test. Fig. 4 depicts the difference between the measured and predicted BPs in the repeatability test. The estimation differences in the repeatability test using least-squares regression (reported in Table 3) were given as references. The difference between the measured and predicted SBPs and DBPs increased from 0.0 ± 5.3 mmHg and 0.0 ± 2.9 mmHg to 1.4 ± 10.2 mmHg and 2.1 ± 7.3 mmHg, respectively.

The means ± SDs of the differences between the measured and predicted BPs in the repeatability test. The differences in the repeatability test, reported in Table 3, are given as references. The difference is defined as the subtraction of measured BP from predicted BP
Discussion
The results in the present study repeated the inverse relation between arterial BP and PTT in normotensive subjects in the first and repeatability tests, wherein the variations of PTT and arterial BP were associated with the exercise intensity. To our understanding, it is the first study to compare the regression coefficients in the first test with those in the repeatability test after half year. The results showed that the coefficients in the regressions from the tests were similar. However, the estimation difference in the repeatability test was quite large when arterial BP was predicted using the regression coefficients in the first test.
In the present study, PTT was highly correlated with SBP but not with DBP. It was probably due to the small variations of DBP. Geddes et al. (1981) has reported the inverse relation between DBP and PTT when pressure was controlled to vary from 15 to 250 mmHg. Compared to large variation of SBP, significant DBP change only occurred acutely after exercise (Datasets 4, 7) and it was not repeated in the repeatability test (shown in Fig. 3d). The small variation could affect the correlation study between DBP and PTT which in turn showed a poor correlation.
The Linearity Between BP and PTT
Blood pressure and pulse transit time usually varied linearly within a normal physiological range in the interventions. The linear relationship between arterial BP and PTT has been shown under different experimental setups, such as during exercise (Muehlsteff et al. 2006), post-exercise (Wong and Zhang 2005, 2006) and cold pressor test (Allen et al. 1981; Zhang and Zhang 2006). It is known that administrations of vasoactive drugs can change BP through the modification of vessel states. The linearity between BP and PTT is also reported in the studies with drugs administration. Zong et al. (1998) demonstrated an approximately linear relationship between arterial BP and PTT with and without vasoactive drugs in humans. This linearity was insignificantly correlated with the drug level applied on the subjects. Ochiai et al. (1999) also observed linear relation between BP and PTT when several vasoactive drugs, with different effects on the vessels, were administrated on the dogs.
Therefore, BP and PTT can be considered as linearly related when pressure changes within the physiological range. Our results repeated the linearity between SBP and PTT in the first and repeatability tests. Because of its linearity, linear regressions were applied on both tests to evaluate the variation of the linearity. The y-intercept and slope of linear regression, α and β, respectively, probably reflect the geometric and elastic factors of arteries based on the PTT model developed by Moens–Korteweg (1978) and empirical findings from Hughes et al. (1979).
It is known that change of arterial stiffness associates with substantial geometric change in artery appeared in the elderly and patients with several kinds of cardiovascular diseases (Yu et al. 2006). As the repeatability test was conducted on the subjects just after a half year and they were not diagnosed with cardiovascular diseases during the period, the arterial stiffness was not expected to change pronouncedly. Therefore, as the implication of arterial geometric and elastic properties, it is not surprising that the regression coefficients in the first and repeatability tests are similar and it is expected that the regression coefficients obtained in the first test are potential to estimate BP after half year.
BP Estimation in the Repeatability Test Using Regression Coefficients in the First Test
Despite the regression coefficients did not change significantly after half year, the difference between the measured and predicted BPs was large. When BP in the repeatability test was predicted using the regression coefficients obtained half year ago, SBP and DBP estmation differences were 1.4 ± 10.2 mmHg and 2.1 ± 7.3 mmHg, respectively.
For further evaluation, the differences between the measured and predicted SBPs in each subject in the repeatability test are illustrated in Fig. 5. It could be seen that large SBP estimation differences were mainly induced by three subjects, S01, S05 and S19. If datasets collected from them were discarded in the analysis, the difference between the measured and predicted SBPs would be reduced to 1.9 ± 7.1 mmHg.

The individual means ± SDs of the differences between the measured and predicted SBPs in the repeatability test. The difference is defined as the subtraction of measured BP from predicted BP
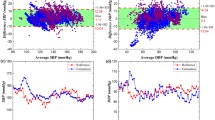
Figure 6 depicts the scatter plots showing the measured SBP and regression of subjects S01, S05 and S19 in the two tests. In Fig. 6a, SBP and PTT of subject S01 in the repeatability test were significantly (p = 0.038 for SBP and p = 0.003 for PTT) smaller than those in the first test. The pronounced SBP and PTT decreases in the repeatability test required a regression line in the first test to shift downwards for good estimation. The large y-intercept obtained in the first test seemed to be the main factor to induce an erroneous over-estimation in the repeatability test. In Fig. 6b, only SBP of subject S19 in the repeatability test was larger than that in the first test significantly (p = 0.003). The small y-intercept in the first test could cause under-estimation in the repeatability test on subject S19. On the other hand, the reason to account for erroneous SBP estimation in subject S05 is totally different. SBP and PTT of subject S05 were insignificantly different in two tests, p = 0.549 and p = 0.964 for PTT and SBP, respectively. The large estimation difference in the repeatability test is probably due to the change of slope instead of y-intercept in Fig. 6c. These examples indicated that the coefficients describing the relationship between BP and PTT could estimate BP half year later with reasonable accuracy in some but not all subjects. For subjects whose baseline BP changed after a period, regression coefficients obtained before were no longer appropriate for BP prediction and resulted in large estimation difference.

The scatter plots of SBP and PTT for subjects a S01 b S19 and c S05 in the first and repeatability tests. The light dot and dotted line represent the measured SBP and the regression line, respectively in the repeatability test
Conclusion
In the present study, we investigated the relationship between BP and PTT and evaluated the accuracy of PTT-based BP estimation by (1) using least-squares method in the first and repeatability tests, respectively; and (2) predicting BP in the repeatability test using the regression coefficients in the first test. Reasonable BP estimations were given in the first and repeatability tests, however, the regression coefficients obtained half year ago could not predict BP well in all subjects when pressure baseline changed in the repeatability test. The development of PTT-based BP estimation algorithm enabling to trace the potential change of baseline BP in subjects after a period probably improves estimation accuracy and reduces the necessity of frequent calibration of cuffless technique.
References
Allen RA, Schneider J, Davidson DM, Winchester MA, Taylor CB. The covariation of blood pressure and pulse transit time in hypertensive patients. Psychophysiology. 1981;18:301–5.
Brock J, Piston D, Stradling J. Use of pulse transit time as a measure of changes in inspiratory effort. J Ambul Monit. 1993;6:195–302.
Ezzati M, Lopez AD, Rodgers A, Murray CJL. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. Geneva: World Health Organization; 2004.
Foo JYA. Pulse transit time in paediatric respiratory sleep studies. Med Eng Phys. 2007;29:17–25.
Geddes LA, Voelz MH, Babbs CF, Bourland JD, Tacker WA. Pulse transit time as an indicator of arterial blood pressure. Psychophysiology. 1981;18:71–4.
Hughes DJ, Babbs CF, Geddes LA. Measurements of Young’s modulus of elasticity of the canine aorta with ultrasound. Ultrasound Imaging. 1979;1:356–67.
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–23.
Korteweg DJ. Ueber die fortpflanzunggesgeschwingdigkeit des schalles in elastischen rohren. Ann Physik Chemie. 1878;5:525–42.
Lane JD, Greenstadt L, Shapiro D. Pulse transit time and blood pressure: an intensive analysis. Psychophysiology. 1983;20:45–9.
Laurent S, Boutougrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236–41.
Muehlsteff J, Aubert XL, Schuett M. Cuffless estimation of systolic blood pressure for short effort bicycle tests: the prominent role of the pre-ejection period. Proceedings of the 28th annual conference of IEEE-EMBC 2006.
Newlin DB. Relationships of pulse transmission times to pre-ejection period and blood pressure. Psychophysiology. 1981;18:316–21.
Ochiai R, Takeda J, Hosaka H, Sogo Y, Tanaka R, Soma T. The relationship between modified pulse wave transit time an cardiovascular changes in isoflurane anesthetized dogs. J Clin Monit Comput. 1999;15:493–501.
Pan RLC, Li JKL. Noninvasive parametric evaluation of stress effects on cardiovascular function. Cardiovasc Eng. 2007;7:74–80.
Pitson D, Chhina N, Knijn S, Van Herwaaden M, Stradling J. Changes in pulse transit time and pulse rate as markers of arousal from sleep in normal subjects. Clin Sci (Lond). 1994;87:269–73.
Pitson DJ, Sandell A, Van den Hout R, Stradling JR. Use of pulse transit time as a measure of inspiratory effort in patients with obstructive sleep apnoea. Eur Respir J. 1995;8:1669–74.
Pollak MH, Obrist PA. Aortic-radial pulse transit time and ECG Q-wave to radial pulse wave interval as indices of beat-by-beat blood pressure change. Psychophysiology. 1983;20:21–8.
Poon CCY, Zhang YT. Cuff-less and noninvasive measurements of arterial blood pressure by pulse transit time. Proceedings of the 27th annual conference of IEEE-EMBC 2005.
Preventing chronic diseases: a vital investment. Geneva: World Health Organization; 2005.
Smith RP, Argod J, Pépin JL, Lévy PA. Pulse transit time: an appraisal of potential clinical applications. Thorax. 1999;54:452–7.
Teng XF, Poon CCY, Zhang YT. Study on the effect of contacting force on pulse transit time. Proceedings of the 2nd IEEE/EMBS International Summer School and Symposium on Medical Devices and Biosensors 2004.
Teng XF, Zhang YT. The effect of applied sensor contact force on pulse transit time. Physiol Meas. 2006;27:675–84.
Teng XF, Zhang YT. Theoretical study on the effect of sensor contact force on pulse transit time. IEEE Trans Biomed Eng. 2007;54:1490–8.
Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR, et al. Repeatability of pulse wave velocity and augmentation index measured by pulse wave analysis. J Hypertens. 1998;16:2079–84.
Wong MYM, Zhang YT. The relationship between pulse transit time and systolic blood pressure on individual subjects after exercises. Proceedings of Transdisciplinary Conference on Distributed Diagnosis and Home Healthcare 2006.
Wong YM, Zhang YT. The effects of exercises on the relationship between pulse transit time and arterial blood pressure. Proceedings of the 27th annual conference of IEEE-EMBC 2005.
Yu HY, Peng HH, Wang JL, Wen CY, Tseng WY. Quantification of pulse wave velocity of the descending aorta using axial velocity profiles from phase-contrast magnetic resonance imaging. Magn Reson Med. 2006;56:876–83.
Zhang XY, Zhang YT. The effect of local mild cold exposure on pulse transit time. Physiol Meas. 2006;27:649–60.
Zong W, Moody GB, Mark RG. Effects of vasoactive drugs on the relationship between ECG- pulse wave delay time and arterial blood pressure in ICU patients. Comput Cardiol. 1998;25:673–6.
Acknowledgments
This work is supported by the Hong Kong Innovation and Technology Fund. The authors would like to acknowledge Golden Meditech Company Ltd, Bird International Ltd, and Bright Steps Corporation for their supports to the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wong, M.YM., Poon, C.CY. & Zhang, YT. An Evaluation of the Cuffless Blood Pressure Estimation Based on Pulse Transit Time Technique: a Half Year Study on Normotensive Subjects. Cardiovasc Eng 9, 32–38 (2009). https://doi.org/10.1007/s10558-009-9070-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10558-009-9070-7