
Abstract
Purpose
Single- and multiple-dose studies were conducted to assess the pharmacokinetics, pharmacodynamics and safety of tolvaptan in healthy Japanese subjects.
Methods
All studies were single-center, randomized, placebo-controlled, single-blind or double-blind. In an ascending single-dose study, subjects were given a single oral dose of 15–120 mg tolvaptan or placebo. In multiple-dose studies, subjects were given 30, 60, 90 or 120 mg tolvaptan or placebo once daily for 7 days.
Results
After a single dose of 15–120 mg tolvaptan, the maximum plasma concentration (Cmax) and the area under the plasma concentration-time curve from zero to time t (AUCt) increased dose-dependently, and increases in AUCt were dose-proportional. Increases in 24-hour cumulative urine volume were dose- and AUC24hr-dependent. Urine excretion rates reached a maximum within 2–4 h after dosing. The maximal urine excretion rates increased dose-dependently, and appeared to reach a plateau at doses≥ 60 mg. A decrease in urine osmolality and an increase in free water clearance indicated an aquaretic effect of tolvaptan. Serum sodium concentrations were increased by tolvaptan and were higher than that with placebo, even 24 h after dosing, while serum potassium concentrations were unchanged. No tolvaptan accumulation was found after multiple dosing for 7 days. Although 24-hour cumulative urine volume following multiple dosing slightly decreased, a sustained diuretic effect was observed throughout the dosing period. The most common adverse event was mild thirst.
Conclusions
Single and multiple oral doses of tolvaptan exhibited dose-dependent aquaretic effects. Tolvaptan was well tolerated at all doses tested.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The antidiuretic hormone arginine vasopressin (AVP) is primarily responsible for maintaining body fluid homeostasis. Its secretion is regulated by osmoreceptors in the hypothalamus and baroreceptors located in the aorta and carotid arteries [1]. An increase in plasma osmolality or a decrease in blood pressure stimulates AVP secretion from the posterior pituitary, thereby inducing water reabsorption at the renal collecting duct via AVP V2-receptors. Congestive heart failure, hepatic failure with ascites and the syndrome of inappropriate antidiuretic hormone secretion are associated with enhanced water reabsorption in the renal collecting ducts. This occurs because of enhanced antidiuretic activity caused by excessive secretion of AVP, and may contribute to electrolyte imbalances such as fluid retention and consequent dilutional hyponatremia. Using conventional saluretics for these conditions may worsen hyponatremia and other electrolyte imbalances as a result of enhanced electrolyte excretion, and may result in neurologic and cardiac complications [2, 3]. To correct such fluid volume-overload conditions, selective V2-receptor antagonists that promote the excretion of excessive body fluid without electrolyte excretion have been investigated [4, 5].
Tolvaptan (OPC-41061; (±)-4’-[(7-chloro-2,3,4,5-tetrahydro-5-hydroxy-1 H-1-benzazepin-1-yl)-carbonyl]-o-tolu-m-toluidide) is an oral nonpeptide selective AVP yV2-receptor antagonist. Tolvaptan has no endogenous agonistic activity on the V2-receptor, as has been reported with other peptide V2-receptor antagonists, and exhibits an aquaretic effect by selectively blocking the binding of AVP to the V2-receptor [6, 7]. Tolvaptan has been approved for the treatment of hyponatremia in the United States and Europe.
The pharmacokinetic and pharmacodynamic profiles of tolvaptan after a single oral dose have been reported by Shoaf et al. [8] in a cohort of primarily Caucasian healthy adult subjects. They reported that 72-hour cumulative urine volume was dose-dependently increased by tolvaptan at 60–480 mg; however, the cumulative urine volume and free water clearance were similar for all doses within 12 h postdose. These results suggest that the lowest dose of tolvaptan elicited maximal responses (i.e. 60 mg), and that higher doses prolong the duration of the diuretic effect. Therefore, to evaluate the pharmacodynamic characteristics of tolvaptan and the pharmacokinetic/pharmacodynamic relationship in more detail, it is necessary to investigate these properties at doses <60 mg. Therefore, we conducted a single-dose study using doses of 15–120 mg and multiple-dose studies using doses of 30–120 mg per day in healthy Japanese subjects. In addition, a food-effect study was performed to assess the effect of a standard Japanese meal on the pharmacokinetic characteristics of a single oral dose of 15 mg tolvaptan.
Methods
Study design and subjects
All studies were conducted at Kitasato University Research Center for Clinical Pharmacology, Tokyo, Japan, in accordance with the ethical principles of the Declaration of Helsinki, applicable regulatory requirements, and Good Clinical Practice. The Institutional Review Board approved each study. Written informed consent was obtained from each subject before entering the study.
The single-dose study was a randomized, single-blind, placebo-controlled, ascending-dose study. Tolvaptan 15 and 30 mg tablets were used as the active treatment and placebo tablets, which were indistinguishable in appearance from the active drug, were used as the control. Subjects were randomly assigned to receive either tolvaptan (n = 6) or placebo (n = 2) in each step, and a single dose of tolvaptan was then orally administered in the morning after a fast of at least 10 h. The doses of tolvaptan were 15, 30, 45, 60, 90 and 120 mg and the initial dose was 15 mg. Escalation to the next dose level was determined after reviewing the clinical data and safety assessments at each dose. Since one patient experienced serious treatment-emergent adverse events (TEAEs) with 30 mg tolvaptan, another eight subjects (two subjects for placebo) were evaluated at the same dose, and an intermediate dose (45 mg) was added.
We performed two multiple-dose, randomized, placebo-controlled, parallel-group studies at 30 and 60 mg (double-blind), and at 90 and 120 mg (single-blind) in an in-patient setting. Tolvaptan 30 mg tablets were used as the active treatment, and placebo tablets, which were indistinguishable in appearance from the active drug, were used as the control. The subjects were randomly assigned to receive either one of two doses of tolvaptan (n = 6 per group), or placebo (n = 6) in each study. The subjects were given a single dose of tolvaptan or placebo in the morning on Day 1 after a fast of at least 10 h, followed by a 48-hour wash-out interval. Subjects were then given tolvaptan or placebo once daily for 7 days (Days 3–9) in the morning after a fast of at least 10 h. Breakfast was served to 2 h postdose between Day 3 and Day 8.
The food-effect study was designed as a randomized, two-group, two-period open-label crossover study. Subjects were randomized to one of two groups and received a single dose of 15 mg tolvaptan under fasted conditions in the first period (Group A, n = 10) or under fed conditions in the first period (Group B, n = 10). After a 2–6-day wash-out period, the subjects received the second treatment.
Each study included healthy, non-smoker Japanese male volunteers aged 20–40 years with a body weight ranging from 90% to 120% of normal (body mass index, 18.5–25.0 kg/m2 in the food-effect study). Subjects were allowed to take water freely, except between 2 h before each dose to 2 h after each dose on Days 1–9, and the amount of water intake was recorded. The intake of St. John’s Wort products, or grapefruit and its processed products, which may potentially induce or inhibit CYP3A4, were prohibited from 1 to 2 weeks before the initial dose and throughout the study period. Patients taking other medications were eligible for the study.
Sample collection
Blood samples to determine tolvaptan concentrations were collected at the following time points: single-dose study: predose, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12, 24, 36, 48, 72, 96, 120 and 144 h postdose; multiple-dose studies: predose, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12, 24, 36 and 48 h postdose on Days 1 and 9, and predose on Days 4–8; food-effect study: predose, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12 and 24 h postdose. Blood samples were collected in heparinized vacuum tubes, gently mixed, and then immediately centrifuged at 4°C for 15 min at 2,000 × g to obtain plasma. Plasma was then stored at −20°C or below until assay.
Blood samples for pharmacodynamic analyses were collected at predose, 2, 4, 6, 8, 12, 24, and 48 h postdose in the single-dose study, and at predose, 2, 4, 6, 8, 12 and 24 h postdose on Days 1–9 in the multiple-dose studies. To determine the serum electrolyte concentration and serum osmolality, blood was also collected at 6 h postdose on Days 4 and 6 in the multiple-dose studies. Blood samples were collected into a vacuum tube containing EDTA-2Na or serum separators, gently mixed, and then immediately centrifuged (10 min, 2,000 × g) to separate the plasma, or were left to stand at room temperature until the blood had coagulated, and were then centrifuged (10 min, 2,000 × g) to separate the serum.
To determine urinary tolvaptan concentrations, urine volume, urinary electrolytes and urine osmolality, the subjects urinated completely just before dosing and at the following intervals: 0–2, 2–4, 4–6, 6–8, 8–12, 12–24 and 24–48 h postdose in the single-dose study; 0–2, 2–4, 4–6, 6–8, 8–12, 12–24 and 24–48 h postdose on Days 1 and 9, and 0–4, 4–8, 8–12 and 12–24 h postdose on Days 3–8 in the multiple-dose studies. Urine samples collected during each interval were homogeneously mixed and fractionated into 10-mL aliquots, and stored at −70°C or below until assay.
Pharmacokinetic analysis
Actual blood sample times were used for pharmacokinetic assessment. Plasma and urinary concentrations of tolvaptan and its metabolites were determined using a validated high-performance liquid chromatography-tandem mass spectrometry method. The lower limit of quantification of plasma tolvaptan concentration was 5 ng/mL in the single- and multiple-dose studies, and 2 ng/mL in the food-effect study. Tolvaptan concentrations below the lower limit of quantification were assigned a value of 0. Plasma and urinary concentrations of tolvaptan were summarized using descriptive statistics. The pharmacokinetic parameters were calculated by noncompartmental methods [9] using WinNonlin software (Pharsight Corp., St. Louis, MO, USA).
In the single-dose study, the following pharmacokinetic parameters were determined for tolvaptan: Cmax, AUCt, area under the plasma concentration-time curve from time 0 to time infinity (AUC∞), time to reach the maximum plasma concentration (tmax), terminal phase elimination half-life (t1/2,z), apparent clearance of the parent drug from plasma after extravascular administration (CL/F), cumulative urinary excretion rate per dose from 0 to 48 h postdose (fe,48hr).
In the multiple-dose studies, the following pharmacokinetic parameters were determined for tolvaptan: Cmax, tmax, t1/2,z, CL/F, area under the plasma concentration-time curve from time 0 to 24 h postdose (AUC24hr) on Days 1 and 9, fe,48hr on Day 1, and cumulative urinary excretion rate per dose from 0 to 24 h postdose (fe,24hr) on Day 9. The accumulation coefficient R8,ac (AUC24hr) was determined by dividing AUC24hr on Day 9 by that on Day 1.
In the food-effect study, Cmax, AUCt, tmax and t1/2,z were determined for tolvaptan.
Pharmacodynamic analysis
In the single- and multiple-dose studies, serum electrolyte concentration, serum osmolality, plasma AVP concentration, urinary electrolyte concentration, urine osmolality, free water clearance, urine volume (interval urine volume, cumulative urine volume, urine excretion rate) were evaluated.
Urine excretion rate (mL/hr) was determined by dividing the interval urine volume (mL) by the time of collection (hours). Interval urinary electrolyte excretion (mEq) was determined by multiplying the urinary electrolyte concentration (mEq/L) by interval urine volume (L). Free water clearance was determined using the formula: urine excretion rate (mL/min) × [serum osmolality (mOsm/L) – urine osmolality (mOsm/L)]/serum osmolality (mOsm/L). The value of serum osmolality in this formula was the mean value before and after each collection interval.
Safety evaluation
The safety evaluation of tolvaptan was based on the assessment of physical signs and symptoms, laboratory tests (hematology, clinical chemistry and urinalysis), vital signs (blood pressure, pulse rate and body temperature), body weight, and 12-lead or Holter electrocardiography.
Statistical analysis
In the single-dose study, linear regression analysis was performed on log-transformed Cmax and AUCt versus log-transformed dose to evaluate the dose-proportionality of Cmax and AUCt values. The 95% confidence interval (CI) of the slope of the regression line, which included the value 1, was considered to be dose-proportional [10]. In the food-effect study, the geometric mean ratios (GMR) of the fed to fasted conditions for Cmax and AUCt, and their 90% CIs, were calculated. Statistical analysis was performed using SAS software (SAS Institute Japan, Tokyo, Japan).
Results
Subject disposition and characteristics
The disposition of the subjects and their characteristics are summarized in Table 1. In the single-dose study, all 56 male subjects (42 tolvaptan/14 placebo) completed the study. The mean ages were 23.9 (range 20–34) years in the tolvaptan group and 23.0 (20–29) years in the placebo group. In the multiple-dose study with tolvaptan at doses of 30 and 60 mg, 12 subjects were treated with tolvaptan and six subjects received placebo, their mean ages were 23.3 (20–31) and 24.7 (20–29) years, respectively. One subject in the 60 mg dose group discontinued the study because of protocol deviations, and was excluded from the pharmacokinetic and pharmacodynamic analyses. The remaining 17 subjects completed the study. In the second multiple-dose study with tolvaptan at doses of 90 and 120 mg, 12 subjects were treated with tolvaptan and six subjects received placebo. The mean ages of the subjects were 26.8 (22–35) and 29.0 (22–36) years, respectively. One subject in the placebo group withdrew consent for personal reasons, and 17 subjects completed the study. In the food-effect study, the mean ages of the subjects were 24.0 (20–32) years in Group A and 24.7 (20–36) years in Group B. A total of 19 subjects completed the study, excluding one subject in group B who discontinued the study at the end of the first period because of an adverse event.
Pharmacokinetic characteristics
The mean plasma concentration of tolvaptan for 24 h after a single oral dose of 15–120 mg tolvaptan is shown in Fig. 1. A summary of the pharmacokinetic properties of tolvaptan is shown in Table 2. The plasma concentration of tolvaptan increased immediately, reaching peak levels within 2–3 h after the dose in each group. The mean Cmax and AUCt values for tolvaptan at doses of 15–120 mg were 135–661 ng/mL and 645–5,908 ng∙hr/mL, respectively, showing a dose-dependent increase. A log–log regression analysis of AUCt versus dose showed a slope of 1.10 with 95% CI (0.85, 1.26), which included the value 1, indicating dose proportionality. However, a log–log regression analysis of Cmax versus dose showed a slope of 0.71 and 95% CI (0.51, 0.92), which did not include the value 1, indicating nonlinearity with increasing dose. Median tmax and mean CL/F values were independent of dose across the dose range of 15–120 mg. t1/2,z increased with increasing dose, and the value for 120 mg tolvaptan was approximately 3 times longer than that for 15 mg tolvaptan. The cumulative urinary excretion rate of tolvaptan per dose appeared to reach a plateau within 48 h postdose; the mean fe,48-h was 0.12–0.25%, suggesting a low contribution of urinary excretion to the elimination of tolvaptan.

Mean plasma concentration of tolvaptan for 24 h after a single oral dose (a). Mean urine excretion rate (b) and mean free water clearance (c) during collection intervals for 24 h after a single oral dose of tolvaptan or placebo. Mean values are plotted at the midpoint of each urine collection interval
A summary of the pharmacokinetic characteristics of tolvaptan on Days 1 and 9 in the multiple-dose studies is shown in Table 3. The mean plasma concentrations of tolvaptan on Day 9 after multiple oral doses of 30–120 mg tolvaptan once daily for 7 days were similar to those after a single oral dose on Day 1 for all doses tested. The mean value of R8,ac (AUC24hr) on Day 9 ranged from 0.82 to 0.98 across the dose groups, indicating that tolvaptan did not accumulate in plasma after multiple dosing. The mean value of fe,24hr after multiple dosing did not greatly differ from those after single dosing, indicating that there were no obvious changes in the renal excretion of tolvaptan after multiple dosing.
In the food-effect study, the median tmax values after a single oral dose of 15 mg tolvaptan under the fasted and fed conditions were 2.0 and 3.0 h, respectively. The tmax was reached later in the fed condition than in the fasted condition. Cmax and AUCt values were both higher in the fed condition than in the fasted condition (Table 4). The Cmax and AUCt under fed conditions increased by 28% and 9%, respectively, compared with those under fasted conditions.
Pharmacodynamic characteristics
A summary of the urinary pharmacodynamic endpoints after a single oral dose of 15–120 mg tolvaptan is shown in Table 5. The time-courses of the mean urinary excretion rate and the mean free water clearance are shown in Fig. 1. The mean 24-hour cumulative urine volume after a single oral dose of tolvaptan generally increased dose-dependently, and the value for 120 mg tolvaptan (11945.8 mL) was approximately 4.6 times that for placebo. In addition, the amount of 24-hour water intake dose-dependently increased from 2087.2 (range 1,135–3,446) to 9796.7 (range 6,880–13,240) mL at doses of 15–120 mg with the increase in urine volume. The urine excretion rates rapidly increased after dosing and reached maximum values within 2–4 h. The maximum mean urine excretion rates increased dose-dependently and remained constant at approximately 700–800 mL/hr at doses of ≥60 mg (Fig. 1b).
Although 24-hour cumulative urinary excretion of sodium (Na+) at doses of ≥45 mg tolvaptan exceeded that with placebo, the amount excreted was only 1.6 times that with placebo, even at the highest dose of tolvaptan tested here (120 mg). The 24-hour cumulative urinary excretion of potassium (K+) at all doses of tolvaptan exceeded that with placebo. However, even at 90 mg tolvaptan, corresponding to the greatest excretion, the value was only 2.3 times that with placebo (Table 5).
Urine osmolalities were markedly decreased 0–2 h postdose at all doses of tolvaptan, and the excretion of hypotonic urine was observed. Free water clearance rapidly increased, reaching a maximum within 2–4 h (Fig. 1c). The 24-hour cumulative free water clearance showed a dose-dependent increase (Table 5).
The time-courses of mean change from baseline (predose) in serum Na+ and K+ concentrations, and the plasma AVP concentration after a single dose of tolvaptan or placebo are shown in Figs. 2 and 3. The serum Na+ concentration increased after dosing, showing a maximal change from baseline at 6–8 h postdose at all doses, except 45 mg tolvaptan, and the changes were greater than those in the placebo group, even at 24 h postdose. The mean change in serum Na+ concentration at 6 h postdose was 0.3 mEq/L with placebo versus 1.5–8.0 mEq/L with tolvaptan. The serum osmolality tended to increase within 6 h postdose, similar to the changes in serum Na+ concentration. The mean change in serum osmolality at 6 h postdose was 1.4 mOsm/L with placebo, and 8.0–14.5 mOsm/L with tolvaptan (data not shown). No changes in mean serum K+ concentration were found at any dose of tolvaptan throughout the study period. The plasma AVP concentration increased after dosing, and the changes in the tolvaptan groups exceeded those in the placebo group, even at 24 h postdose.

Time-courses for mean change from baseline in serum Na+ (a) and K+ (b) concentrations after a single oral dose of tolvaptan or placebo

Time-course for mean change from baseline in plasma arginine vasopressin (AVP) concentrations after a single oral dose of tolvaptan or placebo
Although 24-hour cumulative urine volume decreased slightly after multiple doses of tolvaptan compared with the single dose on Day 1, a sustained dose-dependent diuretic effect of tolvaptan was observed throughout the study (Fig. 4). The urine excretion rate increased rapidly with a time profile similar to that with single dosing (data not shown). The 24-hour cumulative urinary excretion of Na+ was slightly greater at tolvaptan doses ≥90 mg compared with placebo throughout the multiple dosing period (data not shown). Although 24-hour cumulative urinary excretion of K+ at doses of ≥60 mg or higher was approximately 2 times that with placebo for single dosing on Day 1, the difference diminished after multiple dosing (data not shown). A marked reduction in urinary osmolality was also observed during multiple dosing (data not shown). Free water clearance after multiple doses of tolvaptan for 7 days was positive at all doses, similar to that with single dosing, and exceeded those in the placebo group (data not shown).

24-hour cumulative urine volume after a single dose (Day 1) or multiple doses (Days 3–9) of tolvaptan or placebo (mean ± standard deviation)
The mean serum Na+ and K+ concentrations, and plasma AVP concentration after multiple doses of 30 or 120 mg tolvaptan or placebo are shown in Figs. 5 and 6. The serum Na+ concentration with 30 mg tolvaptan before and 24 h after dosing on Day 9 were similar to those with placebo. Although the predose serum Na+ concentration with 120 mg tolvaptan on Day 9 was higher than that for single dosing on Day 1, indicating an increase in serum Na+ concentration after 7 days of administration, the predose value was similar to that at 24 h postdose on Day 9. The magnitude of the increase in the serum Na+ concentration on Day 9 was smaller than that for single dosing on Day 1, indicating that the increase in serum Na+ concentration was not persistent after 7 days of dosing, even at high doses of tolvaptan. The serum K+ concentration with 30 and 120 mg tolvaptan on Day 9 was similar to that with placebo, and no obvious changes were observed after multiple dosing. Serum osmolality showed a similar pattern to the serum Na+ concentration at all doses, and no obvious changes were observed after multiple dosing (data not shown). The plasma AVP concentration on Day 9 in the 30 mg tolvaptan group was similar to that with single dosing on Day 1, but was higher with 120 mg tolvaptan on Day 9 than with single dosing on Day 1, even at 24 h postdose.

Serum Na+ (a) and K+ (b) concentrations after a single dose (Day 1) or after 7 days of dosing (Day 9) of 30 or 120 mg tolvaptan, or placebo (mean ± standard deviation). Data on Day 4 and Day 6 were obtained 6 h after dosing

Plasma arginine vasopressin (AVP) concentration after a single dose (Day 1) or after 7 days of dosing (Day 9) of 30 or 120 mg tolvaptan, or placebo (mean ± standard deviation)
Safety
Table 6 summarizes the TEAEs in each study. In the single-dose study, the most common TEAEs (reported by ≥2 subjects) in the tolvaptan groups were thirst (eight subjects), nasopharyngitis (4), headache not otherwise specified (NOS) (3), blood osmolarity increased (3), increased blood uric acid concentration (3), tachycardia NOS (2), and dizziness (2). All of these events were mild in severity. One subject given with 30 mg tolvaptan experienced two serious TEAEs (sinus arrest and bradycardia NOS) 4 h after tolvaptan administration, which were considered by the investigator to be possibly related to tolvaptan administration. However, these events resolved promptly without any specific treatment. No TEAEs leading to study discontinuation were observed, even at the maximum dose of 120 mg. The most common TEAE found in the food-effect study, was diarrhea, which was reported by two subjects in the fasted condition and by three subjects in the fed condition. All TEAEs found in the multiple-dose studies were mild in severity. The most common TEAEs in the tolvaptan groups were increased blood osmolarity (5 subjects), headache NOS (3), diarrhea NOS (3) and increased blood Na+ concentration (2); all were most likely caused by the pharmacological action of tolvaptan. No serious TEAEs or TEAEs leading to study discontinuation were reported during multiple dosing.
Discussion
Pharmacokinetic characteristics
Since it has become clear that tolvaptan is primarily metabolized via CYP3A4 [11], it was expected that racial differences in pharmacokinetic parameters would be minor for tolvaptan [12]. Therefore, we compared the pharmacokinetic data for Japanese subjects in present single-dose study with those reported by Shoaf et al., which mainly comprised Caucasian subjects (83%) [8]. The Cmax values (mean ± standard deviation) after a single oral dose of 60 and 120 mg tolvaptan were 315 ± 105 and 661 ± 276 ng/mL, for Japanese subjects, versus 450 ± 168 and 564 ± 124 ng/mL, for Caucasians. The AUC∞ values were 2,424 ± 606 and 6,071 ± 2,097 ng∙hr/mL for Japanese subjects, versus 3,660 ± 1,390 and 5,800 ± 1,640 ng∙hr/mL for Caucasians. Thus, these data for Japanese subjects (n = 6) were generally comparable with those for Caucasian subjects (n = 6), suggesting that there were no marked differences in the pharmacokinetic profile of tolvaptan between Japanese and Caucasian individuals. The increases in tolvaptan Cmax were not dose-proportional, consistent with the results reported by Shoaf et al. [8]. One of the reasons for this finding is considered to be a reduced absorption rate as a result of saturated tolvaptan absorption in the upper small intestine with increasing dose. Moreover, a dose-dependent increase in t1/2,z was also observed by Shoaf et al. [8]. This may be because tolvaptan dose-dependently prolonged the time to the last measurable time points, which were needed to calculate t1/2, and reduced the gradient of the fitted curves. The last measurable time-point was 36 h postdose for 15, 30 and 45 mg tolvaptan, 48 h postdose for 60 and 90 mg tolvaptan, and 96 h postdose for 120 mg tolvaptan.
In the assessment of the effect of food on the pharmacokinetics of 15 mg of orally administered tolvaptan, although the fed condition increased Cmax and AUCt by 28% and 9%, compared with the fasted condition, these differences were not considered to be clinically significant (data not shown). In this assessment, standard Japanese meals were given to the subjects. The other study investigated the effects of a standard Japanese meal and a high fat meal on the pharmacokinetics of tolvaptan, and the results revealed that there was no substantial difference between these meals (data not shown).
Pharmacodynamic characteristics
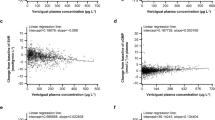
To assess the pharmacokinetic/pharmacodynamic relationship, individual data obtained in the single-dose study were plotted in scatter diagrams, and the correlations between 24-hour cumulative urine volume and AUC24hr are shown in Fig. 7. The 24-hour cumulative urine volume increased markedly and dose-dependently, and this increase was dependent on AUC24hr. The 24-hour cumulative urine volume at 60 mg tolvaptan was similar to that reported by Shoaf et al. [8]. As shown in Fig. 1, the urine excretion rates increased dose-dependently. Although the maximal urine excretion rate plateaued at doses ≥60 mg, the diuretic effect of tolvaptan tended to persist longer at higher doses. In addition, a decrease in urine osmolality and an increase in free water clearance were observed after a single dose of tolvaptan. Free water clearance reached a plateau at doses ≥60 mg, showing similar changes to the urine excretion rate. These findings suggested that the increase in urine excretion rate is related to the increase in free water clearance, and suggest an increase in water excretion (i.e. an aquaretic effect) by inhibition of the AVP V2-receptor. The previous single-dose study with doses ranging from 60 to 480 mg in Caucasian subjects [8] did not find marked dose-dependent increases in the cumulative urine volume for up to 12 h postdose. It was considered that 60 mg tolvaptan, the lowest dose tested in that study, elicited a maximal response. Their results were similar to those in the present study with Japanese subjects because urine excretion rate and free water clearance plateaued at a dose of 60 mg. Thus, it seems likely that the maximal urine excretion rate may not increase beyond 315 ng/mL, corresponding to the Cmax at a dose of 60 mg. Furthermore, since the urine excretion rate and the free water clearance at 10 h (8–12-hour collection interval) after a single dose of 15 mg tolvaptan were similar to those with placebo, a concentration of nearly 30 ng/mL at 8 h postdose seems to be the minimal effective concentration to induce pharmacological effects.

Correlation between 24-hour cumulative urine volume and plasmaAUC24hr after a single oral dose of 30–120 mg tolvaptan in individual subjects (n = 42)
The 24-hour cumulative urine volume decreased slightly after multiple doses of tolvaptan on Day 9 compared with that on Day 1 at all doses. Yamamura, et al. reported a slight decrease in urine volume several days after the initiation of 28-day multiple dosing of tolvaptan in rats [6], similar to our study in healthy subjects. However, although 24-hour cumulative urine volume decreased slightly, it remained steady at this new level, and no changes in the number and dissociation constant of AVP receptors in the liver and kidney between the treated and control groups, such as urine osmolality, were found after the multiple dosing. Therefore, the decrease in urine volume is not considered to be due to tolerance for tolvaptan. Since our study also shows that no change in urine osmolality is found between the first and seventh day of multiple dosing and that certain urine volume is maintained after Day 4 (second day of multiple dosing) or Day 5 (third day of multiple dosing), similar to the study in rats, we consider that the likelihood of tolerance for tolvaptan is low.
Our previous study in rats showed that the urinary Na+ excretion caused by tolvaptan was less than that caused by furosemide, after adjusting the dose of tolvaptan to obtain the same diuretic effect (urine volume) as furosemide [7]. Although the 24-hour urinary Na+ and K+ excretion with tolvaptan slightly exceeded those with placebo, both were much smaller compared with the published data for furosemide [7, 13]. Notably, the 24-hour urinary Na+ and K+ excretion after multiple doses of tolvaptan were not markedly different from those with placebo throughout the study period. Meanwhile, the serum osmolality and the serum Na+ concentration increased after dosing, and the amount of 24-hour water intake also increased with those increases.
Patients who are hospitalized with cardiac failure or hepatic cirrhosis, for example, often have fluid retention and consequent dilutional hyponatremia, which could seriously affect the clinical prognosis. Severe hyponatremia could lead to coma or death. The use of conventional saluretics is known to aggravate electrolyte disorders such as hyponatremia [2, 3]. In the present single- and multiple-dose studies, the serum Na+ concentration tended to increase within the normal range after tolvaptan administration, while the serum K+ concentration remained unchanged throughout the study period. These results indicated that tolvaptan is an aquaretic agent that increases the excretion of excessive water without significantly affecting the urinary excretion of electrolytes, and thus prevents a decrease in the serum Na+ concentration. Therefore, using tolvaptan can avoid worsening of electrolyte disorders such as hyponatremia associated with traditional diuretics. Moreover, coadministration of tolvaptan with furosemide or hydrochlorothiazide (HCTZ) demonstrated that furosemide and HCTZ did not adversely affect the aquaretic properties of tolvaptan, and tolvaptan did not affect the natriuretic activities of furosemide or HCTZ [14]. Thus, tolvaptan may offer clinically relevant benefits when coadministered with a loop diuretic or a thiazide diuretic [15, 16].
Safety
The most common TEAEs that occurred in the single-dose study were mild thirst, which mainly occurred at doses of ≥90 mg. Thirst was also the most commonly reported TEAE in the study by Shoaf et al. [8], and it was considered to be due to the pharmacological action of tolvaptan. In the present single-dose study, one subject experienced two serious TEAEs (sinus arrest and bradycardia NOS) at a low dose (30 mg) of tolvaptan. A marked increase in AVP (121 pg/mL) which was considered to be secondary to sinus arrest, was observed 4 h after dosing, which resulted in a large change in AVP in the 30 mg tolvaptan group (see Fig. 3). However, the Cmax value of this subject was the lowest (120 ng/mL) of the all the subjects in the same group. Additionally, sinus arrest was not observed in the previous single-dose study [8], even at a maximal Cmax value (i.e. 1,656 ng/mL). This subject had a medical history of dizziness upon standing; therefore, we could not exclude the possibility that his sinus node function had decreased before the study. Based on these findings, we considered it unlikely that the sinus arrest was directly caused by tolvaptan.
Conclusions
In conclusion, the Cmax and AUCt for a single oral dose of 15–120 mg tolvaptan increased dose-dependently. Furthermore, the increases in AUCt were dose-proportional. No accumulation of tolvaptan in plasma occurred after administration of 30–120 mg tolvaptan once daily for 7 days. The effects of food on the pharmacokinetics of tolvaptan were not considered to be clinically significant. Increases in urine excretion rate and free water clearance generally corresponded to the plasma concentrations of a single oral dose of tolvaptan, and reached a plateau at doses ≥60 mg. Although the 24-hour cumulative urine volume decreased slightly after multiple doses, compared with a single dose, a sustained dose-dependent diuretic effect was observed over time. Single and multiple oral doses of tolvaptan were well-tolerated at the doses tested (up to 120 mg) and no major safety concerns were noted in healthy Japanese subjects.
References
Schrier RW, Berl T, Anderson RJ. Osmotic and nonosmotic control of vasopressin release. Am J Physiol. 1979;236:F321–32.
Rivera-Santos A, Star RA. Sodium: volume depletion and hyponatremia. In: Seldin D, Giebisch G, editors. Diuretic agents: clinical physiology and pharmacology. San Diego: Academic Press Inc; 1997. p. 559–69.
Palmer BF. Potassium disturbances associated with the use of diuretics. In: Seldin D, Giebisch G, editors. Diuretic agents: clinical physiology and pharmacology. San Diego: Academic Press Inc; 1997. p. 571–83.
Lee CR, Watkins ML, Pattetson JH, et al. Vasopressin: a new target for the treatment of heart failure. Am Heart J. 2003;146:9–18.
Greenberg A, Verballs JG. Vasopressin receptor antagonists. Kidney Int. 2006;69:2124–30.
Yamamura Y, Nakamura S, Itoh S, et al. OPC-41061, a highly potent human vasopressin V2-receptor antagonist: pharmacological profile and aquaretic effect by single and multiple oral dosing in rats. J Pharmacol Exp Ther. 1998;287:860–7.
Hirano T, Yamamura Y, Nakamura S, Onogawa T, Mori T. Effects of the V(2)-receptor antagonist OPC-41061 and the loop diuretic furosemide alone and in combination in rats. J Pharmacol Exp Ther. 2000;292:288–94.
Shoaf SE, Wang Z, Bricmont P, Mallikaarjun S. Pharmacokinetics, pharmacodynamics, and safety of tolvaptan, a nonpeptide AVP antagonist, during ascending single-dose studies in healthy subjects. J Clin Pharmacol. 2007;47:1498–507.
Jusko WJ. Guidelines for collection and analysis of pharmacokinetic data. In: Evans WE, Jusko WJ, Schentag JJ, editors. Applied pharmacokinetics: principles of therapeutic drug monitoring, vol. 2. 3rd ed. Vancouver: Applied Therapeutics; 1992. p. 1–43.
Gough K, Hutchison M, Keene O, et al. Assessment of dose proportionality: report from the statisticians in the pharmaceutical industry/pharmacokinetics UK joint working party. Drug Inf J. 1995;29:1039–48.
Shoaf SE, Elizari MV, Wang Z, et al. Tolvaptan administration does not affect steady state amiodarone concentrations in patients with cardiac arrhythmias. J Cardiovasc Pharmacol Ther. 2005;10:165–71.
Myrand SP, Sekiguchi K, Man MZ, et al. Pharmacokinetics/genotype associations for major cytochrome P450 enzymes in native and first- and third-generation Japanese populations: comparison with Korean, Chinese, and Caucasian populations. Clin Pharmacol Ther. 2008;84:347–61.
Dodion L, Ambroes Y, Lameire N. A comparison of the pharmacokinetics and diuretic effects of two loop diuretics, torasemide and furosemide, in normal volunteers. Eur J Clin Pharmacol. 1986;31:21–7.
Shoaf SE, Bramer SL, Bricmont P, Zimmer CA. Pharmacokinetic and pharmacodynamic interaction between tolvaptan, a non-peptide AVP antagonist, and furosemide or hydrochlorothiazide. J Cardiovasc Pharmacol. 2007;50:213–22.
Schrier RW. The patient with hyponatremia or hypernatremia. In: Schrier RW, editor. Manual of nephrology. 4th ed. Boston: Little, Brown & Co; 1995. p. 20–36.
Zeidel ML. Special diuretics. In: Seldin D, Giebisch G, editors. Diuretic agents: clinical physiology and pharmacology. San Diego: Academic Press Inc; 1997. p. 113–34.
Acknowledgments
These studies were sponsored by Otsuka Pharmaceutical Co., Ltd, Japan. The authors gratefully acknowledge the volunteers and staff who participated in the studies.
None of the authors have any conflicts of interest associated with this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, S.R., Hasunuma, T., Sato, O. et al. Pharmacokinetics, Pharmacodynamics and Safety of Tolvaptan, A Novel, Oral, Selective Nonpeptide AVP V2-receptor Antagonist: Results of Single- and Multiple-Dose Studies in Healthy Japanese Male Volunteers. Cardiovasc Drugs Ther 25 (Suppl 1), 5–17 (2011). https://doi.org/10.1007/s10557-011-6299-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-011-6299-3