
Abstract
We sought to assess the tolerance and safety of adenosine-stress cardiovascular magnetic resonance (CMR) perfusion imaging in patients with coronary artery disease (CAD). We retrospectively examined all adenosine CMR perfusion scans performed in our centre in patients with known or suspected (CAD) and normal volunteers at either 1.5 or 3 T. All subjects were initially screened for contraindications to adenosine. The dose of adenosine infused was 140 μg/kg/min. Significant CAD was defined angiographically as the presence of at least one stenosis of >50% diameter. Data were collected from 351 consecutive subjects (mean age 62 ± 11 years, range 25–85 years-245 men). Of the 351 subjects, 305 had a coronary angiogram, the remaining 46 subjects were normal volunteers studied for research protocols. In total, 233 subjects (76%) were found to have significant CAD of whom 128 had multi-vessel disease. There were no deaths, myocardial infarctions, or episodes of bronchospasm during the CMR study. Transient 2nd (Mobitz II) or 3rd-degree atrioventricular (AV) block occurred in 27 patients (8%). There were no sustained episodes of advanced AV block. Transient chest pain was the most common side effect (199 subjects—57%). The use of intravenous adenosine in CMR perfusion imaging is safe and well-tolerated, even in patients with severe CAD. Where a careful screening policy for contraindications to adenosine is followed, serious adverse events in the CMR scanner are relatively rare and symptoms resolve following termination of the infusion, without the need for aminophylline.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Myocardial perfusion imaging involves stressing the heart with either physiological exercise or a pharmacological agent, which is usually a vasodilator such as adenosine or dipyridamole. These agents produce near-maximal vasodilatation in normal coronary arteries, resulting in an increment in coronary blood flow four to five times above normal. In myocardial segments supplied by a stenotic epicardial vessel resistance in the arteriolar level is already reduced in the resting state in order to maintain regional myocardial blood flow (i.e., coronary vasodilator reserve has been utilized), and only minor or no further reductions can take place. Thus, flow heterogenity occurs during vasodilator stress (increased in the normal territory and relatively unchanged in the territory supplied by the stenotic coronary artery), with areas beyond an arterial stenosis becoming relatively hypoperfused. The clinical rule of thumb in nuclear cardiology is that physiological exercise is performed in patients who can exercise and vasodilator stressors are used in patients who cannot.
Cardiovascular magnetic resonance (CMR) perfusion imaging has progressed rapidly over the past few years and has proven to be a sensitive modality to detect ischemia [1–7]. Because of the limited space within the magnet bore and the sensitivity to motion artifacts, physical stress is impractical, and hence stress CMR perfusion imaging is routinely performed during pharmacological stimulation. Adenosine is the most widely used pharmacological agent for CMR perfusion studies due to its extremely short half-life (<10 s) and transient nature of side effects [8]. Although the safety of perfusion imaging using adenosine has been confirmed in large-scale studies using radionuclide imaging, [9, 10] it is important to examine the safety of adenosine stress perfusion in an MR environment where ECG monitoring is less reliable and resuscitation requires rapid removal of the subject from the magnet.
The purpose of this study was to determine the safety and tolerance of adenosine infusion in conjunction with CMR first-pass perfusion imaging in patients with suspected or known coronary artery disease (CAD).
Methods
We retrospectively examined all adenosine CMR perfusion scans performed in our centre between 03/2003 and 03/2008 for clinical and research purposes in patients with known or suspected CAD and normal volunteers, at either 1.5 or 3 T. Information on safety and adverse events during and immediately after adenosine infusion were routinely recorded, together with hemodynamic data.
Study population
The study population consisted of both research (n = 313) and clinical (n = 38) patients. All research patients were enrolled in studies approved by the institutional research ethics committee. Patients with suspected or known CAD continued their medication as usual. All subjects were initially screened for the presence of contraindications to adenosine such as asthma, unstable angina or acute myocardial infarction within 2 weeks of the study, 2nd or 3rd degree atrioventricular (AV) block and bifascicular block. A 12-lead ECG was performed prior to the CMR scan. We did not proceed to adenosine administration if the patient reported caffeine ingestion within the last 24 h. Prior to the CMR scan a physician carefully explained the procedure to subjects with emphasis on potential adenosine-related symptoms. Subjects were continuously monitored with peripheral oxygen saturation, heart rate and 2-lead ECG throughout the CMR scan. Systemic blood pressure was periodically checked during the scan, and at every minute during and for at least 15 min after the infusion of adenosine. The monitor tracing during the CMR scan does not allow for identification of 1st or Wenckebach 2nd degree AV block and therefore only advanced degrees of AV block (Mobitz II 2nd degree and 3rd degree) were reported. Each subject was questioned during and immediately after termination of adenosine infusion, specifically for the occurrence of the following adverse events: shortness of breath or dyspnea, chest pain and other minor symptoms (flushing, nausea, headache). At least two cardiology fellows trained in cardiopulmonary resuscitation and CMR evacuation procedures were present during the adenosine infusion.
Adenosine infusion protocol
Adenosine (Adenoscan®, Sanofi-Synthelabo) was infused at 140 μg/kg/min through an antecubital vein using an accurate syringe pump (Graseby® 3500). Although the target time of the infusion was a minimum of 3 min, it was to be discontinued earlier in patients developing persistent or symptomatic 3rd degree AV block, severe hypotension (systolic blood pressure <90 mmHg) or bronchospasm. The attending physicians had aminophylline for adenosine receptor antagonism and nitroglycerine for persistent chest pain at hand, and a fully equipped crash trolley with defibrillator was easily accessible.
CMR imaging protocol
All CMR studies were performed using a 1.5 T (Siemens Sonata, Erlangen, Germany) or a 3 T clinical MRI scanner (Siemens Trio, Erlangen, Germany). During the last minute of adenosine infusion a gadolinium-based contrast agent (Gadodiamide, Omniscan, GE Healthcare) was administered intravenously (through a different from adenosine iv line) at 0.04–0.05 (for research scans) or 0.075 (for clinical scans) mmol/kg body weight (injection rate, 6 ml/s), followed by a 15 ml saline flush at the same rate. Perfusion imaging (echo time 1.04 ms, repetition time 2 ms, saturation recovery time 100 ms, voxel size 2.1 × 2.6 × 8 mm; flip angle 18° at 1.5 T and 17° at 3 T) was performed every cardiac cycle during the first pass, using a T1-weighted fast (spoiled) gradient echo sequence. Three or four short-axis slices, positioned from the base to the apex of the left ventricle, were obtained. The same imaging sequence was repeated 20 min later without adenosine to obtain perfusion images at rest.
Coronary angiography
All study participants, apart from the normal volunteers, underwent coronary angiography using standard techniques. Significant CAD was defined visually as the presence of at least one stenosis of >50% diameter in any of the main epicardial coronary arteries or their branches with a diameter of ≥2 mm.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as counts and percentages. All continuous variables were found to be normally distributed by the Kolmogorov–Smirnov test. Differences in continuous variables between groups (normals vs. single-vessel vs. multi-vessel disease) were assessed by one-way analysis of variance (ANOVA) followed by post hoc Tukey’s analysis. Comparisons of categorical variables between groups were performed by χ 2 test or Fisher’s exact test as appropriate. Bonferroni correction to adjust for multiple comparisons has been applied to P-values derived from χ 2 tests. A probability value of P < 0.05 was considered significant and two-tailed P values were used for all statistics. The SPSS statistical software (version 13.0; SPSS Inc., Chicago, Ill., USA) was used.
Results
Data were collected from 351 consecutive subjects (mean age 62 ± 11 years, range 25–85 years-245 men) of whom 305 had a coronary angiogram (the remaining 46 subjects were normal volunteers). 178 scans (51%) were performed at 1.5 T and 173 (49%) at 3 T. In total 233 patients (76%) were found to have significant CAD: 105 were patients with single-vessel disease, 74 with two-vessel disease and 54 with three-vessel disease, whereas 72 patients had no significant CAD. Table 1 shows the baseline characteristics of our subjects, and Fig. 1 shows two typical examples of perfusion studies. We divided our study population into three groups; normal subjects (normal volunteers and individuals with normal arteries on coronary angiography), single-vessel CAD patients, and multi-vessel CAD patients. In total there were 16 left main lesions, 175 left anterior descending lesions, 108 left circumflex and 130 right coronary artery lesions. The vast majority of our subjects (347 individuals—99%) successfully completed the infusion protocol. Four patients (1%) became extremely anxious during the adenosine infusion and requested termination of the CMR study.

Examples from CMR perfusion scans. Representative examples from CMR perfusion scans at adenosine stress (left panels) and rest (right panels). The top panels show the scan of a CAD patient with a significant left anterior descending stenosis. Note the reversible perfusion deficit in the anterior wall (white arrows). The bottom panels show the scan of a normal volunteer. Both CMR scans were performed at 3 T
Hemodynamic response to adenosine
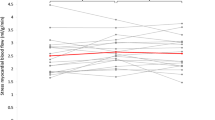
The mean duration of adenosine infusion was 244 ± 60 s with the target minimum duration of 3 min being achieved in 322 (92%) of our subjects. Table 2 shows the hemodynamic effects of adenosine in our subjects. Overall, there was a mild decrease (3 mmHg) in both systolic and diastolic blood pressure with a compensatory increase in heart rate (20 beats/min), resulting in a significant rise in rate-pressure product (23% increase at stress).
Adverse events
There were no deaths, myocardial infarctions, or episodes of bronchospasm or pulmonary edema in our cohort as a result of the stress CMR perfusion study. Transient advanced AV block (Mobitz II 2nd degree and 3rd degree) occurred in 27 subjects (8%), of whom 16 (7%) had significant CAD on angiography, whereas 11 individuals (9%) had normal coronary arteries (P = 0.42). There were no sustained episodes of advanced AV block. Patients under treatment with beta-blockers (n = 214) had similar incidence of advanced AV block (17 subjects—8%) compared with beta-blocker naïve subjects (10 out of 137 subjects—P = 0.83). More than half of our patients reported the presence of chest pain (199 subjects—57%), but in only 5 subjects (1%) was sublingual nitrate administration needed after the infusion was discontinued. Patients with CAD, and particularly multi-vessel disease, complained more frequently of chest pain compared to subjects without CAD (66% vs. 48%, P = 0.012). Several patients reported breathlessness (158 subjects—45%) or other vasodilator side effects like flushing, headache, dizziness (150 subjects—43%). However, all these symptoms resolved with termination of the infusion and no aminophylline reversal was required. The adverse effects of adenosine in our cohort are summarized in Table 3.
Discussion
This study reports the safety of adenosine administration for first-pass CMR perfusion imaging in a patient population with significant prevalence of CAD. Our findings show that adenosine is a highly suitable agent for CMR perfusion imaging as it is well-tolerated and safe even in patients with multi-vessel CAD. The main advantage of adenosine is the extremely short half-life (2–10 s), which makes its effects quickly reversible [8]. This is particularly useful when stressing patients in an MR environment, where there are many attendant difficulties with perfusion imaging, including the reduced robustness of ECG monitoring and the need for remote resuscitation in case of emergency.
Previous large prospective studies established the overall safety of adenosine stress testing in conjunction with radionuclide myocardial perfusion imaging [9, 10]. Over the last decade, CMR perfusion imaging has emerged as a sensitive diagnostic modality to detect ischemia, and several single-centre and multi-centre studies have reported excellent results for the detection of significant CAD using adenosine as the pharmacological stress agent [1–5]. Nevertheless, these studies focused on the diagnostic performance of CMR perfusion imaging in patients with suspected CAD rather than the safety profile of adenosine as a stressor agent in an MR environment. A recent study reported on the safety of adenosine-stress perfusion CMR on 35 patients early after ST-elevation myocardial infarction [11]. CMR was well tolerated, all subjects completed the study protocol and no complications occurred. A second CMR study that has specifically addressed the issue of safety of adenosine stress imaging has been conducted using a mobile 1.5 T cardiac magnetic resonance system. In this study Bernhardt et al. [12] reported no major complications after a 3-min infusion of adenosine in 574 patients. The same group has documented an excellent safety and tolerability profile of adenosine stress MR in 3,174 outpatients [13]. We also found only minor complications resulting from adenosine infusion. There are, however, some significant differences between our study and the studies by Bernhardt et al. [12, 13]. Firstly, 86% of our population had coronary angiography whereas Bernhardt and colleagues present angiographic data only on 70% of their cohort. Secondly, our data are derived from a well-defined population with significant CAD, and particularly multi-vessel disease, whereas most of the patients Bernhardt et al. studied had single vessel disease. Thirdly, we administered adenosine for longer (duration of infusion more than 3 min in 92% of our patients with an average of 4 min), whereas Bernhardt et al. used a 3-min infusion protocol. Importantly, our data indicate that CMR stress perfusion imaging is safe even in patients with multi-vessel disease.
Overall, adenosine infusion was well-tolerated in our cohort and only few minor side-effects were observed. All these resolved within several minutes of stopping the infusion and there was no need for aminophylline administration. Serious side effects such as death, myocardial infarction or serious arrhythmias were not observed. Importantly, adenosine infusion was the reason for terminating the CMR scan in only 4 subjects (1%) who suffered extreme anxiety during the infusion. As expected chest pain occurred frequently in our cohort. This was a common complaint mostly in CAD patients (61%), and particularly subjects with multi-vessel disease (66%), but was also frequent in normal volunteers (48%). Thus, the occurrence of chest pain is not a very reliable criterion to identify patients with CAD. The algogenic mechanism of adenosine is unclear—true myocardial ischemia is not always the cause of it. Interestingly, very few of our CAD patients required nitroglycerin administration to control the pain. Direct activation of myocardial nociceptors, which may occur even without ischemia in normal subjects, is another possible explanation for the chest pain following adenosine administration [14]. Dyspnea was another common side effect in our study population, which again terminated promptly after the infusion was discontinued. The sensation of breathlessness during adenosine administration can be attributed to stimulation of carotid chemoreceptors, which leads to an increase in respiratory rate and depth causing hyperventilation [15]. None of our patients had bronchospasm during adenosine infusion. This is likely to be due to our careful screening policy for asthma, although some studies have reported no major respiratory side-effects after adenosine administration even in patients with severe chronic obstructive pulmonary disease or asthma [16, 17]. Adenosine has also been associated with various degrees of heart block. The incidence of advanced AV block in our cohort is comparable with the published literature, and in all cases heart block was transient and terminated spontaneously without major hemodynamic effects [9, 10, 18]. Patients taking beta-blockers or calcium channel antagonists were not at increased risk for AV block.
One limitation of our study is that we did not follow up patients for more than 1 h after the CMR scans. Nevertheless, delayed or recurrent side effects one hour after the infusion of adenosine are very rare. Moreover, given its ultra-short half life of <10 s, any delayed events can not be attributed to adenosine with certainty.
In conclusion, the use of intravenous adenosine for CMR perfusion imaging is safe and well-tolerated even in patients with severe CAD. Where a careful screening policy for contraindications to adenosine is followed, serious adverse events in the CMR scanner are rare and symptoms resolve following termination of the infusion without the need for aminophylline.
References
Nagel E, Klein C, Paetsch I et al (2003) Magnetic resonance perfusion measurements for the noninvasive detection of coronary artery disease. Circulation 108:432–437. doi:10.1161/01.CIR.0000080915.35024.A9
Cheng AS, Pegg TJ, Karamitsos TD et al (2007) Cardiovascular magnetic resonance perfusion imaging at 3-tesla for the detection of coronary artery disease: a comparison with 1.5-tesla. J Am Coll Cardiol 49:2440–2449. doi:10.1016/j.jacc.2007.03.028
Klem I, Heitner JF, Shah DJ et al (2006) Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhancement infarction imaging. J Am Coll Cardiol 47:1630–1638. doi:10.1016/j.jacc.2005.10.074
Nandalur KR, Dwamena BA, Choudhri AF, Nandalur MR, Carlos RC (2007) Diagnostic performance of stress cardiac magnetic resonance imaging in the detection of coronary artery disease: a meta-analysis. J Am Coll Cardiol 50:1343–1353. doi:10.1016/j.jacc.2007.06.030
Schwitter J, Wacker CM, van Rossum AC et al (2008) MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomography for the detection of coronary artery disease in a multicentre, multivendor, randomized trial. Eur Heart J 29:480–489. doi:10.1093/eurheartj/ehm617
Bernhardt P, Levenson B, Albrecht A, Engels T, Strohm O (2007) Detection of cardiac small vessel disease by adenosine-stress magnetic resonance. Int J Cardiol 121:261–266. doi:10.1016/j.ijcard.2006.11.008
Burgstahler C, Kunze M, Gawaz MP et al (2008) Adenosine stress first pass perfusion for the detection of coronary artery disease in patients with aortic stenosis: a feasibility study. Int J Cardiovasc Imaging 24:195–200. doi:10.1007/s10554-007-9236-6
Wilson RF, Wyche K, Christensen BV, Zimmer S, Laxson DD (1990) Effects of adenosine on human coronary arterial circulation. Circulation 82:1595–1606
Cerqueira MD, Verani MS, Schwaiger M, Heo J, Iskandrian AS (1994) Safety profile of adenosine stress perfusion imaging: results from the Adenoscan Multicenter Trial Registry. J Am Coll Cardiol 23:384–389
Abreu A, Mahmarian JJ, Nishimura S, Boyce TM, Verani MS (1991) Tolerance and safety of pharmacologic coronary vasodilation with adenosine in association with thallium-201 scintigraphy in patients with suspected coronary artery disease. J Am Coll Cardiol 18:730–735
Greenwood JP, Younger JF, Ridgway JP et al (2007) Safety and diagnostic accuracy of stress cardiac magnetic resonance imaging vs. exercise tolerance testing early after acute ST elevation myocardial infarction. Heart 93:1363–1368. doi:10.1136/hrt.2006.106427
Bernhardt P, Steffens M, Kleinertz K et al (2006) Safety of adenosine stress magnetic resonance imaging using a mobile cardiac magnetic resonance system. J Cardiovasc Magn Reson 8:475–478. doi:10.1080/10976640600575270
Bernhardt P, Levenson B, Engels T, Strohm O (2006) Contrast-enhanced adenosine-stress magnetic resonance imaging—feasibility and practicability of a protocol for detection or exclusion of ischemic heart disease in an outpatient setting. Clin Res Cardiol 95:461–467. doi:10.1007/s00392-006-0410-y
Sylven C, Beermann B, Jonzon B, Brandt R (1986) Angina pectoris-like pain provoked by intravenous adenosine in healthy volunteers. Br Med J (Clin Res Ed) 293:227–230
Watt AH, Reid PG, Stephens MR, Routledge PA (1987) Adenosine-induced respiratory stimulation in man depends on site of infusion. Evidence for an action on the carotid body? Br J Clin Pharmacol 23:486–490
Balan KK, Critchley M (2001) Is the dyspnea during adenosine cardiac stress test caused by bronchospasm? Am Heart J 142:142–145. doi:10.1067/mhj.2001.116070
van Gaal WJ, Couthino B, Chan M, Allman KC (2008) The safety and tolerability of adenosine in patients with obstructive airways disease. Int J Cardiol 128:436–438. doi:10.1016/j.ijcard.2007.05.058
Lee J, Heo J, Ogilby JD et al (1992) Atrioventricular block during adenosine thallium imaging. Am Heart J 123:1569–1574. doi:10.1016/0002-8703(92)90811-9
Acknowledgments
This work was supported by the British Heart Foundation, the UK Medical Research Council, and the Oxford Partnership Comprehensive Biomedical Research Center with funding from the Department of Health’s NIHR Biomedical Research Centers funding scheme.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karamitsos, T.D., Arnold, J.R., Pegg, T.J. et al. Tolerance and safety of adenosine stress perfusion cardiovascular magnetic resonance imaging in patients with severe coronary artery disease. Int J Cardiovasc Imaging 25, 277–283 (2009). https://doi.org/10.1007/s10554-008-9392-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-008-9392-3