
Abstract
Purpose
In vitro and animal models suggest that the physiological effects of sleep apnea could contribute to cancer risk, yet epidemiologic studies have been inconsistent.
Methods
We identified a cohort of adults diagnosed with sleep apnea between 2005 and 2014 using regional administrative databases. Linking this cohort to a population-based cancer registry, we identified first incident cancers diagnosed after sleep apnea diagnosis through 2015. We calculated age–sex standardized cancer incidence ratios (SIRs) to compare the observed number of cancers among those with sleep apnea with expected population estimates over a comparable period.
Results
Among 34,402 individuals with sleep apnea, 1,575 first incident cancers were diagnosed during follow-up (mean ± SD; 5.3 ± 2.0 years). Compared to the general population, cancer incidence (SIR 1.26, 95% CI 1.20–1.32) was elevated among sleep apnea patients. We observed significantly elevated incidence for kidney (SIR 2.24, 95% CI 1.82–2.72), melanoma (SIR 1.71, 95% CI 1.42–2.03), breast (SIR 1.43, 95% CI 1.76–2.00), and corpus uteri (SIR 2.80, 95% CI 2.24–2.47) while risk for lung (SIR 0.66, 95% CI 0.54–0.79) and colorectal cancer (SIR 0.71, 95% CI 0.56–0.89) was lower.
Conclusion
These findings suggest an elevated cancer burden, particularly at certain sites, among individuals with diagnosed sleep apnea. Results should be interpreted with caution due to unmeasured confounders (e.g., BMI, diabetes).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sleep apnea is a sleep-related breathing disorder characterized by recurrent cessations of breathing during sleep, afflicting an estimated 25 million US adults [1]. These patients have increased risk for Type 2 diabetes, cardiovascular disease, depression, and motor vehicle accidents, as well as substantially elevated healthcare costs [2,3,4,5,6,7,8].
In recent years, evidence has emerged that sleep apnea may also be a risk factor for cancer development and progression. Both animal and in vitro cancer models show exposure to intermittent hypoxia and sleep fragmentation, two of the major hallmarks of sleep apnea, which could enhance oncogenic pathways [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. However, studies on the sleep apnea and cancer relationship in humans are inconsistent. Four retrospective cohort studies show that overall cancer incidence rates are higher among those with versus those without sleep apnea [25,26,27,28], while two more recent studies show no elevated risk [29, 30]. Additional studies have found a relationship between sleep apnea and increased cancer mortality [26, 31, 32].
Most prior epidemiologic studies on this potential connection have been limited by only exploring overall malignancy rates or associations with a limited number of specific cancer types. Studies considering specific cancer sites suggest an inverse relationship between sleep apnea and incident colon, rectum, prostate, and breast cancers [29], while others have reported increased risk for breast cancer [25, 33], cancers of the central nervous system [34], kidney cancer [29], melanoma [29], pancreatic cancer [29], and prostate cancer [25], in those with sleep apnea. To investigate gaps and to add to the current evidence regarding potential associations between sleep apnea and specific cancer types, we linked a cohort of individuals with a sleep apnea diagnosis to a population-based cancer registry in the Seattle-Puget Sound region (Western Washington State).
Methods
Study design
The study is a retrospective cohort leveraging the University of Washington Medicine (UWM) system and the Cancer Surveillance System (CSS) of Western Washington State; CSS is part of the NCI Surveillance, Epidemiology, and End Results (SEER) Program. The UWM system includes four regional hospitals and an extensive network of primary care neighborhood clinics. The UWM Sleep Center completes > 5,000 clinic visits and performs > 3,000 sleep studies (polysomnograms and home sleep apnea tests) per year.
Sleep apnea ascertainment
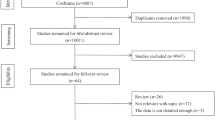
We extracted pertinent information from clinical and administrative databases maintained by the UWM system to identify a cohort of adults aged ≥ 20 years diagnosed with sleep apnea between January 2005 and December 2014 (n = 34,402). This cohort included individuals with obstructive and/or central sleep apnea; however, given that obstructive sleep apnea (OSA) (alone, or in combination with elements of central sleep apnea) accounts for the vast majority of sleep apnea cases (> 90%) [35], our results are most reflective of associations with OSA. We identified sleep apnea diagnoses based on International Classification of Diseases, Ninth Revision, Clinical Modification codes [ICD-9-CM] (codes 327.20, 327.21, 327.23, 327.27, 327.29, 780.51, 780.53, and 780.57). For individuals with multiple sleep apnea diagnoses recorded over the study period, the first such diagnosis was selected as their index diagnosis.
Cancer case ascertainment
Records for individuals diagnosed with sleep apnea in UWM databases were linked to the CSS to ascertain incident cancer diagnoses between January 2005 and December 2015. The CSS collects data on cancer incidence among residents of the 13 counties of Western Washington State. The registry catchment area covers a population of > 4 million people, with an average of 19,000 new cancer diagnoses in adults aged 20–79 years each year during our study period [36]. The UWM is located within the CSS catchment area.
Linkage to cancer registry records was done via expectation maximization algorithms to compute linkage probability scores for possible record pairs ranked by importance of various personal identifiers (first name, middle name, last name, date of birth, and social security number). Individuals could link to multiple CSS records if they were diagnosed with multiple cancers during the study period; however, our primary analyses were limited to each participant’s first cancer diagnosis during the study period.
We used International Classification of Diseases for Oncology, 3rd edition (ICD-03) codes to categorize cancer sites (Table 1). We used the CSS Summary Stage 2000 coding to classify cancer stage at diagnosis [37], allowing us to group incident cancers as in situ, localized, regional stage, or metastatic disease.
Other variables
Patient characteristics pulled from UWM clinical and administrative databases included the following: age at sleep apnea diagnosis, sex, race (White, Black, and others), Hispanic ethnicity (Hispanic, non-Hispanic), and healthcare utilization. Healthcare utilization was quantified as the total number of healthcare visits to UWM facilities and providers in the 5 years subsequent to sleep apnea diagnosis, including outpatient clinic visits and inpatient visits.
Statistical methods
We tabulated the overall and site-specific counts of first incident cancers that occurred after a sleep apnea diagnosis through 31 December 2015. For each member of the sleep apnea cohort, the expected number of person-years of follow-up was computed as the total years between their first sleep apnea diagnosis and cancer diagnosis, death, or end of follow-up (31 December 2015), whichever came first. We calculated age–sex standardized cancer incidence ratios (SIR) to compare the observed number of cancer cases among those with a sleep apnea diagnosis with the number expected based on cancer incidence rates in the underlying population of the Seattle-Puget Sound region over the study period [38]. To estimate the expected number of incident cases, we multiplied cancer incidence rates in sex-specific 5-year age and 10-year age categories (for overall and cancer site-specific analyses, respectively) for the underlying CSS population by the expected person-years in the corresponding age–sex bands of the sleep apnea cohort. The person-time of follow-up was distributed according to the person age with respect to each age bands, such that cohort members contributed person-time at risk to different age categories as they aged during follow-up. This allowed aging during follow-up to be accurately reflected in person-years at risk and consequently in the expected number of cancers. Cancer incidence rates for the CSS region were obtained from the SEER*Stat software [38] and SIR (including their 95% CI) estimates were calculated using the exact method in Stata 14.0 (College Station, Texas) [39].
Results
Baseline characteristics of the UWM sleep apnea cohort are provided in Table 2, both overall (n = 34,402) and for those with an incident cancer diagnosis subsequent to their sleep apnea diagnosis (n = 1,575) with a total of 181,674 person-years. Overall, the mean age in the sleep apnea cohort was 52 years at the time of sleep apnea diagnosis. The majority of individuals within the cohort were male (57%) and of White race (74%). Individuals with a cancer diagnosis subsequent to sleep apnea diagnosis were slightly older at sleep apnea diagnosis, but were otherwise demographically similar to the overall cohort. The mean duration follow-up after sleep apnea diagnosis was 5.3 ± 2.0 years.
Selected characteristics of incident cancers in the sleep apnea cohort are reported in Table 3. The median interval between sleep apnea and cancer diagnosis ranged from 1.3 years for kidney cancer to almost 3 years for breast cancer. The most common cancer sites were breast (15%), prostate (13%), melanoma (8%), lung (7%), kidney (6%), colorectal (5%), corpus uteri (5%), and pancreas (3%). With the exception of sex-specific cancers (i.e., breast, corpus uteri, prostate) and melanoma, the distribution of common cancer sites was similar in men and women within the study cohort. Among those diagnosed with cancer after sleep apnea diagnosis, 61% were diagnosed with as early stage disease (In situ/Localized) versus 50% in the underlying CSS population.
Overall, the incidence of cancer following sleep apnea diagnosis was higher than would be expected based on the general CSS population (SIR 1.26, 95% CI 1.06, 1.21). Cancer incidence was elevated in both men (SIR 1.13, 95% CI 1.06, 1.21) and women (SIR 1.41, 95% CI 1.31, 1.52) with sleep apnea. Of the specific cancer sites evaluated, significantly elevated cancer incidence was noted for kidney cancer (n = 100, SIR 2.24, 95% CI 1.82, 2.73) and melanoma (n = 129, SIR 1.71, 95% CI 1.42, 2.03). Incidence of these two specific cancer types was similarly elevated in men and in women (Table 4). Conversely, reduced incidence was reported for lung cancer (n = 115, SIR 0.66, 95% CI 0.65, 0.79) and colorectal cancer (n = 78, SIR 0.71, 95% CI 0.56, 0.89) (Table 4), with similar patterns in each gender. In sex-specific analyses, women with a prior sleep apnea diagnosis also experienced strongly elevated incidence for cancers of the corpus uteri (n = 84, SIR 2.80, 95% CI 2.24, 3.47) and breast (n = 227, SIR 1.43, 95% CI 1.25, 1.63).
When stratified by age, cancer incidence was most elevated among older adults with sleep apnea (age ≥ 60 years), with evidence of elevated incidence across all evaluated cancer sites (Table 5). Among individuals with sleep apnea aged < 60 years, cancer incidence for several sites was lower than expected; however, cancer incidence overall, and the incidence of melanoma, uterine, and kidney cancers remained elevated in this younger age group.
In addition, the risk of in situ (SIR 5.52, 95% CI 4.74, 6.39), localized (SIR 1.40, 95% CI 1.30, 1.50), regional stage (SIR 1.08, 95% CI 0.96, 1.22) and metastatic (SIR 1.20, 95% CI 1.07, 1.35) cancers were consistently elevated.
Discussion
In this study, we found that overall cancer incidence was about 26% higher in those with a diagnosis of sleep apnea than that expected in the general population. More specifically, we observed elevated incidences of kidney, melanoma, uterine, and breast cancers among those with sleep apnea, particularly among older individuals. In contrast, inverse associations were noted with respect to lung and colorectal cancers. These results suggest that sleep apnea may contribute to overall cancer risk, with a more pronounced association on select cancer sites.
Our findings are consistent with prior animal studies and in vitro models demonstrating the carcinogenic potential of intermittent hypoxia and sleep fragmentation, two hallmarks of sleep apnea. Intermittent hypoxia, defined as a temporary deprivation of adequate oxygen, promotes tumor growth and metastasis in melanoma-injected mice [9, 17, 40], and has been associated with resistance to radiation in cancer cell lines [19, 20, 41]. Among the suggested mechanisms underlying these effects, chronic intermittent hypoxia has been shown to contribute to the generation of excessive reactive oxygen species (leading to oxidative stress induced DNA damage) [10, 40, 42], sustained activation of inflammatory pathways [13, 43], alterations in the miRNA cargo of circulating exosomes [10, 44], and overexpression of the transcriptional regulator hypoxia-inducible factor-1alpha (HIF-1α) [19, 45, 46]. Overexpression of HIF-1α up-regulates proangiogenic mediators, such as Vascular Endothelial Growth Factor (VEGF), thereby stimulating tumor growth, whereas chronic activation of Nuclear factor κB (NFκB) promotes tumorigenesis [19, 45,46,47,48,49]. In particular, overexpression of HIF-1α enhances angiogenesis in clear cell renal cell carcinoma [50]. Persistent sleep fragmentation is also associated with accelerated tumor growth and progression via similar pathways to those recruited by intermittent hypoxia [10, 11, 13]. Therefore, these sleep apnea-induced physiologic changes may plausibly contribute to cancer initiation through the creation of a pro-inflammatory and immunosuppressive microenvironment [11, 13, 16].
A number of human studies are consistent with our findings. A 2012 study utilizing the Wisconsin Sleep Cohort noted a 4.8-fold elevation in cancer mortality among individuals with severe OSA relative to those without sleep-disordered breathing [31]. Two years later, two other studies using a community-based and clinic-based cohort respectively, reported an elevated cancer mortality in those diagnosed with sleep apnea [26, 32]. Subsequently, three studies found a significant association between sleep apnea and cancer incidence with risk ratios ranging from 1.7 to 2.5 [25,26,27]. However, more recent studies are inconsistent with these earlier findings. Kendzerska et al., found no significant association with cancer incidence when comparing OSA patients to the general population (HR 1.02; 95% CI 0.80–1.31) [30]. A meta-analysis of the 4 studies including 86,460 participants found no association between overall cancer incidence and sleep apnea (HR 1.04; 95% CI 0.92, 1.16) [51]. Another meta-analysis including one additional study on breast cancer [33] found an overall elevated risk [51]. Both studies noted cautionary interpretation of the results due to possibility of confounding by cancer risk factors, heterogeneity between studies, and the possibility of publication bias [51, 52]. These prior studies are also summarized in a recent study [53]. Additionally, in the largest study to date, Gozal et al., found no association between OSA and overall cancer risk (HR 0.98; 95% CI 0.90–1.00) [29].
The fact that some prior studies have observed no significant association between sleep apnea and cancer overall may reflect heterogeneity in the relationship of sleep apnea with risk of specific types of cancer. That is, investigations of associations with overall cancer incidence may obscure cancer site-specific associations. Specifically, our study found increased incidence of breast, melanoma, corpus uteri, and kidney cancers in patients with sleep apnea. However, we found reduced incidence with respect to lung and colorectal cancer. At least two prior studies also found an increased risk for breast cancer associated with sleep apnea [25, 33]. In their recent study, Gozal et al., reported no such association with breast cancer; however, they did report elevated incidence of melanoma and kidney cancers and reduced incidence of colorectal cancer among individuals with sleep apnea [29], consistent with our findings.
Furthermore, the sleep apnea and cancer incidence association was stronger in women than in men. However, given that our statistical approach using SIR estimates for men and women involves a different set of weights for each sex, we are unable to assess any potential statistical inference on this gender difference. Additionally, with respect to age, older adults seemed to have higher burden of cancer incidence in this sleep apnea cohort, a finding that has been recently corroborated in a prospective cohort [54]. This might imply that there are other important risk factors such as genetic susceptibility driving the cancer burden in the younger cohort, whereas sleep apnea remains an important risk factor for the older cohort. However, in a murine model of sleep apnea and lung cancer, old age was protective rather than deleterious, suggesting that type of cancer and age may be interactively implicated along with sleep apnea to modify their epidemiological characteristics [55]. Other reasons might be due to differential misclassification of sleep apnea in younger adults, since it is not only generally under-diagnosed in the population, but it is perceived as being more commonly present in older adults, thereby leading to higher proportion of younger subjects remaining undetected. However, incidence of kidney and corpus uteri cancers and melanoma remained elevated in both age groups, which is consistent with the overall estimates.
Lastly, our findings should be interpreted in the context of study limitations. In particular, we lacked data on several potential confounders of the association between sleep apnea and cancer, such as body mass index (BMI), smoking history and socioeconomic status (SES). For instance, being overweight or obese is an established risk factor for kidney, endometrial and breast cancer [56,57,58], as well as sleep apnea [59]. We retrieved BMI information for a random sample of the sleep apnea cohort and observed a high prevalence of obesity (42%) as compared to county-level estimates of adult obesity (22%) for the county in which UWM is located (i.e., King County). Therefore, it would be expected that the elevated incidence observed for these cancers could be lower if adjusted for BMI. However, based on the fact that other studies adjusting for BMI have also noted increased risk for these cancers associated with sleep apnea [25, 29, 33], and given that melanoma incidence (also elevated in our study) has not been consistently linked with BMI [60], lack of adjustment for BMI is unlikely to account for the entirety of our results. However, unadjusted BMI could explain some the association observed with sleep apnea for certain cancer sites such as uterine cancer [61, 62]. Diabetes, a comorbidity linked with both sleep apnea and cancer, could similarly contribute as an unmeasured confounder [63]. Although we posited smoking as another unmeasured confounder, the smoking prevalence (12%) reported in a random sample of the sleep cohort was consistent with rates reported in King County, the largest population of the CSS catchment area [64]. We also relied on administrative codes for identifying individuals with a sleep apnea diagnosis. It is possible that these codes were entered into medical records as part of a medical history rather than reflecting a primary diagnosis; however, we counted follow-up time from the time of the first recorded sleep apnea code during the study period. Our approach to identifying sleep apnea patients precluded us from distinguishing between mild and severe sleep apnea, potentially limiting the study sensitivity to detect significant associations with overall and specific cancer sites.
There are also some limitations implicit in our estimation of person time at risk. Firstly, although we restricted our investigation to cancers diagnosed after sleep apnea, both sleep apnea and cancer are diseases with latency periods that can span several years or decades prior to diagnosis; thus, we cannot be certain that sleep apnea was present before the initiation of a cancer. However, sensitivity analyses excluding the first year of follow-up after a sleep apnea diagnosis yielded an attenuated (but still significantly elevated) SIR of 1.07 (1.01, 1.14) for cancer overall as well as a consistent direction but attenuated risk for cancer sites.
Lastly, our ascertainment of cancer diagnoses was limited to the 13-county catchment area of the CSS cancer registry. As such, we could have missed other cancers diagnosed if or when individuals with sleep apnea moved outside the 13-county region. In addition, we had a relatively short follow-up period (mean 5.3 years); however, other studies with a longer duration of follow-up (> 10 years) [31, 34] have similarly found a putative link between sleep apnea and incidence of a specific cancer or cancer mortality. Furthermore, lumping OSA and CSA into one “sleep apnea” cohort might yield different results if looked at separately due to the pathophysiological differences between these two respiratory sleep disorders. However, given that the majority of our cohort are OSA patients, this is unlikely as also shown by the similar overall cancer incidence estimate when CSA cases are dropped in a sensitivity analysis (SIR 1.25 vs. 1.26).
A strength of our study compared to prior work is our relatively large sample size, which allowed us to evaluate associations with several specific cancer sites [53]. We also had the ability to link sleep apnea cases with a population-based cancer registry, allowing for more comprehensive identification of cancer cases in our cohort.
In conclusion, our study suggests that sleep apnea is a potential risk factor for cancer, and that this association likely differs across cancer sites. Given the widespread and highly treatable nature of sleep apnea, these findings may suggest potential opportunities for reducing population cancer burden if these associations were causal.
References
Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM (2013) Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 177(9):1006–1014. https://doi.org/10.1093/aje/kws342
Acker J, Richter K, Piehl A, Herold J, Ficker J, Niklewski G. Obstructive sleep apnea (OSA) and clinical depression—prevalence in a sleep center. Sleep and Breathing. 2016:1–8
Barger LK, Rajaratnam S, Wang W, OBrien CS, Sullivan JP, Quadri S (2015) Common sleep disorders increase risk of motor vehicle crashes and adverse health outcomes in firefighters. J Clin Sleep Med 11(3):233–240
Clark AJ, Salo P, Lange T et al. Onset of impaired sleep and cardiovascular disease risk factors: A longitudinal study.. 2016
Covassin N, Somers VK (2016) Sleep apnea, hypertension, and hemorrhagic stroke—déjà vu all over again. Journal of the American Society of Hypertension 10(3):197–200
Kendzerska T, Gershon AS, Hawker G, Tomlinson G, Leung RS (2014) Obstructive sleep apnea and incident diabetes. A historical cohort study. American journal of respiratory critical care medicine 190(2):218–225
Tarasiuk A, Reuveni H (2013) The economic impact of obstructive sleep apnea. Curr Opin Pulm Med 19(6):639–644. https://doi.org/10.1097/MCP.0b013e3283659e1e
Kao L, Lee H, Lin H, Tsai M, Chung S (2015) Healthcare service utilization by patients with obstructive sleep apnea: A population-based study. PloS one 10(9):e0137459
Li L, Ren F, Cao J, Chen B (2016) Relevant mechanism of intermittent hypoxia-induced melanoma lung metastases in a murine model of sleep apnea. CHEST Journal 149(4_S):A556–A556
Khalyfa A, Almendros I, Gileles-Hillel A et al (2016) Circulating exosomes potentiate tumor malignant properties in a mouse model of chronic sleep fragmentation. Oncotarget. https://doi.org/10.18632/oncotarget.10578
Zheng J, Almendros I, Wang Y et al (2015) Reduced NADPH oxidase type 2 activity mediates sleep fragmentation-induced effects on TC1 tumors in mice. OncoImmunology 4(2):e976057
Gozal D, Farré R, Nieto FJ (2015) Putative links between sleep apnea and cancer: From hypotheses to evolving evidence. CHEST Journal 148(5):1140–1147
Hakim F, Wang Y, Zhang SX et al (2014) Fragmented sleep accelerates tumor growth and progression through recruitment of tumor-associated macrophages and TLR4 signaling. Cancer Res 74(5):1329–1337. https://doi.org/10.1158/0008-5472.CAN-13-3014
Nanduri J, Prabhakar NR. Intermittent hypoxia: Mechanistic pathways influencing cancer. In: Impact of sleep and sleep disturbances on obesity and cancer. Springer; 2014:103–119
Miao Z, Zhao T, Wang Z et al (2014) Influence of different hypoxia models on metastatic potential of SGC-7901 gastric cancer cells. Tumor Biol 35(7):6801–6808
Zhang J, Guo X, Shi Y, Ma J, Wang G (2014) Intermittent hypoxia with or without hypercapnia is associated with tumorigenesis by decreasing the expression of brain derived neurotrophic factor and miR-34a in rats. Chin Med J (Engl) 127(1):43–47
Almendros I, Montserrat JM, Torres M et al (2013) Intermittent hypoxia increases melanoma metastasis to the lung in a mouse model of sleep apnea. Respiratory physiology neurobiology 186(3):303–307
Almendros I, Montserrat JM, Ramirez J et al (2012) Intermittent hypoxia enhances cancer progression in a mouse model of sleep apnoea. Eur Respir J 39(1):215–217. https://doi.org/10.1183/09031936.00185110
Wan J, Chai H, Yu Z et al (2011) HIF-1α effects on angiogenic potential in human small cell lung carcinoma. Journal of Experimental Clinical Cancer Research 30(1):1
Liu Y, Song X, Wang X et al (2010) Effect of chronic intermittent hypoxia on biological behavior and hypoxia-associated gene expression in lung cancer cells. J Cell Biochem 111(3):554–563
Rofstad EK, Gaustad J, Egeland TA, Mathiesen B, Galappathi K (2010) Tumors exposed to acute cyclic hypoxic stress show enhanced angiogenesis, perfusion and metastatic dissemination. International journal of cancer 127(7):1535–1546
Toffoli S, Michiels C (2008) Intermittent hypoxia is a key regulator of cancer cell and endothelial cell interplay in tumours. FEBS journal 275(12):2991–3002
Carmeliet P, Dor Y, Herbert J et al (1998) Role of HIF-1α in hypoxia-mediated apoptosis, cell proliferation and tumour angiogenesis. Nature 394(6692):485–490
Shweiki D, Itin A, Soffer D, Keshet E (1992) Vascular endothelial growth factor induced by hypoxia may mediate hypoxia-initiated angiogenesis. Nature 359(6398):843–845. https://doi.org/10.1038/359843a0
Fang H, Miao N, Chen C, Sithole T, Chung M (2015) Risk of cancer in patients with insomnia, parasomnia, and obstructive sleep apnea: A nationwide nested case-control study. Journal of Cancer 6(11):1140
Marshall NS, Wong K, Cullen S, Knuiman MW, Grunstein RR (2014) Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the busselton health study cohort. J Clin Sleep Med 10(4):355–362
Campos-Rodriguez F, Martinez-Garcia MA, Martinez M et al (2013) Association between obstructive sleep apnea and cancer incidence in a large multicenter spanish cohort. American journal of respiratory critical care medicine 187(1):99–105
Christensen AS, Clark A, Salo P et al (2013) Symptoms of sleep disordered breathing and risk of cancer: A prospective cohort study. Sleep 36(10):1429–1435. https://doi.org/10.5665/sleep.3030
Gozal D, Ham SA, Mokhlesi B (2016) Sleep apnea and cancer: Analysis of a nationwide population sample. Sleep 39(8):1493–1500. https://doi.org/10.5665/sleep.6004
Kendzerska T, Leung RS, Hawker G, Tomlinson G, Gershon AS (2014) Obstructive sleep apnea and the prevalence and incidence of cancer. CMAJ 186(13):985–992. https://doi.org/10.1503/cmaj.140238
Nieto FJ, Peppard PE, Young T, Finn L, Hla KM, Farré R (2012) Sleep-disordered breathing and cancer mortality: Results from the wisconsin sleep cohort study. American journal of respiratory critical care medicine 186(2):190–194
Martinez-Garcia MA, Campos-Rodriguez F, Duran-Cantolla J et al (2014) Obstructive sleep apnea is associated with cancer mortality in younger patients. Sleep Med 15(7):742–748. https://doi.org/10.1016/j.sleep.2014.01.020
Chang W, Liu M, Chang W et al (2014) Sleep apnea and the subsequent risk of breast cancer in women: a nationwide population-based cohort study. Sleep Med 15(9):1016–1020
Chen J, Hwang J (2014) Sleep apnea increased incidence of primary central nervous system cancers: A nationwide cohort study. Sleep Med 15(7):749–754
Foldvary-Schaefer NR, Waters TE (2017) Sleep-disordered breathing. Continuum (Minneap Minn) 23(4):Sleep Neurology):1093–1116. https://doi.org/10.1212/01.CON.0000522245.13784.f6
Surveillance, epidemiology, and end results program (SEER) seattle-puget sound registry. https://Seer.cancer.gov/registries/sps.html. Accessed 23 May 2017
Fritz AG, RHIT C, Hurlbut AA et al (2001) SEER summary staging manual-2000: codes and coding instructions. National Cancer Institute, Bethesda
Surveillance research program, national cancer institute SEER*Stat software (http://www.seer.cancer.gov/seerstat) version 8.3.4.
StataCorp (2015) Stata statistical software: release 14. StataCorp LP, College station
Almendros I, Gileles-Hillel A, Khalyfa A et al (2015) Adipose tissue macrophage polarization by intermittent hypoxia in a mouse model of OSA: effect of tumor microenvironment. Cancer Lett 361(2):233–239
Akbarpour M, Khalyfa A, Qiao Z et al (2016) Altered CD8+ T-cell lymphocyte function and TC1 cell stemness contribute to enhanced malignant tumor properties in murine models of sleep apnea. Sleep. https://doi.org/10.1093/sleep/zsw040
Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB (2010) Oxidative stress, inflammation, and cancer: How are they linked? Free Radic Biol Med 49(11):1603–1616
Hatfield SM, Kjaergaard J, Lukashev D et al (2015) Immunological mechanisms of the antitumor effects of supplemental oxygenation. Sci Transl Med 7(277):277ra30. https://doi.org/10.1126/scitranslmed.aaa1260
Gharib SA, Seiger AN, Hayes AL, Mehra R, Patel SR (2014) Treatment of obstructive sleep apnea alters cancer-associated transcriptional signatures in circulating leukocytes. Sleep 37(4):709–714, 714A–714T. https://doi.org/10.5665/sleep.3574
Ryan HE, Poloni M, McNulty W et al (2000) Hypoxia-inducible factor-1alpha is a positive factor in solid tumor growth. Cancer Res 60(15):4010–4015
Dewhirst MW (2007) Intermittent hypoxia furthers the rationale for hypoxia-inducible factor-1 targeting. Cancer Res 67(3):854–855
Wang JQ, Jeelall YS, Ferguson LL, Horikawa K (2014) Toll-like receptors and cancer: MYD88 mutation and inflammation. Front Immunol 5:367. https://doi.org/10.3389/fimmu.2014.00367
Madonna G, Ullman CD, Gentilcore G, Palmieri G, Ascierto PA (2012) NF-κB as potential target in the treatment of melanoma. J Transl Med 10(1):53
Li S, Qian X, Zhou W et al (2011) Time-dependent inflammatory factor production and NFκB activation in a rodent model of intermittent hypoxia. Swiss Med Wkly 141:w13309
Gudas LJ, Fu L, Minton DR, Mongan NP, Nanus DM (2014) The role of HIF1α in renal cell carcinoma tumorigenesis. J Mol Med 92(8):825–836
Zhang XB, Peng LH, Lyu Z, Jiang XT, Du YP (2017) Obstructive sleep apnoea and the incidence and mortality of cancer: a meta-analysis. Eur J Cancer Care 26(2):e12427
Shantha GPS, Kumar AA, Cheskin LJ, Pancholy SB (2015) Association between sleep-disordered breathing, obstructive sleep apnea, and cancer incidence: a systematic review and meta-analysis. Sleep Med 16(10):1289–1294
Martinez-Garcia MA, Campos-Rodriguez F, Barbe F (2016) Cancer and OSA: current evidence from human studies. Chest 150(2):451–463. https://doi.org/10.1016/j.chest.2016.04.029
Martinez-Garcia M, Campos-Rodriguez F, Nagore E et al (2018) Sleep-disordered breathing is independently associated with increased aggressiveness of cutaneous melanoma. A multicentre observational study in 443 patients. Chest. https://doi.org/10.1016/j.chest.2018.07.015
Torres M, Campillo N, Nonaka PN et al (2018) Aging reduces intermittent hypoxia-induced lung carcinoma growth in a mouse model of sleep apnea. Am J Respir Crit Care Med
Wang F, Xu Y (2014) Body mass index and risk of renal cell cancer: a dose-response meta-analysis of published cohort studies. Int J Cancer 135(7):1673–1686
Genkinger JM, Spiegelman D, Anderson KE et al (2011) A pooled analysis of 14 cohort studies of anthropometric factors and pancreatic cancer risk. Int J Cancer 129(7):1708–1717
Munsell MF, Sprague BL, Berry DA, Chisholm G, Trentham-Dietz A (2014) Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol Rev 36(1):114–136
Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL (2008) Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proc Am Thorac Soc 5(2):185–192
Shipman A, Millington G (2011) Obesity and the skin. Br J Dermatol 165(4):743–750
Bjørge T, Engeland A, Tretli S, Weiderpass E (2007) Body size in relation to cancer of the uterine corpus in 1 million norwegian women. Int J Cancer 120(2):378–383
Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L (2014) Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5.24 million UK adults. Lancet 384(9945):755–765
Shi Y, Hu FB (2014) The global implications of diabetes and cancer. Lancet 383(9933):1947–1948. https://doi.org/10.1016/S0140-6736(14)60886-2
https://www.doh.wa.gov/portals/1/documents/pubs/345-271-ChronicDiseaseProfileKing.pdf. Accessed 20 Feb 2018
Funding
This work was supported by NIH (Grant No. P30CA015704).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sillah, A., Watson, N.F., Schwartz, S.M. et al. Sleep apnea and subsequent cancer incidence. Cancer Causes Control 29, 987–994 (2018). https://doi.org/10.1007/s10552-018-1073-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-018-1073-5