
Abstract
Purpose
Studies have reported an increased risk of childhood leukemia associated with exposure to magnetic fields. We conducted a large records-based case–control study of childhood leukemia risk and exposure to magnetic fields from power lines in California.
Methods
The study included 5,788 childhood leukemia cases (born in and diagnosed in California 1986–2008) matched to population-based controls on age and sex. We calculated magnetic fields at birth addresses using geographic information systems, aerial imagery, historical information on load and phasing, and site visits.
Results
Based on unconditional logistic regression controlling for age, sex, race/ethnicity, and socioeconomic status using subjects geocoded to a basic standard of accuracy, we report a slight risk deficit in two intermediate exposure groups and a small excess risk in the highest exposure group (odds ratio of 1.50 (95% confidence interval [0.70, 3.23])). Subgroup and sensitivity analyses as well as matched analyses gave similar results. All estimates had wide confidence intervals.
Conclusion
Our large, statewide, record-based case–control study of childhood leukemia in California does not in itself provide clear evidence of risk associated with greater exposure to magnetic fields from power lines, but could be viewed as consistent with previous findings of increased risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over 35 epidemiologic studies have investigated the association of childhood leukemia with residential low-frequency magnetic fields or physical surrogates of magnetic fields [1]. Three pooled analyses have found an increased risk of childhood leukemia for relatively high estimated residential magnetic field exposure [2,3,4]. The consistent association found between childhood leukemia and average magnetic field exposure above 0.3–0.4 µT could be due to chance, selection bias, misclassification, other factors which confound the association, or true causal relationship. As explanation for both individual results and pooled efforts is lacking, selection bias seems as the most likely explanation, but uncertainty remains and other explanations outlined above are possible. This study aims to address this uncertainty by minimizing bias, misclassification, and chance.
All studies necessarily use a surrogate measure for the retrospective magnetic field exposure that occurred years to decades in the past. Such surrogates include the configuration of power line wiring, from both distribution and high voltage overhead transmission lines [5,6,7]; present day measurement of magnetic fields within residences [8, 9] or present day personal measurements [10, 11]; distance to transmission lines [12,13,14]; or historical calculated fields [15,16,17,18,19,20]. Each approach has distinct advantages and limitations.
The advantages of using calculated fields include efficient inclusion of large numbers of subjects, elimination of the need for subject participation and thus minimization of selection and participation bias, the ability to conduct procedures blinded to case/control status and thus minimize information bias, and the ability to model the historical exposures of most relevance.
The California Power Line Study (CAPS) is a population-based case–control study focusing on childhood leukemia. We previously reported on childhood leukemia risk in relation to the distance from birth address to nearby power transmission lines [14]. The current paper presents analysis of childhood leukemia risk in relation to the residential exposure to extremely low-frequency magnetic fields from nearby transmission lines and is the first study of calculated fields and childhood leukemia in the US.
Methods
The study design, including methods of case ascertainment and control selection [21], methods for calculated fields [22], and estimation of distance from birth residence to transmission lines and associated risks [14] have been previously described. We summarize them briefly here.
Case ascertainment and control selection
The statewide population-based California Cancer Registry [23] was used to identify all childhood leukemia cases diagnosed between 1988 and 2008 among children younger than 16 years of age and residing in California at the time of diagnosis. Cancer incidence reporting is mandatory in California, and the CCR meets or exceeds all standards of the Surveillance, Epidemiology, and End Results Program and North American Association of Central Cancer Registries, with over 99% coverage of incident cancers.
A total of 6,645 childhood leukemia cases meeting inclusion criteria were identified from the CCR. Cases were linked to the California Birth Registry (CBR; California Department of Public Health, Vital Statistics Branch). Linkage was successful for 87.1% of leukemia cases (n = 5,788). A primary control for each case was randomly selected from the CBR and matched to the corresponding case (1:1) on date of birth (±6 months) and sex. Controls were eligible only if they had not been diagnosed with any type of cancer in California prior to the time of diagnosis of the corresponding case.
Variables obtained from the CBR, for both cases and controls, included mother’s residential address at time of birth, date of birth, sex, race/ethnicity of parents, birth weight, maternal and paternal ages, maternal and paternal education, and source of payment for delivery. There was substantial missingness on some variables due largely to differences in the information collected on birth certificates from year to year (e.g., maternal education) [24]. No substantial differences in patterns of missingness were detected between cases and controls.
Residential address information
All birth addresses were geocoded using the University of Southern California Geographic Information System (GIS) Laboratory’s open-source geocoder [25]. Depending on the completeness of the address, geocode matches were tax-assessor parcel centroid, street segment centroid, street centroid, US Postal Service ZIP Code Tabulation Area (ZCTA) centroid, town/city centroid, county centroid, or state centroid (for those with unknown addresses).
Calculated fields
A three-tiered approach was used to ascertain distance from home address to nearby overhead transmission lines and identify homes for calculated fields work [21]. (1) For all residences in geographic areas covered by the GIS databases of the four largest electric power companies in California (covering over 85% of California residences), we used these databases to determine distance to transmission lines over 100 kV within 2000 m of the residence. Information on lines with lower voltages (above 60 kV) was also available for two companies. (2) For residences with transmission lines within 200 m and for residences in the service area of smaller utilities (about 7% of subjects), we conducted Google Earth aerial imagery evaluation. (3) For residences which were located at a distance of 80 m from 100 to 200 kV lines, 150 m from 200 to 345 kV lines, or 200 m from 500 kV lines, the magnetic field contribution by the overhead transmission lines to the overall residential environment was assumed to be negligible. For the rest, we conducted site visits and collected detailed data on precise distances and the physical configuration and dimensions of lines near the residence. Phasing, loading, and directional load flow data for years of birth and diagnosis for each subject were obtained. Details on modeling of load and phasing when utility data were missing are presented elsewhere [22]. Magnetic fields were calculated using the EMF Workstation [EPRI, Versions 2010–2013, Palo Alto, CA] and were estimated at the center, closest, and farthest point of each residence.
Statistical analysis
The statistical analysis followed an a priori developed analysis plan, which specified both main and secondary analysis. The main analysis included all cases of leukemia and primary controls with geocode accuracy of street segment or parcel level, which was achieved for 88.5% of the geocoded addresses. The exposure variable was the calculated fields value for the center of the residence, categorized as <0.1 µT (reference group), 0.1–0.2, 0.2–0.4, or ≥0.4 µT; these cutpoints have been used in previous pooled analyses and provided sufficient numbers (at least five cases and five controls) in the highest exposure category for our analyses. Because the geocode accuracy restriction produced unmatched subjects, to maximize the use of available data, we used unconditional logistic regression controlling for the matching variables (sex, date of birth) to estimate odds ratios (ORs). We also controlled for race/ethnicity (White, Black, Asian, Hispanic, Other) and socioeconomic status (SES) using a composite indicator [14]. For comparison, we repeated the analysis several ways: unconditional logistic regression (1) controlling for sex and age at diagnosis only and (2) controlling for an extensive set of potential confounders (sex, date of birth, race/ethnicity, gestational age, birth weight, paternal age, maternal age, maternal years of education, paternal years of education, birth order, payment source for delivery, payment source for prenatal care, and census-based socioeconomic status indicator); conditional logistic regression utilizing the case–control matching on sex and age (3) without control for race/ethnicity and SES; (4) with control for race/ethnicity and SES; and (5) controlling for the extensive confounder set. Race/ethnicity and/or socioeconomic status were missing for 4.9% of subjects and were multiply imputed for all analyses. Missing confounders in the extensive set were also multiply imputed. Multiple imputation was conducted using chained equations and 10 imputations [26, 27].
As a priori specified secondary analyses, we conducted subgroup analyses: restricted to acute lymphocytic leukemia (ALL) cases and controls; stratified by age at diagnosis; and excluding subjects with Down’s syndrome.
We conducted sensitivity analyses that examined various uncertainties: (1) using all subjects regardless of geocode accuracy (i.e., including a 10% matched at zip code level and few more at other geography matches); (2) restricting to subjects from the major four utilities; (3) excluding subjects born in 1996, a year during which birth certificates were being transitioned to electronic format and the availability of residential address data was limited to zip code for some; (4) restricting to subjects with site visits; and (5) restricting to site-visit subjects with lower uncertainty in calculated field estimates, defined as having at most one major source of uncertainty out of three possible sources [22]. Based on recent publications, we added analysis (6) by the decade of birth year (e.g., [28] and [7]) and an analysis restricted to single family residences (site visits only).
We also report analyses using a natural cubic spline to model calculated fields. Spline modeling was conducted using R software [29]; other analyses were conducted using Stata 13.
Results
The study included 5,788 childhood leukemia cases and an equal number of controls. There were more males than females. Race/ethnicity and SES classification were available for more than 95% of subjects. About 84% of subjects were geocoded at the street segment or parcel level. Additional characterization of the study subjects can be found in previous papers [21, 24, 30, 31].
Table 1 presents results of both unmatched and matched analyses with minimal as well as more complete control for potential confounders. Unmatched analyses are restricted to subjects with geocode matching to the street segment or parcel level. Matched analyses are not restricted by geocode accuracy to avoid loss of pairs for whom matching accuracy differed. Results of all analyses were remarkably consistent, with a slight risk deficit in two intermediate exposure groups and a small risk excess in the highest exposure group, e.g., OR of 1.50 (95% CI [0.70, 3.23]) for the main analysis, unconditional logistic regression adjusted for age, sex, race/ethnicity, and SES. All results were imprecise and not statistically significant. For the remainder of the paper, we focus on unconditional logistic regression controlling for age, sex, race/ethnicity, and SES with geocoding at street segment or parcel level.
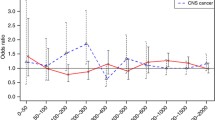
The restricted cubic regression spline showed an increasing OR with increasing exposure, but with wide confidence intervals at high exposure levels (Fig. 1).

Regression spline analysis. From unconditional logistic regression controlling for age, sex, race/ethnicity, and socioeconomic status and using a restricted cubic spline with three knots for calculated fields. Pointwise odds ratios and 95% confidence intervals. Reference line at 1.0
Table 2 provides subgroup analyses for childhood leukemia. Results were very similar to those using the total sample, particularly in the highest exposure group, when restricting to acute lymphocytic leukemia, when stratified by age at diagnosis, or when excluding subjects with Down’s syndrome.
In sensitivity analyses we examined the influence of various sources of uncertainty, such as geocoding accuracy, precise location of residence, and uncertainty in the calculated magnetic fields, on the results (Table 3). Including subjects with low geocode accuracy (i.e., those matched to U.S. Postal Service ZIP Code Tabulation Area, town/city, county or state) or focusing only on major four utility catchment areas (for whom more detailed information was available) did not appreciably change results. When restricted to site-visited residences for which more detailed information was collected, the odds ratio slightly increased but remained imprecise. However, the odds ratio did not further increase when the analysis was further restricted to subjects with low uncertainty scores (those expected to have high quality of calculated fields) or to single family residences (for whom calculated fields are thought to provide better estimates of exposure). Excluding subjects born in 1996, the transitional year for converting to electronic birth record information, did not appreciably change the results. We observed a slightly higher risks for single family homes in the highest exposure group. Analysis by decades of exposure did not reveal substantial changes in risk estimates.
Discussion
We have conducted a large, statewide, record-based case–control study of childhood leukemia in California. Consistent with many other studies, we found small, non-significant increased risks in the highest category of magnetic fields exposure. These findings are also consistent with the findings from the CAPS distance study, where slightly elevated risk estimates were found at residential distances of within 50 m of a power line [14]. While we saw an increase in risk in the highest exposure group, all confidence intervals included the null value and we did not observe stronger associations in subgroups with more reliable exposure assessment. For example, risk estimates were similar in magnitude with improved geocoding accuracy. On the other hand, we observed some increase in risk for site-visited subjects, for whom magnetic fields were calculated. With the better quality exposure assessment, we anticipate that higher associations might be observed if a relationship between magnetic fields and childhood leukemia exists. However, within the site-visited subgroup, risk estimates were not higher for those with low uncertainty score for their magnetic fields calculation. Also we did not find a pronounced increase in risk among those diagnosed prior to age 4 years, for whom birth addresses might be more indicative of a lifetime exposure. Consistent with a Swedish study, we observed a slightly higher risks for single family homes in the highest exposure group. Analysis by decades of exposure did not confirm higher risks in earlier decades as seen in the UK and Danish studies, but our observations do not go back far enough and do not include decades for which these studies observed higher risks.
Moreover, we did not find a stronger association for acute lymphocytic leukemia, as might be expected with a more specific disease definition, should an association exist.
We used population-based registries with complete registration of births and cancers, which eliminated participation bias and differential information bias (recall bias). Misclassification of outcome status is also unlikely in our study due to the completeness and high accuracy of the CCR and the high proportion of cases with successful linkage to the CBR. In addition, all aspects of exposure assessment were blind to case/control status.
A potential disadvantage of basing exposure on high voltage lines is that other sources of residential high magnetic fields are ignored and hence some individuals may be misclassified as not highly exposed (reducing sensitivity). However, when exposure prevalence is low, as is the case for high magnetic fields, the odds ratio estimate is more influenced by specificity than by sensitivity. Our detailed three-stage exposure assessment methodology incorporated several improvements in the assessment of exposure, including more precise measurements of distance and consideration of complex line configurations. This allowed us to achieve high specificity in exposure assessment, which is essential for examining the association between magnetic fields and childhood leukemia risk [22].
Our study had a much larger number of cases and controls in the highest exposure category than in other studies of similar design. This could be due to more residential construction near existing lines or, possibly, higher loads on California lines due to higher energy consumption. Larger numbers in the highly exposed groups allowed us to examine risks in various strata and several methodologic issues raised by previous studies. Despite larger numbers overall, small numbers in some of the subgroup and sensitivity analyses made these results imprecise and difficult to interpret with confidence.
Larger number of highly exposed, elimination of participation and information bias, use of comprehensive cancer and birth registries, and several improvements in exposure assessment are strengths of CAPS that overcome important limitations of many previous studies.
There were some differences in residential mobility between cases and controls in the study. Cases had to be born in California and diagnosed in California, whereas controls must have been born in California but were not required to be residing in the state at the time of diagnosis of the corresponding case. Although some controls who had moved out of state could have been diagnosed with childhood leukemia, this is highly unlikely because the outcome is rare. Mobility can manifest as a selection bias, confounding, increased measurement error, or could also be a potential risk factor [32]. Mobility remains a potential source of questions and an important area for future research. We plan to examine the potential influence of mobility on our results in the future work through case only analysis.
A possible limitation of the study is missing data on potential confounders. However, since information was missing mainly due to differences in the information collected on birth certificates from year to year rather than non-response, the potential for biases is small. In fact, our cases and controls had similar levels of missing values on all variables considered, and multiple imputation of missing data did not change the results. Excluding subjects born in 1996 and subjects with Downs syndrome did not change the results. Unmeasured confounding was also possible; more comprehensive study of potential confounders such as air pollution and pesticide exposure might prove informative.
In conclusion, our large, statewide, record-based case–control study of childhood leukemia cancer in California does not provide clear evidence of risk associated with higher exposure to magnetic fields, but small risks identified in previous studies cannot be excluded.
References
Kheifets L, Shimkhada R (2005) Childhood leukemia and EMF: review of the epidemiologic evidence. Bioelectromagnetics 26(S7):S51–S59
Ahlbom A, Day N, Feychting M et al (2000) A pooled analysis of magnetic fields and childhood leukaemia. Br J Cancer 83(5):692–698
Greenland S, Sheppard AR, Kaune WT et al (2000) A pooled analysis of magnetic fields, wire codes, and childhood leukemia. Childhood Leukemia-EMF Study Group. Epidemiology 11(6):624–634
Kheifets L, Ahlbom A, Crespi CM et al (2010) Pooled analysis of recent studies on magnetic fields and childhood leukaemia. Br J Cancer 103(7):1128–1135
Wertheimer N, Leeper E (1979) Electrical wiring configurations and childhood cancer. Am J Epidemiol 109(3):273–284
Savitz DA, Wachtel H, Barnes FA et al (1988) Case–control study of childhood cancer and exposure to 60-Hz magnetic fields. Am J Epidemiol 128(1):21–38
London SJ, Thomas DC, Bowman JD et al (1991) Exposure to residential electric and magnetic fields and risk of childhood leukemia. Am J Epidemiol 134(9):923–937
Linet MS, Hatch EE, Kleinerman RA et al (1997) Residential exposure to magnetic fields and acute lymphoblastic leukemia in children. N Engl J Med 337(1):1–8
Kabuto M, Nitta H, Yamamoto S et al (2006) Childhood leukemia and magnetic fields in Japan: a case–control study of childhood leukemia and residential power-frequency magnetic fields in Japan. Int J Cancer 119(3):643–650
McBride ML, Gallagher RP, Theriault G et al (1999) Power-frequency electric and magnetic fields and risk of childhood leukemia in Canada. Am J Epidemiol 149(9):831–842
Green LM, Miller AB, Agnew DA et al (1999) Childhood leukemia and personal monitoring of residential exposures to electric and magnetic fields in Ontario, Canada. Cancer Causes Control 10(3):233–243
Draper G, Vincent T, Kroll ME, Swanson J (2005) Childhood cancer in relation to distance from high voltage power lines in England and Wales: a case–control study. BMJ 330(7503):1290
Sermage-Faure C, Demoury C, Rudant J et al (2013) Childhood leukaemia close to high-voltage power lines—the Geocap study, 2002–2007. Br J Cancer 108(9):1899–1906
Crespi CM, Vergara XP, Hooper C et al (2016) Childhood leukaemia and distance from power lines in California: a population-based case–control study. Br J Cancer 115(1):122–128
Feychting M, Alhbom M (1993) Magnetic fields and cancer in children residing near Swedish high-voltage power lines. Am J Epidemiol 138(7):467–481
Verkasalo PK, Pukkala E, Hongisto MY et al (1993) Risk of cancer in Finnish children living close to power lines. BMJ 307(6909):895–899
Tynes T, Haldorsen T (1997) Electromagnetic fields and cancer in children residing near Norwegian high-voltage power lines. Am J Epidemiol 145(3):219–226
Pedersen C, Johansen C, Schuz J et al (2015) Residential exposure to extremely low-frequency magnetic fields and risk of childhood leukaemia, CNS tumor, and lymphoma in Denmark. Br J Cancer 113(9):1370–1374
Kroll ME, Swanson J, Vincent TJ, Draper GJ (2010) Childhood cancer and magnetic fields from high-voltage power lines in England and Wales: a case–control study. Br J Cancer 103(7):1122–1127
Bunch KJ, Swanson J, Vincent TJ, Murphy MF (2016) Epidemiological study of power lines and childhood cancer in the UK: further analyses. J Radiol Prot 36(3):437–455
Kheifets L, Crespi CM, Hooper C et al (2013) Epidemiologic study of residential proximity to transmission lines and childhood cancer in California: description of design, epidemiologic methods and study population. J Expo Sci Environ Epidemiol 25(1):45–52
Vergara XP, Kavet R, Crespi CM et al (2015) Estimating magnetic fields of homes near transmission lines in the california power line study. Environ Res 140:514–523
The California Cancer Registry. Mission Statement & Purpose. http://www.ccrcal.org/Inside_CCR/About_Us.html. Updated March 2009. Accessed 2016
Oksuzyan S, Crespi CM, Cockburn M et al (2012) Birth weight and other perinatal characteristics and childhood leukemia in California. Cancer Epidemiol 36(6):e359–e365
Goldberg DW, Cockburn MG (2010) Improving geocode accuracy with candidate selection criteria. Trans GIS 14(s1):149–176
Raghunathan TE, Lepkowski JM, Van Hoewyk J, Solenberger P (2001) A multivariate technique for multiply imputing missing values using a sequence of regression models. Surv Methodol 27:85–95
Van Buuren S, Boshuizen HC, Knook DL (1999) Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med 18:681–694
Bunch KJ, Keegan TJ, Swanson J et al (2014) Residential distance at birth from overhead high-voltage powerlines: childhood cancer risk in Britain 1962–2008. Br J Cancer 110(5):1402–1408
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/. Published 2014
Oksuzyan S, Crespi CM, Cockburn M et al (2015) Race/ethnicity and the risk of childhood leukaemia: a case–control study in California. J Epidemiol Community Health 69(8):795–802
Oksuzyan S, Crespi CM, Cockburn M, et al. (2015) Socio-economic status and childhood leukemia in California. Cancer Prev Curr Res 3(4)
Kheifets L, Swanson J, Yuan Y et al (2016) Comparative analyses of studies of magnetic fields, radon and gamma radiation. J Radiol Prot 37(2):459
Acknowledgments
The California Power Line Study is funded by the Electric Power Research Institute. Crespi was also partially support by National Institutes of Health CA 16042. The study was approved by University of California, Los Angeles (UCLA) Office for the Protection of Research Subjects, University of Southern California (USC) Institutional Review Board, and California Committee for the Protection of Human Subjects (CPHS). We are extremely grateful to Michael Herz of Pacific Gas and Electric Company, Glenn Sias and Phil Hung from Southern California Edison, Marilyn Dulich of San Diego Gas and Electric Company, Josephine Gonzalez of Los Angeles Department of Water and Power, and other employees of these utilities who contributed generously of their time and provided key data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Kheifets, L., Crespi, C.M., Hooper, C. et al. Residential magnetic fields exposure and childhood leukemia: a population-based case–control study in California. Cancer Causes Control 28, 1117–1123 (2017). https://doi.org/10.1007/s10552-017-0951-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-017-0951-6